
Neural Network-Enabled Identification of Weak Inspiratory Efforts during Pressure Support Ventilation Using Ventilator Waveforms
 , , ,
, , ,
Abstract
:1. Introduction
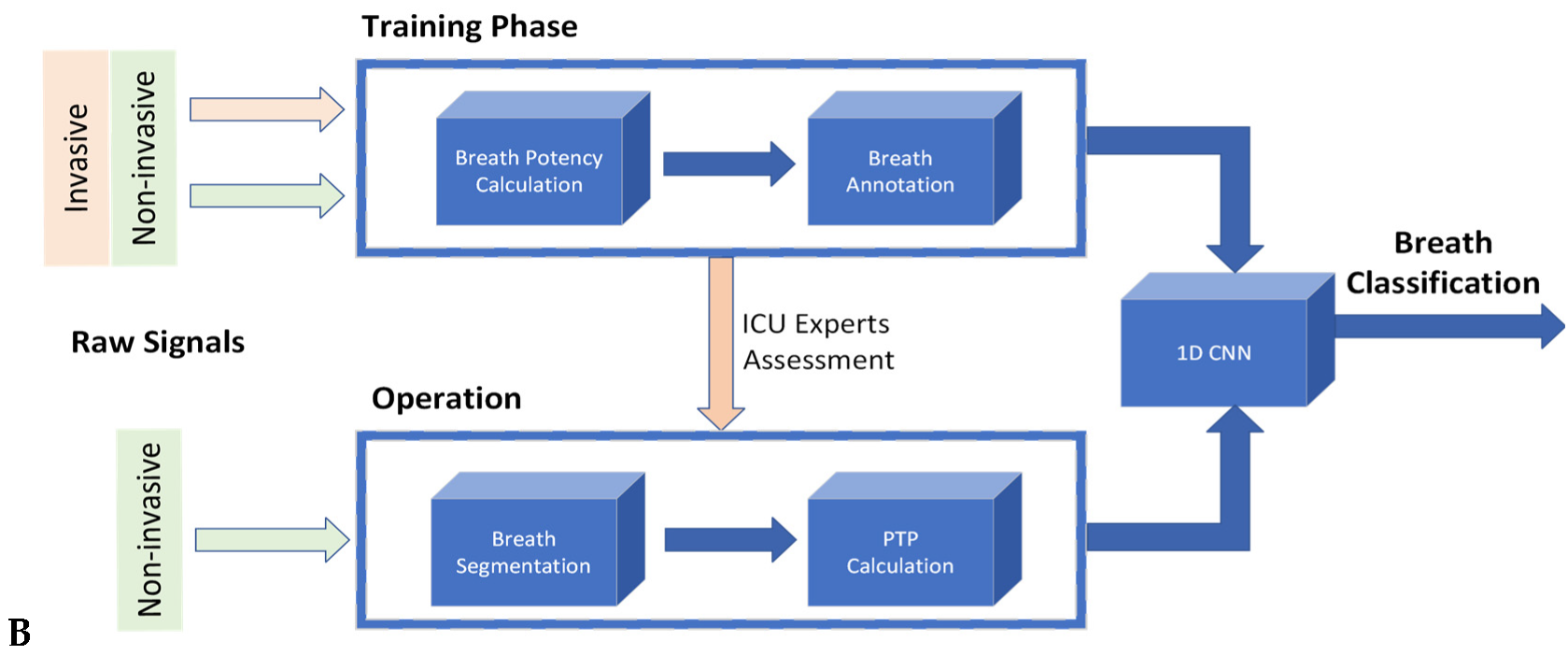
2. Materials and Methods
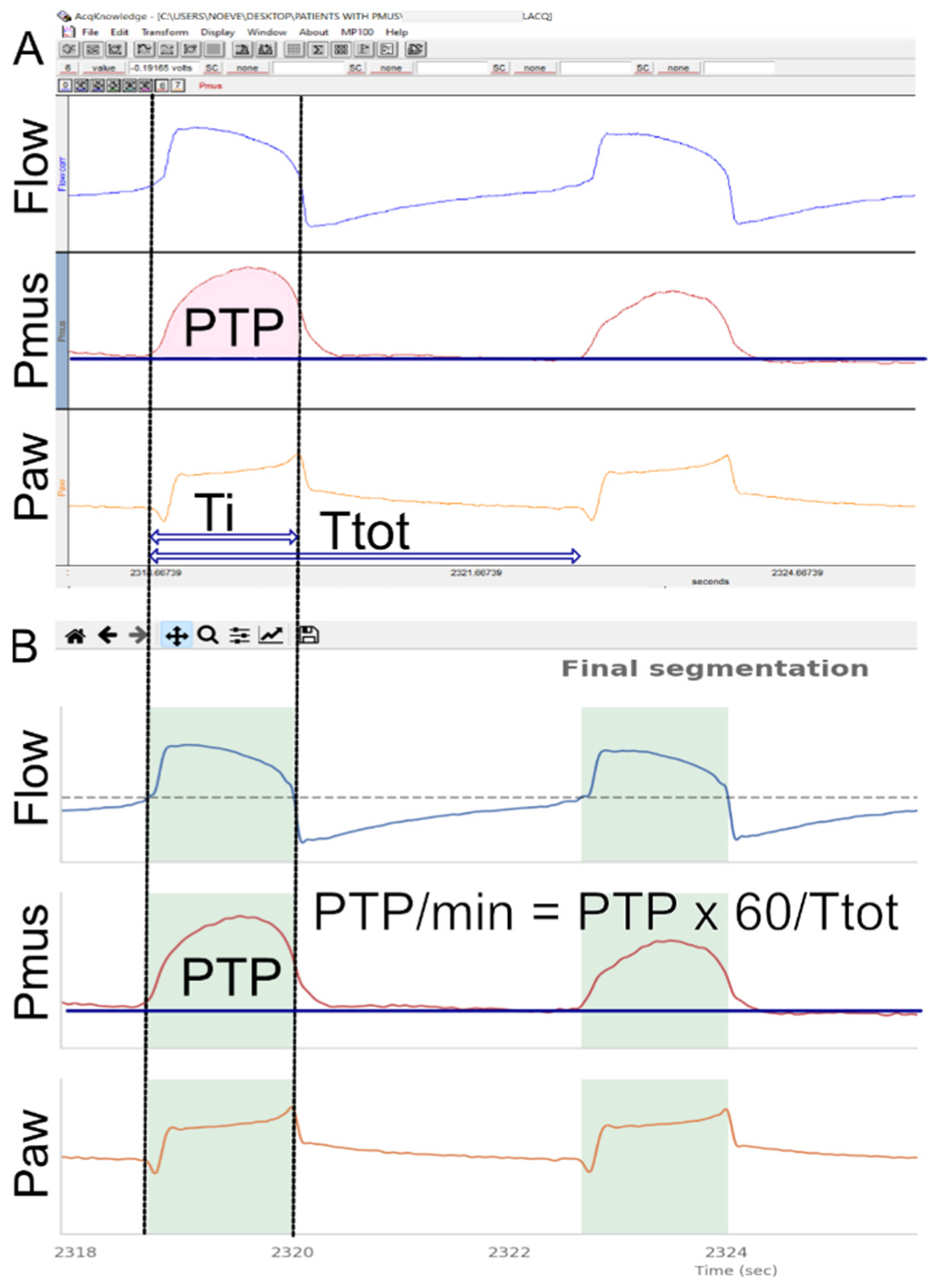
2.1. Development of the Annotated Dataset
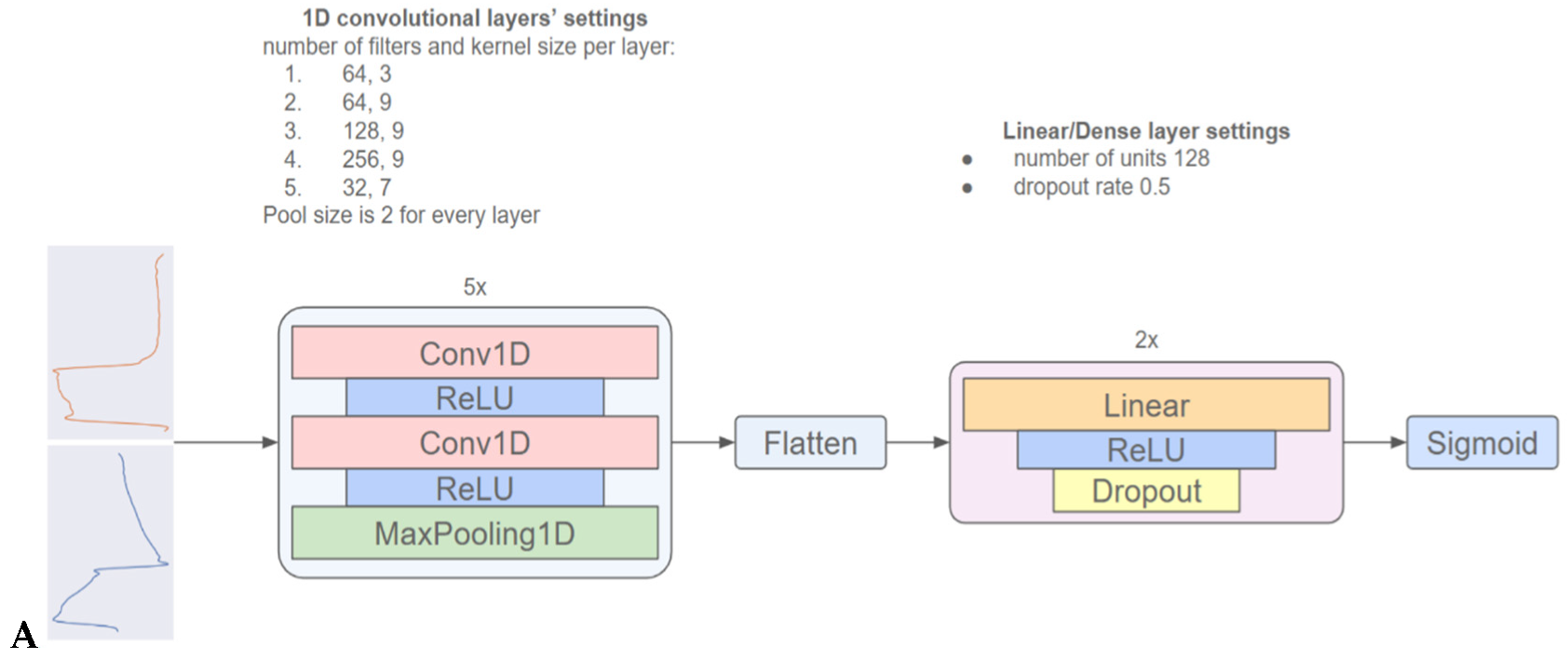
2.2. Development of the 1D-CNN to Identify Weak Efforts
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
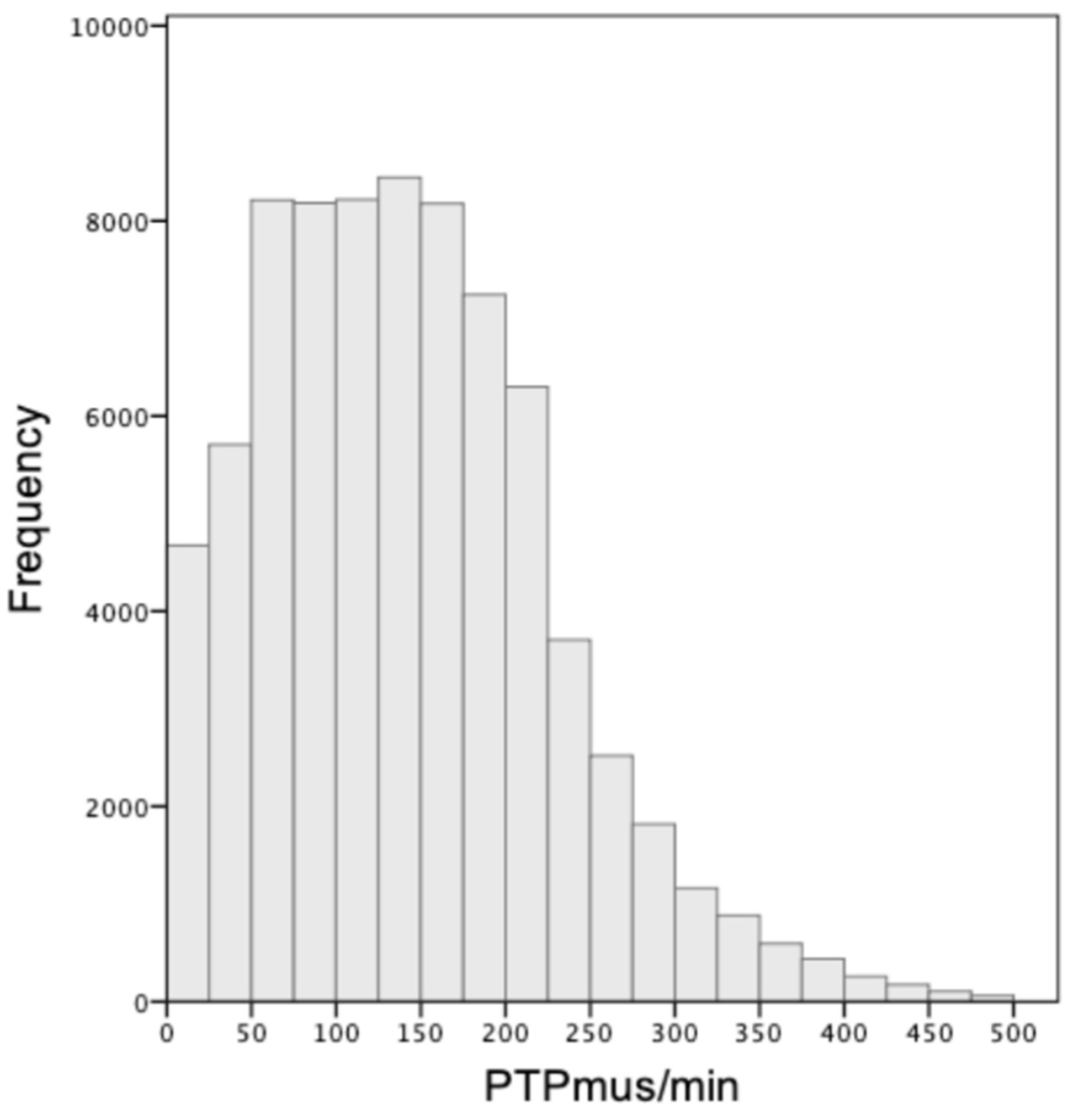
3.2. Validations of the Annotated Dataset
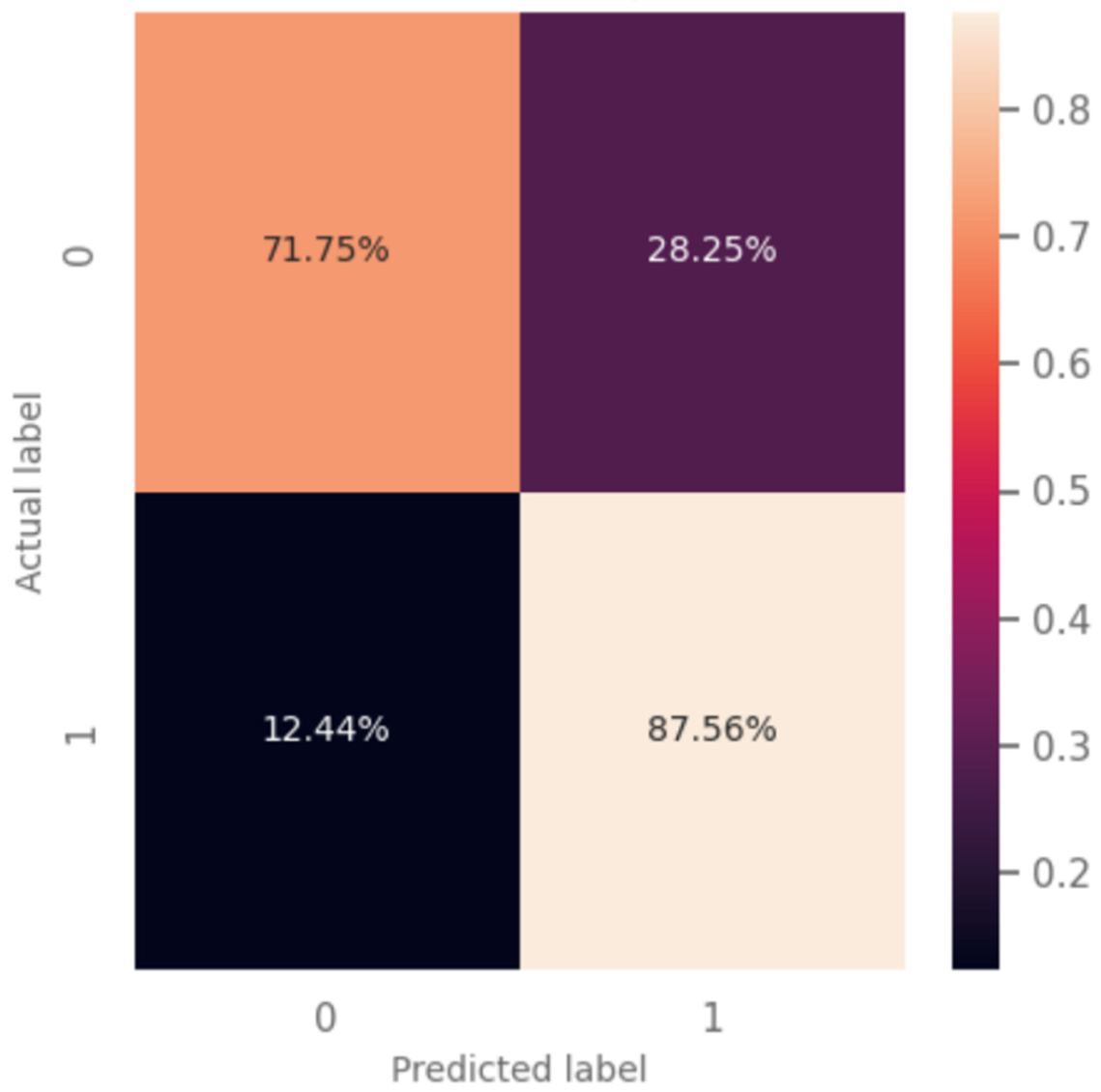
3.3. Predictive Model Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goligher, E.C.; Brochard, L.J.; Reid, W.D.; Fan, E.; Saarela, O.; Slutsky, A.S.; Kavanagh, B.P.; Rubenfeld, G.D.; Ferguson, N.D. Diaphragmatic myotrauma: A mediator of prolonged ventilation and poor patient outcomes in acute respiratory failure. Lancet Respir. Med. 2019, 7, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Jonkman, A.H.; Dianti, J.; Vaporidi, K.; Beitler, J.R.; Patel, B.K.; Yoshida, T.; Jaber, S.; Dres, M.; Mauri, T.; et al. Clinical strategies for implementing lung and diaphragm-protective ventilation: Avoiding insufficient and excessive effort. Intensive Care Med. 2020, 46, 2314–2326. [Google Scholar] [CrossRef] [PubMed]
- Schepens, T.; Dres, M.; Heunks, L.; Goligher, E.C. Diaphragm-protective mechanical ventilation. Curr. Opin. Crit. Care 2019, 25, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.; Nguyen, T.; Taylor, N.; Friscia, M.E.; Budak, M.T.; Rothenberg, P.; Zhu, J.; Sachdeva, R.; Sonnad, S.; Kaiser, L.R.; et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N. Engl. J. Med. 2008, 358, 1327–1335. [Google Scholar] [CrossRef]
- Karageorgos, V.; Proklou, A.; Vaporidi, K. Lung and diaphragm protective ventilation: A synthesis of recent data. Expert Rev. Respir. Med. 2022, 16, 375–390. [Google Scholar] [CrossRef]
- Goligher, E.C.; Dres, M.; Fan, E.; Rubenfeld, G.D.; Scales, D.C.; Herridge, M.S.; Vorona, S.; Sklar, M.C.; Rittayamai, N.; Lanys, A.; et al. Mechanical Ventilation-induced Diaphragm Atrophy Strongly Impacts Clinical Outcomes. Am. J. Respir. Crit. Care Med. 2018, 197, 204–213. [Google Scholar] [CrossRef]
- Yoshida, T.; Brochard, L. Esophageal pressure monitoring: Why, when and how? Curr. Opin. Crit. Care 2018, 24, 216–222. [Google Scholar] [CrossRef]
- Telias, I.; Junhasavasdikul, D.; Rittayamai, N.; Piquilloud, L.; Chen, L.; Ferguson, N.D.; Goligher, E.C.; Brochard, L. Airway Occlusion Pressure As an Estimate of Respiratory Drive and Inspiratory Effort during Assisted Ventilation. Am. J. Respir. Crit. Care Med. 2020, 201, 1086–1098. [Google Scholar] [CrossRef]
- Tobin, M.J.; Laghi, F.; Jubran, A. Narrative review: Ventilator-induced respiratory muscle weakness. Ann. Intern. Med. 2010, 153, 240–245. [Google Scholar] [CrossRef]
- Georgopoulos, D.; Prinianakis, G.; Kondili, E. Bedside waveforms interpretation as a tool to identify patient-ventilator asynchronies. Intensive Care Med. 2006, 32, 34–47. [Google Scholar] [CrossRef]
- Vaporidi, K.; Soundoulounaki, S.; Papadakis, E.; Akoumianaki, E.; Kondili, E.; Georgopoulos, D. Esophageal and transdiaphragmatic pressure swings as indices of inspiratory effort. Respir. Physiol. Neurobiol. 2021, 284, 103561. [Google Scholar] [CrossRef]
- Soundoulounaki, S.; Akoumianaki, E.; Kondili, E.; Pediaditis, E.; Prinianakis, G.; Vaporidi, K.; Georgopoulos, D. Airway pressure morphology and respiratory muscle activity during end-inspiratory occlusions in pressure support ventilation. Crit. Care Lond. Engl. 2020, 24, 467. [Google Scholar] [CrossRef]
- Kondili, E.; Prinianakis, G.; Alexopoulou, C.; Vakouti, E.; Klimathianaki, M.; Georgopoulos, D. Respiratory load compensation during mechanical ventilation—Proportional assist ventilation with load-adjustable gain factors versus pressure support. Intensive Care Med. 2006, 32, 692–699. [Google Scholar] [CrossRef]
- Carteaux, G.; Córdoba-Izquierdo, A.; Lyazidi, A.; Heunks, L.; Thille, A.W.; Brochard, L. Comparison Between Neurally Adjusted Ventilatory Assist and Pressure Support Ventilation Levels in Terms of Respiratory Effort. Crit. Care Med. 2016, 44, 503–511. [Google Scholar] [CrossRef]
- Jubran, A.; Van de Graaff, W.B.; Tobin, M.J. Variability of patient-ventilator interaction with pressure support ventilation in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1995, 152, 129–136. [Google Scholar] [CrossRef]
- Goligher, E.C.; Dres, M.; Patel, B.K.; Sahetya, S.K.; Beitler, J.R.; Telias, I.; Yoshida, T.; Vaporidi, K.; Grieco, D.L.; Schepens, T.; et al. Lung- and Diaphragm-Protective Ventilation. Am. J. Respir. Crit. Care Med. 2020, 202, 950–961. [Google Scholar] [CrossRef]
- Sylligardos, E.; Sigalas, M.; Soundoulounaki, S.; Vaporidi, K.; Trahanias, P. A Deep Learning Approach to Detect Ventilatory Over-Assistance. In Pattern Recognition and Artificial Intelligence; El Yacoubi, M., Granger, E., Yuen, P.C., Pal, U., Vincent, N., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2022; Volume 13364, pp. 504–515. ISBN 978-3-031-09281-7. [Google Scholar]
- Pletsch-Assuncao, R.; Caleffi Pereira, M.; Ferreira, J.G.; Cardenas, L.Z.; de Albuquerque, A.L.P.; de Carvalho, C.R.R.; Caruso, P. Accuracy of Invasive and Noninvasive Parameters for Diagnosing Ventilatory Overassistance During Pressure Support Ventilation. Crit. Care Med. 2018, 46, 411–417. [Google Scholar] [CrossRef]
- Albani, F.; Fusina, F.; Ciabatti, G.; Pisani, L.; Lippolis, V.; Franceschetti, M.E.; Giovannini, A.; di Mussi, R.; Murgolo, F.; Rosano, A.; et al. Flow Index accurately identifies breaths with low or high inspiratory effort during pressure support ventilation. Crit. Care Lond. Engl. 2021, 25, 427. [Google Scholar] [CrossRef]
- Vaporidi, K. NAVA and PAV+ for lung and diaphragm protection. Curr. Opin. Crit. Care 2020, 26, 41–46. [Google Scholar] [CrossRef]
- Piquilloud, L.; Vignaux, L.; Bialais, E.; Roeseler, J.; Sottiaux, T.; Laterre, P.-F.; Jolliet, P.; Tassaux, D. Neurally adjusted ventilatory assist improves patient-ventilator interaction. Intensive Care Med. 2011, 37, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Kataoka, J.; Kuriyama, A.; Norisue, Y.; Fujitani, S. Proportional modes versus pressure support ventilation: A systematic review and meta-analysis. Ann. Intensive Care 2018, 8, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jhou, H.-J.; Chen, P.-H.; Ou-Yang, L.-J.; Lin, C.; Tang, S.-E.; Lee, C.-H. Methods of Weaning from Mechanical Ventilation in Adult: A Network Meta-Analysis. Front. Med. 2021, 8, 752984. [Google Scholar] [CrossRef]
- Telias, I.; Jonkman, A.; Rittayamai, N. Assisted Ventilation: Pressure Support and Bilevel Ventilation Modes. In Mechanical Ventilation from Pathophysiology to Clinical Evidence; Bellani, G., Ed.; Springer International Publishing: Cham, Switzerland, 2022; pp. 49–59. ISBN 978-3-030-93400-2. [Google Scholar]
- Albani, F.; Pisani, L.; Ciabatti, G.; Fusina, F.; Buizza, B.; Granato, A.; Lippolis, V.; Aniballi, E.; Murgolo, F.; Rosano, A.; et al. Flow Index: A novel, non-invasive, continuous, quantitative method to evaluate patient inspiratory effort during pressure support ventilation. Crit. Care Lond. Engl. 2021, 25, 196. [Google Scholar] [CrossRef] [PubMed]
- Miao, M.-Y.; Chen, W.; Zhou, Y.-M.; Gao, R.; Song, D.-J.; Wang, S.-P.; Yang, Y.-L.; Zhang, L.; Zhou, J.-X. Validation of the flow index to detect low inspiratory effort during pressure support ventilation. Ann. Intensive Care 2022, 12, 89. [Google Scholar] [CrossRef] [PubMed]
- Dhar, T.; Dey, N.; Borra, S.; Sherratt, R.S. Challenges of Deep Learning in Medical Image Analysis—Improving Explainability and Trust. IEEE Trans. Technol. Soc. 2023, 3234203. [Google Scholar] [CrossRef]
- Ossai, C.I.; Wickramasinghe, N. Intelligent decision support with machine learning for efficient management of mechanical ventilation in the intensive care unit—A critical overview. Int. J. Med. Inf. 2021, 150, 104469. [Google Scholar] [CrossRef]
- Casagrande, A.; Quintavalle, F.; Fernandez, R.; Blanch, L.; Ferluga, M.; Lena, E.; Fabris, F.; Lucangelo, U. An effective pressure-flow characterization of respiratory asynchronies in mechanical ventilation. J. Clin. Monit. Comput. 2021, 35, 289–296. [Google Scholar] [CrossRef]
- Gholami, B.; Phan, T.S.; Haddad, W.M.; Cason, A.; Mullis, J.; Price, L.; Bailey, J.M. Replicating human expertise of mechanical ventilation waveform analysis in detecting patient-ventilator cycling asynchrony using machine learning. Comput. Biol. Med. 2018, 97, 137–144. [Google Scholar] [CrossRef]
- Zhang, L.; Mao, K.; Duan, K.; Fang, S.; Lu, Y.; Gong, Q.; Lu, F.; Jiang, Y.; Jiang, L.; Fang, W.; et al. Detection of patient-ventilator asynchrony from mechanical ventilation waveforms using a two-layer long short-term memory neural network. Comput. Biol. Med. 2020, 120, 103721. [Google Scholar] [CrossRef]
- Pan, Q.; Zhang, L.; Jia, M.; Pan, J.; Gong, Q.; Lu, Y.; Zhang, Z.; Ge, H.; Fang, L. An interpreTable 1D convolutional neural network for detecting patient-ventilator asynchrony in mechanical ventilation. Comput. Methods Programs Biomed. 2021, 204, 106057. [Google Scholar] [CrossRef]
- Bollepalli, S.C.; Sevakula, R.K.; Au-Yeung, W.-T.M.; Kassab, M.B.; Merchant, F.M.; Bazoukis, G.; Boyer, R.; Isselbacher, E.M.; Armoundas, A.A. Real-Time Arrhythmia Detection Using Hybrid Convolutional Neural Networks. J. Am. Heart Assoc. 2021, 10, e023222. [Google Scholar] [CrossRef]
- Khurshid, S.; Friedman, S.; Reeder, C.; Di Achille, P.; Diamant, N.; Singh, P.; Harrington, L.X.; Wang, X.; Al-Alusi, M.A.; Sarma, G.; et al. ECG-Based Deep Learning and Clinical Risk Factors to Predict Atrial Fibrillation. Circulation 2022, 145, 122–133. [Google Scholar] [CrossRef]
- Galloway, C.D.; Valys, A.V.; Shreibati, J.B.; Treiman, D.L.; Petterson, F.L.; Gundotra, V.P.; Albert, D.E.; Attia, Z.I.; Carter, R.E.; Asirvatham, S.J.; et al. Development and Validation of a Deep-Learning Model to Screen for Hyperkalemia from the Electrocardiogram. JAMA Cardiol. 2019, 4, 428–436. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline characteristics | Age (years) | 70 ± 10 |
| Males | 46% | |
| BMI | 30 ± 8 | |
| APACHE-II score | 19.3 ± 7.5 | |
| Admission diagnosis | Hypoxemic RF | 38% |
| Hypercapnic RF | 19% | |
| Septic Shock | 19% | |
| Acute brain injury | 24% | |
| Ventilation characteristics | Duration of MV prior to recording (days) | 9 (IQR 5–12) |
| PEEP cmH2O | 7 ± 2 | |
| FiO2 | 35% (IQR 30–40%) | |
| PaO2/FiO2 | 252 ± 63 | |
| VT mL/kg IBW | 7.7 (IQR 6.9–9.2) | |
| RR br/min | 21 ± 5 | |
| VE L/min | 9.6 ± 1.6 | |
| Pressure support cmH2O | 7 ± 2 | |
| Respiratory system compliance * mL/cmH2O | 46 ± 14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soundoulounaki, S.; Sylligardos, E.; Akoumianaki, E.; Sigalas, M.; Kondili, E.; Georgopoulos, D.; Trahanias, P.; Vaporidi, K. Neural Network-Enabled Identification of Weak Inspiratory Efforts during Pressure Support Ventilation Using Ventilator Waveforms. J. Pers. Med. 2023, 13, 347. https://doi.org/10.3390/jpm13020347
Soundoulounaki S, Sylligardos E, Akoumianaki E, Sigalas M, Kondili E, Georgopoulos D, Trahanias P, Vaporidi K. Neural Network-Enabled Identification of Weak Inspiratory Efforts during Pressure Support Ventilation Using Ventilator Waveforms. Journal of Personalized Medicine. 2023; 13(2):347. https://doi.org/10.3390/jpm13020347
Chicago/Turabian StyleSoundoulounaki, Stella, Emmanouil Sylligardos, Evangelia Akoumianaki, Markos Sigalas, Eumorfia Kondili, Dimitrios Georgopoulos, Panos Trahanias, and Katerina Vaporidi. 2023. "Neural Network-Enabled Identification of Weak Inspiratory Efforts during Pressure Support Ventilation Using Ventilator Waveforms" Journal of Personalized Medicine 13, no. 2: 347. https://doi.org/10.3390/jpm13020347