
Association of Oral Health with Risk of Rheumatoid Arthritis: A Nationwide Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
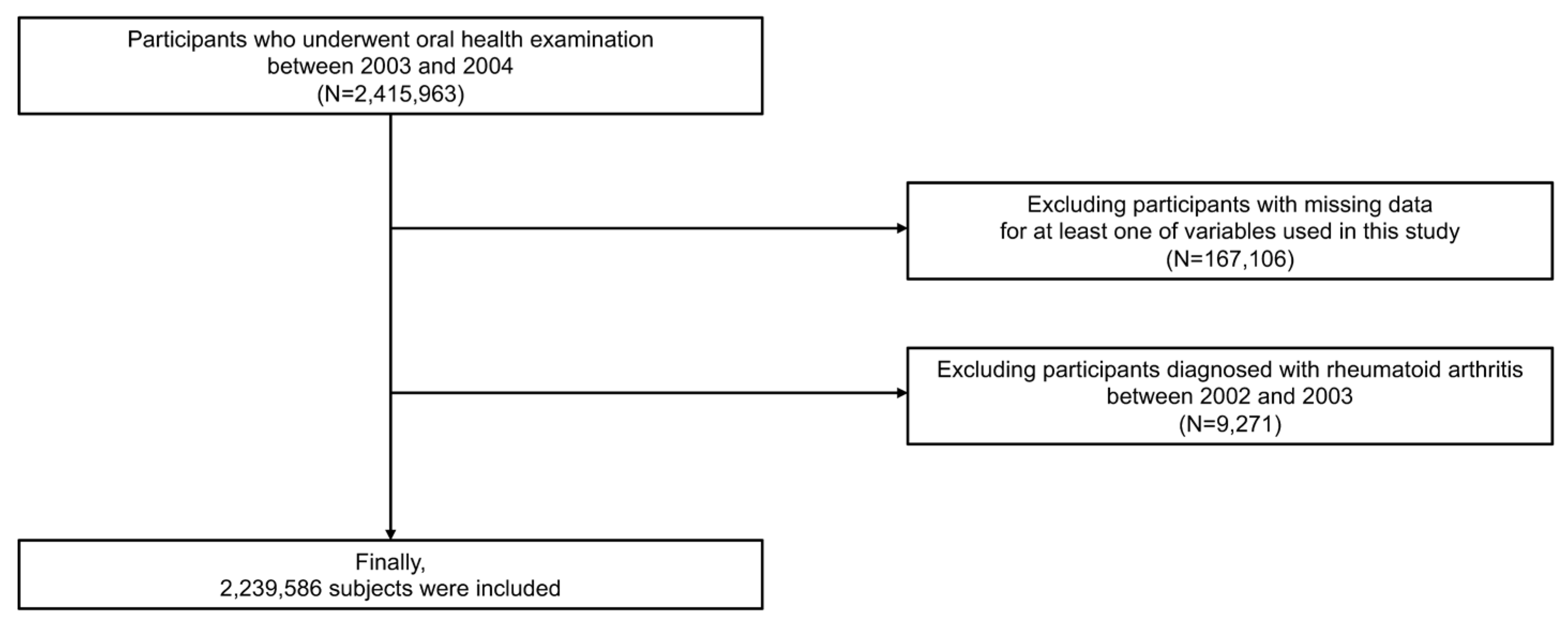
2.2. Study Population
2.3. Definitions and Variables
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Dye, B.A. Global periodontal disease epidemiology. Periodontol 2000 2012, 58, 10–25. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Prim. 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Liang, S.; Payne, M.A.; Hashim, A.; Jotwani, R.; Eskan, M.A.; McIntosh, M.L.; Alsam, A.; Kirkwood, K.L.; Lambris, J.D.; et al. Low-abundance biofilm species orchestrates inflammatory periodontal disease through the commensal microbiota and complement. Cell Host Microbe 2011, 10, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krutyhołowa, A.; Strzelec, K.; Dziedzic, A.; Bereta, G.P.; Łazarz-Bartyzel, K.; Potempa, J.; Gawron, K. Host and bacterial factors linking periodontitis and rheumatoid arthritis. Front. Immunol. 2022, 13, 980805. [Google Scholar] [CrossRef]
- Garlet, G.P. Destructive and protective roles of cytokines in periodontitis: A re-appraisal from host defense and tissue destruction viewpoints. J. Dent. Res. 2010, 89, 1349–1363. [Google Scholar] [CrossRef]
- Martínez-García, M.; Hernández-Lemus, E. Periodontal inflammation and systemic diseases: An overview. Front. Physiol. 2021, 12, 709438. [Google Scholar] [CrossRef]
- Giuca, M.R.; Lardani, L.; Ligori, S.; Carli, E.; Giuca, G.; Miceli, M. Oral manifestations in paediatric patients with hepatobiliary diseases: A review. J. Biol. Regul. Homeost. Agents 2021, 35, 117–125. [Google Scholar]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [Green Version]
- Song, T.J.; Kim, J.W.; Kim, J. Oral health and changes in lipid profile: A nationwide cohort study. J. Clin. Periodontol. 2020, 47, 1437–1445. [Google Scholar] [CrossRef]
- Woo, H.G.; Chang, Y.; Lee, J.S.; Song, T.J. Association of tooth loss with new-onset parkinson’s disease: A nationwide population-based cohort study. Park. Dis. 2020, 2020, 4760512. [Google Scholar] [CrossRef]
- Chang, Y.; Woo, H.G.; Lee, J.S.; Song, T.J. Better oral hygiene is associated with lower risk of stroke. J. Periodontol. 2021, 92, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Lee, J.S.; Kim, J.; Lee, H.; Chang, Y.; Woo, H.G.; Kim, J.W.; Song, T.J. Oral health and gastrointestinal cancer: A nationwide cohort study. J. Clin. Periodontol. 2020, 47, 796–808. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, H.J.; Jeon, J.; Song, T.J. Association between oral health and cardiovascular outcomes in patients with hypertension: A nationwide cohort study. J. Hypertens. 2022, 40, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Song, T.J.; Chang, Y.; Jeon, J.; Kim, J. Oral health and longitudinal changes in fasting glucose levels: A nationwide cohort study. PLoS ONE 2021, 16, e0253769. [Google Scholar] [CrossRef]
- Kim, H.; Sung, Y.-K. Epidemiology of rheumatoid arthritis in korea. J. Rheum. Dis. 2021, 28, 60–67. [Google Scholar] [CrossRef]
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; McInnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Prim. 2018, 4, 18001. [Google Scholar] [CrossRef]
- de Pablo, P.; Dietrich, T.; McAlindon, T.E. Association of periodontal disease and tooth loss with rheumatoid arthritis in the us population. J. Rheumatol. 2008, 35, 70–76. [Google Scholar]
- Chen, H.H.; Huang, N.; Chen, Y.M.; Chen, T.J.; Chou, P.; Lee, Y.L.; Chou, Y.J.; Lan, J.L.; Lai, K.L.; Lin, C.H.; et al. Association between a history of periodontitis and the risk of rheumatoid arthritis: A nationwide, population-based, case-control study. Ann. Rheum. Dis. 2013, 72, 1206–1211. [Google Scholar] [CrossRef]
- Bonfil, J.J.; Dillier, F.L.; Mercier, P.; Reviron, D.; Foti, B.; Sambuc, R.; Brodeur, J.M.; Sedarat, C. A “case control” study on the rôle of hla dr4 in severe periodontitis and rapidly progressive periodontitis. Identification of types and subtypes using molecular biology (pcr.Sso). J. Clin. Periodontol. 1999, 26, 77–84. [Google Scholar] [CrossRef]
- Kallberg, H.; Padyukov, L.; Plenge, R.M.; Ronnelid, J.; Gregersen, P.K.; van der Helm-van Mil, A.H.; Toes, R.E.; Huizinga, T.W.; Klareskog, L.; Alfredsson, L. Gene-gene and gene-environment interactions involving hla-drb1, ptpn22, and smoking in two subsets of rheumatoid arthritis. Am. J. Hum. Genet. 2007, 80, 867–875. [Google Scholar] [CrossRef] [Green Version]
- Klareskog, L.; Stolt, P.; Lundberg, K.; Källberg, H.; Bengtsson, C.; Grunewald, J.; Rönnelid, J.; Harris, H.E.; Ulfgren, A.K.; Rantapää-Dahlqvist, S.; et al. A new model for an etiology of rheumatoid arthritis: Smoking may trigger hla-dr (shared epitope)-restricted immune reactions to autoantigens modified by citrullination. Arthritis Rheum. 2006, 54, 38–46. [Google Scholar] [CrossRef] [PubMed]
- van Winkelhoff, A.J.; Bosch-Tijhof, C.J.; Winkel, E.G.; van der Reijden, W.A. Smoking affects the subgingival microflora in periodontitis. J. Periodontol. 2001, 72, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Martinez, R.E.; Abud-Mendoza, C.; Patiño-Marin, N.; Rizo-Rodríguez, J.C.; Little, J.W.; Loyola-Rodríguez, J.P. Detection of periodontal bacterial DNA in serum and synovial fluid in refractory rheumatoid arthritis patients. J. Clin. Periodontol. 2009, 36, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- de Smit, M.; Westra, J.; Vissink, A.; Doornbos-van der Meer, B.; Brouwer, E.; van Winkelhoff, A.J. Periodontitis in established rheumatoid arthritis patients: A cross-sectional clinical, microbiological and serological study. Arthritis Res. Ther. 2012, 14, R222. [Google Scholar] [CrossRef] [Green Version]
- Joseph, R.; Rajappan, S.; Nath, S.G.; Paul, B.J. Association between chronic periodontitis and rheumatoid arthritis: A hospital-based case-control study. Rheumatol. Int. 2013, 33, 103–109. [Google Scholar] [CrossRef]
- Chang, Y.; Woo, H.G.; Park, J.; Lee, J.S.; Song, T.J. Improved oral hygiene care is associated with decreased risk of occurrence for atrial fibrillation and heart failure: A nationwide population-based cohort study. Eur. J. Prev. Cardiol. 2020, 27, 1835–1845. [Google Scholar] [CrossRef]
- Chang, Y.; Lee, J.S.; Lee, K.J.; Woo, H.G.; Song, T.J. Improved oral hygiene is associated with decreased risk of new-onset diabetes: A nationwide population-based cohort study. Diabetologia 2020, 63, 924–933. [Google Scholar] [CrossRef]
- Park, J.-H.; Kwoen, M.-J.; Lee, J.-R.; Kim, K.-S.; Lee, H.-J.; Kim, J.-W.; Lee, H. Gradual, but not sudden, dose-dependent increase of onj risk with bisphosphonate exposure: A nationwide cohort study in women with osteoporosis. Front. Endocrinol. 2021, 12, 1674. [Google Scholar] [CrossRef]
- Park, M.S.; Jeon, J.; Song, T.J.; Kim, J. Association of periodontitis with microvascular complications of diabetes mellitus: A nationwide cohort study. J. Diabetes Complicat. 2022, 36, 108107. [Google Scholar] [CrossRef]
- Chang, Y.; Lee, J.S.; Woo, H.G.; Ryu, D.R.; Kim, J.W.; Song, T.J. Improved oral hygiene care and chronic kidney disease occurrence: A nationwide population-based retrospective cohort study. Medicine 2021, 100, e27845. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The national health insurance service-national health screening cohort (nhis-heals) in korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, H.G.; Chang, Y.K.; Lee, J.S.; Song, T.J. Association of periodontal disease with the occurrence of unruptured cerebral aneurysm among adults in korea: A nationwide population-based cohort study. Medicina 2021, 57, 910. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.-K.; Sung, Y.-K.; Choi, C.-B.; Kwon, J.-M.; Lee, E.-K.; Bae, S.-C. Development of an algorithm for identifying rheumatoid arthritis in the korean national health insurance claims database. Rheumatol. Int. 2013, 33, 2985–2992. [Google Scholar] [CrossRef] [PubMed]
- Arkema, E.V.; Karlson, E.W.; Costenbader, K.H. A prospective study of periodontal disease and risk of rheumatoid arthritis. J. Rheumatol. 2010, 37, 1800–1804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuggle, N.R.; Smith, T.O.; Kaul, A.; Sofat, N. Hand to mouth: A systematic review and meta-analysis of the association between rheumatoid arthritis and periodontitis. Front. Immunol. 2016, 7, 80. [Google Scholar] [CrossRef] [Green Version]
- Araújo, V.M.; Melo, I.M.; Lima, V. Relationship between periodontitis and rheumatoid arthritis: Review of the literature. Mediat. Inflamm. 2015, 2015, 259074. [Google Scholar] [CrossRef] [Green Version]
- Koziel, J.; Mydel, P.; Potempa, J. The link between periodontal disease and rheumatoid arthritis: An updated review. Curr. Rheumatol. Rep. 2014, 16, 408. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Park, J.B.; Yim, H.W.; Lee, J.; Kwok, S.K.; Ju, J.H.; Kim, W.U.; Park, S.H. Rheumatoid arthritis is associated with early tooth loss: Results from korea national health and nutrition examination survey v to vi. Korean J. Intern. Med. 2019, 34, 1381–1391. [Google Scholar] [CrossRef] [Green Version]
- Ando, A.; Ohsawa, M.; Yaegashi, Y.; Sakata, K.; Tanno, K.; Onoda, T.; Itai, K.; Tanaka, F.; Makita, S.; Omama, S.; et al. Factors related to tooth loss among community-dwelling middle-aged and elderly japanese men. J. Epidemiol. 2013, 23, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, H.; Hashimoto, S.; Shimazaki, Y. Relationship between tooth loss and the medications used for the treatment of rheumatoid arthritis in japanese patients with rheumatoid arthritis: A cross-sectional study. J. Clin. Med. 2021, 10, 876. [Google Scholar] [CrossRef]
- Jeffery, L.E.; Raza, K.; Hewison, M. Vitamin d in rheumatoid arthritis-towards clinical application. Nat. Rev. Rheumatol. 2016, 12, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Ogrendik, M.; Kokino, S.; Ozdemir, F.; Bird, P.S.; Hamlet, S. Serum antibodies to oral anaerobic bacteria in patients with rheumatoid arthritis. MedGenMed 2005, 7, 2. [Google Scholar] [PubMed]
- Hajishengallis, G.; Lamont, R.J. Breaking bad: Manipulation of the host response by porphyromonas gingivalis. Eur. J. Immunol. 2014, 44, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courbon, G.; Rinaudo-Gaujous, M.; Blasco-Baque, V.; Auger, I.; Caire, R.; Mijola, L.; Vico, L.; Paul, S.; Marotte, H. Porphyromonas gingivalis experimentally induces periodontis and an anti-ccp2-associated arthritis in the rat. Ann. Rheum. Dis. 2019, 78, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Mikuls, T.R.; Payne, J.B.; Yu, F.; Thiele, G.M.; Reynolds, R.J.; Cannon, G.W.; Markt, J.; McGowan, D.; Kerr, G.S.; Redman, R.S.; et al. Periodontitis and porphyromonas gingivalis in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014, 66, 1090–1100. [Google Scholar] [CrossRef] [Green Version]
- Schmickler, J.; Rupprecht, A.; Patschan, S.; Patschan, D.; Müller, G.A.; Haak, R.; Mausberg, R.F.; Schmalz, G.; Kottmann, T.; Ziebolz, D. Cross-sectional evaluation of periodontal status and microbiologic and rheumatoid parameters in a large cohort of patients with rheumatoid arthritis. J. Periodontol. 2017, 88, 368–379. [Google Scholar] [CrossRef]
- Konig, M.F.; Abusleme, L.; Reinholdt, J.; Palmer, R.J.; Teles, R.P.; Sampson, K.; Rosen, A.; Nigrovic, P.A.; Sokolove, J.; Giles, J.T.; et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci. Transl Med. 2016, 8, 369ra176. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, M.; Jacobsen, S.; Klarlund, M.; Pedersen, B.V.; Wiik, A.; Wohlfahrt, J.; Frisch, M. Environmental risk factors differ between rheumatoid arthritis with and without auto-antibodies against cyclic citrullinated peptides. Arthritis Res. Ther. 2006, 8, R133. [Google Scholar] [CrossRef] [Green Version]
- Lertpimonchai, A.; Rattanasiri, S.; Arj-Ong Vallibhakara, S.; Attia, J.; Thakkinstian, A. The association between oral hygiene and periodontitis: A systematic review and meta-analysis. Int. Dent. J. 2017, 67, 332–343. [Google Scholar] [CrossRef] [Green Version]
- Pagano, S.; Coniglio, M.; Valenti, C.; Federici, M.I.; Lombardo, G.; Cianetti, S.; Marinucci, L. Biological effects of cannabidiol on normal human healthy cell populations: Systematic review of the literature. Biomed. Pharmacother. 2020, 132, 110728. [Google Scholar] [CrossRef]
- Baeza, M.; Morales, A.; Cisterna, C.; Cavalla, F.; Jara, G.; Isamitt, Y.; Pino, P.; Gamonal, J. Effect of periodontal treatment in patients with periodontitis and diabetes: Systematic review and meta-analysis. J. Appl. Oral Sci. 2020, 28, e20190248. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.H.; Kuo, H.C.; Liu, H.Y.; Wu, M.Y.; Chang, W.J.; Chen, J.T.; Cherng, Y.G.; Chen, T.J.; Dai, Y.X.; Wu, H.L.; et al. Association between dental scaling and reduced risk of end-stage renal disease: A nationwide matched cohort study. Int. J. Environ. Res. Public Health 2021, 18, 8910. [Google Scholar] [CrossRef] [PubMed]
- Khare, N.; Vanza, B.; Sagar, D.; Saurav, K.; Chauhan, R.; Mishra, S. Nonsurgical periodontal therapy decreases the severity of rheumatoid arthritis: A case-control study. J. Contemp. Dent. Pract. 2016, 17, 484–488. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.B.; Nguyen, T.T.; Huynh, N.C.; Nguyen, K.D.; Le, T.A.; Hoang, H.T. Effects of non-surgical periodontal treatment in rheumatoid arthritis patients: A randomized clinical trial. Dent. Med. Probl. 2021, 58, 97–105. [Google Scholar] [CrossRef]
- Kurgan, Ş.; Fentoğlu, Ö.; Önder, C.; Serdar, M.; Eser, F.; Tatakis, D.N.; Günhan, M. The effects of periodontal therapy on gingival crevicular fluid matrix metalloproteinase-8, interleukin-6 and prostaglandin e2 levels in patients with rheumatoid arthritis. J. Periodontal. Res. 2016, 51, 586–595. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Total | Periodontitis (-) | Periodontitis (+) | p-Value | Standardized Difference |
|---|---|---|---|---|---|
| No. of participants (%) | 2,239,586 | 2,178,141 (97.3) | 61,445 (2.7) | ||
| Age, years | 42.30 ± 12.77 | 42.13 ± 12.72 | 48.18 ± 13.11 | <0.001 | 0.47 |
| Sex | <0.001 | 0.09 | |||
| Male | 1,486,710 (66.4) | 1,443,442 (66.3) | 43,268 (70.4) | ||
| Female | 75,2876 (33.6) | 734,699 (33.7) | 18,177 (29.6) | ||
| Body mass index (kg/m2) | 23.55 ± 14.43 | 23.55 ± 14.61 | 23.80 ± 4.27 | <0.001 | 0.02 |
| Household income | <0.001 | −0.05 | |||
| Q1, lowest | 586,108 (26.2) | 568,304 (26.1) | 17,804 (29.0) | ||
| Q2 | 811,459 (36.2) | 789,865 (36.3) | 21,594 (35.1) | ||
| Q3 | 585,974 (26.2) | 570,645 (26.2) | 15,329 (25.0) | ||
| Q4, highest | 256,045 (11.4) | 249,327 (11.5) | 6718 (10.9) | ||
| Smoking status | <0.001 | 0.08 | |||
| Never | 1,254,341 (56.0) | 1,222,277 (56.1) | 32,064 (52.2) | ||
| Former | 240,702 (10.8) | 233,633 (10.7) | 7069 (11.5) | ||
| Current | 744,543 (33.2) | 722,231 (33.2) | 22,312 (36.3) | ||
| Alcohol consumption (days/week) | <0.001 | 0.13 | |||
| None | 1,497,601 (66.9) | 1,459,259 (67.0) | 38,342 (62.4) | ||
| 1−4 | 683,708 (30.5) | 663,955 (30.5) | 19,753 (32.2) | ||
| ≥5 | 58,277 (2.6) | 54,927 (2.5) | 3350 (5.5) | ||
| Regular physical activity (days/week) | <0.001 | −0.03 | |||
| None | 1,166,099 (52.1) | 1,132,327 (52.0) | 33,772 (55.0) | ||
| 1−4 | 912,091 (40.7) | 88,9517 (40.8) | 22,574 (36.7) | ||
| ≥5 | 161,396 (7.2) | 156,297 (7.2) | 5099 (8.3) | ||
| Comorbidities | |||||
| Hypertension | 417,862 (18.7) | 402,078 (18.5) | 15,784 (25.7) | <0.001 | 0.17 |
| Diabetes mellitus | 169,278 (7.6) | 161,760 (7.4) | 7518 (12.2) | <0.001 | 0.16 |
| Dyslipidemia | 282,436 (12.6) | 273,606 (12.6) | 8830 (14.4) | <0.001 | 0.05 |
| Atrial fibrillation | 3,741 (0.2) | 3,587 (0.2) | 154 (0.3) | <0.001 | 0.02 |
| Cancer | 20,580 (0.9) | 19,813 (0.9) | 767 (1.3) | <0.001 | 0.03 |
| Renal disease | 11,188 (0.5) | 10,755 (0.5) | 433 (0.7) | <0.001 | 0.03 |
| Oral health status | |||||
| Number of missing teeth | <0.001 | 0.35 | |||
| 0 | 1,841,776 (82.2) | 1,800,326 (82.7) | 41,450 (67.5) | ||
| 1−7 | 364,467 (16.3) | 34,7095 (15.9) | 17,372 (28.3) | ||
| 8−14 | 19,417 (0.9) | 17,486 (0.8) | 1931 (3.1) | ||
| ≥15 | 13,926 (0.6) | 13,234 (0.6) | 692 (1.1) | ||
| Oral hygiene behaviors | |||||
| Frequency of tooth brushing (times/day) | <0.001 | −0.20 | |||
| 0−1 | 278,143 (12.4) | 267,593 (12.3) | 10,550 (17.2) | ||
| 2 | 1,038,206 (46.4) | 1,007,319 (46.3) | 30,887 (50.3) | ||
| ≥3 | 923,237 (41.2) | 903,229 (41.5) | 20,008 (32.6) | ||
| Dental scaling | <0.001 | −0.11 | |||
| No | 1,726,903 (77.1) | 1,676,892 (77.0) | 50,011 (81.4) | ||
| Yes | 512,683 (22.9) | 501,249 (23.0) | 11,434 (18.6) |
| Number of Participants | Number of Events | Event Rate (%) (95% CI) | Person-Years | Incidence Rate (Per 1000 Person-Years) | Adjusted HR (95% CI) | p-Value | |
|---|---|---|---|---|---|---|---|
| Oral health status | |||||||
| Periodontitis | |||||||
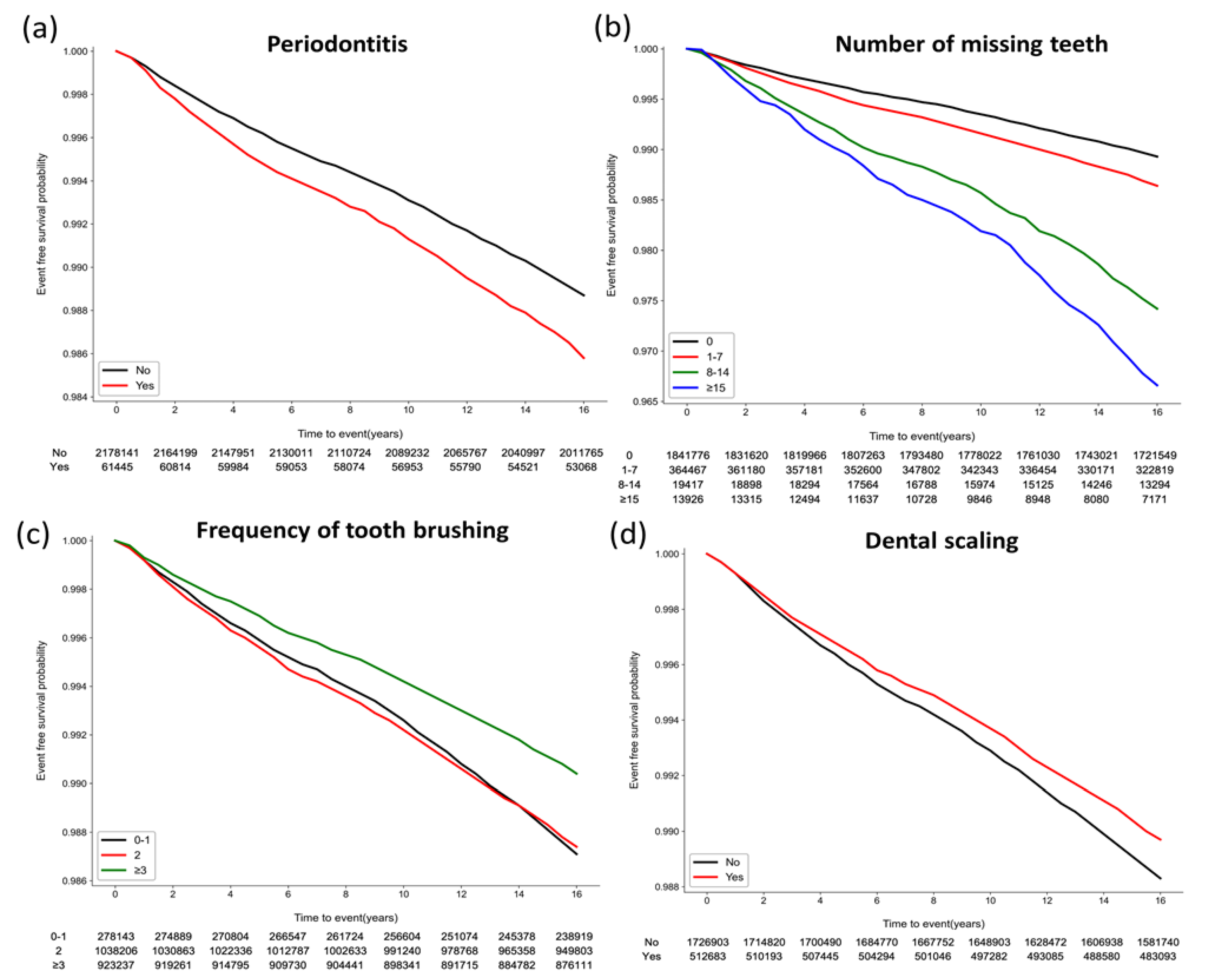
| No | 2,178,141 | 26,124 | 1.20 (1.18, 1.21) | 35,519,239.96 | 0.74 | 1 (reference) | |
| Yes | 61,445 | 905 | 1.47 (1.38, 1.57) | 981,934.40 | 0.92 | 1.16 (1.08, 1.24) | <0.001 |
| Number of missing teeth | |||||||
| 0 | 1,841,776 | 20,930 | 1.14 (1.12, 1.15) | 30,190,662.71 | 0.69 | 1 (reference) | |
| 1−7 | 364,467 | 5219 | 1.43 (1.39, 1.47) | 5,848,836.32 | 0.89 | 1.20 (1.17, 1.24) | <0.001 |
| 8−14 | 19,417 | 475 | 2.45 (2.23, 2.67) | 281,567.14 | 1.69 | 1.49 (1.36, 1.63) | <0.001 |
| ≥15 | 13,926 | 405 | 2.91 (2.62, 3.19) | 180,108.18 | 2.25 | 1.52 (1.38, 1.69) | <0.001 |
| Oral hygiene behaviors | |||||||
| Frequency of tooth brushing (times/day) | |||||||
| 0−1 | 278,143 | 3753 | 1.35 (1.31, 1.39) | 4,403,805.12 | 0.85 | 1 (reference) | |
| 2 | 1,038,206 | 13,899 | 1.34 (1.32, 1.36) | 16,904,333.57 | 0.82 | 0.98 (0.95, 1.02) | 0.300 |
| ≥3 | 923,237 | 9377 | 1.02 (1.00, 1.04) | 15,193,035.67 | 0.62 | 0.76 (0.73, 0.79) | <0.001 |
| Dental scaling | |||||||
| No | 1,726,903 | 21,398 | 1.24 (1.22, 1.26) | 28,070,869.40 | 0.76 | 1 (reference) | |
| Yes | 512,683 | 5631 | 1.10 (1.07, 1.13) | 8,430,304.96 | 0.67 | 0.96 (0.94, 0.99) | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, Y.; Chung, M.K.; Park, J.-H.; Song, T.-J. Association of Oral Health with Risk of Rheumatoid Arthritis: A Nationwide Cohort Study. J. Pers. Med. 2023, 13, 340. https://doi.org/10.3390/jpm13020340
Chang Y, Chung MK, Park J-H, Song T-J. Association of Oral Health with Risk of Rheumatoid Arthritis: A Nationwide Cohort Study. Journal of Personalized Medicine. 2023; 13(2):340. https://doi.org/10.3390/jpm13020340
Chicago/Turabian StyleChang, Yoonkyung, Min Kyung Chung, Jung-Hyun Park, and Tae-Jin Song. 2023. "Association of Oral Health with Risk of Rheumatoid Arthritis: A Nationwide Cohort Study" Journal of Personalized Medicine 13, no. 2: 340. https://doi.org/10.3390/jpm13020340