
Positive Clinical Outcomes for Severe Reported Pain Using Robust Non-Addictive Home Electrotherapy—A Case-Series
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocols
2.2. Characteristics of H-Wave® Electrotherapy
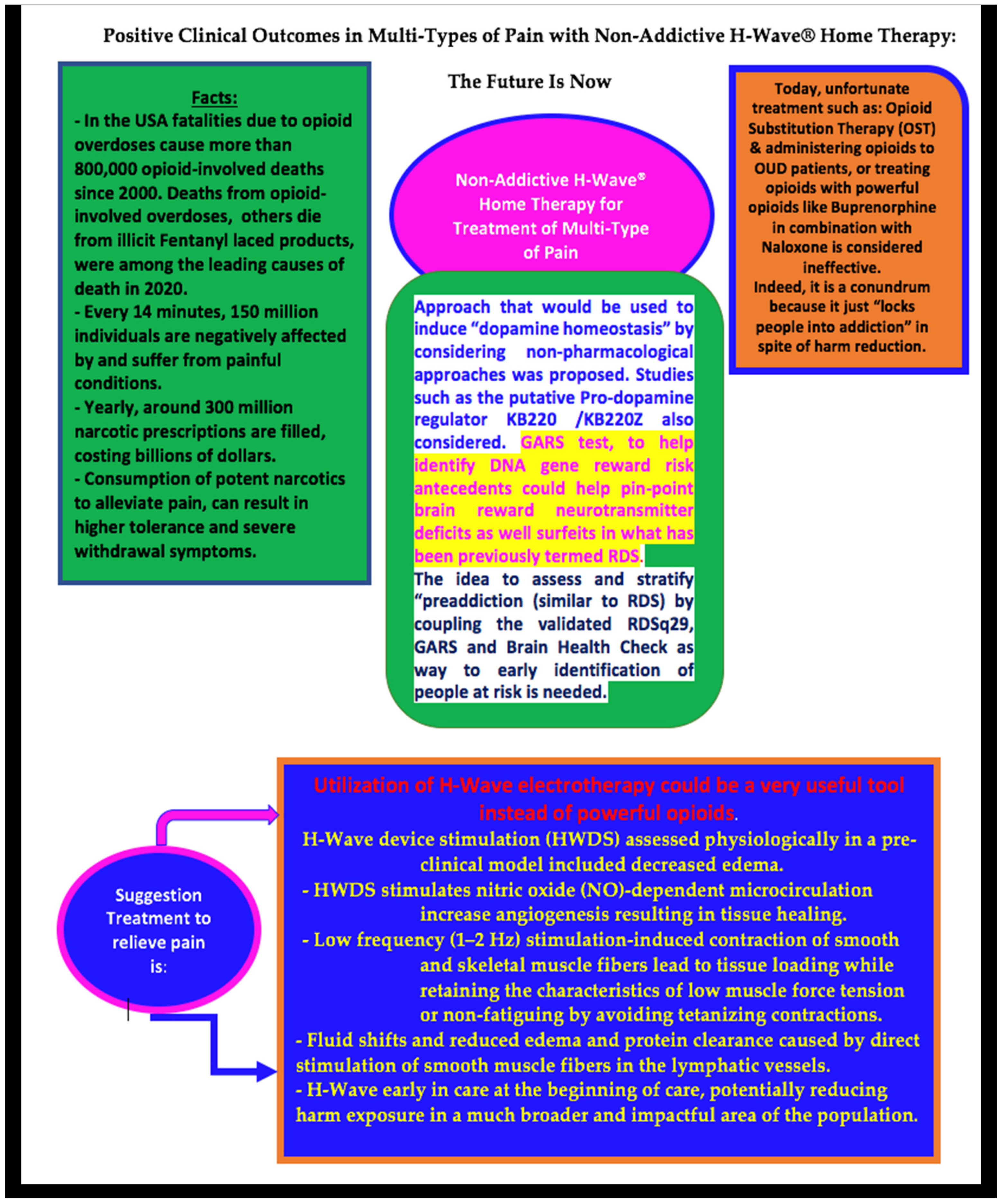
- Low frequency (1–2 Hz) stimulation-induced contraction of smooth and skeletal muscle (red, slow-twitch) fibers lead to tissue loading while retaining the characteristics of low muscle force tension or non-fatiguing by avoiding tetanizing contractions.
- NO-dependent arteriolar vasodilation (revealed by rat studies).
- Bromouridine staining showed enhanced angiogenesis in repetitive stimulation in rats.
- Fluid shifts and reduced edema and protein clearance are caused by direct stimulation of smooth muscle fibers in the lymphatic vessels.
- A high frequency (60–70 Hz) mode can be used simultaneously to act intrinsically upon the nerve, affecting the function of the sodium pump within the nerve, to create a lasting anesthetic/analgesic effect.
- Direct stimulation of the smooth muscles of lymphatic vessels and small-diameter skeletal muscle fibers by low-frequency (1–2 Hz) stimulation resulting in interstitial fluid shifts. Long rhythmical contractions of these particular muscles caused by HWDS lead to a decline in accretion of inflammation-associated proteins, an essential part of pain and associated disability in chronic injury or trauma patients.
- HWDS at high frequency (60 Hz) affects the function of sodium pumps in nerves leading to analgesic and/or anesthetic effects.
- NO-dependent stimulation of skeletal muscles induced by HWDS results in significant microcirculation increase, as evident from preclinical studies.
- Angiogenesis causes a profound and rapid increase in blood flow, which is seen in rat hind limbs post-repetitive HWDS.
2.3. Statistics
2.4. Demographics (See Table 1)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | 68.8 ± 9.4 (range 58–78) | |
| Sex | Male 75%; Female 25% | |
| Region of Care | LE | 100% |
| Knee | 75% | |
| Ankle | 25% | |
| Foot | 25% | |
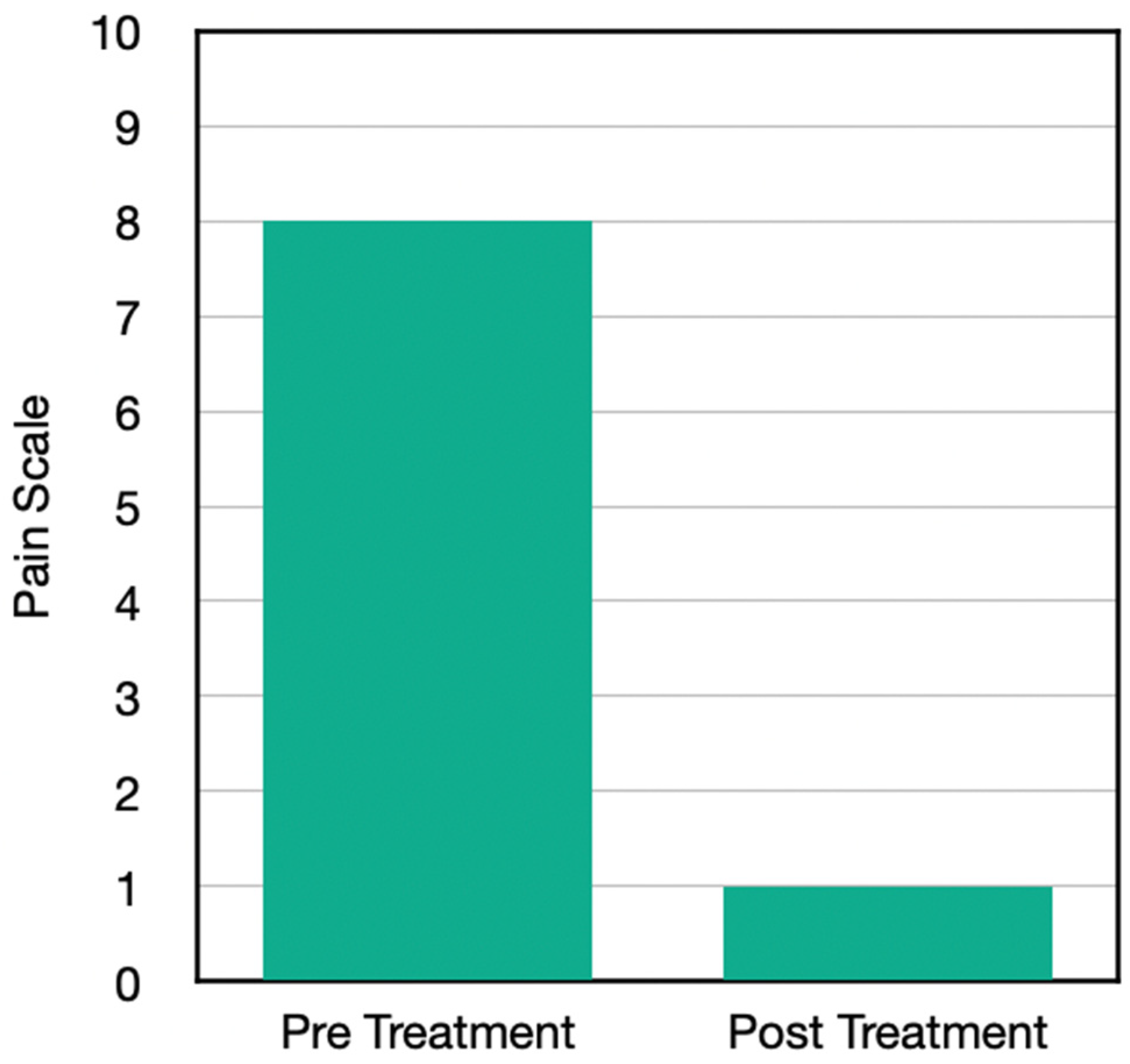
| Initial Pain | 8.3 ± 1.0 | |
| Post-treatment Pain | 1.3 ± 1.3 | |
| Delta/10 | 8.6 ± 1.1 | |
| Taking Medicine | Yes 50%; No 50% | |
| Reduction of Medicine after Treatment | One patient reported 100% reduction, the other patient reported 75% reduction. | |
| Functional Improvement after Treatment | walk further | 100% |
| stand longer | 100% | |
| more housework | 75% | |
| greater ability to drive an automobile | 50% | |
| lift more | 50% | |
| sit longer | 25% | |
| sleep better | 25% | |
2.5. Statistical Analysis
2.6. H-Wave Questionnaire(See Table 2)
| What Conditions or Body Part Did You Utilize the H-Wave for? |
|---|
| If you were taking medication (for this condition) at the time you received your H-Wave, has H-Wave allowed you to decrease or eliminate the amount of medication taken? |
| If decreased, approximate by what percentage? |
| Has H-Wave allowed you to increase function or perform more activity than you could without it? If yes, please select all of the examples of things you are now able to do: No increased function; More family interaction; More housework; Walk further; Lift more; Greater ability to drive a vehicle; Sit longer; Sleep better; Stand longer; Other functions increased |
| Before using H-Wave, rate your average level of pain you were living with (0–10, 0-no pain, 10-extreme pain) |
| After using H-wave, rate your average level of pain you are living with (0–10, 0-no pain, 10-extreme pain) |
| How many times do you treat yourself per day? |
| How many days per week do you treat yourself? |
| How long is each treatment with the H-Wave? (Less than 30 min; 30–45 min; 45–60 min; 60+ min) |
3. Results
3.1. Case Presentations
3.1.1. Case One
3.1.2. Case Two
3.1.3. Case Three
3.1.4. Case Four
4. Statistical Analysis Result
5. Discussion
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dumas, E.O.; Pollack, G.M. Opioid Tolerance Development: A Pharmacokinetic/Pharmacodynamic Perspective. AAPS J. 2008, 10, 537–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kampman, K.; Jarvis, M. American Society of Addiction Medicine (ASAM) National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use. J. Addict. Med. 2015, 9, 358–367. [Google Scholar] [CrossRef]
- Blum, K.; Soni, D.; Badgaiyan, R.D.; Baron, D. Overcoming reward deficiency syndrome by the induction of “dopamine homeostasis” instead of opioids for addiction: Illusion or reality? J. Osteopath Med. 2022, 122, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Hill, E.; Han, D.; Dumouchel, P.; Dehak, N.; Quatieri, T.; Moehs, C.; Oscar-Berman, M.; Giordano, J.; Simpatico, T.; Barh, D.; et al. Long term Suboxone™ emotional reactivity as measured by automatic detection in speech. PLoS ONE 2013, 8, e69043. [Google Scholar] [CrossRef]
- Blum, K.; Baron, D.; McLaughlin Thanos, P.K.; Giordano, J.; Dennen Ceccanti, M.; Badgaiyan, R.D. Summary Document Research on RDS Anti-addiction Modeling: Annotated Bibliography. J. Syst. Integr. Neurosci. 2022, 8, 2–35. [Google Scholar] [CrossRef]
- Blum, K.; Dennen, C.A.; Elman, I.; Bowirrat, A.; Thanos, P.K.; Badgaiyan, R.D.; Downs, B.W.; Bagchi, D.; Baron, D.; Braverman, E.R.; et al. Should Reward Deficiency Syndrome (RDS) Be Considered an Umbrella Disorder for Mental Illness and Associated Genetic and Epigenetic Induced Dysregulation of Brain Reward Circuitry? J. Pers. Med. 2022, 12, 1719. [Google Scholar] [CrossRef]
- Blum, K.; McLaughlin, T.; Bowirrat, A.; Modestino, E.J.; Baron, D.; Gomez, L.L.; Ceccanti, M.; Braverman, E.R.; Thanos, P.K.; Cadet, J.L.; et al. Reward Deficiency Syndrome (RDS) Surprisingly Is Evolutionary and Found Everywhere: Is It “Blowin’ in the Wind”? J. Pers. Med. 2022, 12, 321. [Google Scholar] [CrossRef]
- Blum, K.; Bowirrat, A.; Braverman, E.R.; Baron, D.; Cadet, J.L.; Kazmi, S.; Elman, I.; Thanos, P.K.; Badgaiyan, R.D.; Downs, W.B.; et al. Reward Deficiency Syndrome (RDS): A Cytoarchitectural Common Neurobiological Trait of All Addictions. Int. J. Environ. Res. Public Health 2021, 18, 11529. [Google Scholar] [CrossRef]
- Kótyuk, E.; Urbán, R.; Hende, B.; Richman, M.; Magi, A.; Király, O.; Barta, C.; Griffiths, M.D.; Potenza, M.N.; Badgaiyan, R.D.; et al. Development and validation of the Reward Deficiency Syndrome Questionnaire (RDSQ-29). J. Psychopharmacol. 2022, 36, 409–422. [Google Scholar] [CrossRef]
- Braverman, E.R.; Dennen, C.A.; Gold, M.S.; Bowirrat, A.; Gupta, A.; Baron, D.; Roy, A.K.; Smith, D.E.; Cadet, J.L.; Blum, K. Proposing a “Brain Health Checkup (BHC)” as a Global Potential “Standard of Care” to Overcome Reward Dysregulation in Primary Care Medicine: Coupling Genetic Risk Testing and Induction of “Dopamine Homeostasis”. Int. J. Environ. Res. Public Health 2022, 19, 5480. [Google Scholar] [CrossRef]
- Nami, M.; Thatcher, R.; Kashou, N.; Lopes, D.; Lobo, M.; Bolanos, J.F.; Morris, K.; Sadri, M.; Bustos, T.; Sanchez, G.E.; et al. A Proposed Brain-, Spine-, and Mental- Health Screening Methodology (NEUROSCREEN) for Healthcare Systems: Position of the Society for Brain Mapping and Therapeutics. J. Alzheimers Dis. 2022, 86, 21–42. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, B.; Rossi, G. Combining Ketamine, Brain Stimulation (rTMS) and Mindfulness Therapy (TIMBER) for Opioid Addiction. Cureus 2020, 12, e11798. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, J.J., 3rd; Hanlon, C.A.; Marshalek, P.J.; Rezai, A.R.; Krinke, L. Transcranial magnetic stimulation, deep brain stimulation, and other forms of neuromodulation for substance use disorders: Review of modalities and implications for treatment. J. Neurol. Sci. 2020, 418, 117149. [Google Scholar] [CrossRef]
- Lent, M.R.; Callahan, H.R.; Womer, P.; Mullen, P.M.; Shook, C.B.; DiTomasso, R.A.; Felgoise, S.H.; Festinger, D.S. A mental health professional survey of cognitive-behavioral therapy for the treatment of opioid use disorder. J. Clin. Psychol. 2021, 77, 1607–1613. [Google Scholar] [CrossRef] [PubMed]
- Alexander, K.; Kronk, R.; Sekula, K.; Short, V.; Abatemarco, D. Implementation of a Mindfulness Intervention for Women in Treatment for Opioid Use Disorder and Its Effects on Depression Symptoms. Issues Ment. Health Nurs. 2019, 40, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Schiffer, F. Unilateral transcranial photobiomodulation for opioid addiction in clinical practice: A clinical overview and case series. J. Psychiatr. Res. 2021, 133, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Brubaker, A.; Meghani, S.H.; Bruner, D.W.; Yeager, K.A. Spirituality and Quality of Life in Black Patients With Cancer Pain. J. Pain Symptom Manag. 2018, 56, 390–398. [Google Scholar] [CrossRef] [Green Version]
- Piacentine, L.B. Spirituality, religiosity, depression, anxiety, and drug-use consequences during methadone maintenance therapy. West. J. Nurs. Res. 2013, 35, 795–814. [Google Scholar] [CrossRef] [Green Version]
- Acheampong, A.B.; Lasopa, S.; Striley, C.W.; Cottler, L.B. Gender Differences in the Association Between Religion/Spirituality and Simultaneous Polysubstance Use (SPU). J. Relig. Health 2016, 55, 1574–1584. [Google Scholar] [CrossRef]
- Conner, B.T.; Anglin, M.D.; Annon, J.; Longshore, D. Effect of religiosity and spirituality on drug treatment outcomes. J. Behav. Health Serv. Res. 2009, 36, 189–198. [Google Scholar] [CrossRef]
- Heinz, A.J.; Disney, E.R.; Epstein, D.H.; Glezen, L.A.; Clark, P.I.; Preston, K.L. A focus-group study on spirituality and substance-user treatment. Subst. Use Misuse 2010, 45, 134–153. [Google Scholar] [CrossRef]
- Galanter, M.; Dermatis, H.; Bunt, G.; Williams, C.; Trujillo, M.; Steinke, P. Assessment of spirituality and its relevance to addiction treatment. J. Subst. Abus. Treat. 2007, 33, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Mallik, D.; Bowen, S.; Yang, Y.; Perkins, R.; Sandoz, E.K. Raja yoga meditation and medication-assisted treatment for relapse prevention: A pilot study. J. Subst. Abus. Treat. 2019, 96, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Noormohammadi, M.R.; Nikfarjam, M.; Deris, F.; Parvin, N. Spiritual Well-Being and Associated Factors with Relapse in Opioid Addicts. J. Clin. Diagn. Res. 2017, 11, VC07–VC10. [Google Scholar] [CrossRef] [PubMed]
- Alali, A.; Behrouzi, M.K.; Salari, N.; Bazrafshan, M.R.; Rahmati, M. The Effectiveness of Group Spiritual Intervention on Self-esteem and Happiness Among Men Undergoing Methadone Maintenance Treatment. Curr. Drug Res. Rev. 2019, 11, 67–72. [Google Scholar] [CrossRef]
- Avants, S.K.; Marcotte, D.; Arnold, R.; Margolin, A. Spiritual beliefs, world assumptions, and HIV risk behavior among heroin and cocaine users. Psychol. Addict. Behav. 2003, 17, 159–162. [Google Scholar] [CrossRef] [PubMed]
- DiScala, S.L.; Faley, B.; Lewis, V.; Vartan, C.M.; Silverman, M. Spiritual Healing in a Hospice Veteran Led to a Successful Opioid Taper: A Case Report. J. Pain Palliat. Care Pharmacother. 2021, 35, 117–122. [Google Scholar] [CrossRef]
- Roy, A.K.; Bowirrat, A.; Smith, D.E.; Braverman, E.R.; Jalali, R.; Badgaiyan, R.D.; Baron, D.; Llanos-Gomez, L.; Barh, D.; Blum, K. Neurobiology and Spirituality in Addiction Recovery. Acta Sci. Neurol. 2021, 4, 64–71. [Google Scholar]
- Schoenthaler, S.J.; Blum, K.; Braverman, E.R.; Giordano, J.; Thompson, B.; Oscar-Berman, M.; Badgaiyan, R.D.; Madigan, M.A.; Dushaj, K.; Li, M.; et al. NIDA-Drug Addiction Treatment Outcome Study (DATOS) Relapse as a Function of Spirituality/Religiosity. J. Reward. Defic. Syndr. 2015, 1, 36–45. [Google Scholar] [CrossRef] [Green Version]
- Newberg, A.B. The neuroscientific study of spiritual practices. Front. Psychol. 2014, 5, 215. [Google Scholar] [CrossRef]
- Pergolizzi, J.V.; Magnusson, P.; LeQuang, J.A.; Breve, F.; Taylor, R.; Wollmuth, C.; Varrassi, G. Can NSAIDs and Acetaminophen Effectively Replace Opioid Treatment Options for Acute Pain? Expert Opin. Pharmacother. 2021, 22, 1119–1126. [Google Scholar] [CrossRef]
- Bajaj, A.; Blum, K.; Bowirrat, A.; Gupta, A.; Baron, D.; Fugel, D.; Nicholson, A.; Fitch, T.; Downs, B.W.; Bagchi, D.; et al. DNA Directed Pro-Dopamine Regulation Coupling Subluxation Repair, H-Wave® and Other Neurobiologically Based Modalities to Address Complexities of Chronic Pain in a Female Diagnosed with Reward Deficiency Syndrome (RDS): Emergence of Induction of “Dopamine Homeostasis” in the Face of the Opioid Crisis. J. Pers. Med. 2022, 12, 1416. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Bowirrat, A.; Gomez, L.L.; Baron, D.; Elman, I.; Giordano, J.; Jalali, R.; Badgaiyan, R.D.; Modestino, E.J.; Gold, M.S.; et al. Hypothesizing in the Face of the Opioid Crisis Coupling Genetic Addiction Risk Severity (GARS) Testing with Electrotherapeutic Nonopioid Modalities Such as H-Wave Could Attenuate Both Pain and Hedonic Addictive Behaviors. Int. J. Environ. Res. Public Health 2022, 19, 552. [Google Scholar] [CrossRef]
- Williamson, T.K.; Rodriguez, H.C.; Gonzaba, A.; Poddar, N.; Norwood, S.M.; Gupta, A. H-Wave® Device Stimulation: A Critical Review. J. Pers. Med. 2021, 11, 1134. [Google Scholar] [CrossRef]
- Williamson, T.K.; Rodriguez, H.C.; Han, D.; Norwood, S.M.; Gupta, A. Job-Related Performance and Quality of Life Benefits in First Responders Given Access to H-Wave® Device Stimulation: A Retrospective Cohort Study. J. Pers. Med. 2022, 12, 1674. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.; Chen, A.L.; Chen, T.J.; Prihoda, T.J.; Schoolfield, J.; DiNubile, N.; Waite, R.L.; Arcuri, V.; Kerner, M.; Braverman, E.R.; et al. The H-Wave® device is an effective and safe non-pharmacological analgesic for chronic pain: A meta-analysis. Adv. Ther. 2008, 25, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Van Der Schier, R.; Roozekrans, M.; Van Velzen, M.; Dahan, A.; Niesters, M. Opioid-induced respiratory depression: Reversal by non-opioid drugs. F1000Prime Rep. 2014, 6, 79. [Google Scholar] [CrossRef] [Green Version]
- Blum, K.; Ho, C.-K.; Chen, A.L.; Fulton, M.; Fulton, B.; Westcott, W.L.; Reinl, G.; Braverman, E.R.; DiNubile, N.; Chen, T.J. The H-Wave® Device Induces NO Dependent Augmented Microcirculation and Angiogenesis, Providing Both Analgesia and Tissue Healing in Sports Injuries. Physician Sportsmed. 2008, 36, 103–114. [Google Scholar] [CrossRef]
- Kumar, D.; Marshall, H.J. Diabetic Peripheral Neuropathy: Amelioration of Pain With Transcutaneous Electrostimulation. Diabetes Care 1997, 20, 1702–1705. [Google Scholar] [CrossRef]
- Kumar, D.; Alvaro, M.S.; Julka, I.S.; Marshall, H.J. Diabetic Peripheral Neuropathy: Effectiveness of electrotherapy and amitriptyline for symptomatic relief. Diabetes Care 1998, 21, 1322–1325. [Google Scholar] [CrossRef]
- Julka, I.S.; Alvaro, M.; Kumar, D. Beneficial effects of electrical stimulation on neuropathic symptoms in diabetes patients. J. Foot Ankle Surg. 1998, 37, 191–194. [Google Scholar] [CrossRef]
- Blum, K.; Oscar-Berman, M.; Blum, S.H.; Madigan, M.A.; Waite, R.L.; McLaughlin, T.; Barh, D. Can Genetic Testing Coupled with Enhanced Dopaminergic Activation Reduce Recidivism Rates in the Workers Compensation Legacy Cases? J. Alcohol. Drug Depend. 2014, 2, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, J.B.; White, A.G.; Birnbaum, H.G.; Schiller, M.; Brown, D.A.; Roland, C. A model to identify patients at risk for prescription opioid abuse, dependence, and misuse. Pain Med. 2012, 13, 1162–1173. [Google Scholar] [CrossRef] [Green Version]
- Chen, A.L.; Chen, T.J.; Waite, R.L.; Reinking, J.; Tung, H.L.; Rhoades, P.; Downs, B.W.; Braverman, E.; Braverman, D.; Kerner, M.; et al. Hypothesizing that brain reward circuitry genes are genetic antecedents of pain sensitivity and critical diagnostic and pharmacogenomic treatment targets for chronic pain conditions. Med. Hypotheses. 2009, 72, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Borsook, D.; Linnman, C.; Faria, V.; Strassman, A.M.; Becerra, L.; Elman, I. Reward deficiency and anti-reward in pain chronification. Neurosci. Biobehav. Rev. 2016, 68, 282–297. [Google Scholar] [CrossRef]
- Elman, I.; Borsook, D. Common Brain Mechanisms of Chronic Pain and Addiction. Neuron 2016, 89, 11–36. [Google Scholar] [CrossRef] [Green Version]
- Elman, I.; Borsook, D.; Volkow, N.D. Pain and suicidality: Insights from reward and addiction neuroscience. Prog. Neurobiol. 2013, 109, 1–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsook, D.; Youssef, A.M.; Simons, L.; Elman, I.; Eccleston, C. When pain gets stuck: The evolution of pain chronification and treatment resistance. Pain 2018, 159, 2421–2436. [Google Scholar] [CrossRef] [PubMed]
- Borsook, D.; Edwards, R.; Elman, I.; Becerra, L.; Levine, J. Pain and analgesia: The value of salience circuits. Prog. Neurobiol. 2013, 104, 93–105. [Google Scholar] [CrossRef] [Green Version]
- Borsook, D.; Becerra, L.; Carlezon WAJr Shaw, M.; Renshaw, P.; Elman, I.; Levine, J. Reward-aversion circuitry in analgesia and pain: Implications for psychiatric disorders. Eur. J. Pain 2007, 11, 7–20. [Google Scholar] [CrossRef]
- Che, X.; Cash, R.F.H.; Luo, X.; Luo, H.; Lu, X.; Xu, F.; Zang, Y.F.; Fitzgerald, P.B.; Fitzgibbon, B.M. High-frequency rTMS over the dorsolateral prefrontal cortex on chronic and provoked pain: A systematic review and meta-analysis. Brain Stimul. 2021, 14, 1135–1146. [Google Scholar] [CrossRef] [PubMed]
- Trinh, A.; Williamson, T.K.; Han, D.; Hazlewood, J.E.; Norwood, S.M.; Gupta, A. Clinical and Quality of Life Benefits for End-Stage Workers’ Compensation Chronic Pain Claimants following H-Wave® Device Stimulation: A Retrospective Observational Study with Mean 2-Year Follow-Up. J. Clin. Med. 2023, 12, 1148. [Google Scholar] [CrossRef] [PubMed]






| Question | Case 1 | Case 2 | Case 3 | Case 4 |
|---|---|---|---|---|
| What conditions or body part did you utilize the H-Wave for? | Knee | Achilles | Knee | Knee |
| If you were taking medication (for this condition) at the you received your H-Wave, has H-Wave allowed you to decrease or eliminate the amount of medication taken? | No | No | Yes | Yes |
| If decreased, approximate by what percentage? | N/A | N/A | 100 | 75 |
| Has H-Wave allowed you to increase function or perform more activity than you could without it? If yes, please select all of the examples of things you are now able to do: | Yes | Yes | Yes | Yes |
| More family interaction | No | Yes | No | No |
| More housework | No | Yes | Yes | No |
| Walk further | Yes | Yes | Yes | Yes |
| Lift more | No | Yes | Yes | No |
| Greater ability to drive a vehicle | No | Yes | Yes | No |
| Sit longer | No | No | Yes | No |
| Sleep better | No | Yes | No | No |
| Stand longer | Yes | Yes | Yes | Yes |
| Other functions increased | N/A | N/A | N/A | Climb Stairs; Exercise; Balance |
| Before using H-Wave, rate your average level of pain you were living with (0–10, 0-no pain, 10-extreme pain) | 9 | 7 | 8 | 9 |
| After using H-Wave, rate your average level of pain you are living with (0–10, 0-no pain, 10-extreme pain) | 3 | 0 | 1 | 1 |
| How many times do you treat yourself per day? | 1 | 2 | 1 | 1 |
| How many days per week do you treat yourself? | 3 | 7 | 3 | 4 |
| How long is each treatment with the H-Wave? (Less than 30 min; 30–45 min; 45–60 min; 60+ min) | <30 | 30 | 30–45 | 30–45 |
| Current use of H-Wave | No | Yes | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajaj, A.; Han, D.; Elman, I.; Thanos, P.K.; Dennen, C.A.; Badgaiyan, R.D.; Bowirrat, A.; Barh, D.; Blum, K. Positive Clinical Outcomes for Severe Reported Pain Using Robust Non-Addictive Home Electrotherapy—A Case-Series. J. Pers. Med. 2023, 13, 336. https://doi.org/10.3390/jpm13020336
Bajaj A, Han D, Elman I, Thanos PK, Dennen CA, Badgaiyan RD, Bowirrat A, Barh D, Blum K. Positive Clinical Outcomes for Severe Reported Pain Using Robust Non-Addictive Home Electrotherapy—A Case-Series. Journal of Personalized Medicine. 2023; 13(2):336. https://doi.org/10.3390/jpm13020336
Chicago/Turabian StyleBajaj, Anish, David Han, Igor Elman, Panayotis K. Thanos, Catherine A. Dennen, Rajendra D. Badgaiyan, Abdalla Bowirrat, Debmalya Barh, and Kenneth Blum. 2023. "Positive Clinical Outcomes for Severe Reported Pain Using Robust Non-Addictive Home Electrotherapy—A Case-Series" Journal of Personalized Medicine 13, no. 2: 336. https://doi.org/10.3390/jpm13020336