
Reproducibility of Mesopic and Photopic Pupil Sizes in Myopic Children Using a Dedicated Pupillometer with Human-Assisted or Automated Reading
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Approvals
2.3. Examinations
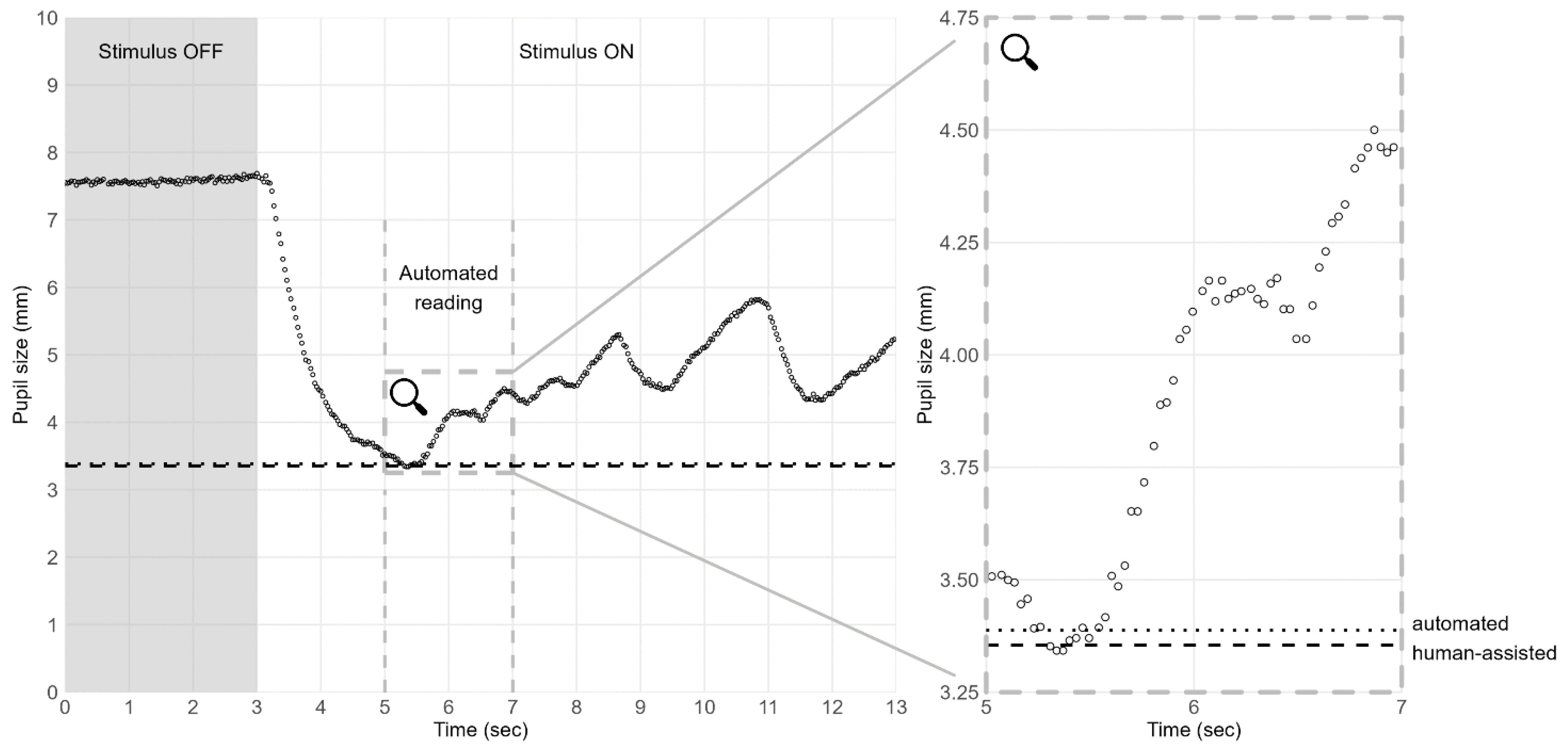
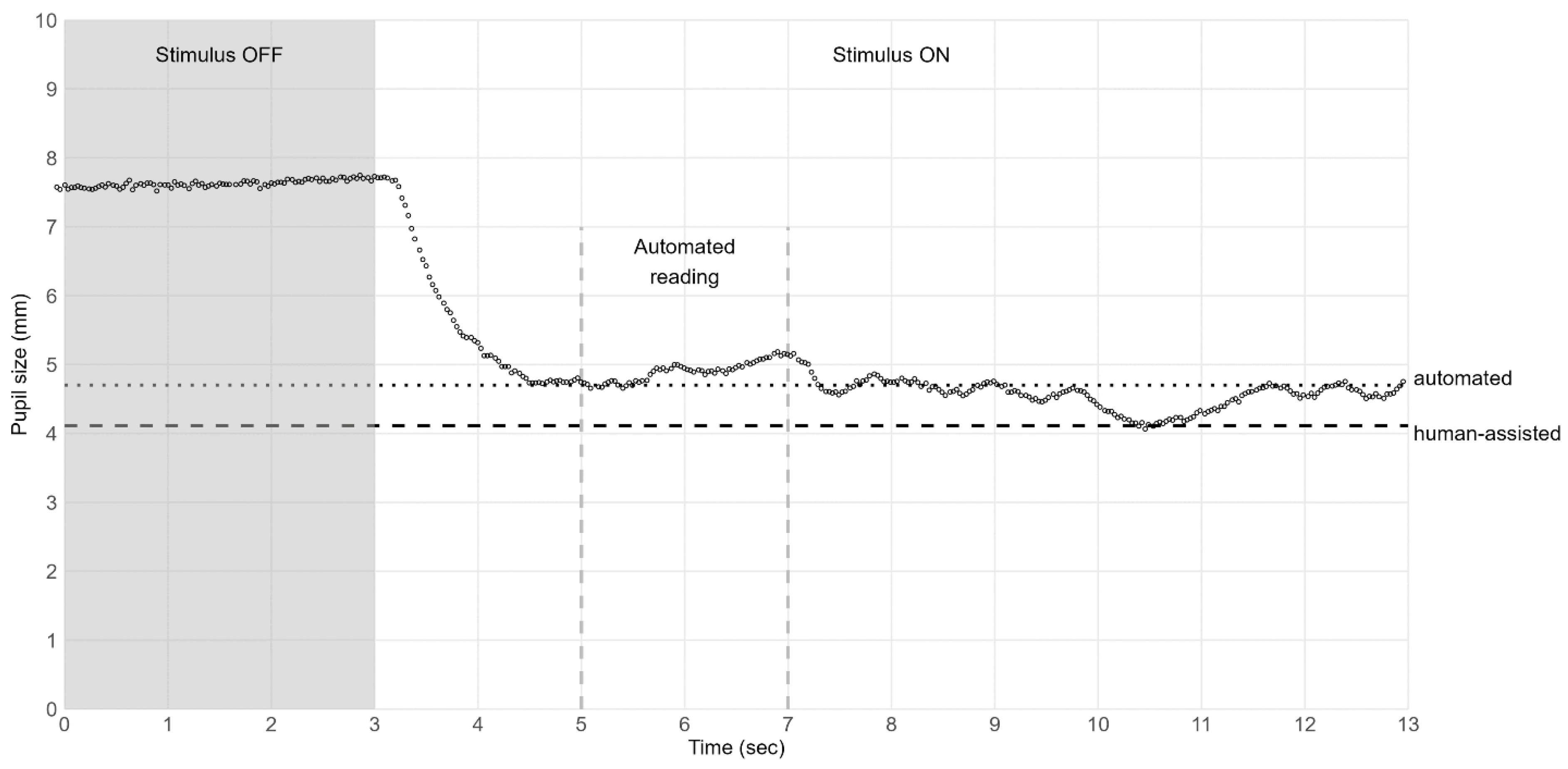
2.4. Automated Data Reading
2.5. Statistical Analysis
3. Results
3.1. Pupil Diameter
3.2. Reproducibility over Time
3.3. Reproducibility between Human-Assisted and Automated Readings
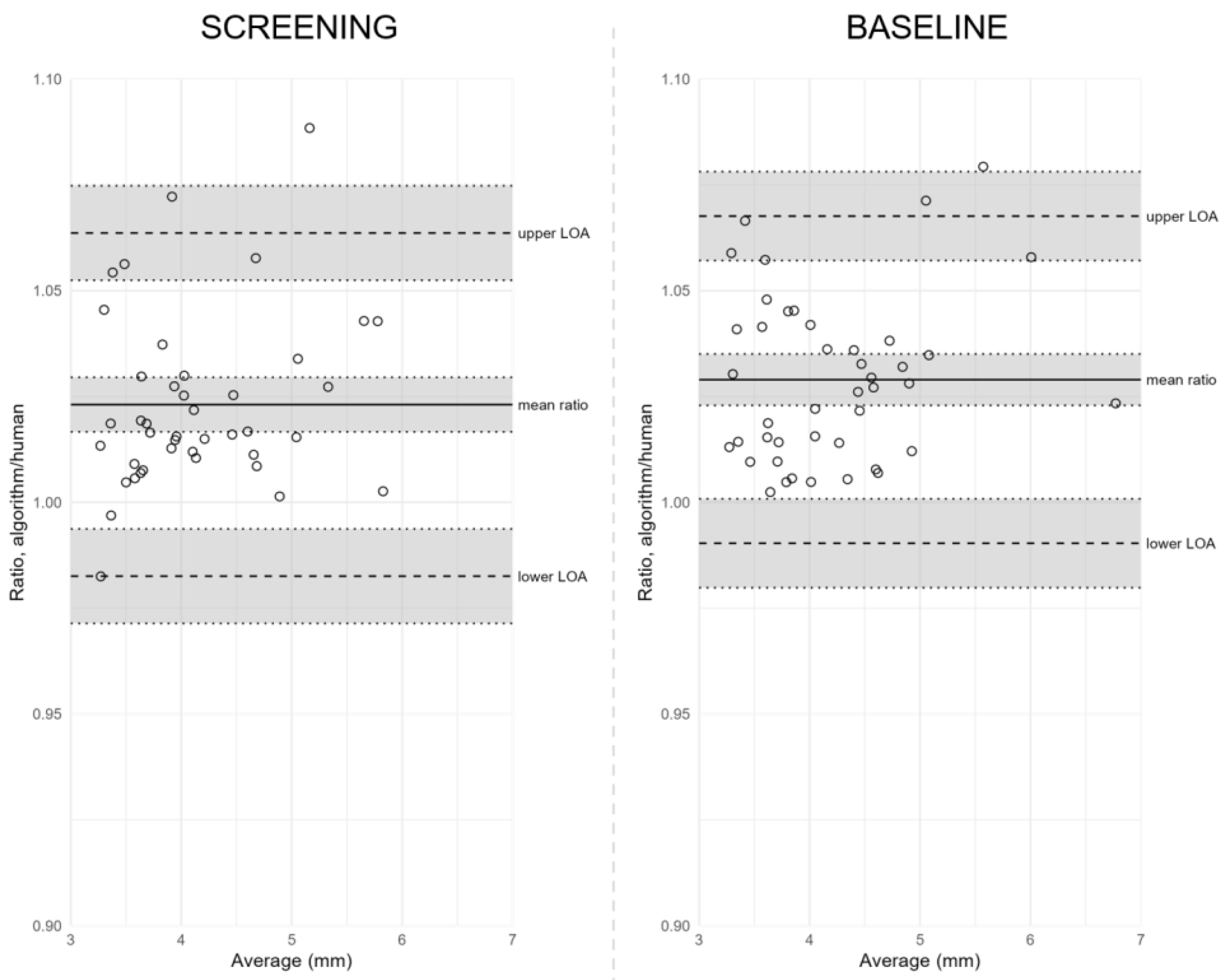
3.4. Using Ratios to Assess the Reproducibility between Human-Assisted and Automated Readings
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathôt, S. Pupillometry: Psychology, Physiology, and Function. J. Cogn. 2018, 1, 16. [Google Scholar] [CrossRef] [PubMed]
- Mathur, A.; Gehrmann, J.; Atchison, D.A. Influences of luminance and accommodation stimuli on pupil size and pupil center location. Investig. Opthalmology Vis. Sci. 2014, 55, 2166–2172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillon, M.; Dumbleton, K.; Theodoratos, P.; Gobbe, M.; Wooley, C.B.; Moody, K. The Effects of Age, Refractive Status, and Luminance on Pupil Size. Optom. Vis. Sci. 2016, 93, 1093–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, Q.; Ng, A.L.K.; Cheng, G.P.M.; Woo, V.C.P.; Cho, P. Repeatability of pupil size measurements with NIDEK OPD-Scan III in myopic children. Ophthalmic Physiol. Opt. 2021, 41, 431–436. [Google Scholar] [CrossRef]
- Kloosterman, N.A.; Meindertsma, T.; van Loon, A.M.; Lamme, V.A.F.; Bonneh, Y.S.; Donner, T.H. Pupil size tracks perceptual content and surprise. Eur. J. Neurosci. 2015, 41, 1068–1078. [Google Scholar] [CrossRef]
- Linke, S.J.; Baviera, J.; Munzer, G.; Fricke, O.H.; Richard, G.; Katz, T. Mesopic pupil size in a refractive surgery population (13,959 eyes). Optom. Vis. Sci. 2012, 89, 1156–1164. [Google Scholar] [CrossRef]
- Chua, W.H.; Balakrishnan, V.; Chan, Y.H.; Tong, L.; Ling, Y.; Quah, B.L.; Tan, D. Atropine for the Treatment of Childhood Myopia. Ophthalmology 2006, 113, 2285–2291. [Google Scholar] [CrossRef]
- Chia, A.; Lu, Q.S.; Tan, D. Five-Year Clinical Trial on Atropine for the Treatment of Myopia 2 Myopia Control with Atropine 0.01% Eyedrops. Ophthalmology 2016, 123, 391–399. [Google Scholar] [CrossRef]
- Yam, J.C.; Zhang, X.J.; Zhang, Y.; Wang, Y.M.; Tang, S.M.; Li, F.F.; Kam, K.W.; Ko, S.T.; Yip, B.H.K.; Young, A.L.; et al. Three-Year Clinical Trial of Low-Concentration Atropine for Myopia Progression (LAMP) Study: Continued versus Washout: Phase 3 Report. Ophthalmology 2022, 129, 308–321. [Google Scholar] [CrossRef]
- Mcbrien, N.A.; Stell, W.K.; Carr, B. How does atropine exert its anti-myopia effects? Ophthalmic Physiol. Opt. 2013, 33, 373–378. [Google Scholar] [CrossRef]
- Wu, P.-C.; Chuang, M.-N.; Choi, J.; Chen, H.; Wu, G.; Ohno-Matsui, K.; Jonas, J.B.; Cheung, C.M.G. Update in myopia and treatment strategy of atropine use in myopia control. Eye 2019, 33, 3–13. [Google Scholar] [CrossRef] [Green Version]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [Green Version]
- Morgan, I.G.; Ohno-Matsui, K.; Saw, S.M. Myopia. Lancet 2012, 379, 1739–1748. [Google Scholar] [CrossRef]
- Saw, S.M.; Gazzard, G.; Shin-Yen, E.C.; Chua, W.H. Myopia and associated pathological complications. Ophthalmic Physiol. Opt. 2005, 25, 381–391. [Google Scholar] [CrossRef]
- Ikuno, Y. Overview of the complications of high myopia. Retina 2017, 37, 2347–2351. [Google Scholar] [CrossRef]
- Jonas, J.B.; Ang, M.; Cho, P.; Guggenheim, J.A.; He, M.G.; Jong, M.; Logan, N.S.; Liu, M.; Morgan, I.; Ohno-Matsui, K.; et al. IMI Prevention of Myopia and Its Progression. Investig. Ophthalmol. Vis. Sci. 2021, 62, 6. [Google Scholar] [CrossRef]
- Chia, A.; Chua, W.H.; Cheung, Y.B.; Wong, W.L.; Lingham, A.; Fong, A.; Tan, D. Atropine for the treatment of childhood Myopia: Safety and efficacy of 0.5%, 0.1%, and 0.01% doses (Atropine for the Treatment of Myopia 2). Ophthalmology 2012, 119, 347–354. [Google Scholar] [CrossRef]
- Yam, J.C.; Jiang, Y.; Tang, S.M.; Law, A.K.P.; Chan, J.J.; Wong, E.; Ko, S.T.; Young, A.L.; Tham, C.C.; Chen, L.J.; et al. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology 2019, 126, 113–124. [Google Scholar] [CrossRef]
- Tan, Q.; Ng, A.L.; Choy, B.N.; Cheng, G.P.; Woo, V.C.; Cho, P. One-year results of 0.01% atropine with orthokeratology (AOK) study: A randomised clinical trial. Ophthalmic Physiol. Opt. 2020, 40, 557–566. [Google Scholar] [CrossRef]
- Mckinney, W. Data Structures for Statistical Computing in Python. In Proceedings of the 9th Python in Science Conference, Austin, TX, USA, 28 June–3 July 2010; van der Walt, S., Millman, J., Eds.; The National Science Foundation: Alexandria, VA, USA, 2010. [Google Scholar]
- Harris, C.R.; Millman, K.J.; van der Walt, S.J.; Gommers, R.; Virtanen, P.; Cournapeau, D.; Wieser, E.; Taylor, J.; Berg, S.; Smith, N.J.; et al. Array programming with NumPy. Nature 2020, 585, 357–362. [Google Scholar] [CrossRef]
- Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; Bright, J.; et al. SciPy 1.0: Fundamental algorithms for scientific computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, L.; Gather, U. The Identification of Multiple Outliers. J. Am. Stat. Assoc. 1993, 88, 782–792. [Google Scholar] [CrossRef]
- Pearson, R.K.; Neuvo, Y.; Astola, J.; Gabbouj, M. Generalized Hampel Filters. EURASIP J. Adv. Signal Process. 2016, 2016, 87. [Google Scholar] [CrossRef] [Green Version]
- Rousseeuw, P.J.; Croux, C. Alternatives to the Median Absolute Deviation. J. Am. Stat. Assoc. 1993, 88, 1273. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Use R! Springer International Publishing: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Wachler, B.S.; Krueger, R.R. Agreement and repeatability of infrared pupillometry and the comparison method. Ophthalmology 1999, 106, 319–323. [Google Scholar] [CrossRef]
- Kohnen, T.; Terzi, E.; Bühren, J.; Kohnen, E.M.; Ackermann, H. Comparison of a digital and a handheld infrared pupillometer for determining scotopic pupil diameter. J. Cataract Refract. Surg. 2003, 29, 112–117. [Google Scholar] [CrossRef]
- Schnitzler, E.M.; Baumeister, M.; Kohnen, T. Scotopic measurement of normal pupils: Colvard versus Video Vision Analyzer infrared pupillometer. J. Cataract Refract. Surg. 2000, 26, 859–866. [Google Scholar] [CrossRef]
- Spadea, L.; Giammaria, D.; Ferrante, R.; Balestrazzi, E. Pre-excimer laser and post-excimer laser refractive surgery measurements of scotopic pupil diameter using 2 pupillometers. Ophthalmology 2005, 112, 1003–1008. [Google Scholar] [CrossRef]
- Bergamin, O.; Kardon, R.H. Greater pupillary escape differentiates central from peripheral visual field loss. Ophthalmology 2002, 109, 771–780. [Google Scholar] [CrossRef]
- Kelbsch, C.; Strasser, T.; Chen, Y.; Feigl, B.; Gamlin, P.D.; Kardon, R.; Peters, T.; Roecklein, K.A.; Steinhauer, S.R.; Szabadi, E.; et al. Standards in pupillography. Front. Neurol. 2019, 10, 129. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Screening | Baseline | |||
|---|---|---|---|---|
| Reading Method | Mesopic | Photopic | Mesopic | Photopic |
| Human-assisted, mm | 4.12 (0.70) | 2.73 (0.29) | 4.14 (0.74) | 2.72 (0.28) |
| Automated, mm | 4.24 (0.76) | 2.76 (0.30) | 4.26 (0.78) | 2.76 (0.29) † |
| N | Mean Difference (95% CI) | Limits of Agreement (95% CI) | Coefficient | Correlation between Averages and Differences | |||
|---|---|---|---|---|---|---|---|
| Comparisons | Bias (mm) | Lower LOA (mm) | Upper LOA (mm) | 1.96 × SD (mm) | Pearson’s r p Value | ||
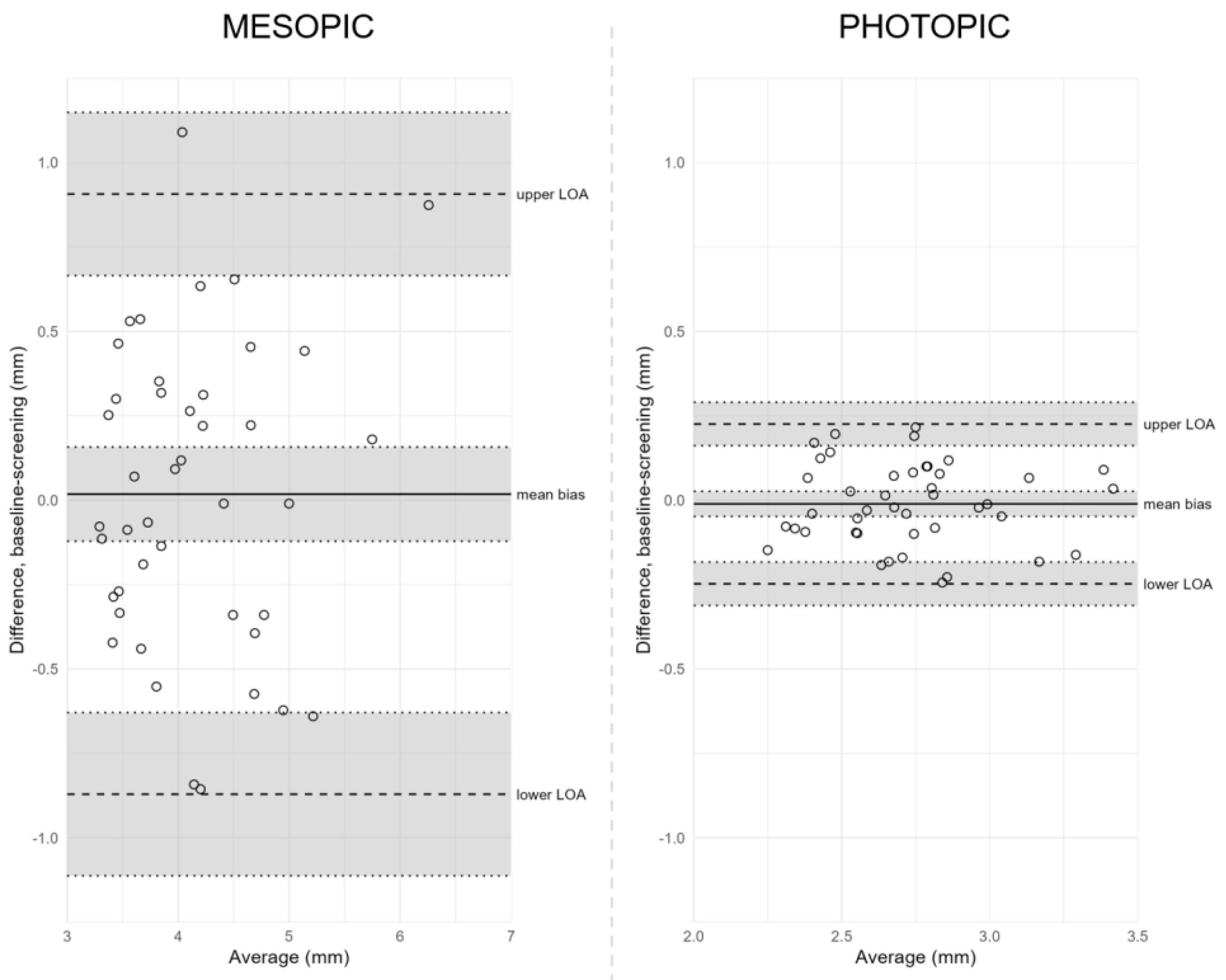
| MESOPIC | Between Visits | ||||||
| Screening vs. Baseline | 43 | 0.02 (−0.12 to 0.16) | −0.87 (−1.11 to −0.63) | 0.91 (0.67 to 1.15) | 0.89 | r = −0.088 p = 0.58 | |
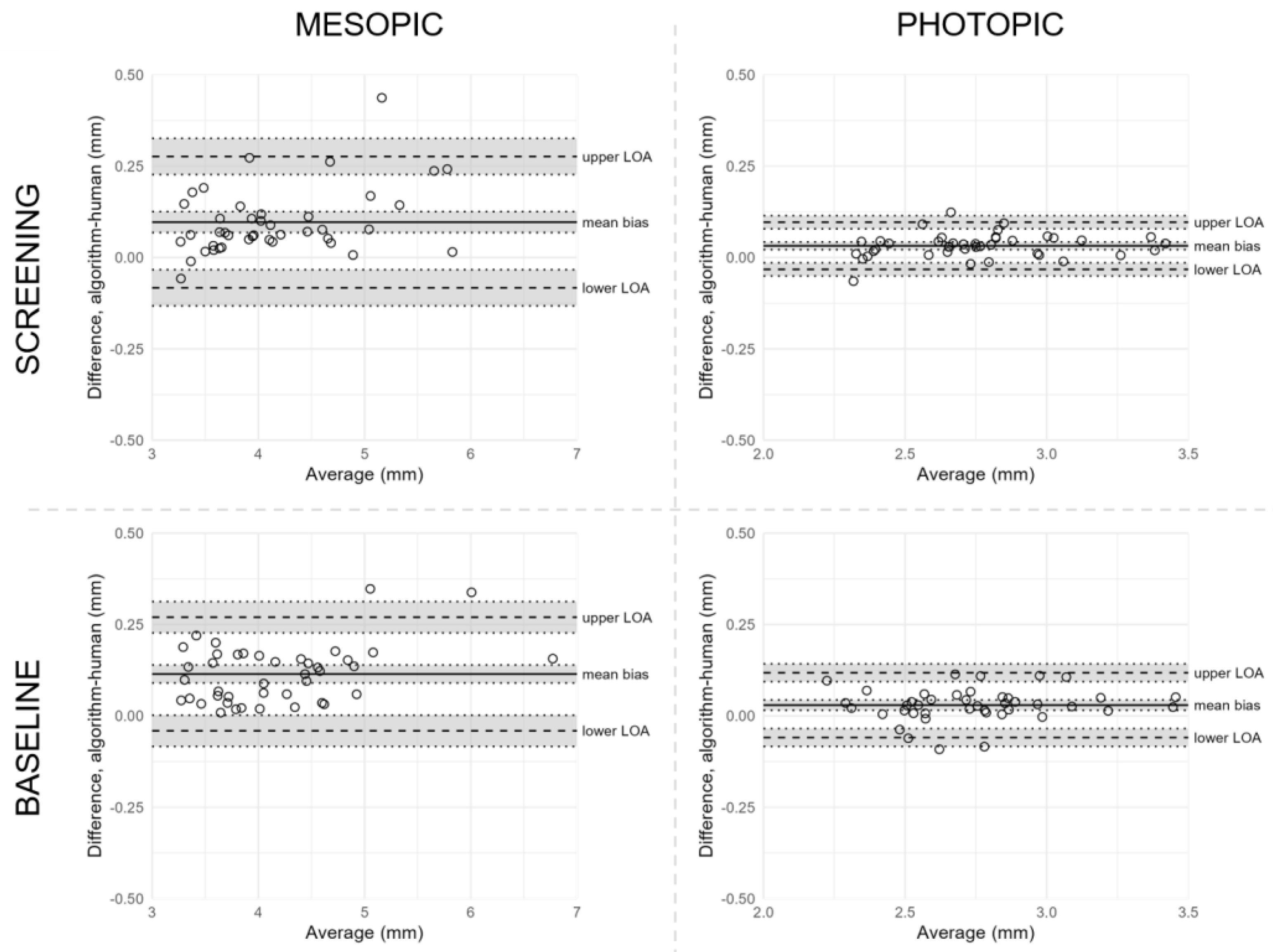
| Between Reading Methods | |||||||
| Screening | |||||||
| All | 43 | 0.11 (0.07 to 0.15) | −0.14 (−0.21 to −0.07) | 0.36 (0.29 to 0.43) | 0.25 | r = 0.48 p = 0.0037 | |
| Outlier(s) excluded | 42 | 0.10 (0.07 to 0.13) | −0.08 (−0.13 to −0.03) | 0.28 (0.23 to 0.33) | 0.18 | r = 0.39 p = 0.011 | |
| Baseline | |||||||
| All | 43 | 0.12 (0.09 to 0.15) | −0.06 (−0.11 to −0.01) | 0.30 (0.25 to 0.35) | 0.18 | r = 0.45 p = 0.0022 | |
| Outlier(s) excluded | 42 | 0.11 (0.09 to 0.14) | −0.04 (−0.08 to 0.00) | 0.27 (0.23 to 0.31) | 0.15 | r = 0.38 p = 0.014 | |
| PHOTOPIC | Between Visits | ||||||
| Screening vs. Baseline | 43 | −0.01 (−0.05 to 0.03) | −0.25 (−0.31 to −0.18) | 0.23 (0.16 to 0.29) | 0.24 | r = −0.035 p = 0.82 | |
| Between Reading Methods | |||||||
| Screening | |||||||
| All | 43 | 0.03 (0.01 to 0.05) | −0.09 (−0.12 to −0.05) | 0.15 (0.12 to 0.18) | 0.12 | r = 0.27 p = 0.079 | |
| Outlier(s) excluded | 41 | 0.03 (0.02 to 0.04) | −0.03 (−0.05 to −0.01) | 0.10 (0.08 to 0.11) | 0.06 | r = 0.16 p = 0.31 | |
| Baseline | 42 † | 0.03 (0.02 to 0.04) | −0.06 (−0.08 to −0.03) | 0.12 (0.09 to 0.14) | 0.09 | r = 0.11 p = 0.47 | |
| N | Mean Ratio (95% CI) | Limits of Agreement (95% CI) | Coefficient | Correlation Between Ratios and Differences | |||
|---|---|---|---|---|---|---|---|
| Comparisons | Lower LOA | Upper LOA | 1.96 × SD | Pearson’s r p Value | |||
| MESOPIC | Between Reading Methods | ||||||
| Screening | |||||||
| All | 43 | 1.026 (1.017 to 1.034) | 0.973 (0.958 to 0.987) | 1.079 (1.065 to 1.093) | 0.053 | r = 0.31 p = 0.047 | |
| Outlier(s) excluded | 42 | 1.023 (1.017 to 1.030) | 0.983 (0.971 to 0.994) | 1.064 (1.052 to 1.075) | 0.041 | r = 0.21 p = 0.19 | |
| Baseline | |||||||
| All | 43 | 1.029 (1.023 to 1.035) | 0.990 (0.980 to 1.001) | 1.068 (1.057 to 1.078) | 0.039 | r = 0.18 p = 0.25 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hvid-Hansen, A.; Bækgaard, P.; Jacobsen, N.; Hjortdal, J.; Møller, F.; Kessel, L. Reproducibility of Mesopic and Photopic Pupil Sizes in Myopic Children Using a Dedicated Pupillometer with Human-Assisted or Automated Reading. J. Pers. Med. 2023, 13, 273. https://doi.org/10.3390/jpm13020273
Hvid-Hansen A, Bækgaard P, Jacobsen N, Hjortdal J, Møller F, Kessel L. Reproducibility of Mesopic and Photopic Pupil Sizes in Myopic Children Using a Dedicated Pupillometer with Human-Assisted or Automated Reading. Journal of Personalized Medicine. 2023; 13(2):273. https://doi.org/10.3390/jpm13020273
Chicago/Turabian StyleHvid-Hansen, Anders, Per Bækgaard, Nina Jacobsen, Jesper Hjortdal, Flemming Møller, and Line Kessel. 2023. "Reproducibility of Mesopic and Photopic Pupil Sizes in Myopic Children Using a Dedicated Pupillometer with Human-Assisted or Automated Reading" Journal of Personalized Medicine 13, no. 2: 273. https://doi.org/10.3390/jpm13020273