
Construction of Tongue Image-Based Machine Learning Model for Screening Patients with Gastric Precancerous Lesions

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrollment, and Data Collection
2.2. Gastroscopy and Histological Examination
2.3. Data Pre-Processing and Data Structuring
2.4. PLGC Screening Model Construction
2.5. Statistical Analysis
3. Results
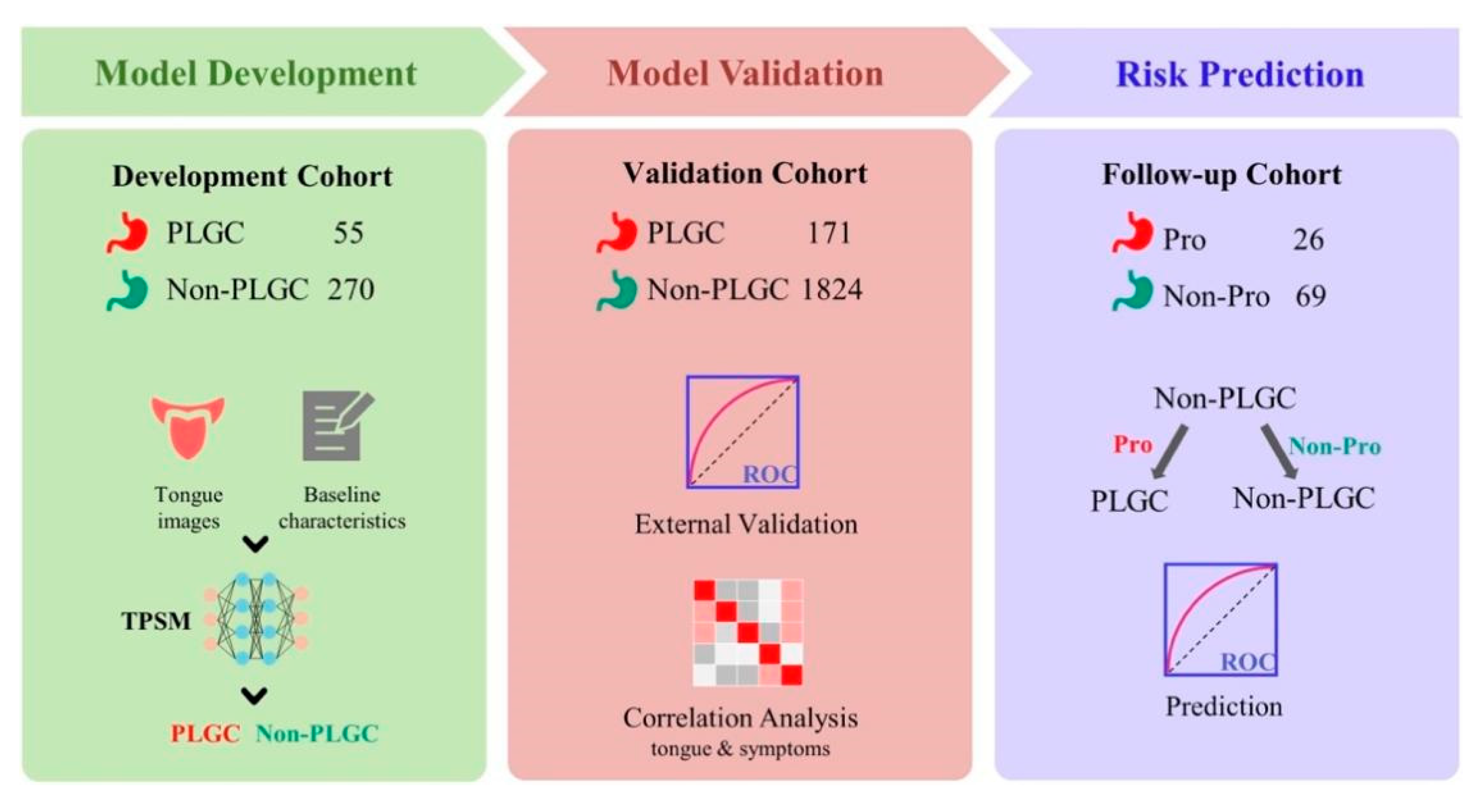
3.1. The Overall Design of Our Study
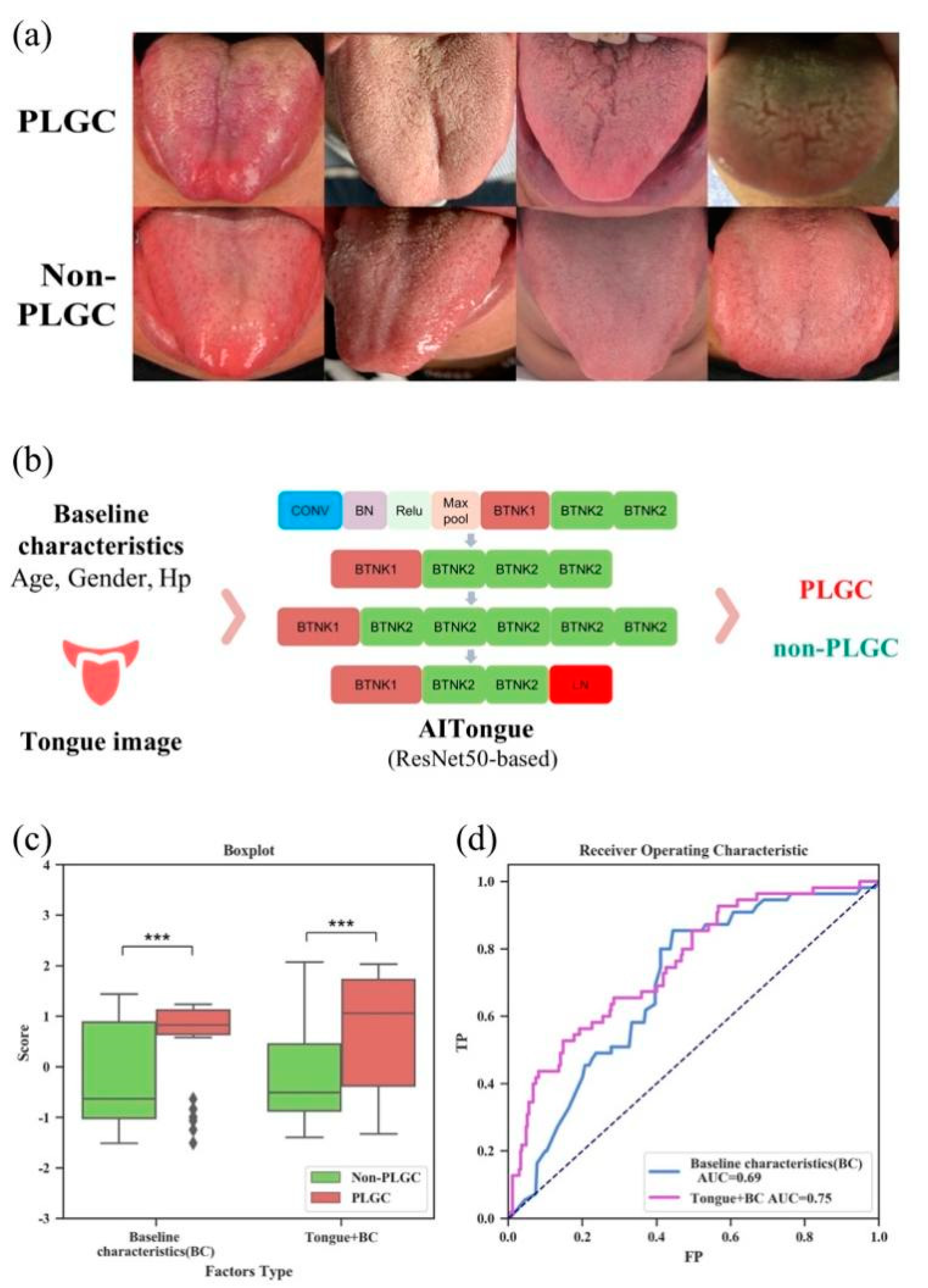
3.2. Construction of AITongue Model with Integrating Tongue Image Characteristics
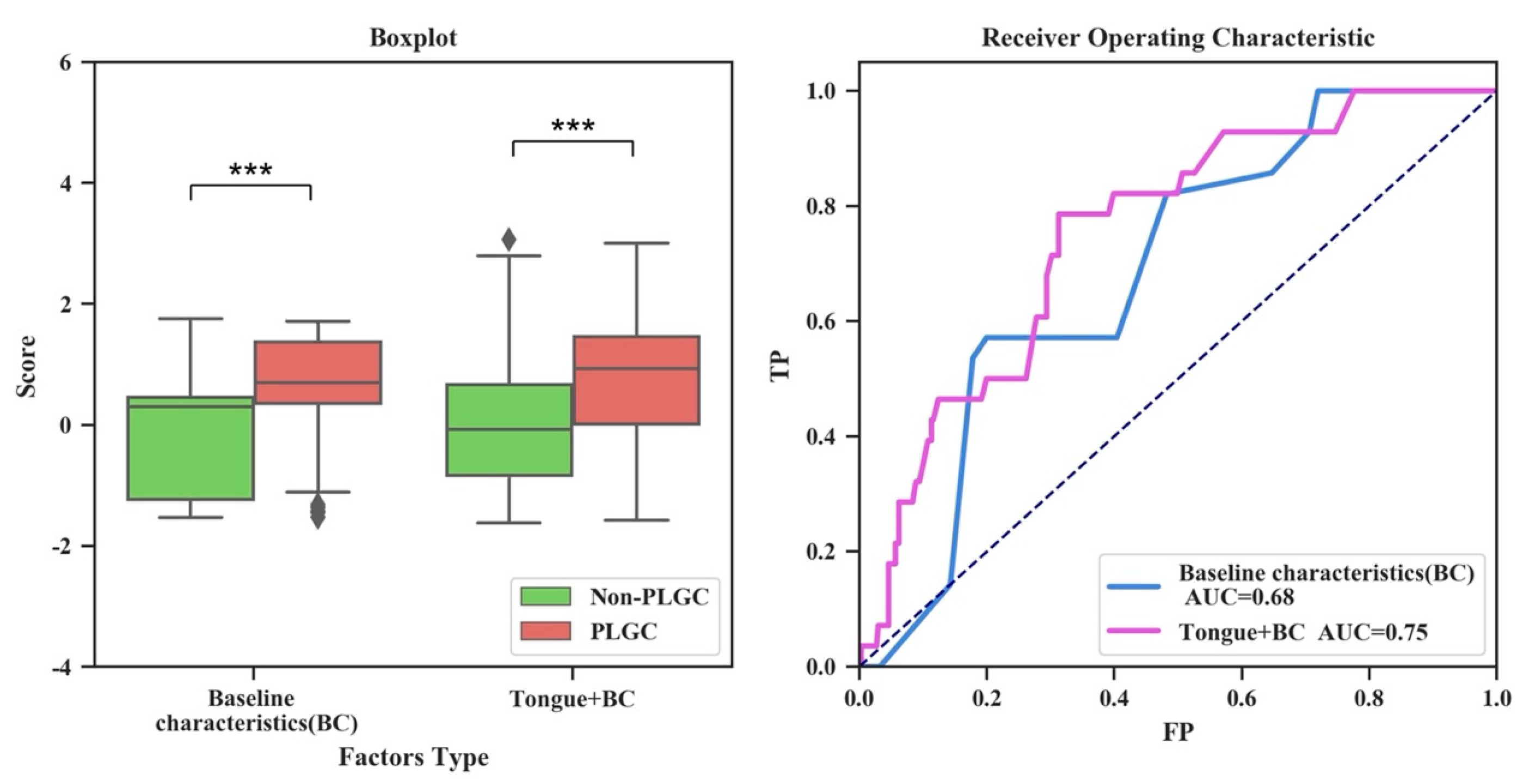
3.3. External Validation of PLGC Screening
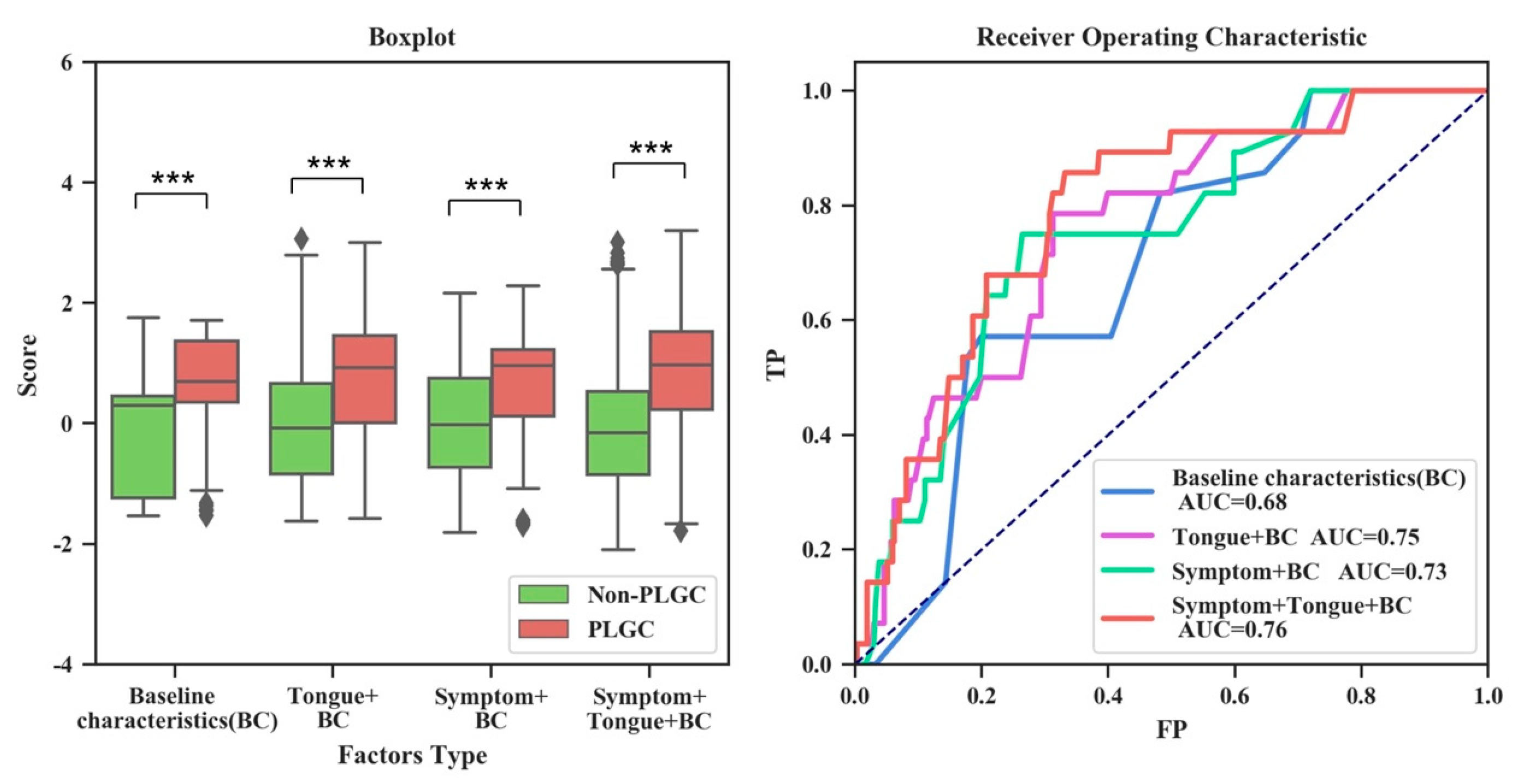
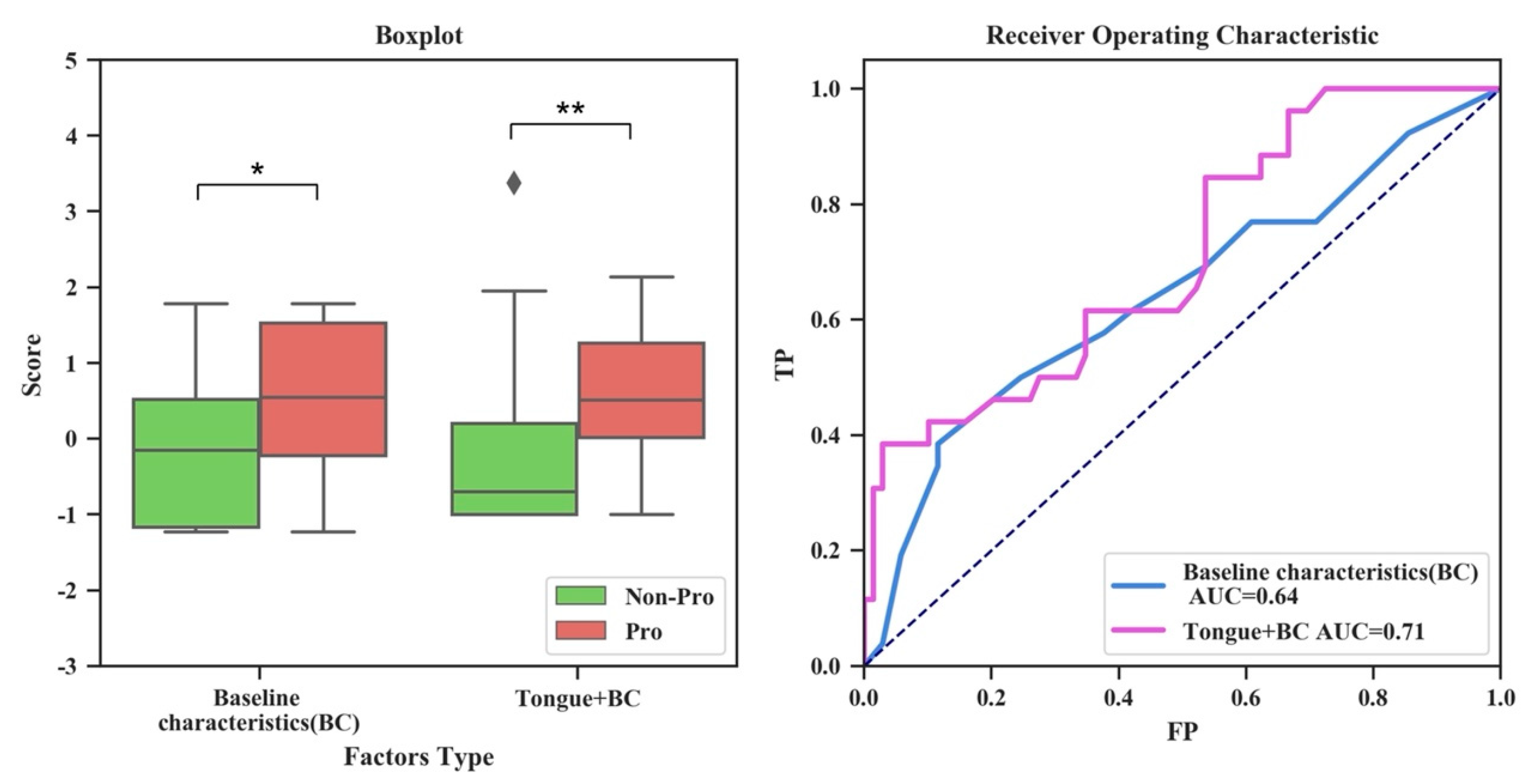
3.4. Evaluation of the Validity of Tongue Image Characteristics for Risk Prediction of PLGC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zong, L.; Abe, M.; Seto, Y.; Ji, J. The challenge of screening for early gastric cancer in China. Lancet 2016, 388, 2606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlemper, R.J.; Riddell, R.H.; Kato, Y.; Borchard, F.; Cooper, H.S.; Dawsey, S.M.; Dixon, M.F.; Fenoglio-Preiser, C.M.; Fléjou, J.F.; Geboes, K.; et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut 2000, 47, 251–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, H.; Ekheden, I.G.; Zheng, Z.; Ericsson, J.; Nyren, O.; Ye, W. Incidence of gastric cancer among patients with gastric precancerous lesions: Observational cohort study in a low risk Western population. BMJ 2015, 351, h3867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, A.C.; van Grieken, N.C.; Looman, C.W.; Casparie, M.K.; de Vries, E.; Meijer, G.A.; Kuipers, E.J. Gastric cancer risk in patients with premalignant gastric lesions: A nationwide cohort study in the Netherlands. Gastroenterology 2008, 134, 945–952. [Google Scholar] [CrossRef]
- Piazuelo, M.B.; Bravo, L.E.; Mera, R.M.; Camargo, M.C.; Bravo, J.C.; Delgado, A.G.; Washington, M.K.; Rosero, A.; Garcia, L.S.; Realpe, J.L.; et al. The Colombian Chemoprevention Trial: 20-Year Follow-Up of a Cohort of Patients with Gastric Precancerous Lesions. Gastroenterology 2021, 160, 1106–1117.e1103. [Google Scholar] [CrossRef]
- Rugge, M.; Meggio, A.; Pravadelli, C.; Barbareschi, M.; Fassan, M.; Gentilini, M.; Zorzi, M.; Pretis, G.; Graham, D.Y.; Genta, R.M. Gastritis staging in the endoscopic follow-up for the secondary prevention of gastric cancer: A 5-year prospective study of 1755 patients. Gut 2019, 68, 11–17. [Google Scholar] [CrossRef]
- Yan, H.; Li, M.; Cao, L.; Chen, H.; Lai, H.; Guan, Q.; Chen, H.; Zhou, W.; Zheng, B.; Guo, Z.; et al. A robust qualitative transcriptional signature for the correct pathological diagnosis of gastric cancer. J. Transl. Med. 2019, 17, 63. [Google Scholar] [CrossRef]
- Endoscopy CSoD. Consensus on screening and endoscopic diagnosis and treatment of early gastric cancer in China (Changsha, 2014). Zhonghua Xiao Hua Nei Jing Za Zhi 2014, 31, 361–377. [Google Scholar]
- Du, Y.; Bai, Y.; Xie, P.; Fang, J.; Wang, X.; Hou, X.; Tian, D.; Wang, C.; Liu, Y.; Sha, W.; et al. Chronic gastritis in China: A national multi-center survey. BMC Gastroenterol. 2014, 14, 21. [Google Scholar] [CrossRef] [Green Version]
- Tu, H.; Sun, L.; Dong, X.; Gong, Y.; Xu, Q.; Jing, J.; Bostick, R.M.; Wu, X.; Yuan, Y. A Serological Biopsy Using Five Stomach-Specific Circulating Biomarkers for Gastric Cancer Risk Assessment: A Multi-Phase Study. Am. J. Gastroenterol. 2017, 112, 704–715. [Google Scholar] [CrossRef]
- Huang, S.; Guo, Y.; Li, Z.W.; Shui, G.; Tian, H.; Li, B.W.; Kadeerhan, G.; Li, Z.X.; Li, X.; Zhang, Y.; et al. Identification and Validation of Plasma Metabolomic Signatures in Precancerous Gastric Lesions That Progress to Cancer. JAMA Netw Open 2021, 4, e2114186. [Google Scholar] [CrossRef]
- Huang, K.K.; Ramnarayanan, K.; Zhu, F.; Srivastava, S.; Xu, C.; Tan, A.L.K.; Lee, M.; Tay, S.; Das, K.; Xing, M.; et al. Genomic and Epigenomic Profiling of High-Risk Intestinal Metaplasia Reveals Molecular Determinants of Progression to Gastric Cancer. Cancer Cell 2018, 33, 137–150.e135. [Google Scholar] [CrossRef] [Green Version]
- Cubiella, J.; Perez Aisa, A.; Cuatrecasas, M.; Diez Redondo, P.; Fernandez Esparrach, G.; Marin-Gabriel, J.C.; Moreira, L.; Nunez, H.; Pardo Lopez, M.L.; Rodriguez de Santiago, E.; et al. Gastric cancer screening in low incidence populations: Position statement of AEG, SEED and SEAP. Gastroenterol. Hepatol. 2021, 44, 67–86. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Libanio, D.; Marcos-Pinto, R.; Areia, M.; Leja, M.; Esposito, G.; Garrido, M.; Kikuste, I.; Megraud, F.; Matysiak-Budnik, T.; et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019, 51, 365–388. [Google Scholar]
- Afrash, M.R.; Shafiee, M.; Kazemi-Arpanahi, H. Establishing machine learning models to predict the early risk of gastric cancer based on lifestyle factors. BMC Gastroenterol. 2023, 23, 6. [Google Scholar] [CrossRef]
- Jiang, T.; Guo, X.J.; Tu, L.P.; Lu, Z.; Cui, J.; Ma, X.X.; Hu, X.J.; Yao, X.H.; Cui, L.T.; Li, Y.Z.; et al. Application of computer tongue image analysis technology in the diagnosis of NAFLD. Comput. Biol. Med. 2021, 135, 104622. [Google Scholar] [CrossRef]
- Li, J.; Huang, J.; Jiang, T.; Tu, L.; Cui, L.; Cui, J.; Ma, X.; Yao, X.; Shi, Y.; Wang, S.; et al. A multi-step approach for tongue image classification in patients with diabetes. Comput. Biol. Med. 2022, 149, 105935. [Google Scholar] [CrossRef]
- Zhuang, Q.; Gan, S.; Zhang, L. Human-computer interaction based health diagnostics using ResNet34 for tongue image classification. Comput. Methods Programs Biomed. 2022, 226, 107096. [Google Scholar] [CrossRef]
- Hu, Y.; Wen, G.; Luo, M.; Yang, P.; Dai, D.; Yu, Z.; Wang, C.; Hall, W. Fully-channel regional attention network for disease-location recognition with tongue images. Artif. Intell. Med. 2021, 118, 102110. [Google Scholar] [CrossRef]
- Zhang, B.; Kumar, B.V.; Zhang, D. Detecting diabetes mellitus and nonproliferative diabetic retinopathy using tongue color, texture, and geometry features. IEEE Trans. Biomed. Eng. 2014, 61, 491–501. [Google Scholar] [CrossRef]
- Shang, Z.; Du, Z.G.; Guan, B.; Ji, X.Y.; Chen, L.C.; Wang, Y.J.; Ma, Y. Correlation analysis between characteristics under gastroscope and image information of tongue in patients with chronic gastriti. J. Tradit. Chin. Med. 2022, 42, 102–107. [Google Scholar]
- Kainuma, M.; Furusyo, N.; Urita, Y.; Nagata, M.; Ihara, T.; Oji, T.; Nakaguchi, T.; Namiki, T.; Hayashi, J. The association between objective tongue color and endoscopic findings: Results from the Kyushu and Okinawa population study (KOPS). BMC Complement. Altern. Med. 2015, 15, 372. [Google Scholar] [CrossRef] [Green Version]
- Gholami, E.; Tabbakh, S.R.K.; kheirabadi, M. Increasing the accuracy in the diagnosis of stomach cancer based on color and lint features of tongue. Biomed. Signal Process. Control 2021, 69, 102782. [Google Scholar] [CrossRef]
- Zhu, X.; Ma, Y.; Guo, D.; Men, J.; Xue, C.; Cao, X.; Zhang, Z. A Framework to Predict Gastric Cancer Based on Tongue Features and Deep Learning. Micromachines 2023, 14, 53. [Google Scholar] [CrossRef]
- Li, J.; Yuan, P.; Hu, X.; Huang, J.; Cui, L.; Cui, J.; Ma, X.; Jiang, T.; Yao, X.; Li, J.; et al. A tongue features fusion approach to predicting prediabetes and diabetes with machine learning. J. Biomed. Inform. 2021, 115, 103693. [Google Scholar] [CrossRef]
- Lu, C.; Zhu, H.; Zhao, D.; Zhang, J.; Yang, K.; Lv, Y.; Peng, M.; Xu, X.; Huang, J.; Shao, Z.; et al. Oral-Gut Microbiome Analysis in Patients with Metabolic-Associated Fatty Liver Disease Having Different Tongue Image Feature. Front. Cell. Infect. Microbiol. 2022, 12, 787143. [Google Scholar] [CrossRef]
- Pang, W.; Zhang, D.; Zhang, J.; Li, N.; Zheng, W.; Wang, H.; Liu, C.; Yang, F.; Pang, B. Tongue features of patients with coronavirus disease 2019: A retrospective cross-sectional study. Integr. Med. Res. 2020, 9, 100493. [Google Scholar] [CrossRef]
- Cui, J.; Hou, S.; Liu, B.; Yang, M.; Wei, L.; Du, S.; Li, S. Species composition and overall diversity are significantly correlated between the tongue coating and gastric fluid microbiomes in gastritis patients. BMC Med. Genom. 2022, 15, 60. [Google Scholar] [CrossRef]
- Cui, J.; Cui, H.; Yang, M.; Du, S.; Li, J.; Li, Y.; Liu, L.; Zhang, X.; Li, S. Tongue coating microbiome as a potential biomarker for gastritis including precancerous cascade. Protein Cell 2019, 10, 496–509. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Xiang, C.; Zhang, C.; Xu, B.; Wu, J.; Wang, R.; Yang, Y.; Shi, L.; Zhang, J.; Zhan, Z. Microbial biomarkers of common tongue coatings in patients with gastric cancer. Microb. Pathog. 2019, 127, 97–105. [Google Scholar] [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]
- Zhou, W.; Yang, K.; Zeng, J.; Lai, X.; Wang, X.; Ji, C.; Li, Y.; Zhang, P.; Li, S. FordNet: Recommending traditional Chinese medicine formula via deep neural network integrating phenotype and molecule. Pharmacol. Res. 2021, 173. [Google Scholar] [CrossRef]
- Skrede, O.J.; De Raedt, S.; Kleppe, A.; Hveem, T.S.; Liestol, K.; Maddison, J.; Askautrud, H.A.; Pradhan, M.; Nesheim, J.A.; Albregtsen, F.; et al. Deep learning for prediction of colorectal cancer outcome: A discovery and validation study. Lancet 2020, 395, 350–360. [Google Scholar] [CrossRef]
- Zhou, H.; Liu, Z.; Li, T.; Chen, Y.; Huang, W.; Zhang, Z. Classification of precancerous lesions based on fusion of multiple hierarchical features. Comput. Biol. Med. 2023, 229, 107301. [Google Scholar]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.; van Ginneken, B.; Sanchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Yaqoob, M.M.; Nazir, M.; Yousafzai, A.; Khan, M.A.; Shaikh, A.A.; Algarni, A.D.; Elmannai, H. Modified Artificial Bee Colony Based Feature Optimized Federated Learning for Heart Disease Diagnosis in Healthcare. Appl. Sci. 2022, 12, 12080. [Google Scholar] [CrossRef]
- van der Laak, J.; Litjens, G.; Ciompi, F. Deep learning in histopathology: The path to the clinic. Nat. Med. 2021, 27, 775–784. [Google Scholar] [CrossRef]
- Bulten, W.; Pinckaers, H.; van Boven, H.; Vink, R.; de Bel, T.; van Ginneken, B.; van der Laak, J.; Hulsbergen-van de Kaa, C.; Litjens, G. Automated deep-learning system for Gleason grading of prostate cancer using biopsies: A diagnostic study. Lancet Oncol. 2020, 21, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Chen, Q.; Hu, X.; Yuan, P.; Cui, L.; Tu, L.; Cui, J.; Huang, J.; Jiang, T.; Ma, X.; et al. Establishment of noninvasive diabetes risk prediction model based on tongue features and machine learning techniques. Int. J. Med. Inform. 2021, 149, 104429. [Google Scholar] [CrossRef]
- Dixon, M.F.; Genta, R.M.; Yardley, J.H.; Correa, P. Classification and grading of gastritis. The updated Sydney System. International Workshop on the Histopathology of Gastritis, Houston 1994. Am. J. Surg. Pathol. 1996, 20, 1161–1181. [Google Scholar] [CrossRef]
- You, W.C.; Blot, W.J.; Li, J.Y.; Chang, Y.S.; Jin, M.L.; Kneller, R.; Zhang, L.; Han, Z.X.; Zeng, X.R.; Liu, W.D.; et al. Precancerous gastric lesions in a population at high risk of stomach cancer. Cancer Res. 1993, 53, 1317–1321. [Google Scholar] [PubMed]
- Zhang, L.; Blot, W.J.; You, W.C.; Chang, Y.S.; Kneller, R.W.; Jin, M.L.; Li, J.Y.; Zhao, L.; Liu, W.D.; Zhang, J.S.; et al. Helicobacter pylori antibodies in relation to precancerous gastric lesions in a high-risk Chinese population. Cancer Epidemiol. Biomark. Prev. 1996, 5, 627–630. [Google Scholar]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You Only Look Once: Unified, Real-Time Object Detection. Proc. Cvpr. IEEE 2016, 779–788. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016. [Google Scholar]
- Li, S.; Wang, R.; Zhang, Y.; Zhang, X.; Layon, A.J.; Li, Y.; Chen, M. Symptom Combinations Associated with Outcome and Therapeutic Effects in a Cohort of Cases with SARS. Am. J. Chin. Med. 2006, 34, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Cai, Q.; Zhu, C.; Yuan, Y.; Feng, Q.; Feng, Y.; Hao, Y.; Li, J.; Zhang, K.; Ye, G.; Ye, L.; et al. Development and validation of a prediction rule for estimating gastric cancer risk in the Chinese high-risk population: A nationwide multicentre study. Gut 2019, 68, 1576–1587. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Lu, A.P.; Zhang, L.; Li, Y.D. Anti-Helicobacter pylori immunoglobulin G (IgG) and IgA antibody responses and the value of clinical presentations in diagnosis of H. pylori infection in patients with precancerous lesions. World J. Gastroenterol. 2003, 9, 755–758. [Google Scholar] [CrossRef]
- Redeen, S.; Petersson, F.; Jonsson, K.A.; Borch, K. Relationship of gastroscopic features to histological findings in gastritis and Helicobacter pylori infection in a general population sample. Endoscopy 2003, 35, 946–950. [Google Scholar]
- Su, S.; Lu, A.; Li, S.; Jia, W. Evidence-Based ZHENG: A Traditional Chinese Medicine Syndrome. Evid. Based Complement Altern. Med. 2012, 2012, 246538. [Google Scholar] [CrossRef]
- Kanawong, R.; Ajayi, T.; Ma, T.; Xu, D.; Li, S.; Duan, Y. Automated tongue feature extraction for ZHENG classification in traditional Chinese medicine. Evid.-Based Complement. Altern. Med. 2012, 2012, 912852. [Google Scholar] [CrossRef] [Green Version]
- Kanawong, R.; Xu, W.; Xu, D.; Li, S.; Ma, T.; Duan, Y. An automatic tongue detection and segmentation framework for computer-aided tongue image analysis. Int. J. Funct. Inform. Pers. Med. 2012, 4, 56–68. [Google Scholar] [CrossRef]
- Wang, P.; Shi, B.; Wen, Y.; Tang, X. Construction of risk prediction model for precancerous lesions of gastric cancer combined with disease and syndrome. Chin. J. Integr. Tradit. Chin. West. Med. 2018, 38, 773–778. (in Chinese). [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohorts | Groups | Counts | Age (Mean ± SD) | Gender (Male/Female) |
|---|---|---|---|---|
| Development cohort | PLGC | 55 | 58.6 ± 10.5 | 31/24 |
| non-PLGC | 270 | 48.0 ± 13.6 | 135/135 | |
| Validation cohort | PLGC | 171 | 58.5 ± 9.3 | 100/71 |
| non-PLGC | 1824 | 49.9 ± 13.1 | 685/1139 | |
| Follow-up cohort | Pro | 26 | 51.7 ± 8.7 | 14/12 |
| non-Pro | 69 | 46.1 ± 11.9 | 24/45 |
| Characteristics | High Risk (94) | Low Risk (233) | p Value | ||
|---|---|---|---|---|---|
| Counts | Ratio | Counts | Ratio | ||
| Coating (Yellow) | 16 | 0.17 | 16 | 0.07 | 9.6 × 10−3 |
| Greasy | 28 | 0.30 | 34 | 0.15 | 2.6 × 10−3 |
| Fissured | 19 | 0.20 | 26 | 0.11 | 4.8 × 10−2 |
| Coating (Thick) | 14 | 0.15 | 15 | 0.06 | 2.6 × 10−2 |
| Dark | 12 | 0.13 | 7 | 0.03 | 1.6 × 10−3 |
| Variable | Total (N = 1995) No. (%) | Non-PLGC (N = 1824) No. (%) | PLGC (N = 171) No. (%) | p Value * | Adjusted OR (95% CI) † | p Value # |
|---|---|---|---|---|---|---|
| Baseline Factors | ||||||
| Age, Years | 3.7× 10−15 | |||||
| >50 | 1067 (0.53) | 926 (0.51) | 141 (0.82) | 4.14 ([2.59,6.61]) | 2.9 × 10−9 | |
| ≤50 | 928 (0.47) | 898 (0.49) | 30 (0.18) | |||
| Gender | 1.3 × 10−7 | |||||
| Male | 785 (0.39) | 685 (0.38) | 100 (0.58) | 1.47 ([1.00,2.14]) | 4.8 × 10−2 | |
| Female | 1210 (0.61) | 1139 (0.62) | 71 (0.42) | |||
| Hp | 0.71 | |||||
| Yes | 174 (0.24) | 142 (0.24) | 32 (0.22) | 1.15 ([0.73,1.81]) | 0.55 | |
| No | 556 (0.76) | 445 (0.76) | 111 (0.78) | |||
| Tongue Diagnostic Labels | ||||||
| Coating | 1.9 × 10−10 | |||||
| Yellow | 327 (0.16) | 269 (0.15) | 58 (0.34) | 3.66 ([2.38,5.62]) | 3.4 × 10−9 | |
| White | 1668 (0.84) | 1555 (0.85) | 113 (0.66) | |||
| Fissure | 3.8 × 10−9 | |||||
| Yes | 187 (0.09) | 149 (0.08) | 38 (0.22) | 2.26 ([1.37,3.73]) | 1.4 × 10−3 | |
| No | 1808 (0.91) | 1675 (0.92) | 133 (0.78) | |||
| Greasy | 3.3 × 10−4 | |||||
| Yes | 422 (0.21) | 367 (0.20) | 55 (0.32) | 2.23 ([1.44,3.46]) | 3.3 × 10−4 | |
| No | 1573 (0.79) | 1457 (0.80) | 116 (0.68) | |||
| Coating | 1.3 × 10−3 | |||||
| Thick | 239 (0.12) | 205 (0.11) | 34 (0.20) | 2.18 ([1.29,3.67]) | 3.6 × 10−3 | |
| Thin | 1756 (0.88) | 1619 (0.89) | 137 (0.80) | |||
| Dark | 0.03 | |||||
| Yes | 312 (0.16) | 275 (0.15) | 37 (0.22) | 1.93 ([1.20,3.11]) | 6.7 × 10−3 | |
| No | 1683 (0.84) | 1549 (0.85) | 134 (0.78) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, C.; Zhang, P.; Du, S.; Li, Y.; Li, S. Construction of Tongue Image-Based Machine Learning Model for Screening Patients with Gastric Precancerous Lesions. J. Pers. Med. 2023, 13, 271. https://doi.org/10.3390/jpm13020271
Ma C, Zhang P, Du S, Li Y, Li S. Construction of Tongue Image-Based Machine Learning Model for Screening Patients with Gastric Precancerous Lesions. Journal of Personalized Medicine. 2023; 13(2):271. https://doi.org/10.3390/jpm13020271
Chicago/Turabian StyleMa, Changzheng, Peng Zhang, Shiyu Du, Yan Li, and Shao Li. 2023. "Construction of Tongue Image-Based Machine Learning Model for Screening Patients with Gastric Precancerous Lesions" Journal of Personalized Medicine 13, no. 2: 271. https://doi.org/10.3390/jpm13020271