
An Individualized Multi-Modal Approach for Detection of Medication “Off” Episodes in Parkinson’s Disease via Wearable Sensors
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
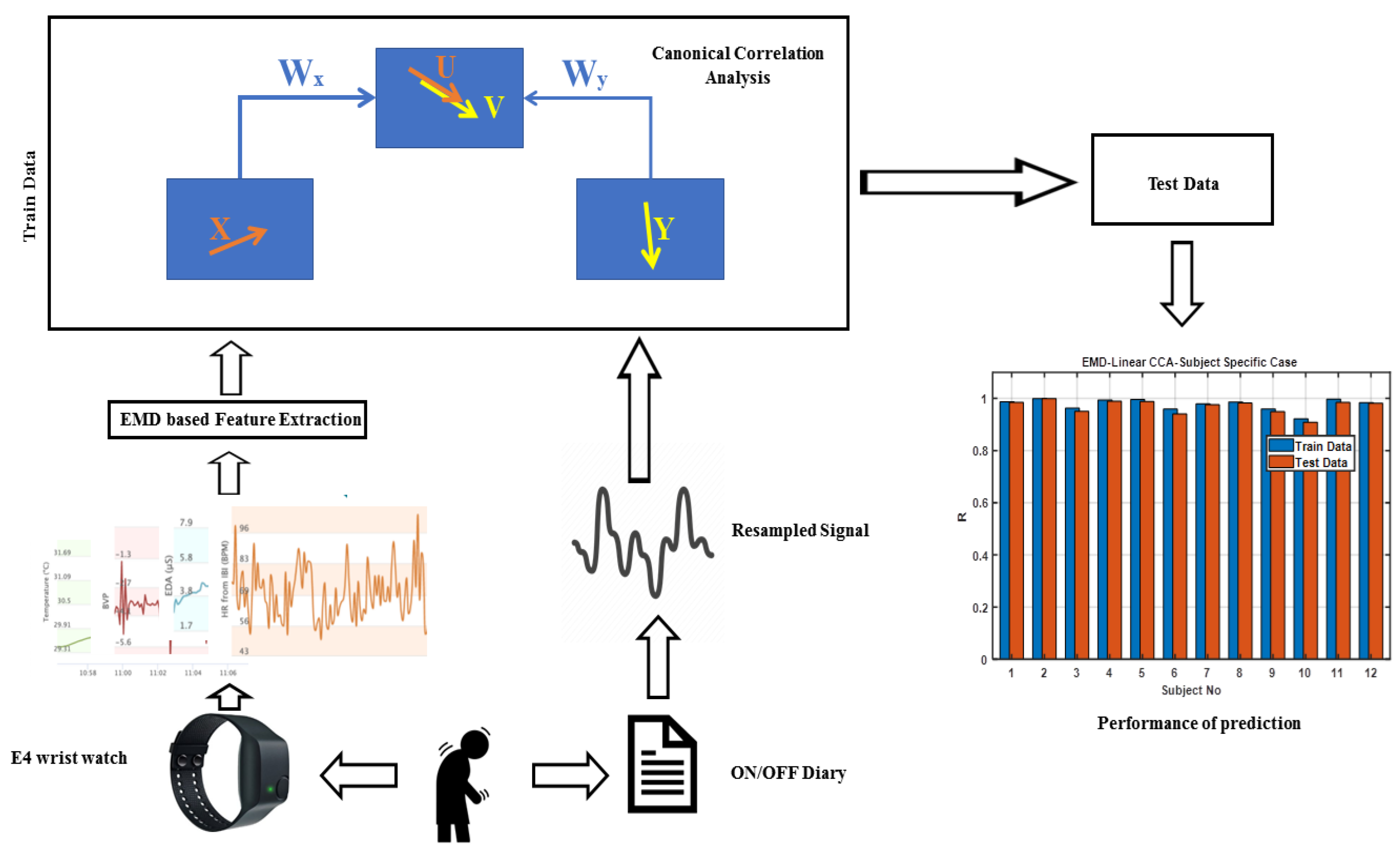
2.2. Method
2.2.1. Pre-Processing and Feature Extraction
2.2.2. Intersubject Approach
2.2.3. Subject-Specific Approach
3. Results
3.1. Intersubject Approach
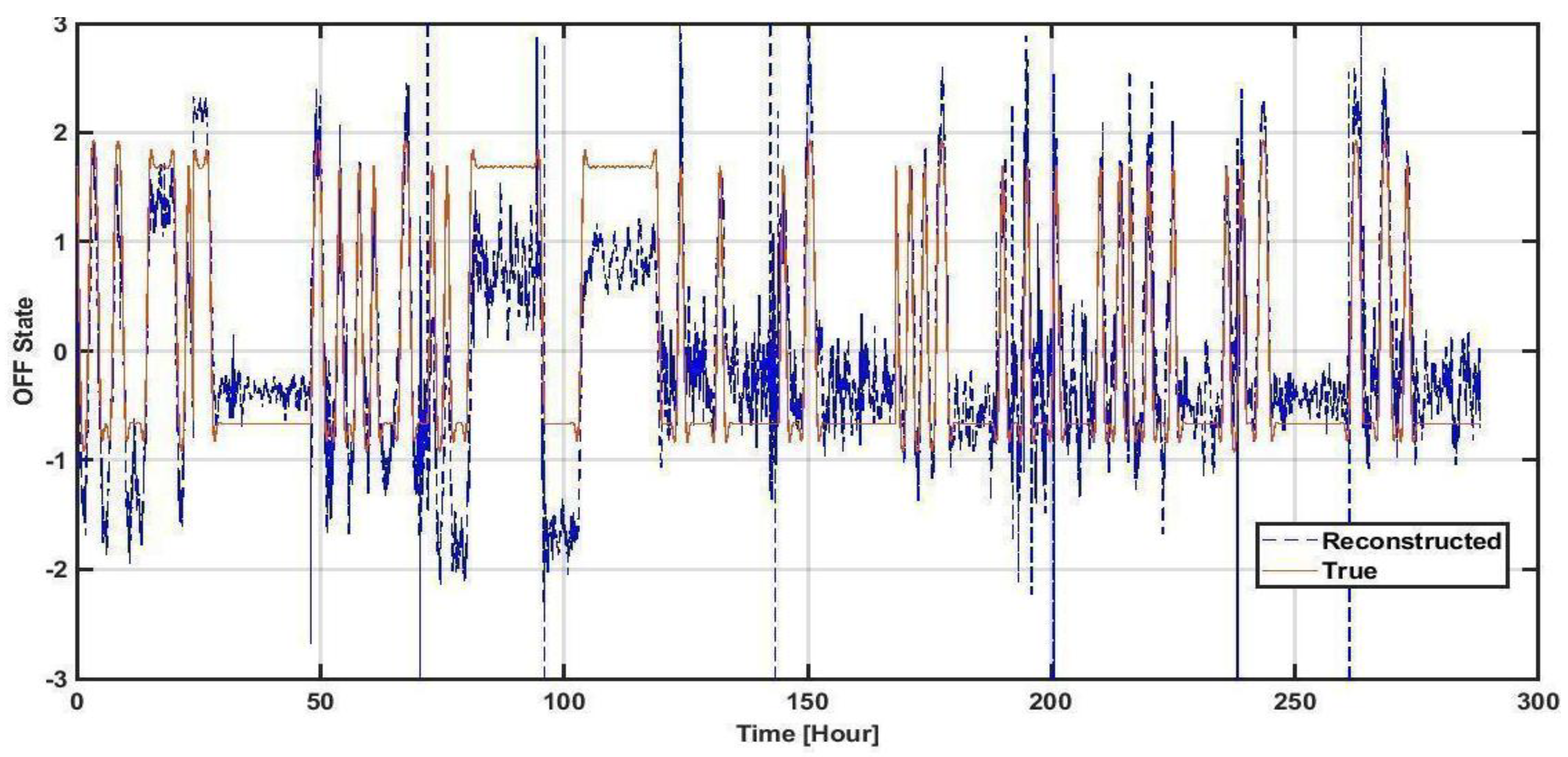
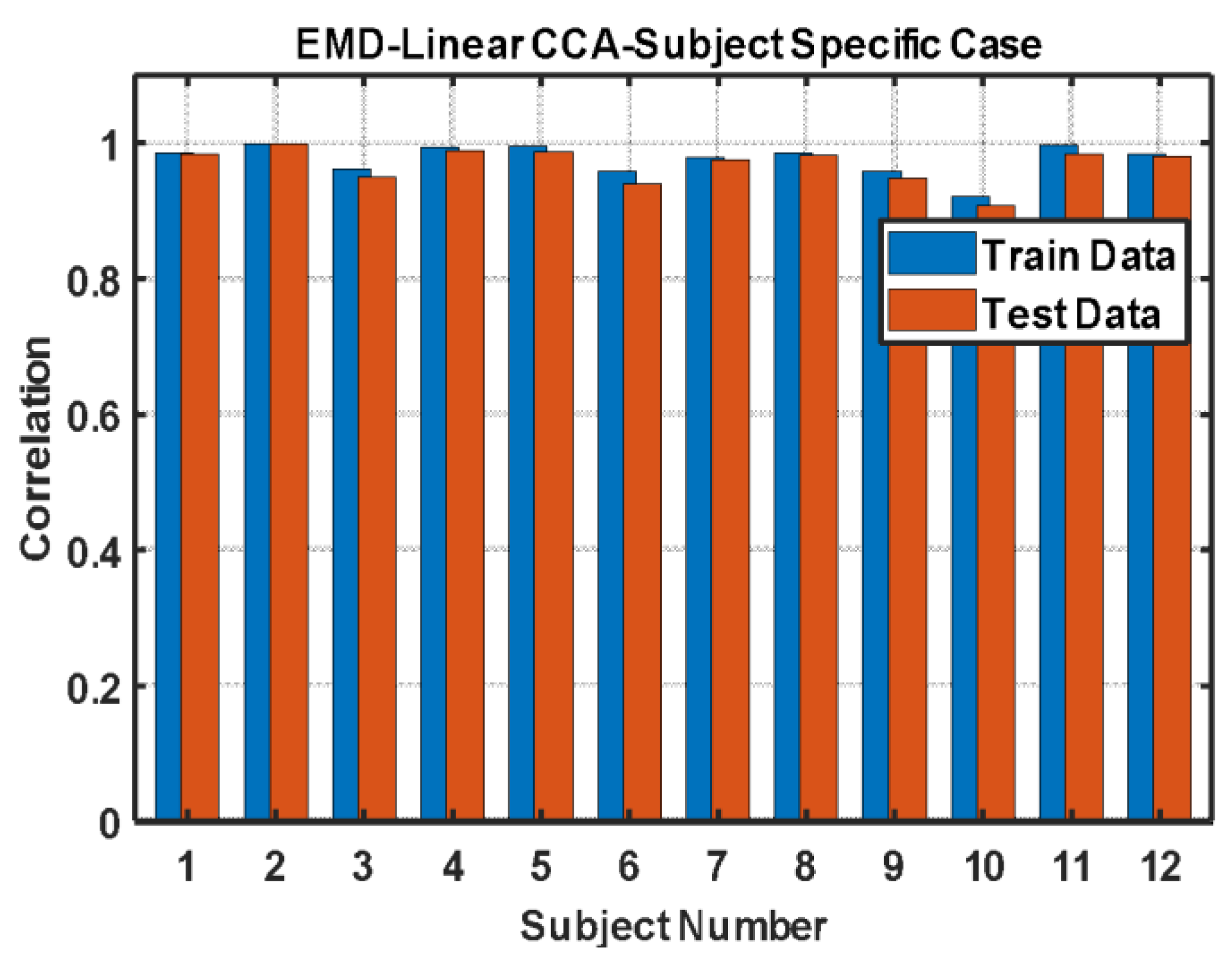
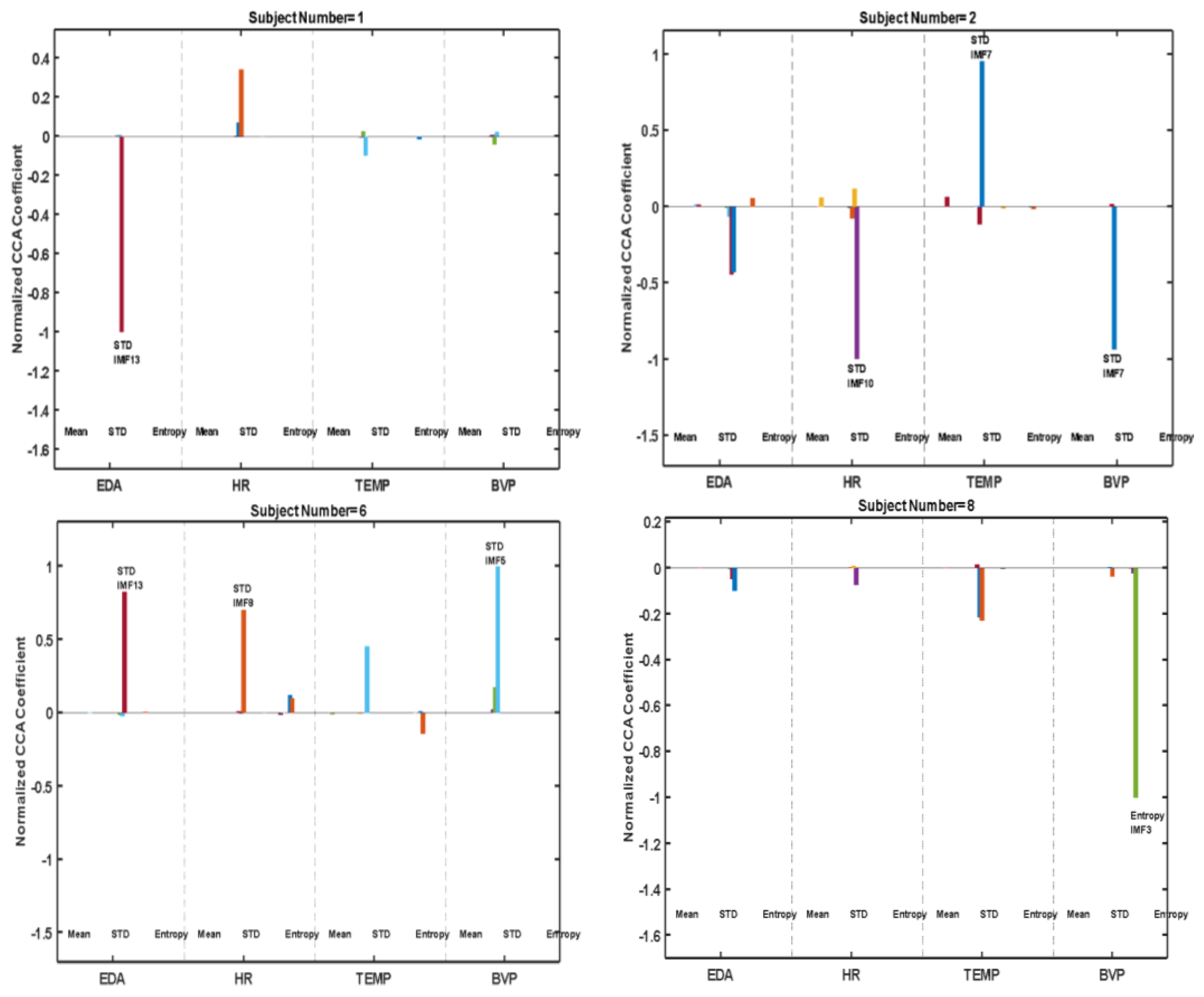
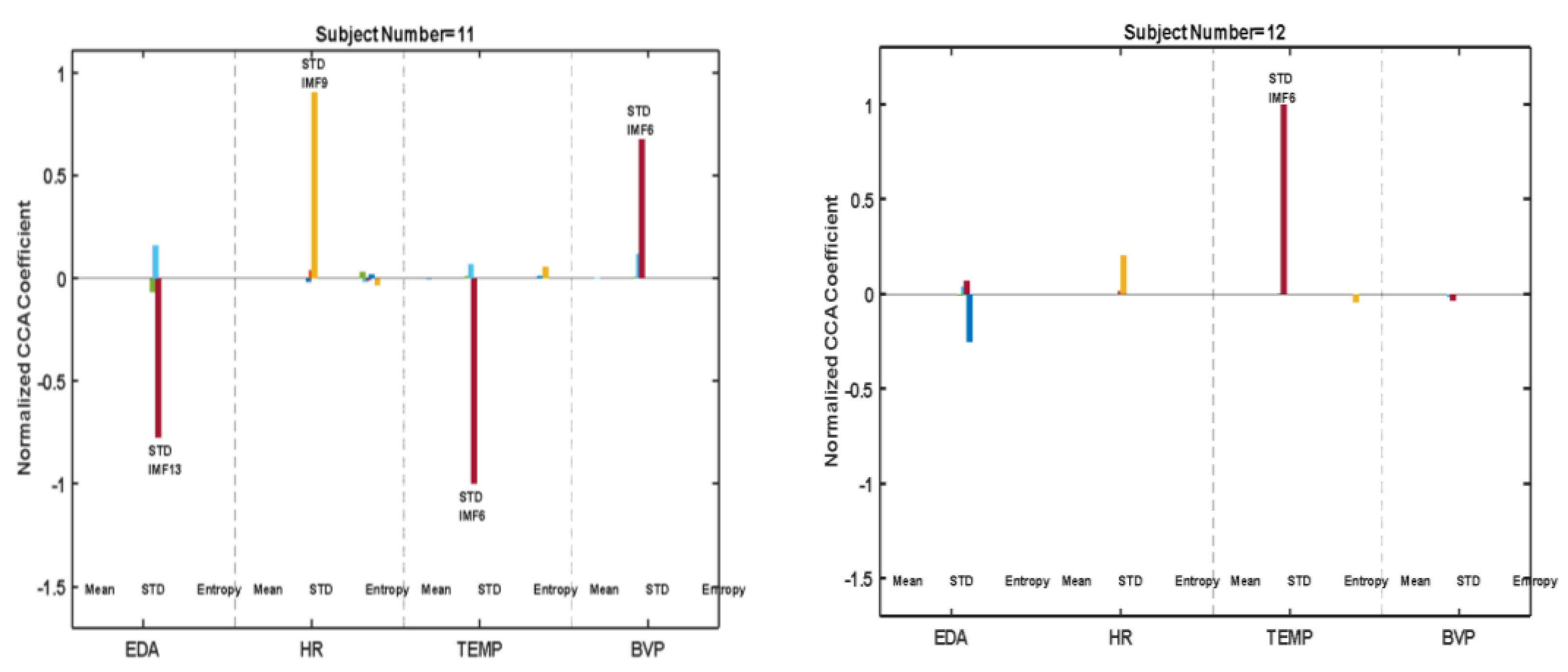
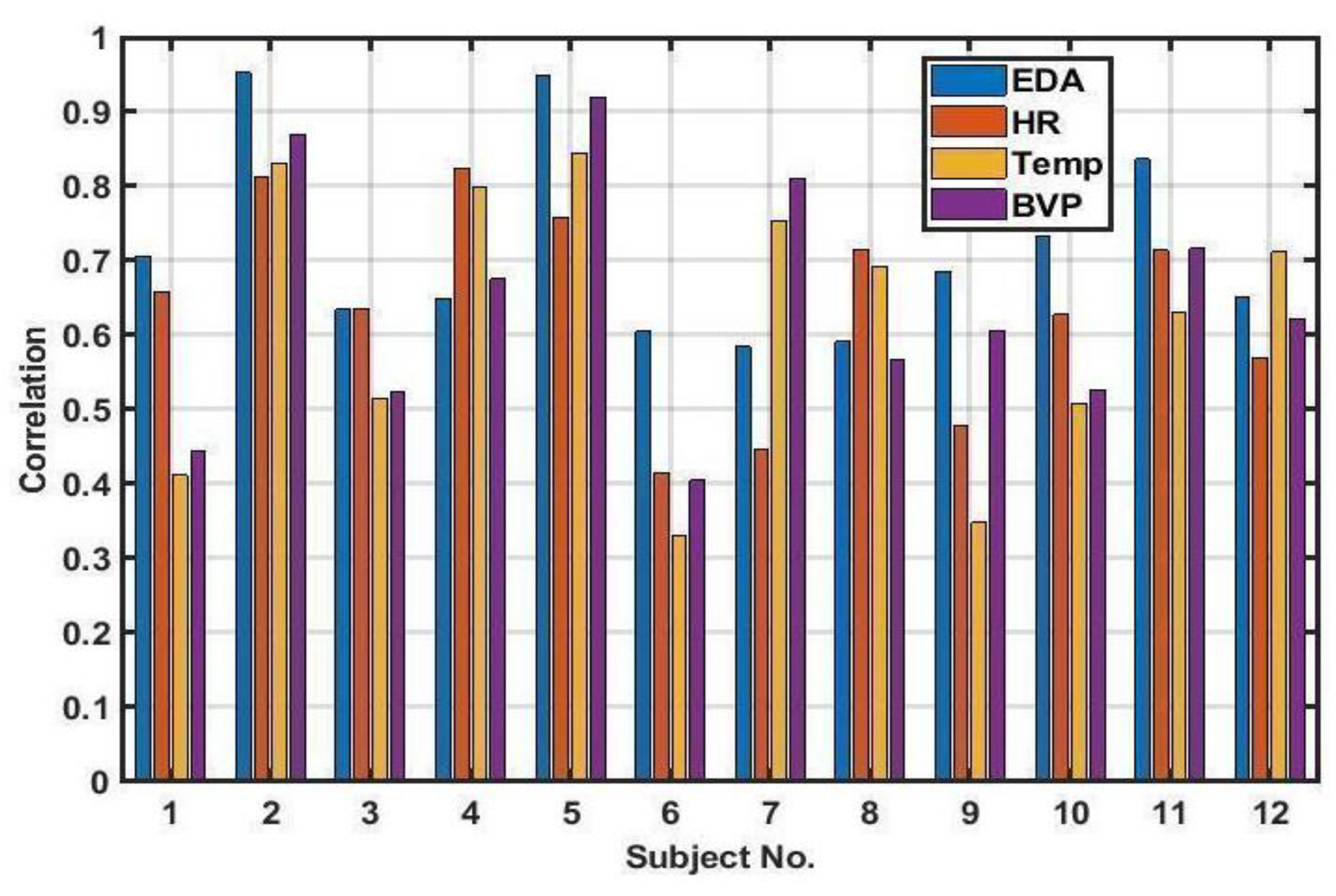
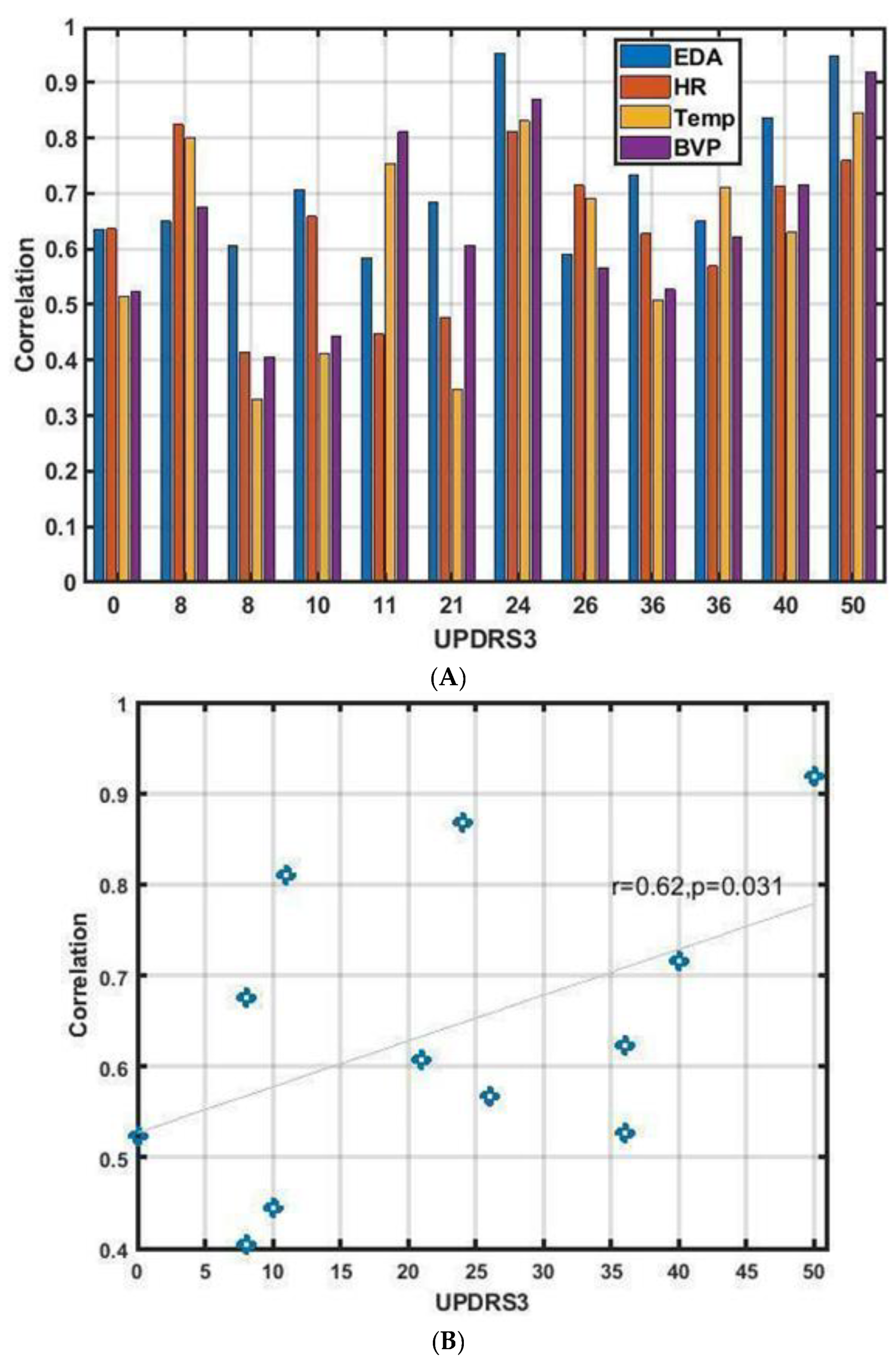
3.2. Subject-Specific Approach
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hillen, M.E.; Sage, J.I. Nonmotor fluctuations in patients with Parkinson’s disease. Neurology 1996, 47, 1180–1183. [Google Scholar] [CrossRef] [PubMed]
- Reardon, K.A.; Shiff, M.; Kempster, P.A. Evolution of motor fluctuations in Parkinson’s disease: A longitudinal study over 6 years. Mov. Disord. 1999, 14, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Kish, S.J.; Shannak, K.; Hornykiewicz, O. Uneven pattern of dopamine loss in the striatum of patients with idiopathic Parkinson’s disease. N. Engl. J. Med. 1988, 318, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Contin, M.; Martinelli, P. Pharmacokinetics of levodopa. J. Neurol. 2010, 257, 253–261. [Google Scholar] [CrossRef]
- Contin, M.; Riva, R.; Albani, F.; Baruzzi, A. Pharmacokinetic optimisation in the treatment of Parkinson’s disease. Clin. Pharmacokinet. 1996, 30, 463–481. [Google Scholar] [CrossRef]
- Jenkinson, N.; Brown, P. New insights into the relationship between dopamine, beta oscillations and motor function. Trends Neurosci. 2011, 34, 611–618. [Google Scholar] [CrossRef]
- Martínez-Fernández, R.; Schmitt, E.; Martinez-Martin, P.; Krack, P. The hidden sister of motor fluctuations in Parkinson’s disease: A review on nonmotor fluctuations. Mov. Disord. 2016, 31, 1080–1094. [Google Scholar] [CrossRef]
- Kashihara, K. Weight loss in Parkinson’s disease. J. Neurol. 2006, 253, vii38–vii41. [Google Scholar] [CrossRef]
- Chase, T.N. The significance of continuous dopaminergic stimulation in the treatment of Parkinson’s disease. Drugs 1998, 55, 1–9. [Google Scholar] [CrossRef]
- Olanow, C.W.; Obeso, J.A.; Stocchi, F. Drug insight: Continuous dopaminergic stimulation in the treatment of Parkinson’s disease. Nat. Clin. Pract. Neurol. 2006, 2, 382–392. [Google Scholar] [CrossRef]
- Nyholm, D. Duodopa® treatment for advanced Parkinson’s disease: A review of efficacy and safety. Park. Relat. Disord. 2012, 18, 916–929. [Google Scholar] [CrossRef] [PubMed]
- Nutt, J.G. Continuous dopaminergic stimulation: Is it the answer to the motor complications of levodopa? Mov. Disord. 2007, 22, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tai, L.-C.; Liaw, T.; Lin, Y.; Nyein, H.Y.Y.; Bariya, M.; Ji, W.; Hettick, M.; Zhao, C.; Zhao, J.; Hou, L.; et al. Wearable sweat band for noninvasive levodopa monitoring. Nano Lett. 2019, 19, 6346–6351. [Google Scholar] [CrossRef]
- Moon, J.M.; Teymourian, H.; De la Paz, E.; Sempionatto, J.R.; Mahato, K.; Sonsaard, T.; Huang, N.; Longardner, K.; Litvan, I.; Wang, J. Non-Invasive Sweat-Based Tracking of L-Dopa Pharmacokinetic Profiles Following an Oral Tablet Administration. Angew. Chem. 2021, 133, 19222–19226. [Google Scholar] [CrossRef]
- Goud, K.Y.; Moonla, C.; Mishra, R.K.; Yu, C.; Narayan, R.; Litvan, I.; Wang, J. Wearable electrochemical microneedle sensor for continuous monitoring of levodopa: Toward Parkinson management. ACS Sens. 2019, 4, 2196–2204. [Google Scholar] [CrossRef]
- Adams, J.L.; Dinesh, K.; Snyder, C.W.; Xiong, M.; Tarolli, C.G.; Sharma, S.; Dorsey, E.R.; Sharma, G. A real-world study of wearable sensors in Parkinson’s disease. NPJ Park. Dis. 2021, 7, 106. [Google Scholar] [CrossRef]
- Daneault, J.-F.; Vergara-Diaz, G.; Parisi, F.; Admati, C.; Alfonso, C.; Bertoli, M.; Bonizzoni, E.; Carvalho, G.F.; Costante, G.; Fabara, E.E.; et al. Accelerometer data collected with a minimum set of wearable sensors from subjects with Parkinson’s disease. Sci. Data 2021, 8, 48. [Google Scholar] [CrossRef]
- Fisher, J.M.; Hammerla, N.Y.; Ploetz, T.; Andras, P.; Rochester, L.; Walker, R.W. Unsupervised home monitoring of Parkinson’s disease motor symptoms using body-worn accelerometers. Park. Relat. Disord. 2016, 33, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Habets, J.G.V.; Herff, C.; Kubben, P.L.; Kuijf, M.L.; Temel, Y.; Evers, L.J.W.; Bloem, B.R.; Starr, P.A.; Gilron, R.; Little, S. Rapid dynamic naturalistic monitoring of bradykinesia in Parkinson’s disease using a wrist-worn accelerometer. Sensors 2021, 21, 7876. [Google Scholar] [CrossRef]
- Ijima, Y.; Furudate, Y.; Chiba, K.; Ishida, Y.; Mikami, S. Automated Recognition of Off Phenomenon in Parkinson’s Disease During Walking: Measurement in Daily Life with Wearable Device. In Proceedings of the 2022 IEEE 4th Global Conference on Life Sciences and Technologies (LifeTech), Osaka, Japan, 7–9 March 2022. [Google Scholar]
- Victorino, J.N.; Shibata, Y.; Inoue, S.; Shibata, T. Predicting Wearing-Off of Parkinson’s Disease Patients Using a Wrist-Worn Fitness Tracker and a Smartphone: A Case Study. Appl. Sci. 2021, 11, 7354. [Google Scholar] [CrossRef]
- Ruonala, V.; Tarvainen, M.P.; Karjalainen, P.A.; Pekkonen, E.; Rissanen, S.M. Autonomic nervous system response to L-dopa in patients with advanced Parkinson’s disease. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015. [Google Scholar]
- Aquino, C.C.; Fox, S.H. Clinical spectrum of levodopa-induced complications. Mov. Disord. 2015, 30, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Devos, D.; Kroumova, M.; Bordet, R.; Vodougnon, H.; Guieu, J.D.; Libersa, C.; Destée, A. Heart rate variability and Parkinson’s disease severity. J. Neural Transm. 2003, 110, 997–1011. [Google Scholar] [PubMed]
- Posada-Quintero, H.F.; Florian, J.P.; Orjuela-Cañón, D.; Chon, K.H. Highly sensitive index of sympathetic activity based on time-frequency spectral analysis of electrodermal activity. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2016, 311, R582–R591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanková, S.; Straka, I.; Košutzká, Z.; Valkovič, P.; Minár, M. Levodopa-Carbidopa Intestinal Gel Improves Symptoms of Orthostatic Hypotension in Patients with Parkinson’s Disease—Prospective Pilot Interventional Study. J. Pers. Med. 2022, 12, 718. [Google Scholar] [CrossRef]
- Brim, B.; Struhal, W. Thermoregulatory dysfunctions in idiopathic Parkinson’s disease. In International Review of Movement Disorders; Elsevier: Amsterdam, The Netherlands, 2021; pp. 285–298. [Google Scholar]
- Abbruzzese, G.; Antonini, A.; Barone, P.; Stocchi, F.; Tamburini, T.; Bernardi, L.; Amboni, M.; Vacca, L.; Posocco, V.; Colombo, D. Linguistic, psychometric validation and diagnostic ability assessment of an Italian version of a 19-item wearing-off questionnaire for wearing-off detection in Parkinson’s disease. Neurol. Sci. 2012, 33, 1319–1327. [Google Scholar] [CrossRef]
- Stacy, M.; Bowron, A.; Guttman, M.; Hauser, R.; Hughes, K.; Larsen, J.P.; LeWitt, P.; Oertel, W.; Quinn, N.; Sethi, K.; et al. Identification of motor and nonmotor wearing-off in Parkinson’s disease: Comparison of a patient questionnaire versus a clinician assessment. Mov. Disord. 2005, 20, 726–733. [Google Scholar] [CrossRef]
- Visser, M.; Marinus, J.; Stiggelbout, A.M.; Van Hilten, J.J. Assessment of autonomic dysfunction in Parkinson’s disease: The SCOPA-AUT. Mov. Disord. 2004, 19, 1306–1312. [Google Scholar] [CrossRef]
- Schuurmans, A.A.T.; De Looff, P.; Nijhof, K.S.; Rosada, C.; Scholte, R.H.J.; Popma, A.; Otten, R. Validity of the Empatica E4 wristband to measure heart rate variability (HRV) parameters: A comparison to electrocardiography (ECG). J. Med. Syst. 2020, 44, 190. [Google Scholar] [CrossRef]
- Milstein, N.; Gordon, I. Validating measures of electrodermal activity and heart rate variability derived from the empatica e4 utilized in research settings that involve interactive dyadic states. Front. Behav. Neurosci. 2020, 14, 148. [Google Scholar] [CrossRef]
- Crochiere, R.E.; Rabiner, L.R. Multirate Digital Signal Processing; Prentice-Hall: Englewood Cliffs, NJ, USA, 1983; Volume 18. [Google Scholar]
- Diez, P.F.; Mut, V.; Laciar, E.; Torres, A.; Avila, E. Application of the empirical mode decomposition to the extraction of features from EEG signals for mental task classification. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009. [Google Scholar]
- Rilling, G.; Flandrin, P.; Goncalves, P. On empirical mode decomposition and its algorithms. In Proceedings of the IEEE-EURASIP Workshop on Nonlinear Signal and Image Processing, Trieste, Italy, 8–11 June 2003. [Google Scholar]
- Zhao, M.; Liu, J.; Wang, Y.; Zhu, H. On the EMD sifting property and instantaneous parameters. Adv. Data Sci. Adapt. Anal. 2016, 8, 1650010. [Google Scholar] [CrossRef]
- Lee, S.; Liu, A.; Wang, Z.J.; McKeown, M.J. Abnormal phase coupling in Parkinson’s disease and normalization effects of subthreshold vestibular stimulation. Front. Hum. Neurosci. 2019, 13, 118. [Google Scholar] [CrossRef] [Green Version]
- Marsden, C.; Parkes, J. Success and problems of long-term levodopa therapy in Parkinson’s disease. Lancet 1977, 309, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Parkinson Study Group. Pramipexole vs levodopa as initial treatment for Parkinson disease: A randomized controlled trial. JAMA 2000, 284, 1931–1938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stacy, M.; Hauser, R. Development of a patient questionnaire to facilitate recognition of motor and non-motor wearing-off in Parkinson’s disease. J. Neural Transm. 2007, 114, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Violante, M.; Ospina-García, N.; Dávila-Avila, N.M.; Cruz-Fino, D.; De La Cruz-Landero, A.; Cervantes-Arriaga, A. Motor and non-motor wearing-off and its impact in the quality of life of patients with Parkinson’s disease. Arq. Neuro-Psiquiatr. 2018, 76, 517–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esen, F.; Çelebi, G.; Ertekin, C.; Çolakoglu, Z.; Çolakoǧlu, Z. Electrodermal activity in patients with Parkinson’s disease. Clin. Auton. Res. 1997, 7, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Pursiainen, V.; Haapaniemi, T.H.; Korpelainen, J.T.; Sotaniemi, K.A.; Myllylä, V.V. Sweating in Parkinsonian patients with wearing-off. Mov. Disord. 2007, 22, 828–832. [Google Scholar] [CrossRef]
- Suzuki, M.; Nakamura, T.; Hirayama, M.; Ueda, M.; Katsuno, M.; Sobue, G. Cardiac parasympathetic dysfunction in the early phase of Parkinson’s disease. J. Neurol. 2017, 264, 333–340. [Google Scholar] [CrossRef]
- Woodrow, H.; Horne, M.K.; Fernando, C.V.; Kotschet, K.E. A blinded, controlled trial of objective measurement in Parkinson’s disease. NPJ Park. Dis. 2020, 6, 35. [Google Scholar] [CrossRef]
- Farzanehfar, P.; Woodrow, H.; Horne, M. Sensor Measurements Can Characterize Fluctuations and Wearing Off in Parkinson’s Disease and Guide Therapy to Improve Motor, Non-motor and Quality of Life Scores. Front. Aging Neurosci. 2022, 14, 852992. [Google Scholar] [CrossRef]
- Farzanehfar, P.; Woodrow, H.; Horne, M. Assessment of Wearing Off in Parkinson’s disease using objective measurement. J. Neurol. 2021, 268, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Nakamura, T.; Hirayama, M.; Ueda, M.; Hatanaka, M.; Harada, Y.; Nakatochi, M.; Nakatsubo, D.; Maesawa, S.; Saito, R.; et al. Wearable sensor device-based detection of decreased heart rate variability in Parkinson’s disease. J. Neural Transm. 2022, 129, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Stacy, M. The wearing-off phenomenon and the use of questionnaires to facilitate its recognition in Parkinson’s disease. J. Neural Transm. 2010, 117, 837–846. [Google Scholar] [CrossRef]
- Raudino, F. Non motor off in Parkinson’s disease. Acta Neurol. Scand. 2001, 104, 312–315. [Google Scholar] [CrossRef] [PubMed]
- Pursiainen, V.; Korpelainen, J.T.; Haapaniemi, T.H.; Sotaniemi, K.A.; Myllylä, V.V. Blood pressure and heart rate in parkinsonian patients with and without wearing-off. Eur. J. Neurol. 2007, 14, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Ossig, C.; Gandor, F.; Fauser, M.; Bosredon, C.; Churilov, L.; Reichmann, H.; Horne, M.K.; Ebersbach, G.; Storch, A. Correlation of quantitative motor state assessment using a kinetograph and patient diaries in advanced PD: Data from an observational study. PLoS ONE 2016, 11, e0161559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maier, F.; Prigatano, G.P. Impaired self-awareness of motor disturbances in Parkinson’s disease. Arch. Clin. Neuropsychol. 2017, 32, 802–809. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject No. | Age (Years) | Sex | Disease Duration (Years) | UPDRS3 | MoCA | BDI-II |
|---|---|---|---|---|---|---|
| 1 | 62 | Female | 3 | 10 | Unavailable | 7 |
| 2 | 60 | Male | 7 | 24 | 29 | 5 |
| 3 | 43 | Male | 5 | 0 | Unavailable | 13 |
| 4 | 64 | Male | 15 | 8 | 29 | 0 |
| 5 | 72 | Male | 13 | 50 | 28 | 4 |
| 6 | 74 | Female | 13 | 8 | 27 | 6 |
| 7 | 36 | Male | 12 | 11 | 30 | 8 |
| 8 | 72 | Male | 13 | 26 | 29 | 9 |
| 9 | 64 | Female | 11 | 21 | 29 | 4 |
| 10 | 54 | Male | 6 | 36 | 30 | 8 |
| 11 | 67 | Female | 4 | 40 | 26 | 6 |
| 12 | 58 | Male | 6 | 36 | 22 | 14 |
| Sensor Signal | Mean and STD of Correlation |
|---|---|
| EDA | Mean = 0.71, STD = 0.14 |
| HR | Mean = 0.57, STD = 0.15 |
| TEMP | Mean = 0.51, STD = 0.26 |
| BVP | Mean = 0.65, STD = 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arasteh, E.; Mirian, M.S.; Verchere, W.D.; Surathi, P.; Nene, D.; Allahdadian, S.; Doo, M.; Park, K.W.; Ray, S.; McKeown, M.J. An Individualized Multi-Modal Approach for Detection of Medication “Off” Episodes in Parkinson’s Disease via Wearable Sensors. J. Pers. Med. 2023, 13, 265. https://doi.org/10.3390/jpm13020265
Arasteh E, Mirian MS, Verchere WD, Surathi P, Nene D, Allahdadian S, Doo M, Park KW, Ray S, McKeown MJ. An Individualized Multi-Modal Approach for Detection of Medication “Off” Episodes in Parkinson’s Disease via Wearable Sensors. Journal of Personalized Medicine. 2023; 13(2):265. https://doi.org/10.3390/jpm13020265
Chicago/Turabian StyleArasteh, Emad, Maryam S. Mirian, Wyatt D. Verchere, Pratibha Surathi, Devavrat Nene, Sepideh Allahdadian, Michelle Doo, Kye Won Park, Somdattaa Ray, and Martin J. McKeown. 2023. "An Individualized Multi-Modal Approach for Detection of Medication “Off” Episodes in Parkinson’s Disease via Wearable Sensors" Journal of Personalized Medicine 13, no. 2: 265. https://doi.org/10.3390/jpm13020265