
Robotic Surgery and Functional Esophageal Disorders: A Systematic Review and Meta-Analysis
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Eligibility Criteria
2.2. Data Extraction and Assessment of Risk of Bias in Included Studies
2.3. Statistical Analysis
3. Results
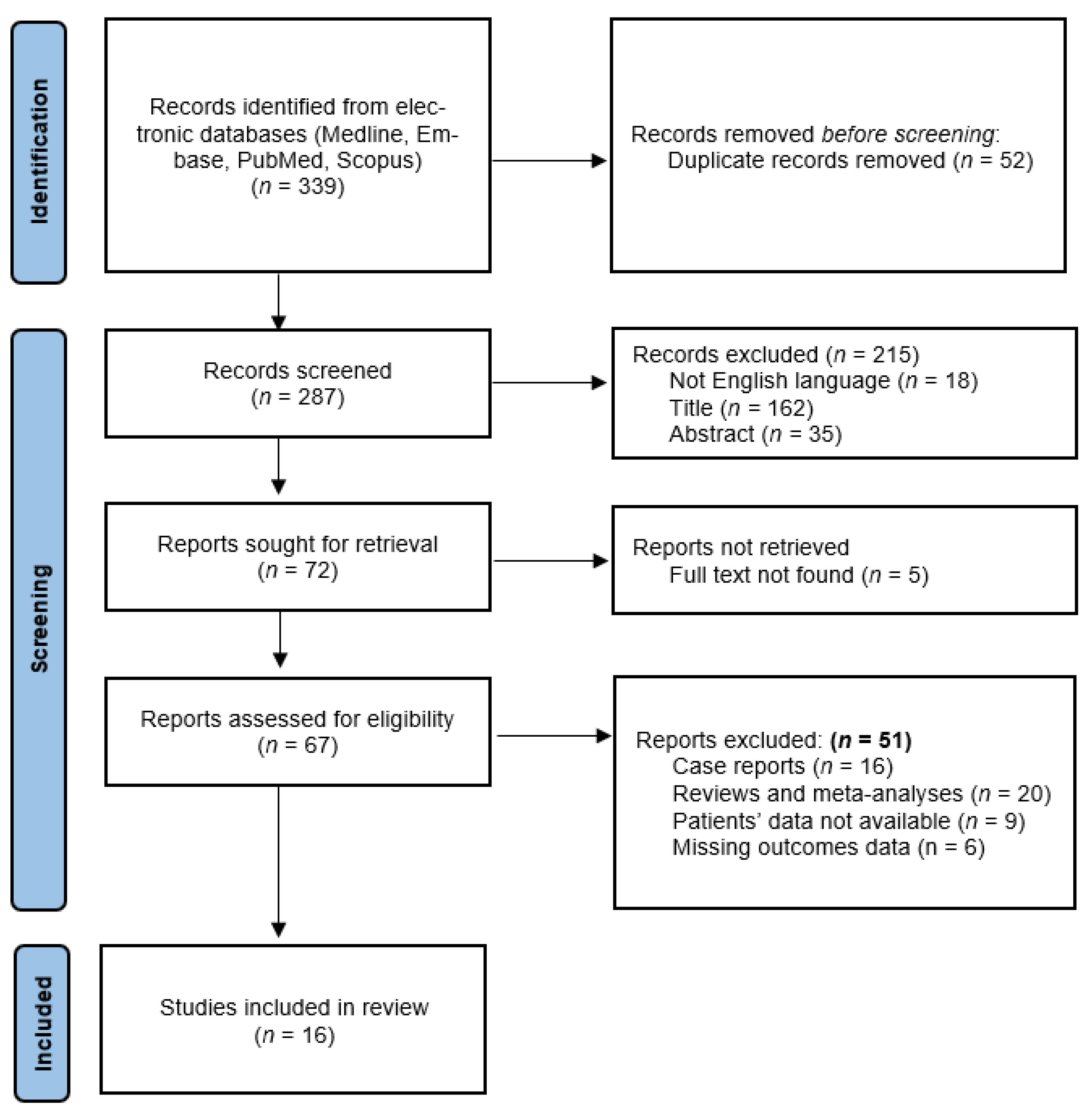
3.1. Study Selection
3.2. Baseline Characteristics of the Included Studies
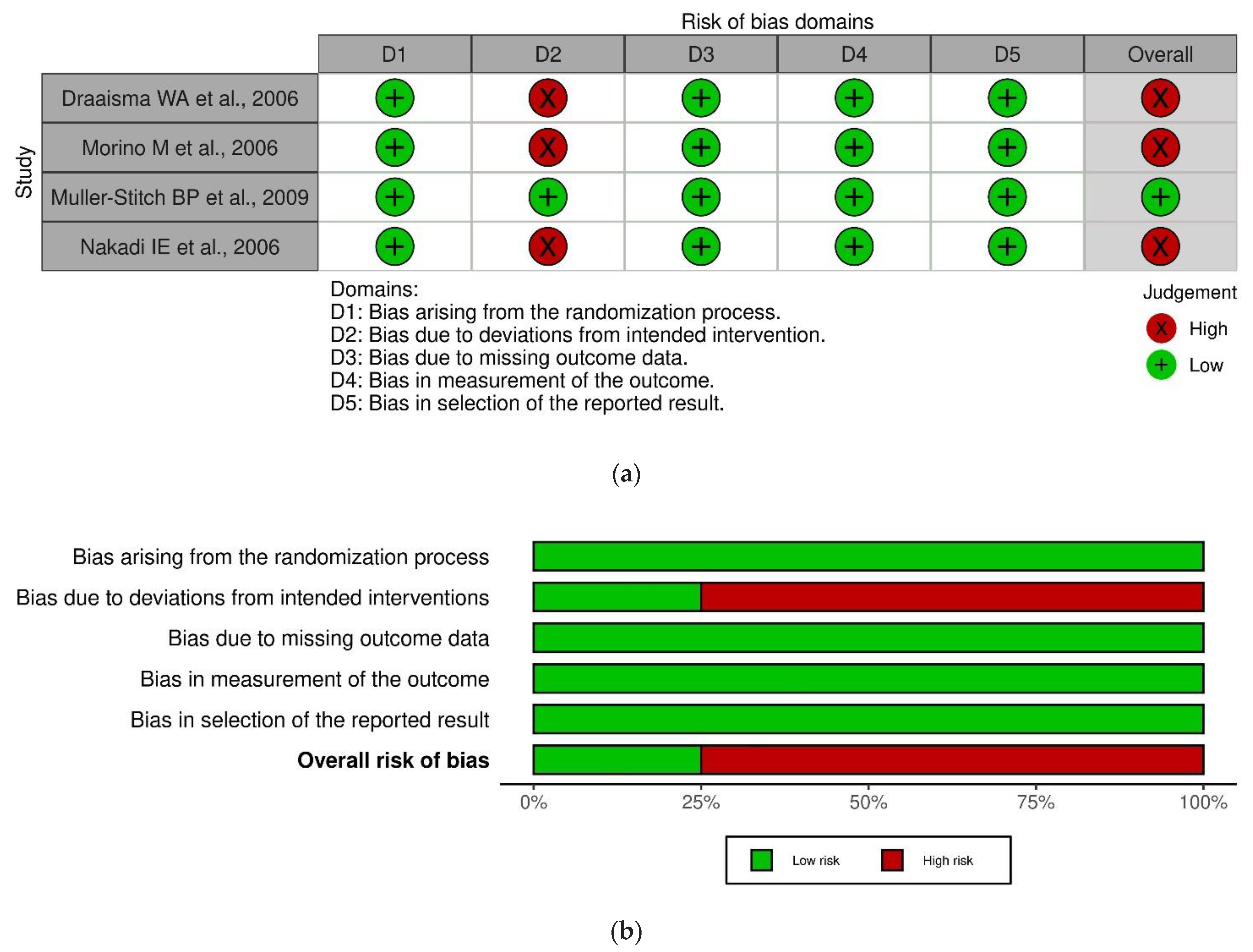
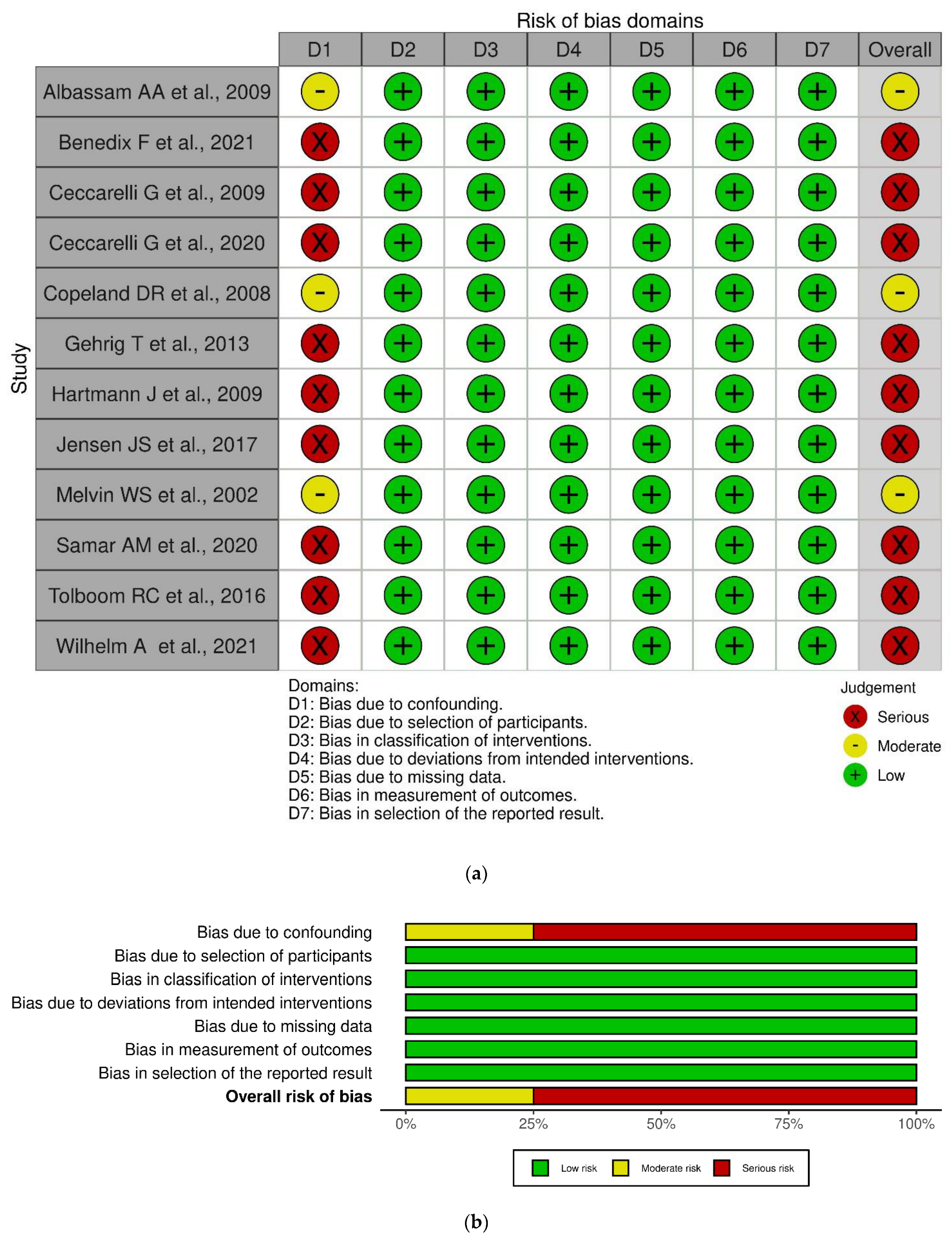
3.3. Risk of Bias
3.4. Primary Outcomes
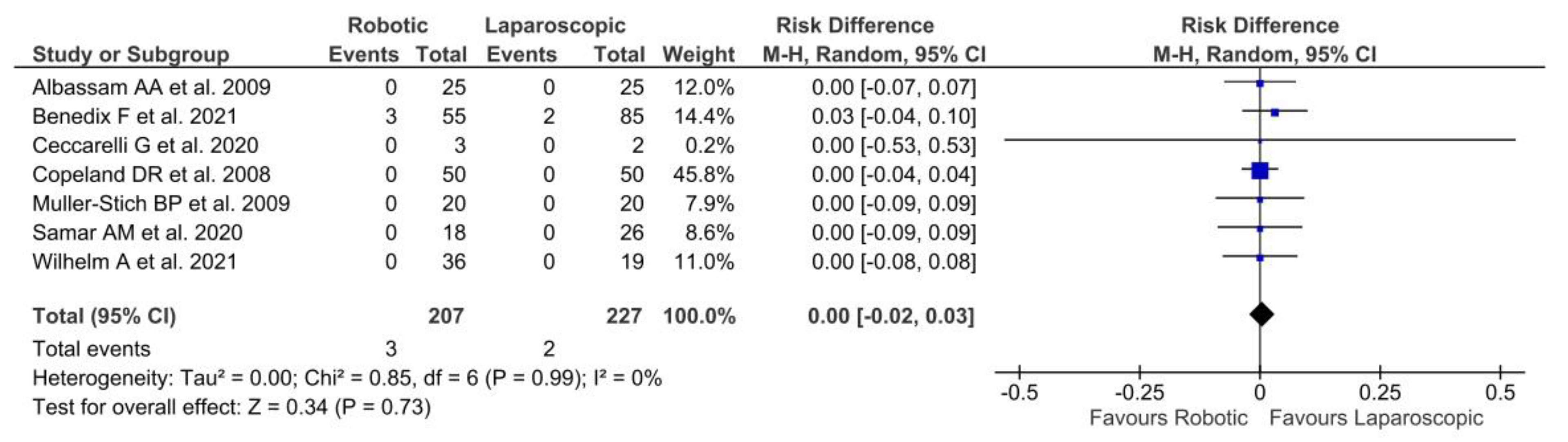
3.4.1. 30-Days Readmission Rates
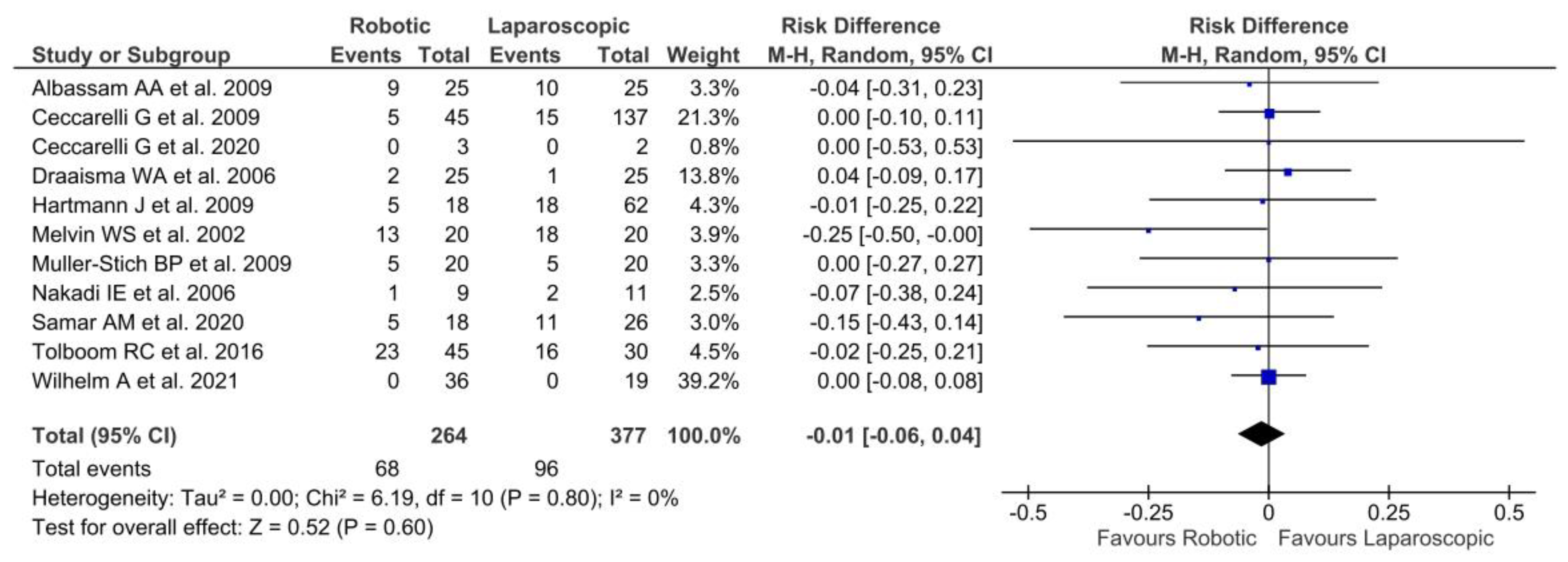
3.4.2. Persistence of Symptoms
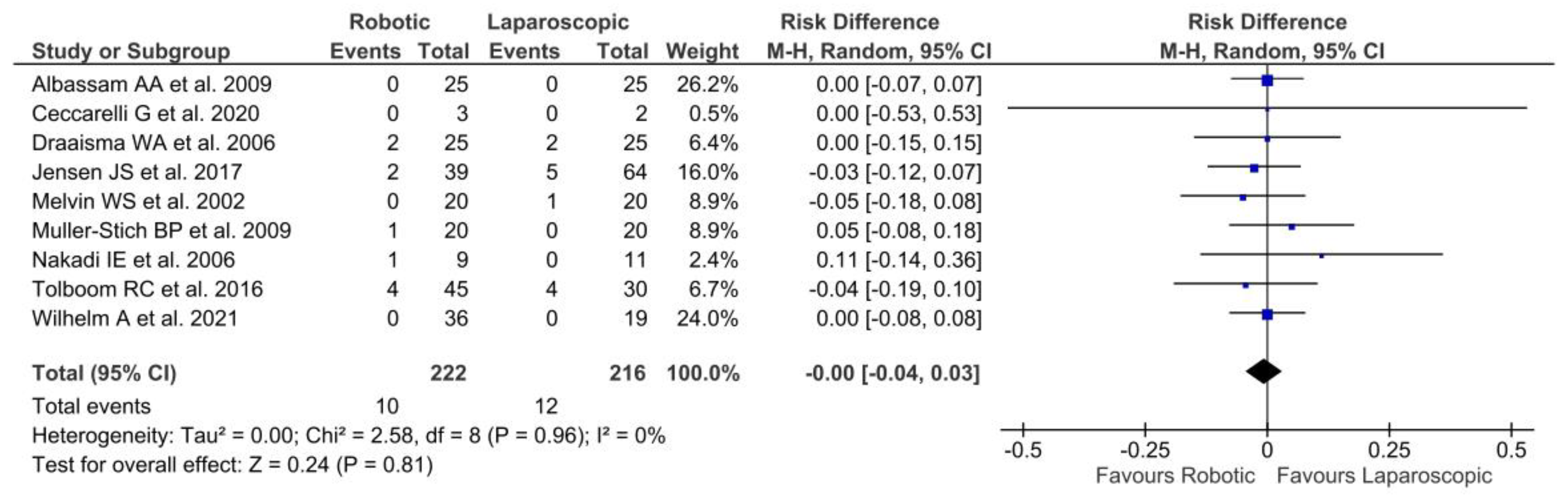
3.4.3. Recurrence
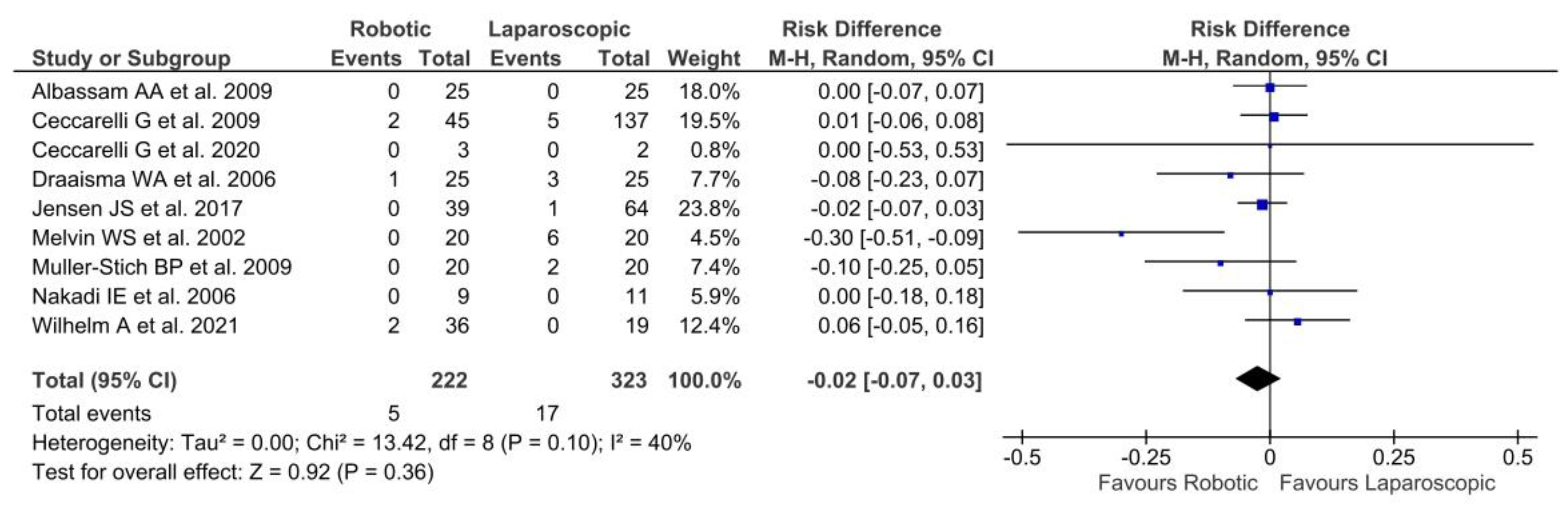
3.4.4. Reoperation
3.5. Publication Bias
4. Discussion
- -
- the functional outcomes obtained by a laparoscopic versus robotic approach.
- -
- data concerning a follow-up longer than 5 years for both medical and surgicalapproach.
- -
- indications and parameters for GERD-surgery.
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darling, G.; Deschamps, C. Technical Controversies in Fundoplication Surgery. Thorac. Surg. Clin. 2005, 15, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Dallemagne, B.; Weerts, J.M.; Jehaes, C.; Markiewicz, S.; Lombard, R. Laparoscopic Nissen fundoplication: Preliminary report. Surg. Laparosc. Endosc. 1991, 1, 138–143. [Google Scholar] [PubMed]
- Wright, A.S.; Gould, J.C.; Melvin, W.S. Computer-assisted robotic antireflux surgery. Minerva Gastroenterol. E Dietol. 2004, 50, 253–260. [Google Scholar]
- Lunca, S.; Bouras, G.; Stanescu, A.C. Gastrointestinal robot-assisted surgery. A current perspective. Rom. J. Gastroenterol. 2005, 14, 385–391. [Google Scholar] [PubMed]
- Cadière, G.B.; Himpens, J.; Vertruyen, M.; Bruyns, J.; Fourtanier, G. Fundoplicature Selon Nissen Réalisée à Distance Du Pa-tient Par Robotique [Nissen Fundoplication Done by Remotely Controlled Robotic Technique]. Ann. Chir. 1999, 53, 137–141. [Google Scholar]
- Ruurda, J.P.; Draaisma, W.A.; van Hillegersberg, R.; Rinkes, I.H.B.; Gooszen, H.G.; Janssen, L.W.; Simmermacher, R.K.; Broeders, I.A. Robot-Assisted Endoscopic Surgery: A Four-Year Single-Center Experience. Dig. Surg. 2005, 22, 313–320. [Google Scholar] [CrossRef]
- Brenkman, H.J.; Parry, K.; van Hillegersberg, R.; Ruurda, J.P. Robot-Assisted Laparoscopic Hiatal Hernia Repair: Promising Anatomical and Functional Results. J. Laparoendosc. Adv. Surg. Tech. 2016, 26, 465–469. [Google Scholar] [CrossRef]
- Falkenback, D.; Lehane, C.W.; Lord, R.V.N. Robot-assisted oesophageal and gastric surgery for benign disease: Antireflux operations and Heller’s myotomy. ANZ J. Surg. 2014, 85, 113–120. [Google Scholar] [CrossRef]
- Kastenmeier, A.; Gonzales, H.; Gould, J.C. Robotic Applications in the Treatment of Diseases of the Esophagus. Surg. Laparosc. Endosc. Percutaneous Tech. 2012, 22, 304–309. [Google Scholar] [CrossRef]
- Mi, J.; Kang, Y.; Chen, X.; Wang, B.; Wang, Z. Whether robot-assisted laparoscopic fundoplication is better for gastroesophageal reflux disease in adults: A systematic review and meta-analysis. Surg. Endosc. 2010, 24, 1803–1814. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE Reporting Guidelines for Meta-analyses of Observational Studies. JAMA Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messori, A.; Maratea, D.; Fadda, V.; Trippoli, S. Using risk difference as opposed to odds-ratio in meta-analysis. Int. J. Cardiol. 2013, 164, 127. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res. Methodol. 2014, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, T.A.; Barbui, C.; Cipriani, A.; Brambilla, P.; Watanabe, N. Imputing missing standard deviations in meta-analyses can provide accurate results. J. Clin. Epidemiol. 2006, 59, 7–10. [Google Scholar] [CrossRef]
- Barili, F.; Parolari, A.; Kappetein, P.; Freemantle, N. Statistical Primer: Heterogeneity, random- or fixed-effects model analyses? Interact. Cardiovasc. Thorac. Surg. 2018, 27, 317–321. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Papers Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albassam, A.A.; Mallick, M.S.; Gado, A.; Shoukry, M. Nissen Fundoplication, Robotic-assisted Versus Laparoscopic Procedure: A Comparative Study in Children. Eur. J. Pediatr. Surg. 2009, 19, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Benedix, F.; Adolf, D.; Peglow, S.; Gstettenbauer, L.M.; Croner, R. Short-term outcome after robot-assisted hiatal hernia and anti-reflux surgery—Is there a benefit for the patient? Langenbeck’s Arch. Surg. 2021, 406, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Patriti, A.; Biancafarina, A.; Spaziani, A.; Bartoli, A.; Bellochi, R.; Casciola, L. Intraoperative and Postoperative Outcome of Robot-Assisted and Traditional Laparoscopic Nissen Fundoplication. Eur. Surg. Res. 2009, 43, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Ceccarelli, G.; Pasculli, A.; Bugiantella, W.; De Rosa, M.; Catena, F.; Rondelli, F.; Costa, G.; Rocca, A.; Longaroni, M.; Testini, M. Minimally invasive laparoscopic and robot-assisted emergency treatment of strangulated giant hiatal hernias: Report of five cases and literature review. World J. Emerg. Surg. 2020, 15, 1–12. [Google Scholar] [CrossRef]
- Copeland, D.R.; Boneti, C.; Kokoska, E.R.; Jackson, R.J.; Smith, S.D. Evaluation of Initial Experience and Comparison of the da Vinci Surgical System With Established Laparoscopic and Open Pediatric Nissen Fundoplication Surgery. JSLS J. Soc. Laparosc. Robot. Surg. 2008, 12, 238–240. [Google Scholar]
- Draaisma, W.A.; Ruurda, J.P.; Scheffer, R.C.H.; Simmermacher, R.K.J.; Gooszen, H.G.; Jong, H.G.R.; Buskens, E.; Broeders, I.A.M.J. Randomized clinical trial of standard laparoscopic versus robot-assisted laparoscopic Nissen fundoplication for gastro-oesophageal reflux disease. Br. J. Surg. 2006, 93, 1351–1359. [Google Scholar] [CrossRef] [Green Version]
- Gehrig, T.; Mehrabi, A.; Fischer, L.; Kenngott, H.; Hinz, U.; Gutt, C.N.; Müller-Stich, B.P. Robotic-assisted paraesophageal hernia repair—A case–control study. Langenbeck’s Arch. Surg. 2012, 398, 691–696. [Google Scholar] [CrossRef]
- Hartmann, J.; Menenakos, C.; Ordemann, J.; Nocon, M.; Raue, W.; Braumann, C. Long-term results of quality of life after standard laparoscopic vs. robot-assisted laparoscopic fundoplications for gastro-oesophageal reflux disease. A comparative clinical trial. Int. J. Med Robot. Comput. Assist. Surg. 2009, 5, 32–37. [Google Scholar] [CrossRef]
- Jensen, J.S.; Antonsen, H.K.; Durup, J. Two years of experience with robot-assisted anti-reflux surgery: A retrospective cohort study. Int. J. Surg. 2017, 39, 260–266. [Google Scholar] [CrossRef]
- Melvin, W. Computer-Enhanced vs. Standard Laparoscopic Antireflux Surgery. J. Gastrointest. Surg. 2002, 6, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Morino, M.; Pellegrino, L.; Giaccone, C.; Garrone, C.; Rebecchi, F. Randomized clinical trial of robot-assisted versus laparoscopic Nissen fundoplication. Br. J. Surg. 2006, 93, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Müller-Stich, B.P.; Reiter, M.A.; Mehrabi, A.; Wente, M.N.; Fischer, L.; Köninger, J.; Gutt, C.N. No relevant difference in quality of life and functional outcome at 12 months’ follow-up—A randomised controlled trial comparing robot-assisted versus conventional laparoscopic Nissen fundoplication. Langenbeck’s Arch. Surg. 2009, 394, 441–446. [Google Scholar] [CrossRef]
- El Nakadi, I.; Mélot, C.; Closset, J.; De Moor, V.; Bétroune, K.; Feron, P.; Lingier, P.; Gelin, M. Evaluation of da Vinci Nissen Fundoplication Clinical Results and Cost Minimization. World J. Surg. 2006, 30, 1050–1054. [Google Scholar] [CrossRef]
- Samar, A.M.; Bond, A.; Ranaboldo, C. Comparison of FreeHand® robot-assisted with human-assisted laparoscopic fundoplication. Minim. Invasive Ther. Allied Technol. 2020, 31, 24–27. [Google Scholar] [CrossRef]
- Tolboom, R.C.; Draaisma, W.A.; Broeders, I.A.M.J. Evaluation of conventional laparoscopic versus robot-assisted laparoscopic redo hiatal hernia and antireflux surgery: A cohort study. J. Robot. Surg. 2016, 10, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilhelm, A.; Nocera, F.; Schneider, R.; Koechlin, L.; Daume, D.L.; Fourie, L.; Steinemann, D.; von Flüe, M.; Peterli, R.; Angehrn, F.V.; et al. Robot-assisted vs. laparoscopic repair of complete upside-down stomach hiatal hernia (the RATHER-study): A prospective comparative single center study. Surg. Endosc. 2021, 1–9. [Google Scholar] [CrossRef]
- Jayne, D.; Pigazzi, A.; Marshall, H.; Croft, J.; Corrigan, N.; Copeland, J.; Quirke, P.; West, N.; Rautio, T.; Thomassen, N.; et al. Effect of Robotic-Assisted vs Conventional Laparoscopic Surgery on Risk of Conversion to Open Laparotomy Among Patients Undergoing Resection for Rectal Cancer: The ROLARR Randomized Clinical Trial. JAMA 2017, 318, 1569–1580. [Google Scholar] [CrossRef] [PubMed]
- Milone, M.; de’Angelis, N.; Beghdadi, N.; Brunetti, F.; Manigrasso, M.; De Simone, G.; Servillo, G.; Vertaldi, S.; De Palma, G.D. Conversions related to adhesions in abdominal surgery. Robotic versus laparoscopic approach: A multicentre experience. Int. J. Med Robot. Comput. Assist. Surg. 2020, 17, e2186. [Google Scholar] [CrossRef]
- Milone, M.; Manigrasso, M.; Anoldo, P.; D’Amore, A.; Elmore, U.; Giglio, M.C.; Rompianesi, G.; Vertaldi, S.; Troisi, R.I.; Francis, N.K.; et al. The Role of Robotic Visceral Surgery in Patients with Adhesions: A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 307. [Google Scholar] [CrossRef]
- Spechler, S.J. Evaluation and Treatment of Patients with Persistent Reflux Symptoms Despite Proton Pump Inhibitor Treatment. Gastroenterol. Clin. N. Am. 2020, 49, 437–450. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Study Period | Patients (n) | Male/Female (n) | Age (years) (SD) | BMI (kg/m2) (SD) | Diagnosis | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | ||||
| Albassam AA et al., 2009 [22] | Retrospective | Jan. 2005–Jul. 2008 | 50 | 25 | 25 | 9/16 | 11/14 | 3.8 (3.25) | 5.4 (3.42) | 10.9 (4.65) | 10.1 (3.14) | GERD |
| Benedix F et al., 2021 [23] | Retrospective | Jan. 2016–Jul. 2020 | 140 | 85 | 55 | 29/56 | 18/37 | 62.9 (11.6) | 63.5 (12.3) | 29.3 (3.8) | 29.5 (4.4) | Hiatal hernia and GERD |
| Ceccarelli G et al., 2009 [24] | Retrospective | Oct. 1992–Sep. 2007 | 183 | 137 | 45 | - | - | 52.5 (8.3) | 55.0 (11.75) | 27.0 (2.0) | 28.0 (3.0) | GERD |
| Ceccarelli G et al., 2020 [25] | Retrospective | Dec. 2009–Dec. 2019 | 5 | 2 | 3 | 2/0 | 3/0 | 72.5 (13.5) | 68.3 (14.2) | 30.0 (2.6) | 29.1 (5.6) | Giant Hiatal hernia |
| Copeland DR et al., 2008 [26] | Retrospective | 1994–2005 | 100 | 50 | 50 | - | - | 8.9 (5.9) | 9.75 (5.3) | 33.0 (24.0) | 37.0 (23.0) | - |
| Draaisma WA et al., 2006 [27] | RCT | Jan. 2003–Oct. 2005 | 50 | 25 | 25 | 17/8 | 16/9 | 50.5 (12.7) | 39.0 (0.5) | 31.0 (7.0) | 27.0 (4.5) | GERD |
| Gehrig T et al., 2013 [28] | Retrospective | 2003–2007 | 29 | 17 | 12 | 12/5 | 3/9 | 60.2 (11.8) | 68.1 (7.9) | 26.6 (4.4) | 25.4 (2.6) | Paraesophageal hernia |
| Hartmann J et al., 2009 [29] | Retrospective | Jan. 2003–Dec. 2003 | 80 | 62 | 18 | 30/33 | 9/9 | 53.0 (14.0) | 57.0 (13.0) | 30.0 (4.7) | 27.2 (4.3) | GERD |
| Jensen JS et al., 2017 [30] | Retrospective | Apr. 2013–Apr. 2015 | 103 | 64 | 39 | 23/41 | 18/21 | 49.4 (15.4) | 52.0 (14.6) | 26.9 (3.4) | 26.5 (3.1) | GERD |
| Melvin WS et al., 2002 [31] | Prospective | - | 40 | 20 | 20 | 7/13 | 13/7 | 49.6 (0.5) | 42.9 (0.5) | - | - | GERD |
| Morino M et al., 2006 [32] | RCT | - | 50 | 25 | 25 | 18/7 | 19/6 | 46.3 (11.3) | 43.0 (12.8) | 26.1 (2.3) | 25.5 (2.9) | GERD |
| Muller-Stich BP et al., 2009 [33] | RCT | Aug. 2004–Dec. 2005 | 40 | 20 | 20 | 12/8 | 10/10 | 50.5 (12.4) | 49.6 (12.0) | 26.2 (3.4) | 29.2 (5.83) | GERD |
| Nakadi IE et al., 2006 [34] | RCT | - | 20 | 11 | 9 | 8/3 | 6/3 | 48.0 (4.0) | 44.0 (4.0) | 24.8 (0.7) | 25.3 (1.2) | GERD |
| Samar AM et al., 2020 [35] | Retrospective | Jan. 2014–Jun. 2016 | 44 | 26 | 18 | 13/13 | 9/9 | 55.7 (8.2) | 49.2 (7.75) | - | - | - |
| Tolboom RC et al., 2016 [36] | Retrospective | Jan. 2008–Dec. 2013 | 75 | 30 | 45 | 11/19 | 12/33 | 57.2 (2.2) | 56.0 (2.2) | - | - | Hiatal hernia and GERD |
| Wilhelm A et al., 2021 [37] | Prospective | July 2015–June 2019 | 55 | 19 | 36 | 5/14 | 13/23 | 71.7 (13.5) | 69.0 (11.5) | 29.0 (6.5) | 30.0 (3.5) | Hiatal hernia |
| Study | De Novo Surgery | Redo Surgery | Nissen Fundoplication | Dor Fundoplication | Toupet Fundoplication | No Fundoplication | Operative Time (min) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | |
| Albassam AA et al., 2009 [22] | 24 | 24 | 1 | 1 | 25 | 25 | 0 | 0 | 0 | 0 | 0 | 0 | 193.12 (26.6) | 186.04 (21,1) |
| Benedix F et al., 2021 [23] | - | - | - | - | 0 | 0 | 0 | 0 | 85 | 55 | 0 | 0 | 125.0 (35.5) | 149.0 (42.1) |
| Ceccarelli G et al., 2009 [24] | - | - | - | - | 137 | 45 | 0 | 0 | 0 | 0 | 0 | 0 | 86.2 (14.2) | 65.0 (10.8) |
| Ceccarelli G et al., 2020 [25] | 2 | 3 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 165.0 (5.0) | 203.3 (17.8) |
| Copeland DR et al., 2008 [26] | 50 | 50 | 0 | 0 | 50 | 50 | 0 | 0 | 0 | 0 | 0 | 0 | 107.0 (31.0) | 160.0 (61.0) |
| Draaisma WA et al., 2006 [27] | 25 | 25 | 0 | - | 25 | 25 | 0 | 0 | 0 | 0 | 0 | 0 | 115.0 (37.5) | 125.0 (25.0) |
| Gehrig T et al., 2013 [28] | 17 | 12 | 0 | 0 | 9 | 6 | 0 | 0 | 0 | 0 | 8 | 6 | 168.0 (42.0) | 172.0 (31.0) |
| Hartmann J et al., 2009 [29] | 62 | 18 | 0 | 0 | 0 | 0 | 62 | 18 | 0 | 0 | 0 | 0 | 116.0 (63.0) | 207.0 (45.0) |
| Jensen JS et al., 2017 [30] | 64 | 39 | 0 | 0 | 49 | 15 | 0 | 0 | 15 | 24 | 0 | 0 | 86.0 (19.0) | 135.0 (27.0) |
| Melvin WS et al., 2002 [31] | 20 | 20 | 0 | 0 | 17 | 17 | 0 | 0 | 3 | 3 | 0 | 0 | 101.7 (30.7) | 160.2 (45.7) |
| Morino M et al., 2006 [32] | 25 | 25 | 0 | 0 | 25 | 25 | 0 | 0 | 0 | 0 | 0 | 0 | 91.1 (10.6) | 131.6 (18.3) |
| Muller-Stich BP et al., 2009 [33] | 20 | 20 | 0 | 0 | 20 | 20 | 0 | 0 | 0 | 0 | 0 | 0 | 102.0 (19.0) | 88.0 (18.0) |
| Nakadi IE et al., 2006 [34] | 11 | 9 | 0 | 0 | 11 | 9 | 0 | 0 | 0 | 0 | 0 | 0 | 96.0 (5.0) | 137.0 (12.0) |
| Samar AM et al., 2020 [35] | - | - | - | - | 15 | 3 | 7 * | 2 * | 4 | 13 | 0 | 0 | 164.0 (43.0) | 129.0 (22.0) |
| Tolboom RC et al., 2016 [36] | 0 | 0 | 30 | 45 | 6 | 4 | 2 | 12 | 20 | 27 | 1 | 2 | 98.7 (6.2) | 120.0 (2.5) |
| Wilhelm A et al., 2021 [37] | - | - | - | - | 4 | 0 | 0 | 0 | 15 | 29 | 0 | 7 | 179.5 (42.0) | 182.2 (6.9) |
| Study | Mean Follow-Up (months) | 30-days Readmission (n) | Persistence of Symptoms (n) | Delayed Gastrinc Emptying (n) | Pyrosis (n) | Dysphagia (n) | Recurrence (n) | Reoperation (n) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | Lap | Rob | |
| Albassam AA et al., 2009 [22] | 19.25 | 19.25 | 0 | 0 | 10 | 9 | 1 | 2 | - | - | 1 | 0 | 0 | 0 | 0 | 0 |
| Benedix F et al., 2021 [23] | 3 | 3 | 2 | 3 | - | - | 0 | 0 | - | - | 8 | 5 | - | - | 1 | 1 |
| Ceccarelli G et al., 2009 [24] | 93.6 | 43.2 | - | - | 15 | 5 | - | - | - | - | 3 | 1 | 5 | 2 | - | - |
| Ceccarelli G et al., 2020 [25] | 6 | 6 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | - | - | 0 | 0 | 0 | 0 |
| Copeland DR et al., 2008 [26] | 1 | 1 | 0 | 0 | - | - | - | - | - | - | 14 | 15 | - | - | - | - |
| Draaisma WA et al., 2006 [27] | 6 | 6 | - | - | 1 | 2 | - | - | - | - | 2 | 1 | 3 | 1 | 2 | 2 |
| Gehrig T et al., 2013 [28] | - | - | - | - | - | - | 2 | 0 | - | - | - | - | - | - | 0 | 1 |
| Hartmann J et al., 2009 [29] | - | - | - | - | 18 | 5 | - | 0 | - | - | - | - | - | - | - | - |
| Jensen JS et al., 2017 [30] | 22.5 | 26 | - | - | - | - | 0 | 0 | - | - | 4 | 2 | 1 | 0 | 5 | 2 |
| Melvin WS et al., 2002 [31] | 10.5 | 6.7 | - | - | 18 | 13 | - | 0 | 4 | 3 | 5 | 3 | 6 | 0 | 1 | 0 |
| Morino M et al., 2006 [32] | 12 | 12 | - | - | - | - | - | - | 0 | 0 | 0 | 0 | - | - | - | - |
| Muller-Stich BP et al., 2009 [33] | 12 | 12 | 0 | 0 | 5 | 5 | - | - | - | - | 0 | 1 | 2 | 0 | 0 | 1 |
| Nakadi IE et al., 2006 [34] | 12 | 12 | - | - | 2 | 1 | - | - | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Samar AM et al., 2020 [35] | 1 | 1 | - | - | 11 | 5 | - | - | 2 | 2 | 4 | 2 | - | - | - | - |
| Tolboom RC et al., 2016 [36] | 11.7 | 3 | - | - | 16 | 23 | 3 | 3 | 9 | 6 | 3 | 6 | - | - | 4 | 4 |
| Wilhelm A et al., 2021 [37] | 28.7 | 31 | 0 | 0 | 0 | 0 | 0 | 1 | - | - | 1 | 1 | 0 | 2 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vertaldi, S.; D’Amore, A.; Manigrasso, M.; Anoldo, P.; Chini, A.; Maione, F.; Pesce, M.; Sarnelli, G.; De Palma, G.D.; Milone, M. Robotic Surgery and Functional Esophageal Disorders: A Systematic Review and Meta-Analysis. J. Pers. Med. 2023, 13, 231. https://doi.org/10.3390/jpm13020231
Vertaldi S, D’Amore A, Manigrasso M, Anoldo P, Chini A, Maione F, Pesce M, Sarnelli G, De Palma GD, Milone M. Robotic Surgery and Functional Esophageal Disorders: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2023; 13(2):231. https://doi.org/10.3390/jpm13020231
Chicago/Turabian StyleVertaldi, Sara, Anna D’Amore, Michele Manigrasso, Pietro Anoldo, Alessia Chini, Francesco Maione, Marcella Pesce, Giovanni Sarnelli, Giovanni Domenico De Palma, and Marco Milone. 2023. "Robotic Surgery and Functional Esophageal Disorders: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 13, no. 2: 231. https://doi.org/10.3390/jpm13020231