
Comparisons of Mechanical Power and Respiratory Mechanics in Pressure-Controlled Ventilation and Volume-Controlled Ventilation during Laparoscopic Cholecystectomy in Elderly Patients

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Silva, P.L.; Ball, L.; Rocco, P.R.; Pelosi, P. Power to mechanical power to minimize ventilator-induced lung injury? Intensive Care Med. Exp. 2019, 7, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cressoni, M.; Gotti, M.; Chiurazzi, C.; Massari, D.; Algieri, I.; Amini, M.; Cammaroto, A.; Brioni, M.; Montaruli, C.; Nikolla, K.; et al. Mechanical Power and Development of Ventilator-induced Lung Injury. Anesthesiology 2016, 124, 1100–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neto, A.S.; Deliberato, R.O.; Johnson, A.E.W.; Bos, L.D.; Amorim, P.; Pereira, S.M.; Cazati, D.C.; Cordioli, R.L.; Correa, T.D.; Pollard, T.J.; et al. Mechanical power of ventilation is associated with mortality in critically ill patients: An analysis of patients in two observational cohorts. Intensive Care Med. 2018, 44, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Karalapillai, D.; Weinberg, L.; Neto, A.S.; Peyton, P.; Ellard, L.; Hu, R.; Pearce, B.; Tan, C.O.; Story, D.; O’Donnell, M.; et al. Intra-operative ventilator mechanical power as a predictor of postoperative pulmonary complications in surgical patients: A secondary analysis of a randomised clinical trial. Eur. J. Anaesthesiol. 2022, 39, 67–74. [Google Scholar] [CrossRef]
- Santer, P.; Wachtendorf, L.J.; Suleiman, A.; Houle, T.T.; Fassbender, P.; Costa, E.L.; Talmor, D.; Eikermann, M.; Baedorf-Kassis, E.; Schaefer, M.S. Mechanical power during general anesthesia and postoperative respiratory failure: A multicenter retrospective cohort study. Anesthesiology 2022, 137, 41–54. [Google Scholar] [CrossRef]
- Oğurlu, M.; Küçük, M.; Bilgin, F.; Sizlan, A.; Yanarateş, O.; Eksert, S.; Karaşahin, E.; Coşar, A. Pressure-controlled vs. volume-controlled ventilation during laparoscopic gynecologic surgery. J. Minim. Invasive Gynecol. 2010, 17, 295–300. [Google Scholar] [CrossRef]
- Lee, J.M.; Lee, S.K.; Rhim, C.C.; Seo, K.H.; Han, M.; Kim, S.Y.; Park, E.Y. Comparison of volume-controlled, pressure-controlled, and pressure-controlled volume-guaranteed ventilation during robot-assisted laparoscopic gynecologic surgery in the Trendelenburg position. Int. J. Med. Sci. 2020, 17, 2728–2734. [Google Scholar] [CrossRef]
- Schick, V.; Dusse, F.; Eckardt, R.; Kerkhoff, S.; Commotio, S.; Hinkelbein, J.; Mathes, A. Comparison of Volume-Guaranteed or -Targeted, Pressure-Controlled Ventilation with Volume-Controlled Ventilation during Elective Surgery: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 1276. [Google Scholar] [CrossRef]
- Yao, W.; Yang, M.; Cheng, Q.; Shan, S.; Yang, B.; Han, Q.; Ma, J. Effect of Pressure-Controlled Ventilation-Volume Guaranteed on One-Lung Ventilation in Elderly Patients Undergoing Thoracotomy. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e921417-1–e921417-7. [Google Scholar] [CrossRef]
- Chiumello, D.; Gotti, M.; Guanziroli, M.; Formenti, P.; Umbrello, M.; Pasticci, I.; Mistraletti, G.; Busana, M. Bedside calculation of mechanical power during volume- and pressure-controlled mechanical ventilation. Crit. Care 2020, 24, 417. [Google Scholar] [CrossRef]
- Ahn, H.J.; Park, M.; Kim, J.A.; Yang, M.; Yoon, S.; Kim, B.R.; Bahk, J.-H.; Oh, Y.J.; Lee, E.-H. Driving pressure guided ventilation. Korean J. Anesthesiol. 2020, 73, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Urner, M.; Jüni, P.; Hansen, B.; Wettstein, M.S.; Ferguson, N.D.; Fan, E. Time-varying intensity of mechanical ventilation and mortality in patients with acute respiratory failure: A registry-based, prospective cohort study. Lancet Respir. Med. 2020, 8, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Slutsky, A.S.; Ranieri, V.M. Ventilator-induced lung injury. N. Engl. J. Med. 2013, 369, 2126–2136. [Google Scholar] [CrossRef] [Green Version]
- Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.B.P.; Meade, M.O.; Slutsky, A.S.; Brochard, L.; Costa, E.L.V.; Schoenfeld, D.A.; Stewart, T.E.; Briel, M.; Talmor, D.S.; Mercat, A.; et al. Driving Pressure and Survival in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2015, 372, 747–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahetya, S.K.; Goligher, E.C.; Brower, R.G. Fifty Years of Research in ARDS.Setting Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2017, 195, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Hotchkiss, J.R., Jr.; Blanch, L.; Murias, G.; Adams, A.B.; Olson, D.A.; Wangensteen, O.D.; Leo, P.H.; Marini, J.J. Effects of decreased respiratory frequency on ventilator-induced lung injury. Am. J. Respir. Crit. Care Med. 2000, 161, 463–468. [Google Scholar] [CrossRef]
- Tonetti, T.; Vasques, F.; Rapetti, F.; Maiolo, G.; Collino, F.; Romitti, F.; Camporota, L.; Cressoni, M.; Cadringher, P.; Quintel, M.; et al. Driving pressure and mechanical power: New targets for VILI prevention. Ann. Transl. Med. 2017, 5, 286. [Google Scholar] [CrossRef] [Green Version]
- Gattinoni, L.; Tonetti, T.; Cressoni, M.; Cadringher, P.; Herrmann, P.; Moerer, O.; Protti, A.; Gotti, M.; Chiurazzi, C.; Carlesso, E.; et al. Ventilator-related causes of lung injury: The mechanical power. Intensive Care Med. 2016, 42, 1567–1575. [Google Scholar] [CrossRef]
- Giosa, L.; Busana, M.; Pasticci, I.; Bonifazi, M.; Macrì, M.M.; Romitti, F.; Vassalli, F.; Chiumello, D.; Quintel, M.; Marini, J.J.; et al. Mechanical power at a glance: A simple surrogate for volume-controlled ventilation. Intensive Care Med. Exp. 2019, 7, 61. [Google Scholar] [CrossRef]
- Becher, T.; van der Staay, M.; Schädler, D.; Frerichs, I.; Weiler, N. Calculation of mechanical power for pressure-controlled ventilation. Intensive Care Med. 2019, 45, 1321–1323. [Google Scholar] [CrossRef] [PubMed]
- van der Meijden, S.; Molenaar, M.; Somhorst, P.; Schoe, A. Calculating mechanical power for pressure-controlled ventilation. Intensive Care Med. 2019, 45, 1495–1497. [Google Scholar] [CrossRef] [PubMed]
- Baskaran, D.; Kothari, A. Pressure-controlled volume guaranteed mode improves respiratory dynamics during laparoscopic cholecystectomy: A comparison with conventional modes. Anesth. Essays Res. 2018, 12, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-P.; Wang, H.-B.; Liu, Y.-J.; Lou, X.-P.; Wang, X.-D.; Kong, Y. Comparison of Pressure- and Volume-Controlled Ventilation in Laparoscopic Surgery: A Meta-analysis of Randomized Controlled Trial. Clin. Investig. Med. 2015, 38, 119–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.N.; Kim, D.W.; Jeong, M.A.; Sin, Y.H.; Lee, S.K. Comparison of pressure-controlled ventilation with volume-controlled ventilation during one-lung ventilation: A systematic review and meta-analysis. BMC Anesthesiol. 2015, 16, 72. [Google Scholar] [CrossRef] [Green Version]
- Lin, F.; Pan, L.; Huang, B.; Ruan, L.; Liang, R.; Qian, W.; Ge, W. Pressure-controlled versus volume-controlled ventilation during one-lung ventilation in elderly patients with poor pulmonary function. Ann. Thorac. Med. 2014, 9, 203–208. [Google Scholar] [CrossRef]
- Choi, S.; Yang, S.Y.; Choi, G.J.; Kim, B.G.; Kang, H. Comparison of pressure- and volume-controlled ventilation during laparoscopic colectomy in patients with colorectal cancer. Sci. Rep. 2019, 9, 17007. [Google Scholar] [CrossRef] [Green Version]
- Wang, P.; Zhao, S.; Gao, Z.; Hu, J.; Lu, Y.; Chen, J. Use of volume controlled vs. pressure controlled volume guaranteed ventilation in elderly patients undergoing laparoscopic surgery with laryngeal mask airway. BMC Anesthesiol. 2021, 21, 69. [Google Scholar] [CrossRef]
- Neto, A.S.; Hemmes, S.N.; Barbas, C.S.; Beiderlinden, M.; Fernandez-Bustamante, A.; Futier, E.; Gajic, O.; El-Tahan, M.R.; Ghamdi, A.A.; Günay, E.; et al. Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: A meta-analysis of individual patient data. Lancet Respir. Med. 2016, 4, 272–280. [Google Scholar] [CrossRef]
- Caironi, P.; Cressoni, M.; Chiumello, D.A.; Ranieri, M.; Quintel, M.; Russo, S.G.; Cornejo, R.; Bugedo, G.; Carlesso, E.; Russo, R.; et al. Lung Opening and Closing during Ventilation of Acute Respiratory Distress Syndrome. Am. J. Respir. Crit. Care Med. 2010, 181, 578–586. [Google Scholar] [CrossRef]
- Entriken, C.; Pritts, T.A. Perioperative Pulmonary Support of the Elderly. Curr. Geriatr. Rep. 2021, 10, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, T.M.; Giraud, G.D.; Togioka, B.M.; Jones, D.B.; Cigarroa, J.E. Cardiovascular and ventilatory consequences of laparoscopic surgery. Circulation 2017, 135, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.H.; Hahm, T.S.; Kim, J.A.; Sim, W.S.; Choi, D.H.; Lee, E.K.; Lee, S.M. Prolonged inspiratory time produces better gas exchange in patients undergoing laparoscopic surgery: A randomised trial. Acta Anaesthesiol. Scand. 2013, 57, 613–622. [Google Scholar] [CrossRef]
- Bellani, G.; Sosio, S. Plateau Pressure during Pressure Control Ventilation. Aboutopen 2019, 6, 76–77. [Google Scholar] [CrossRef] [Green Version]
- Kalmar, A.F.; Foubert, L.; Hendrickx, J.F.; Mottrie, A.; Absalom, A.; Mortier, E.P.; Struys, M.M. Influence of steep Trendelenburg position and CO2 pneumoperitoneum on cardiovascular, cerebrovascular, and respiratory homeostasis during robotic prostatectomy. Br. J. Anaesth. 2010, 104, 433–439. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
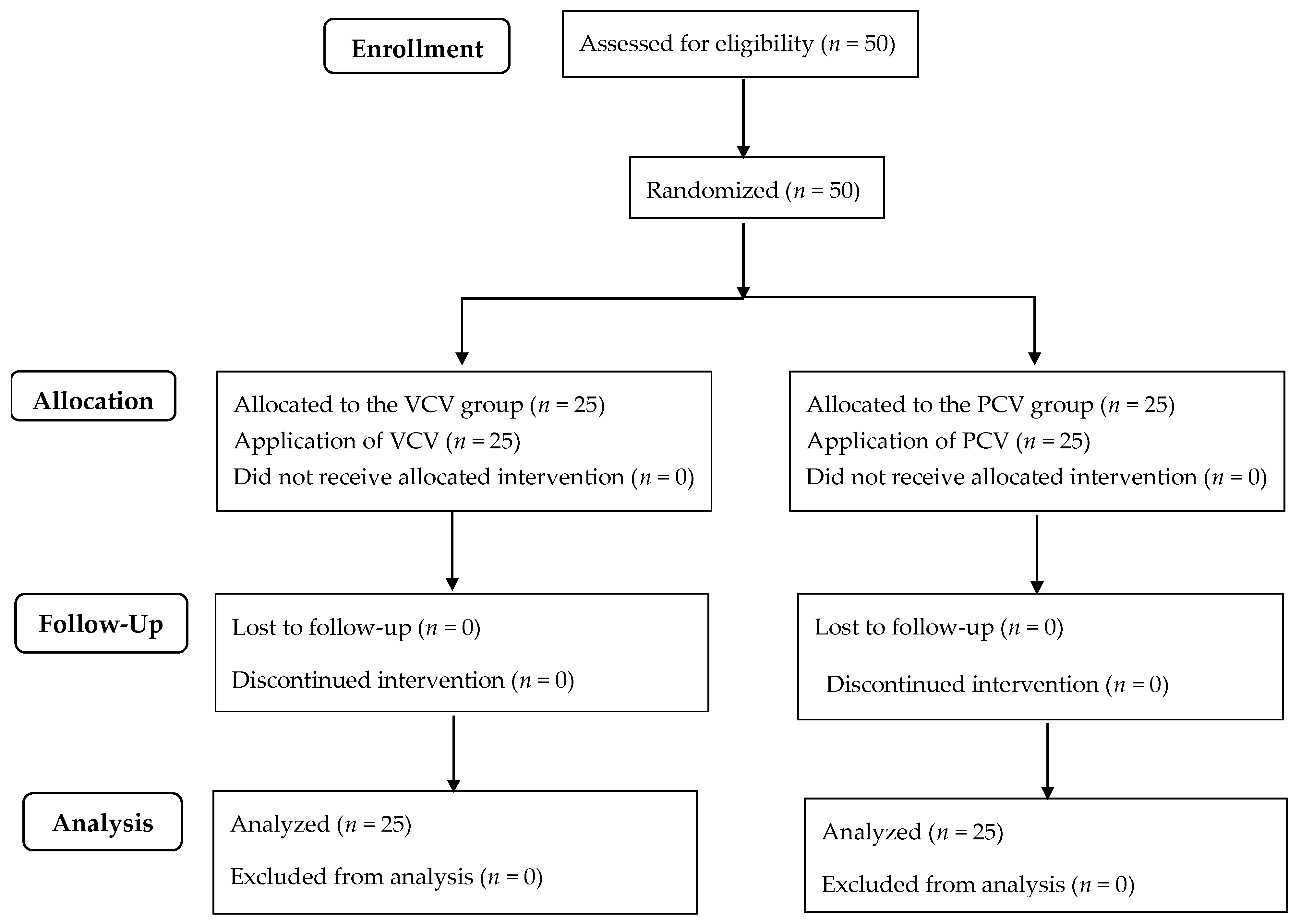
| VCV (n = 25) | PCV (n = 25) | p Value | |
|---|---|---|---|
| Age, years | 70.3 ± 4.7 | 71.8 ± 4.2 | 0.258 |
| Gender, M/F | 10/15 | 17/8 | 0.384 |
| Weight, kg | 62.2 ± 9.9 | 63.5 ± 9.3 | 0.638 |
| Height, cm | 160.9 ± 7.3 | 161. ± 8.0 | 0.941 |
| ASA PS, I/II | 4/21 | 6/19 | 0.363 |
| Anesthesia time, min | 92.5 ± 23.1 | 81.8 ± 19.9 | 0.086 |
| Operation time, min | 63.0 ± 22.9 | 57.4 ± 21.0 | 0.369 |
| Pneumoperitoneum time, min | 48.6 ± 21.5 | 42.0 ± 18.1 | 0.247 |
| Postoperative hospital stay, days | 3 (3–4) | 3 (3–4) | 0.822 |
| Variables | Group | IND | PP15 | PP30 | END | Group * Time |
|---|---|---|---|---|---|---|
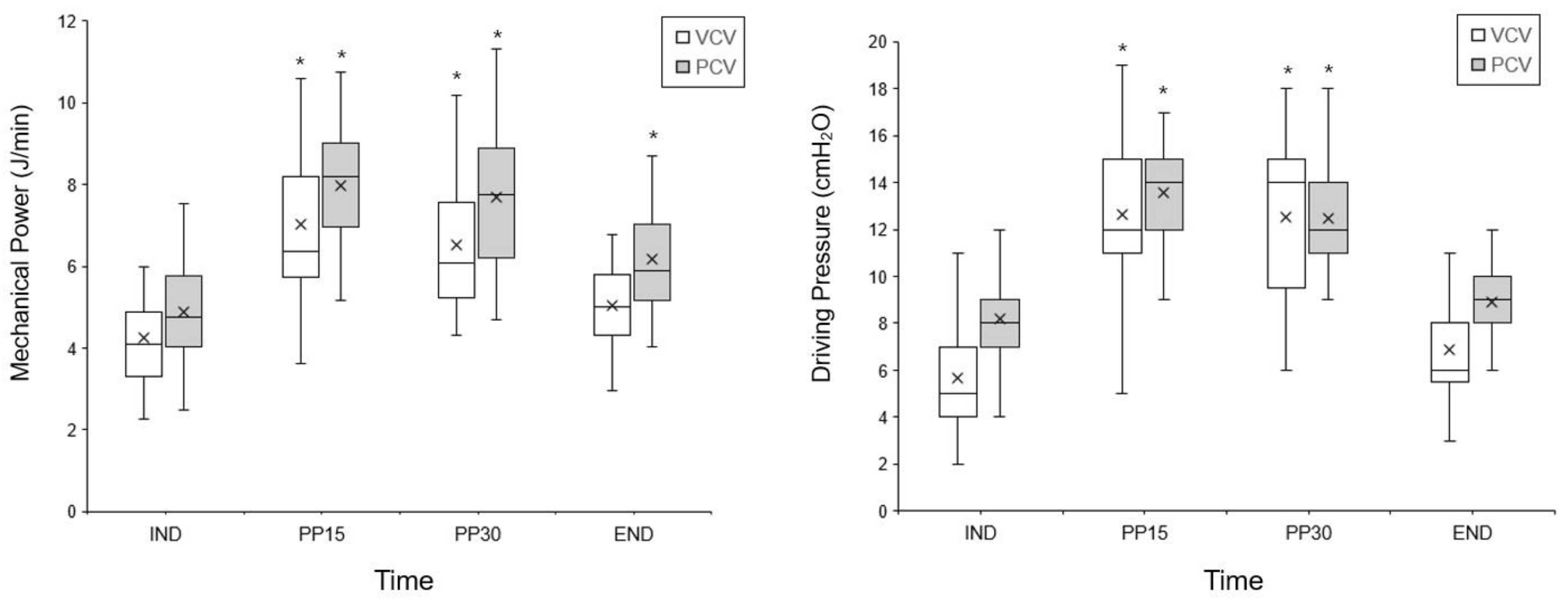
| Dynamic mechanical power, J/min | VCV | 3.6 ± 0.9 | 6.2 ± 1.7 * | 5.9 ± 1.6 * | 4.5 ± 1.1 | 0.007 |
| PCV | 3.5 ± 0.8 | 5.1 ± 1.0 * | 4.9 ± 1.1 * | 4.2 ± 0.8 * | ||
| Dynamic driving pressure, cmH2O | VCV | 9.2 ± 2.5 | 16.6 ± 2.8 * | 16.0 ± 2.7 * | 10.1 ± 1.9 | 0.001 |
| PCV | 8.2 ± 2.2 | 13.6 ± 2.7 * | 12.5 ± 2.5 * | 8.9 ± 1.6 |
| Variables | Group | IND | PP15 | PP30 | END | Group * Time |
|---|---|---|---|---|---|---|
| Tidal volume, mL/min | VCV | 347 ± 52 | 352 ± 48 | 347 ± 47 | 345 ± 54 | 0.089 |
| PCV | 354 ± 67 | 370 ± 56 | 371 ± 55 | 372 ± 59 | ||
| Respiratory rate, breaths/min | VCV | 11 ± 2 | 13 ± 2 * | 13 ± 2 * | 13 ± 2 * | 0.156 |
| PCV | 11 ± 1 | 12 ± 2 | 12 ± 2 | 12 ± 2 | ||
| Peak inspiratory pressure, cmH2O | VCV | 14 ± 2 | 22 ± 3 * | 21 ± 3 * | 15 ± 2 | 0.001 |
| PCV | 13 ± 2 | 19 ± 3 * | 17 ± 3 * | 14 ± 2 | ||
| Minute volume, L/min | VCV | 3.6 ± 0.8 | 4.6 ± 1.1 | 4.6 ± 1.0 | 4.5 ± 1.1 | 0.265 |
| PCV | 3.8 ± 0.7 | 4.5 ± 0.9 | 4.5 ± 0.8 | 4.6 ± 0.8 | ||
| Mean airway pressure, cmH2O | VCV | 8 ± 1 | 11 ± 2 * | 11 ± 1 * | 9 ± 1 | 0.762 |
| PCV | 9 ± 1 | 12 ± 1 * | 12 ± 2 * | 10 ± 1 | ||
| ETCO2, mmHg | VCV | 33 ± 3 | 37 ± 2 * | 37 ± 2 * | 38 ± 3 * | 0.552 |
| PCV | 34 ± 3 | 37 ± 2 * | 37 ± 2 * | 38 ± 3 * | ||
| Measured plateau pressure, cmH2O | VCV | 11 ± 3 | 18 ± 3 * | 18 ± 3 * | 12 ± 2 | |
| PCV | NA | NA | NA | NA | ||
| Dynamic compliance, mL/cmH2O | VCV | 39.7 ± 10.8 | 21.7 ± 4.5 * | 22.5 ± 6.1 * | 35.2 ± 8.1 | 0.524 |
| PCV | 45.6 ± 12.6 | 28.3 ± 7.0 * | 30.7 ± 7.1 * | 43.1 ± 10.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, Y.Y.; Chang, Y.J.; Lee, D.; Kim, Y.B.; Jung, J.; Kwak, H.J. Comparisons of Mechanical Power and Respiratory Mechanics in Pressure-Controlled Ventilation and Volume-Controlled Ventilation during Laparoscopic Cholecystectomy in Elderly Patients. J. Pers. Med. 2023, 13, 201. https://doi.org/10.3390/jpm13020201
Jo YY, Chang YJ, Lee D, Kim YB, Jung J, Kwak HJ. Comparisons of Mechanical Power and Respiratory Mechanics in Pressure-Controlled Ventilation and Volume-Controlled Ventilation during Laparoscopic Cholecystectomy in Elderly Patients. Journal of Personalized Medicine. 2023; 13(2):201. https://doi.org/10.3390/jpm13020201
Chicago/Turabian StyleJo, Youn Yi, Young Jin Chang, Dongchul Lee, Yong Beom Kim, Junsu Jung, and Hyun Jeong Kwak. 2023. "Comparisons of Mechanical Power and Respiratory Mechanics in Pressure-Controlled Ventilation and Volume-Controlled Ventilation during Laparoscopic Cholecystectomy in Elderly Patients" Journal of Personalized Medicine 13, no. 2: 201. https://doi.org/10.3390/jpm13020201