
Quantification of Extracellular Volume in CT in Neoadjuvant Chemotherapy in Breast Cancer: New Frontiers in Assessing the Cardiotoxicity of Anthracyclines and Trastuzumab
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Chemotherapeutic Schemes Used
2.3. CT Acquisition Protocols
- Arterial phase, generally about 15–18 s after contrast injection;
- Portal phase, 1 min after contrast injection;
- Delayed phase, about 5 min after contrast injection.
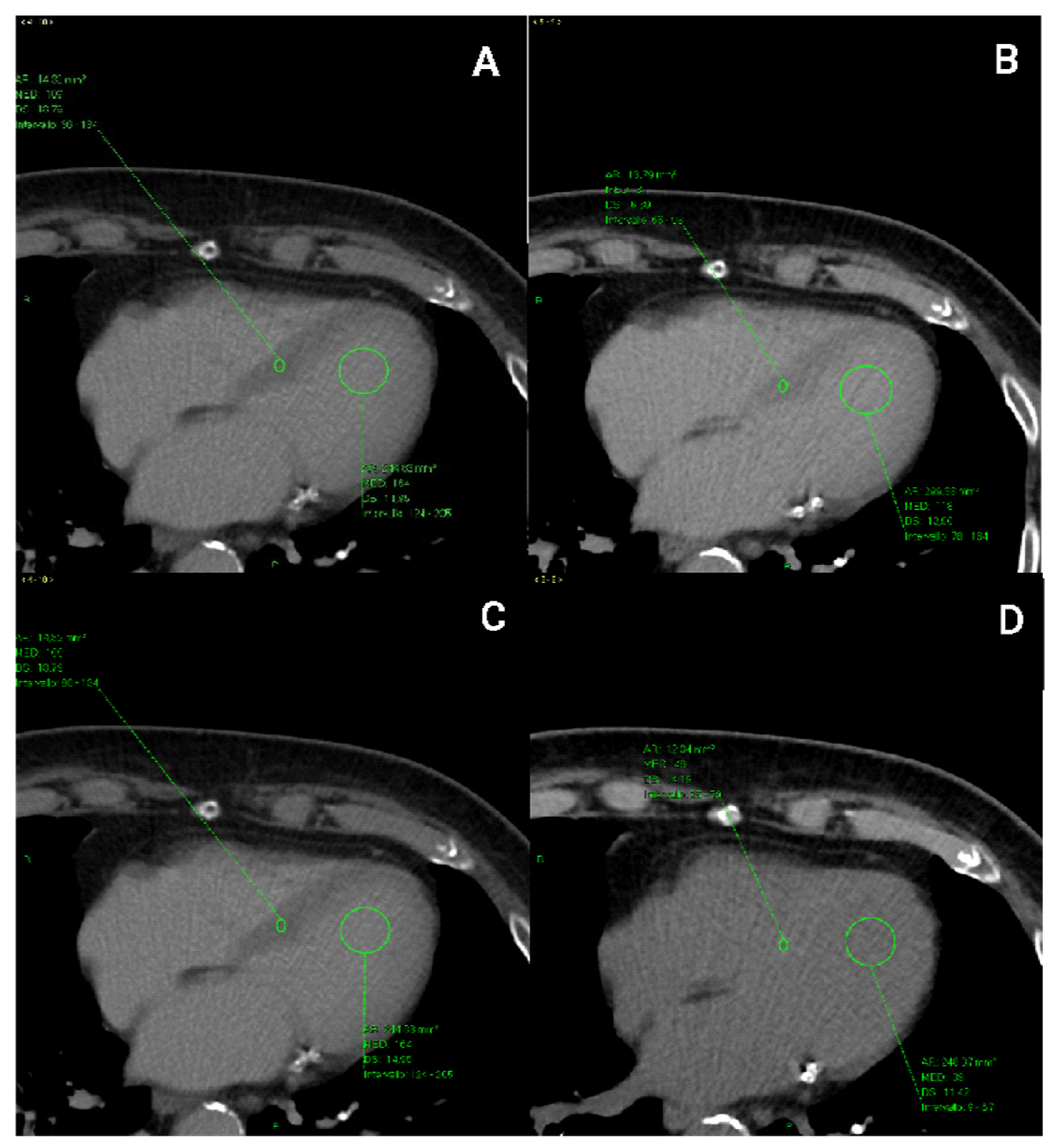
2.4. CT Image Analysis
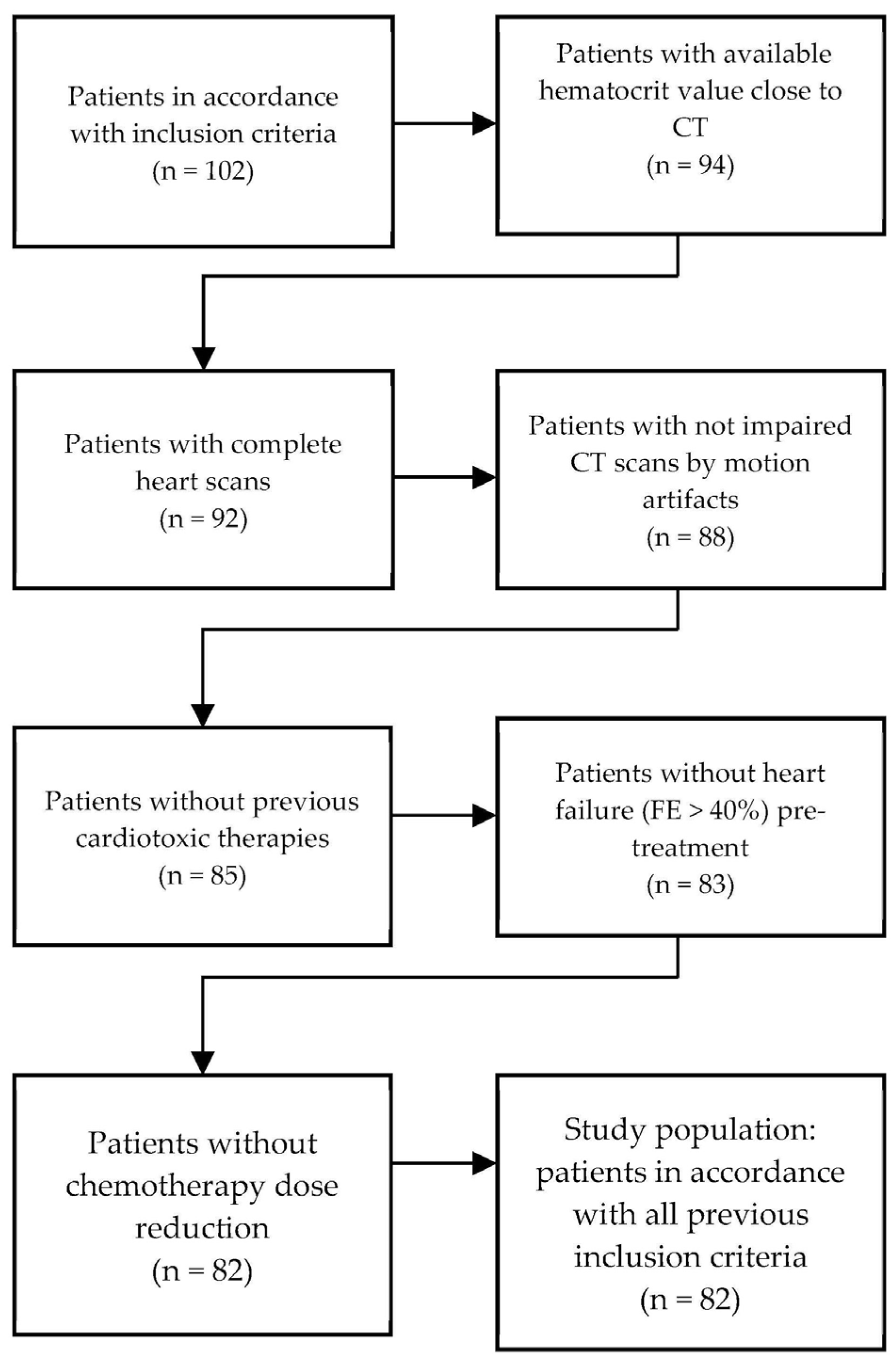
2.5. Participant Selection and Study Population
2.6. Statistical Analysis
3. Results
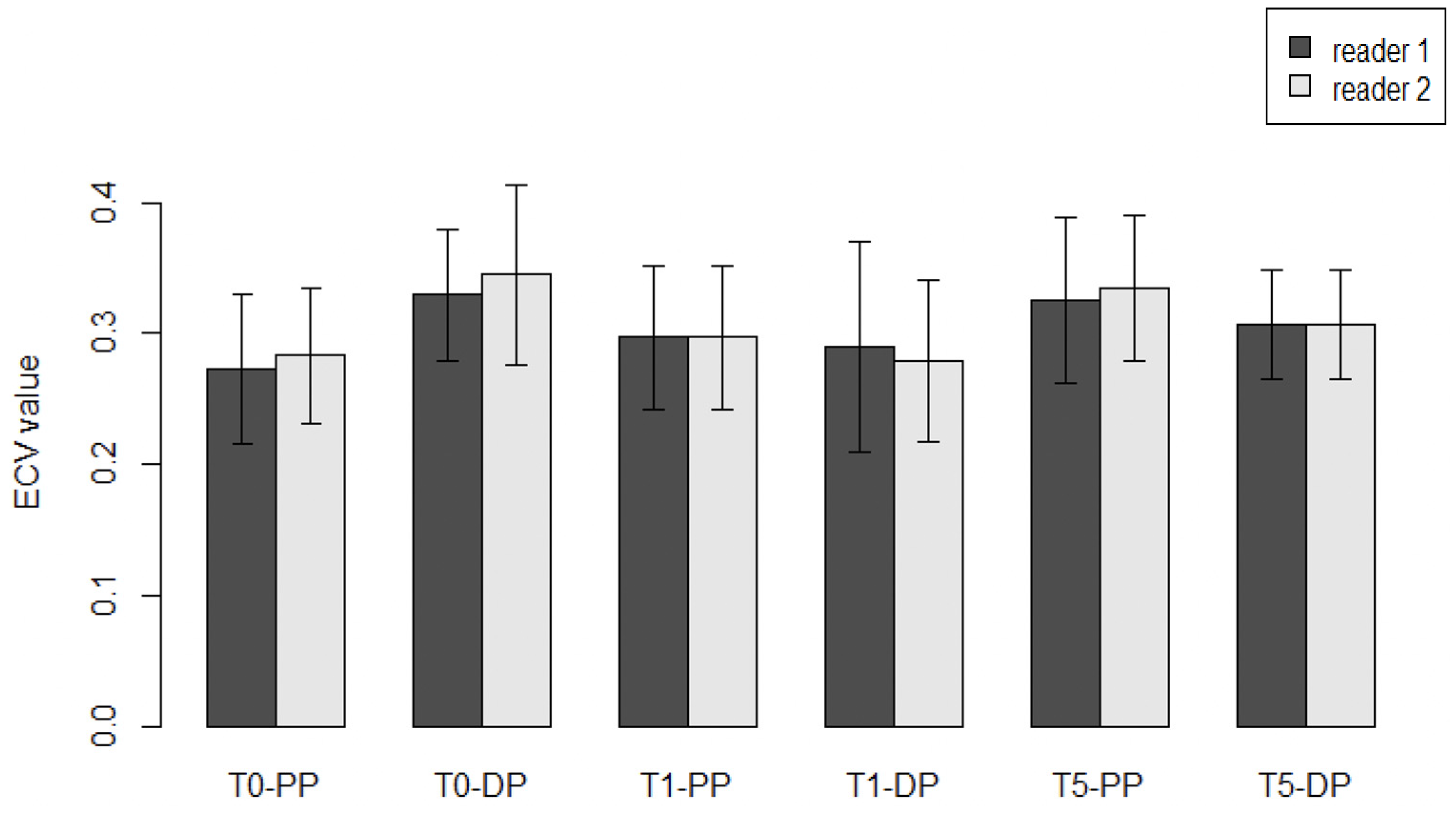
3.1. Inter-Observer Differences and Reproducibility between Operators
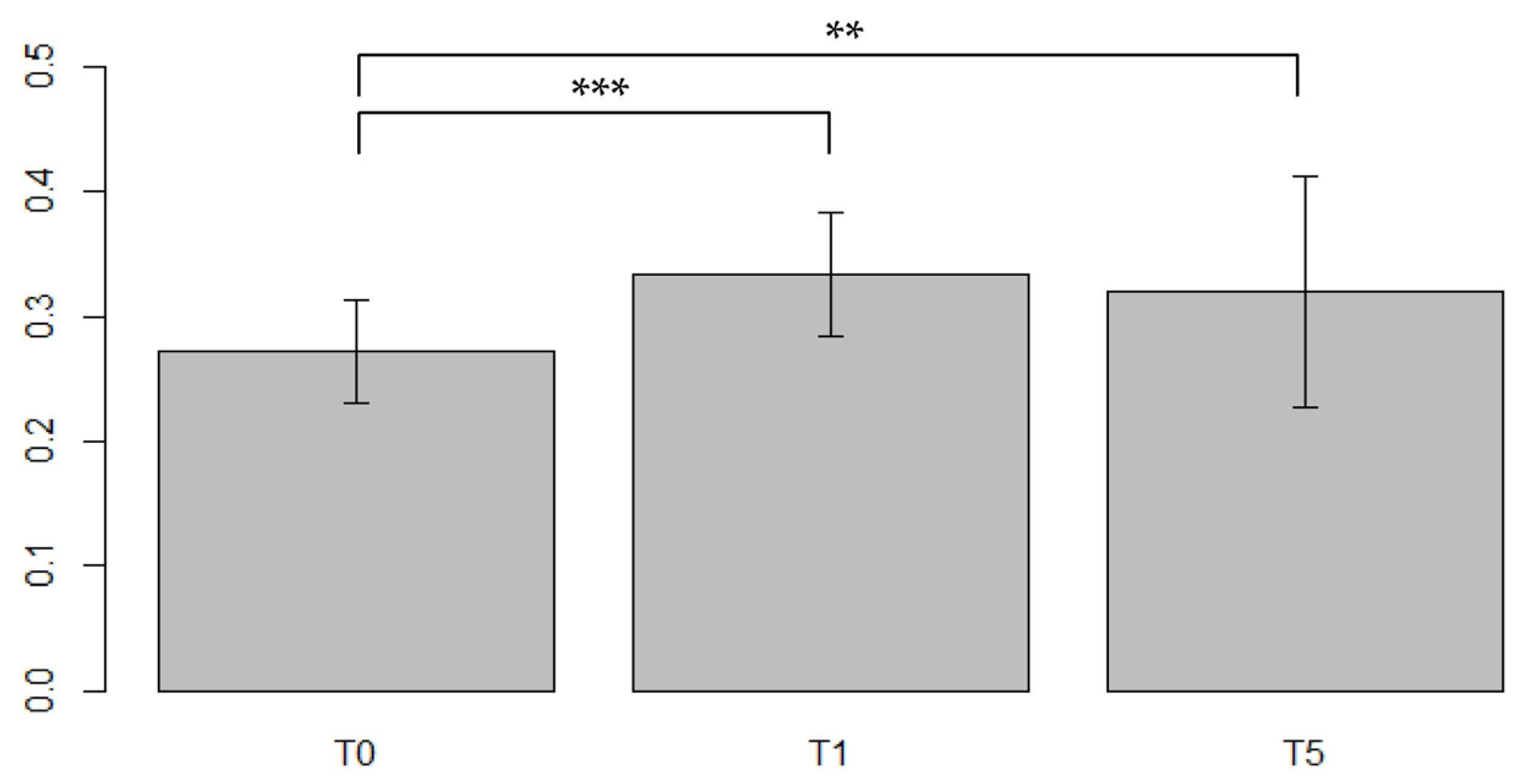
3.2. Results for the General Population of Women Treated with Cardiotoxic NACT
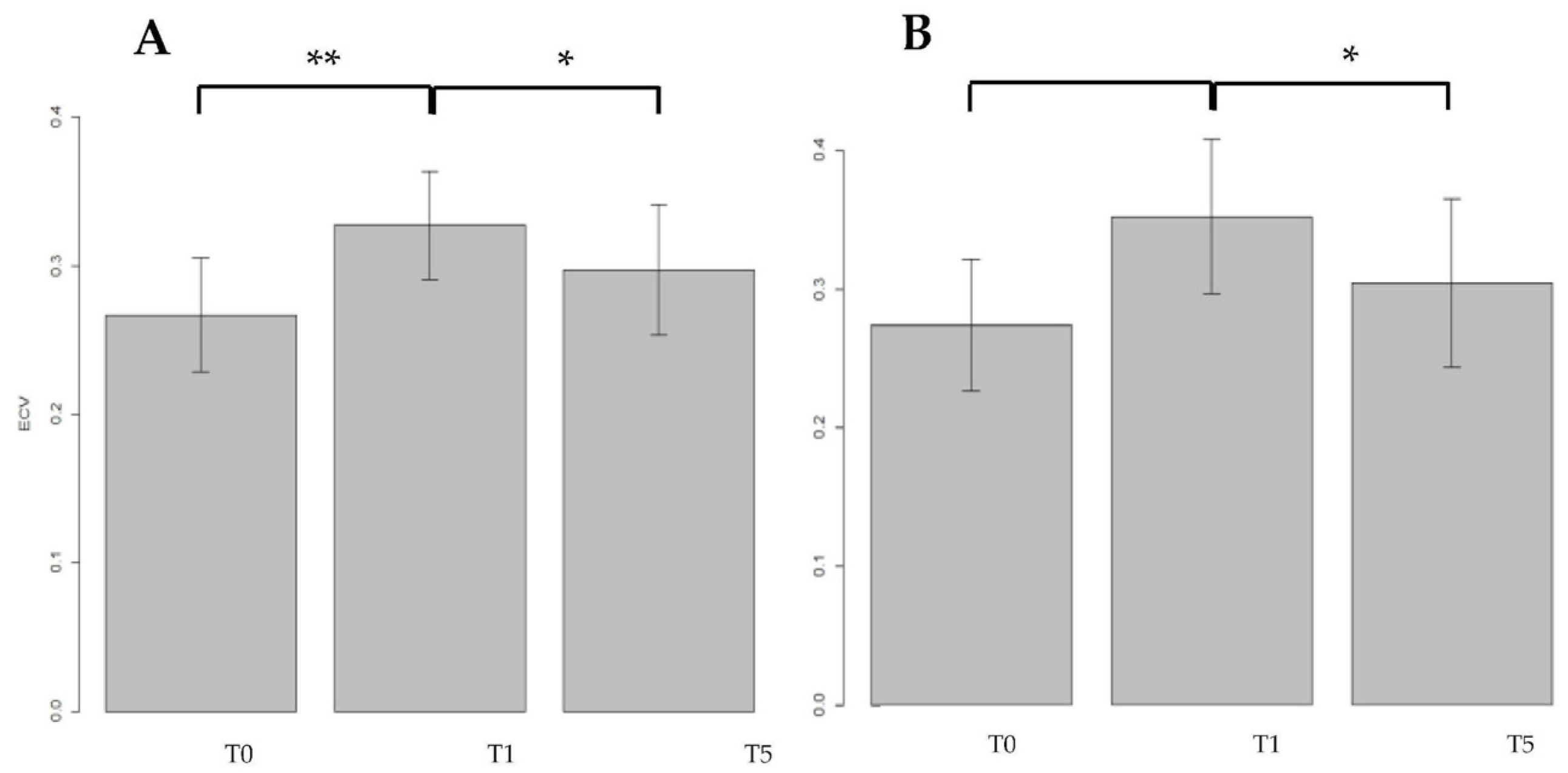
3.2.1. ECV Measured in the General Population in the Portal Phase (PP) Setting
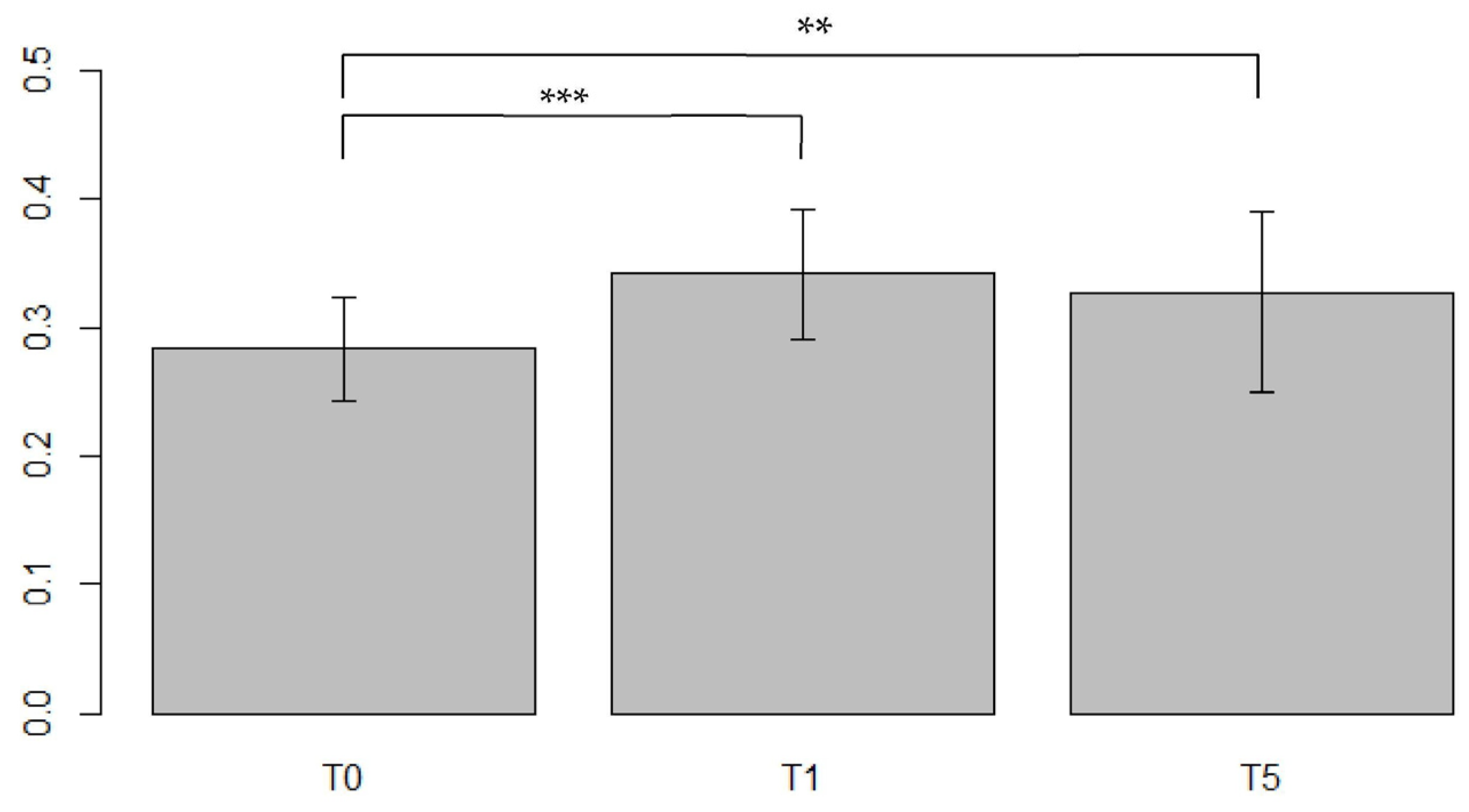
3.2.2. ECV Measured in the General Population in the Delayed Phase (DP) Setting
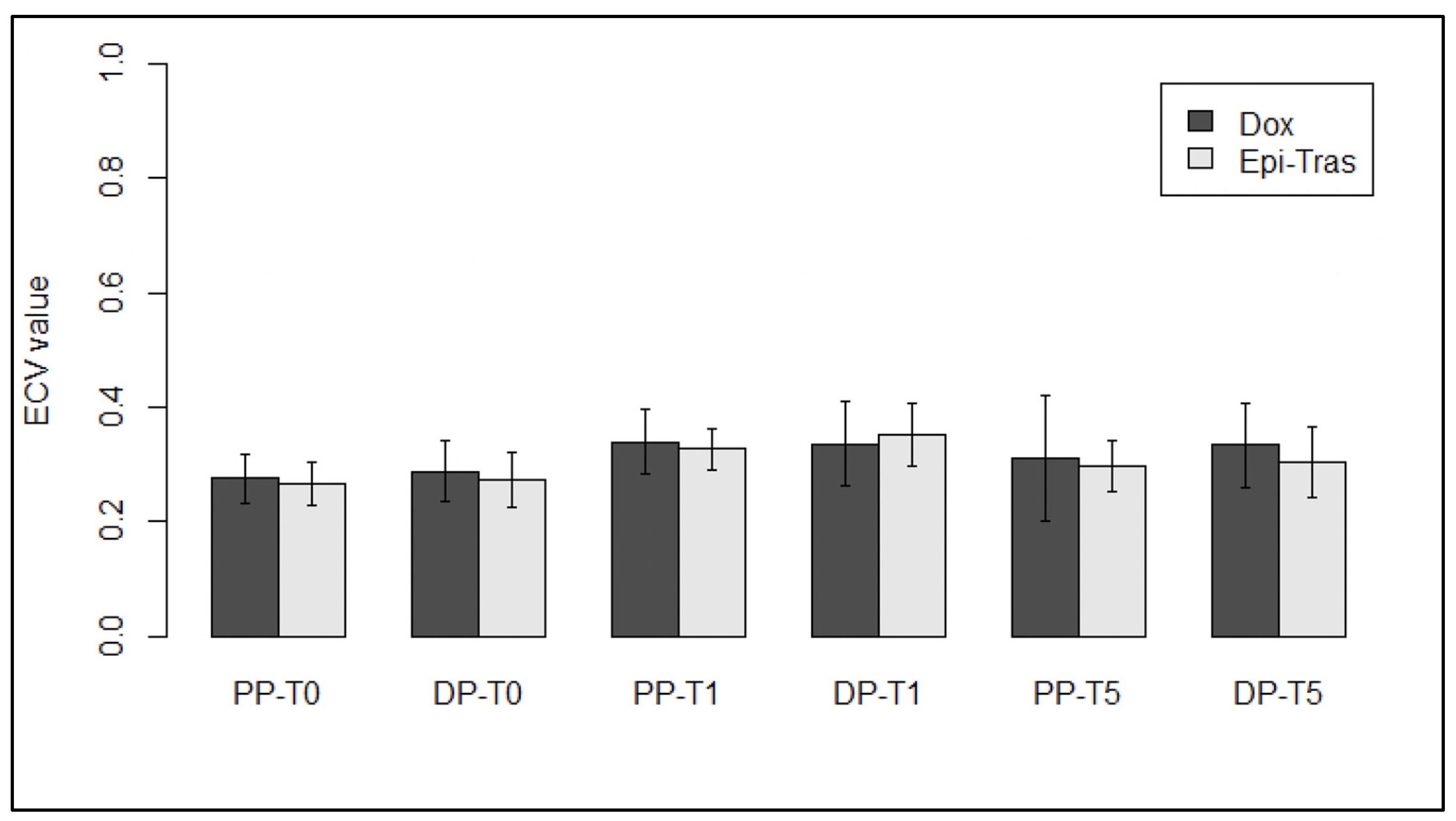
3.3. Results for Doxorubicin Treated (DOX-Treated) Women in the PP and DP Settings
3.4. Results for Myocardial ECV in Patients Treated with EPI–TRAS Women in the PP and DP Setting
3.5. Results for Myocardial ECV in Patients Treated with DOX versus Patients Treated with EPI–TRAS
3.6. Clinical Assessments and CTRCD Events in the Treated Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Health Organization. The Top 10 Causes of Death. Available online: http://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 1 February 2022).
- Vanni, G.; Pellicciaro, M.; Materazzo, M.; Bruno, V.; Oldani, C.; Pistolese, C.A.; Buonomo, C.; Caspi, J.; Gualtieri, P.; Chiaravalloti, A.; et al. Lockdown of Breast Cancer Screening for COVID-19: Possible Scenario. Vivo 2020, 34, 3047–3053. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Ma, J.; Gaudet, M.M.; Newman, L.A.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L. Breast Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 438–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orsaria, P.; Varvaras, D.; Vanni, G.; Pagnani, G.; Scaggiante, J.; Frusone, F.; Granai, A.V.; Petrella, G.; Buonomo, O.C. Nodal Status Assessment in Breast Cancer: Strategies of Clinical Grounds and Quality of Life Implications. Int. J. Breast Cancer 2014, 2014, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; de la Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and Safety of Neoadjuvant Pertuzumab and Trastuzumab in Women with Locally Advanced, Inflammatory, or Early HER2-Positive Breast Cancer (NeoSphere): A Randomised Multicentre, Open-Label, Phase 2 Trial. Lancet Oncol. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- Orsaria, P.; Caredda, E.; Genova, F.; Materazzo, M.; Capuano, I.; Vanni, G.; Granai, A.V.; DE Majo, A.; Portarena, I.; Sileri, P.; et al. Additional Nodal Disease Prediction in Breast Cancer with Sentinel Lymph Node Metastasis Based on Clinicopathological Features. Anticancer. Res. 2018, 37, 2109–2117. [Google Scholar] [CrossRef]
- Pramod, N.; Nigam, A.; Basree, M.; Mawalkar, R.; Mehra, S.; Shinde, N.; Tozbikian, G.; Williams, N.; Majumder, S.; Ramaswamy, B. Comprehensive Review of Molecular Mechanisms and Clinical Features of Invasive Lobular Cancer. Oncologist 2021, 26, e943–e953. [Google Scholar] [CrossRef]
- Materazzo, M.; Vanni, G.; Pellicciaro, M.; Anemona, L.; Servadei, F.; Giacobbi, E.; Farinaccio, A.; Pistolese, C.A.; Perretta, T.; Chiocchi, M.; et al. Case Report: Early Breast Cancer Recurrence Mimicking BIA-ALCL in a Patient With Multiple Breast Procedures. Front. Surg. 2021, 8, 606864. [Google Scholar] [CrossRef]
- Sawyer, D.B. Anthracyclines and Heart Failure. N. Engl. J. Med. 2013, 368, 1154–1156. [Google Scholar] [CrossRef] [Green Version]
- Sala, V.; della Sala, A.; Hirsch, E.; Ghigo, A. Signaling Pathways Underlying Anthracycline Cardiotoxicity. Antioxid. Redox Signal. 2020, 32, 1098–1114. [Google Scholar] [CrossRef]
- Cardinale, D.; Biasillo, G.; Salvatici, M.; Sandri, M.T.; Cipolla, C.M. Using Biomarkers to Predict and to Prevent Cardiotoxicity of Cancer Therapy. Expert Rev. Mol. Diagn. 2017, 17, 245–256. [Google Scholar] [CrossRef]
- Monti, C.B.; Zanardo, M.; Bosetti, T.; Alì, M.; de Benedictis, E.; Luporini, A.; Secchi, F.; Sardanelli, F. Assessment of Myocardial Extracellular Volume on Body Computed Tomography in Breast Cancer Patients Treated with Anthracyclines. Quant. Imaging Med. Surg. 2020, 10, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, L.; Gulizia, M.M.; di Lenarda, A.; Maurea, N.; Abrignani, M.G.; Bisceglia, I.; Bovelli, D.; de Gennaro, L.; del Sindaco, D.; Macera, F.; et al. ANMCO/AICO/AIOM Consensus Document: Clinical and Management Pathways in Cardio-Oncology. G. Ital. Cardiol. 2017, 18, 14–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Severino, P.; Maestrini, V.; Mariani, M.V.; Birtolo, L.I.; Scarpati, R.; Mancone, M.; Fedele, F. Structural and Myocardial Dysfunction in Heart Failure beyond Ejection Fraction. Heart Fail. Rev. 2020, 25, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. 2021. Available online: https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-and-Chronic-Heart-Failure (accessed on 5 March 2022).
- Benyounes, N.; van der Vynckt, C.; Tibi, T.; Iglesias, A.; Gout, O.; Lang, S.; Salomon, L. Left Ventricular End Diastolic Volume and Ejection Fraction Calculation: Correlation between Three Echocardiographic Methods. Cardiol. Res. Pract. 2020, 2020, 8076582. [Google Scholar] [CrossRef] [PubMed]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical Recommendations for Cardiovascular Magnetic Resonance Mapping of T1, T2, T2* and Extracellular Volume: A Consensus Statement by the Society for Cardiovascular Magnetic Resonance (SCMR) Endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef] [Green Version]
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 Mapping and Extracellular Volume (ECV) in Clinical Practice: A Comprehensive Review. J. Cardiovasc. Magn. Reson. 2016, 18, 89. [Google Scholar] [CrossRef] [Green Version]
- Cannaò, P.M.; Altabella, L.; Petrini, M.; Alì, M.; Secchi, F.; Sardanelli, F. Novel Cardiac Magnetic Resonance Biomarkers: Native T1 and Extracellular Volume Myocardial Mapping. Eur. Heart J. Suppl. 2016, 18 (Suppl. E), E64–E71. [Google Scholar] [CrossRef] [Green Version]
- Nacif, M.S.; Kawel, N.; Lee, J.J.; Chen, X.; Yao, J.; Zavodni, A.; Sibley, C.T.; Lima, J.A.C.; Liu, S.; Bluemke, D.A. Interstitial Myocardial Fibrosis Assessed as Extracellular Volume Fraction with Low-Radiation-Dose Cardiac CT. Radiology 2012, 264, 876–883. [Google Scholar] [CrossRef] [Green Version]
- Bandula, S.; White, S.K.; Flett, A.S.; Lawrence, D.; Pugliese, F.; Ashworth, M.T.; Punwani, S.; Taylor, S.A.; Moon, J.C. Measurement of Myocardial Extracellular Volume Fraction by Using Equilibrium Contrast-Enhanced CT: Validation against Histologic Findings. Radiology 2013, 269, 396–403. [Google Scholar] [CrossRef]
- Schindler, T.H.; Sharma, V.; Bhandiwad, A. Cardiac Computed Tomography-Derived Extracellular Volume Fraction in the Identification of Cardiotoxicity: Another Emerging Imaging Option. Int. J. Cardiol. Heart Vasc. 2021, 34, 100806. [Google Scholar] [CrossRef]
- Egashira, K.; Sueta, D.; Tomiguchi, M.; Kidoh, M.; Oda, S.; Usuku, H.; Hidaka, K.; Goto-Yamaguchi, L.; Sueta, A.; Komorita, T.; et al. Cardiac Computed Tomography-Derived Extracellular Volume Fraction in Late Anthracycline-Induced Cardiotoxicity. Int. J. Cardiol. Heart Vasc. 2021, 34, 100797. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.A.; Naish, J.H.; Bishop, P.; Coutts, G.; Clark, D.; Zhao, S.; Ray, S.G.; Yonan, N.; Williams, S.G.; Flett, A.S.; et al. Comprehensive Validation of Cardiovascular Magnetic Resonance Techniques for the Assessment of Myocardial Extracellular Volume. Circ. Cardiovasc. Imaging 2013, 6, 373–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christenson, E.S.; James, T.; Agrawal, V.; Park, B.H. Use of Biomarkers for the Assessment of Chemotherapy-Induced Cardiac Toxicity. Clin. Biochem. 2015, 48, 223–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvatici, M.; Cardinale, D.; Colombo, A.; Sandri, M.T. Cancer Cardiotoxicity and Cardiac Biomarkers. In Biomarkers in Disease: Methods, Discoveries and Applications: Biomarkers in Cancer; Springer: Berlin/Heidelberg, Germany, 2015; pp. 73–105. [Google Scholar] [CrossRef]
- Loria, V.; Dato, I.; Graziani, F.; Biasucci, L.M. Myeloperoxidase: A New Biomarker of Inflammation in Ischemic Heart Disease and Acute Coronary Syndromes. Mediat. Inflamm. 2008, 2008, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, R.; Riondino, S.; Formica, V.; Torino, F.; Martuscelli, E.; Roselli, M. MiRNAs and CircRNAs for the Diagnosis of Anthracycline-Induced Cardiotoxicity in Breast Cancer Patients: A Narrative Review. J. Pers. Med. 2022, 12, 1059. [Google Scholar] [CrossRef] [PubMed]
- Jordan, J.H.; Vasu, S.; Morgan, T.M.; D’Agostino, R.B.; Meléndez, G.C.; Hamilton, C.A.; Arai, A.E.; Liu, S.; Liu, C.-Y.; Lima, J.A.C.; et al. Anthracycline-Associated T1 Mapping Characteristics Are Elevated Independent of the Presence of Cardiovascular Comorbidities in Cancer Survivors. Circ. Cardiovasc. Imaging 2016, 9, e004325. [Google Scholar] [CrossRef] [Green Version]
- Ferreira de Souza, T.; Quinaglia A C Silva, T.; Osorio Costa, F.; Shah, R.; Neilan, T.G.; Velloso, L.; Nadruz, W.; Brenelli, F.; Sposito, A.C.; Matos-Souza, J.R.; et al. Anthracycline Therapy Is Associated With Cardiomyocyte Atrophy and Preclinical Manifestations of Heart Disease. JACC Cardiovasc. Imaging 2018, 11, 1045–1055. [Google Scholar] [CrossRef]
- Naresh, N.K.; Misener, S.; Zhang, Z.; Yang, C.; Ruh, A.; Bertolino, N.; Epstein, F.H.; Collins, J.D.; Markl, M.; Procissi, D.; et al. Cardiac MRI Myocardial Functional and Tissue Characterization Detects Early Cardiac Dysfunction in a Mouse Model of Chemotherapy-Induced Cardiotoxicity. NMR Biomed. 2020, 33, e4327. [Google Scholar] [CrossRef]
- Jeyaprakash, P.; Sangha, S.; Ellenberger, K.; Sivapathan, S.; Pathan, F.; Negishi, K. Cardiotoxic Effect of Modern Anthracycline Dosing on Left Ventricular Ejection Fraction: A Systematic Review and Meta-Analysis of Placebo Arms From Randomized Controlled Trials. J. Am. Heart Assoc. 2021, 10, e018802. [Google Scholar] [CrossRef]
- Nicolazzi, M.A.; Carnicelli, A.; Fuorlo, M.; Scaldaferri, A.; Masetti, R.; Landolfi, R.; Favuzzi, A.M.R. Anthracycline and Trastuzumab-Induced Cardiotoxicity in Breast Cancer. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 2175–2185. [Google Scholar] [CrossRef] [PubMed]
- Ewer, M.S.; Lippman, S.M. Type II Chemotherapy-Related Cardiac Dysfunction: Time to Recognize a New Entity. J. Clin. Oncol. 2005, 23, 2900–2902. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.K.; Casper, E.S.; Geller, N.L.; Hakes, T.B.; Kaufman, R.J.; Currie, V.; Schwartz, W.; Cassidy, C.; Petroni, G.R.; Young, C.W. A Prospective Randomized Comparison of Epirubicin and Doxorubicin in Patients with Advanced Breast Cancer. J. Clin. Oncol. 1985, 3, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Torti, F.M.; Bristow, M.M.; Lum, B.L.; Carter, S.K.; Howes, A.E.; Aston, D.A.; Brown, B.W.; Hannigan, J.F.; Meyers, F.J.; Mitchell, E.P. Cardiotoxicity of Epirubicin and Doxorubicin: Assessment by Endomyocardial Biopsy. Cancer Res. 1986, 46, 3722–3727. [Google Scholar] [PubMed]
- Telli, M.L.; Hunt, S.A.; Carlson, R.W.; Guardino, A.E. Trastuzumab-Related Cardiotoxicity: Calling Into Question the Concept of Reversibility. J. Clin. Oncol. 2007, 25, 3525–3533. [Google Scholar] [CrossRef]
- Moudgil, R.; Haddad, H. Chemotherapy-Related Cardiac Dysfunction. Curr. Opin. Cardiol. 2017, 32, 181–188. [Google Scholar] [CrossRef]
- Ewer, M.S.; Benjamin, R.S. Cardiac Complications of Cancer Treatment, 5th ed.; Cancer Medicine; Holland, J., Frei, E., Eds.; BC Decker: Hamilton, ON, Canada, 2000. [Google Scholar]
- López-Sendón, J.; Álvarez-Ortega, C.; Zamora Auñon, P.; Buño Soto, A.; Lyon, A.R.; Farmakis, D.; Cardinale, D.; Canales Albendea, M.; Feliu Batlle, J.; Rodríguez Rodríguez, I.; et al. Classification, Prevalence, and Outcomes of Anticancer Therapy-Induced Cardiotoxicity: The CARDIOTOX Registry. Eur. Heart J. 2020, 41, 1720–1729. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Value (n = 82) |
|---|---|
| Age (years), mean ± DS | 54.9 ± 5 |
| Type of carcinoma | |
| Infiltrating ductal | 62 |
| Infiltrating lobular | 4 |
| Poorly differentiated | 14 |
| Undifferentiated | 2 |
| Disease stage (TNM) | |
| Ic | 8 |
| II | 44 |
| III | 14 |
| IV | 16 |
| Treated with doxorubicin | 54 |
| epirubicin-trastuzumab | 28 |
| LVEF (%), mean ± SD | 64% ± 5% |
| Hematocrit (%), mean ± SD | 36.8% ± 4% |
| Portal phase | Operator 1 Mean (SD) | Operator 2 Mean (SD) | p-value |
| Baseline (T0) | 0.270 # (0.06) # | 0.290 # (0.08) # | 0.09 # |
| 1st year FU (T1) | 0.326 (0.06) | 0.329 (0.05) | 0.77 |
| 5th year FU (T5) | 0.300 # (0.05) # | 0.310 # (0.07) # | 0.68 # |
| Delayed Phase | Operator 1 Mean (SD) | Operator 2 Mean (SD) | p-value# |
| Baseline (T0) | 0.283 (0.05) | 0.279 (0.06) | 0.64 |
| 1st year FU (T1) | 0.345 (0.07) | 0.335 (0.06) | 0.47 |
| 5th year FU (T5) | 0.327 # (0.07) # | 0.312 # (0.07) # | 0.34 # |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiocchi, M.; Cerocchi, M.; Di Tosto, F.; Rosenfeld, R.; Pasqualetto, M.; Vanni, G.; De Stasio, V.; Pugliese, L.; Di Donna, C.; Idone, G.; et al. Quantification of Extracellular Volume in CT in Neoadjuvant Chemotherapy in Breast Cancer: New Frontiers in Assessing the Cardiotoxicity of Anthracyclines and Trastuzumab. J. Pers. Med. 2023, 13, 199. https://doi.org/10.3390/jpm13020199
Chiocchi M, Cerocchi M, Di Tosto F, Rosenfeld R, Pasqualetto M, Vanni G, De Stasio V, Pugliese L, Di Donna C, Idone G, et al. Quantification of Extracellular Volume in CT in Neoadjuvant Chemotherapy in Breast Cancer: New Frontiers in Assessing the Cardiotoxicity of Anthracyclines and Trastuzumab. Journal of Personalized Medicine. 2023; 13(2):199. https://doi.org/10.3390/jpm13020199
Chicago/Turabian StyleChiocchi, Marcello, Martina Cerocchi, Federica Di Tosto, Roberto Rosenfeld, Monia Pasqualetto, Gianluca Vanni, Vincenzo De Stasio, Luca Pugliese, Carlo Di Donna, Gaetano Idone, and et al. 2023. "Quantification of Extracellular Volume in CT in Neoadjuvant Chemotherapy in Breast Cancer: New Frontiers in Assessing the Cardiotoxicity of Anthracyclines and Trastuzumab" Journal of Personalized Medicine 13, no. 2: 199. https://doi.org/10.3390/jpm13020199