
Is Age a Limiting Factor for Audiological Results in Active Middle Ear Implants?
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Procedures
2.2.1. Audiological Assessment
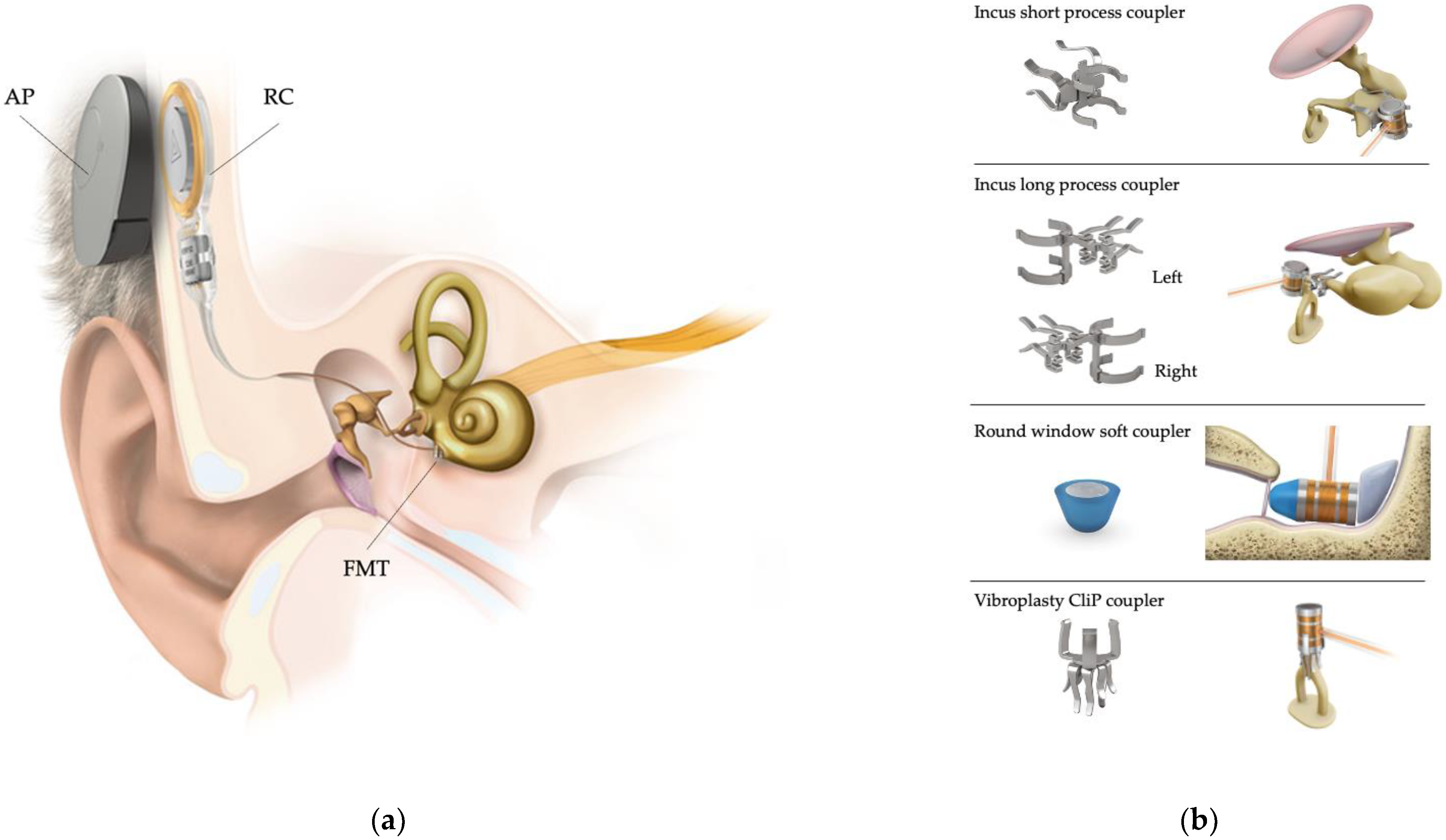
2.2.2. Surgical Procedure
2.2.3. Questionnaires
2.2.4. Data Analysis
3. Results
3.1. Participants
3.2. Surgical Outcomes
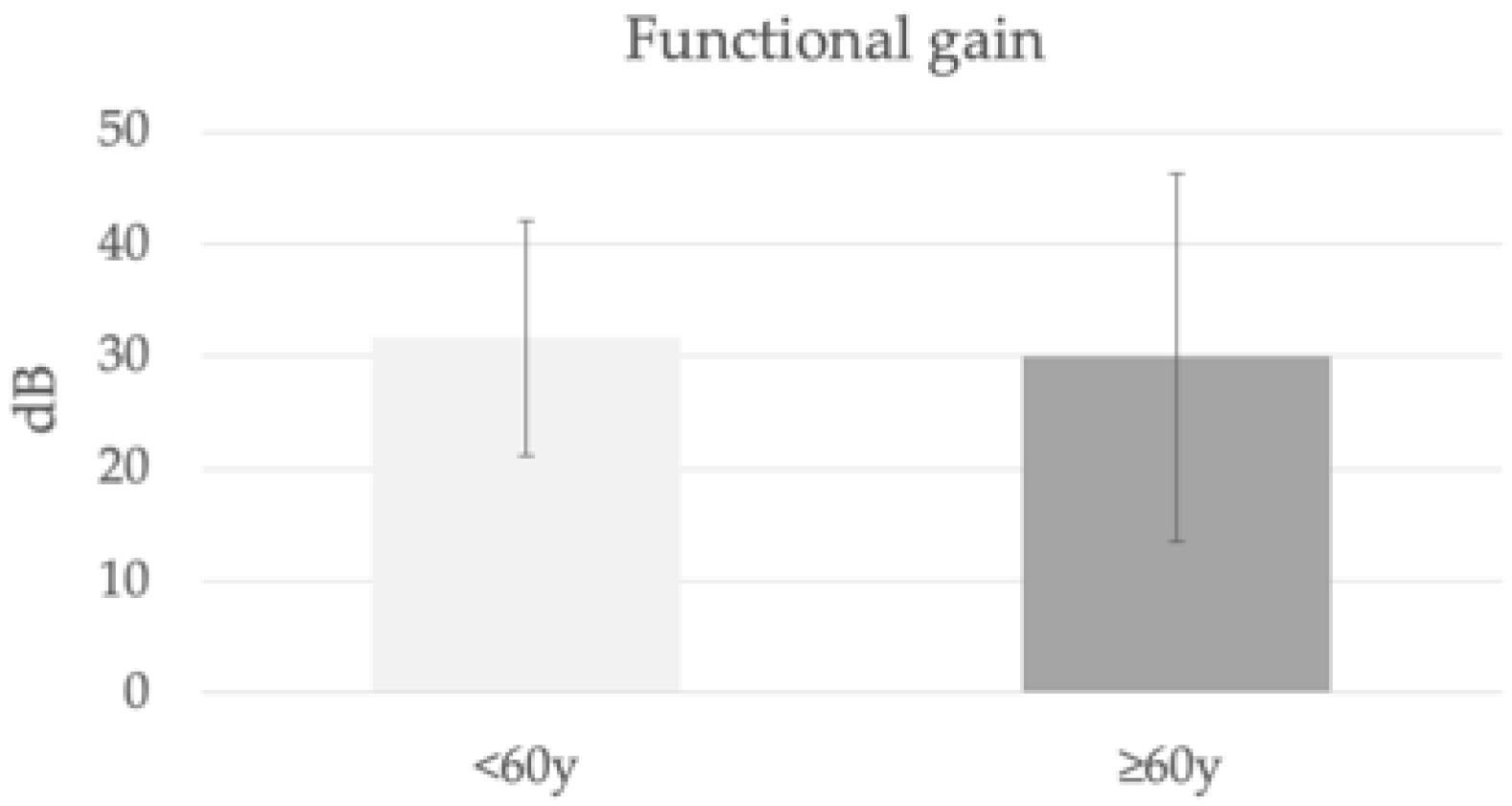
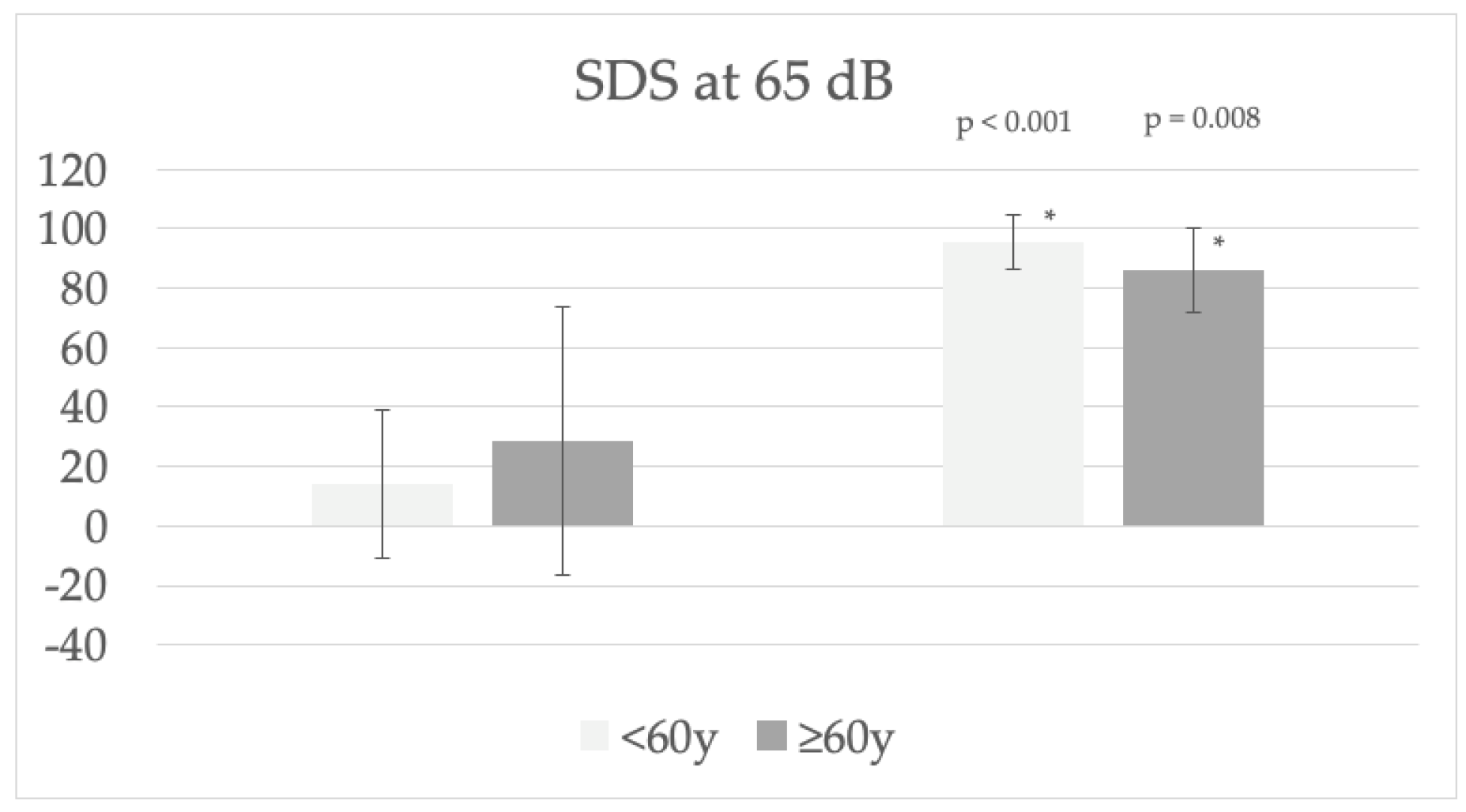
3.3. Audiological Assessment
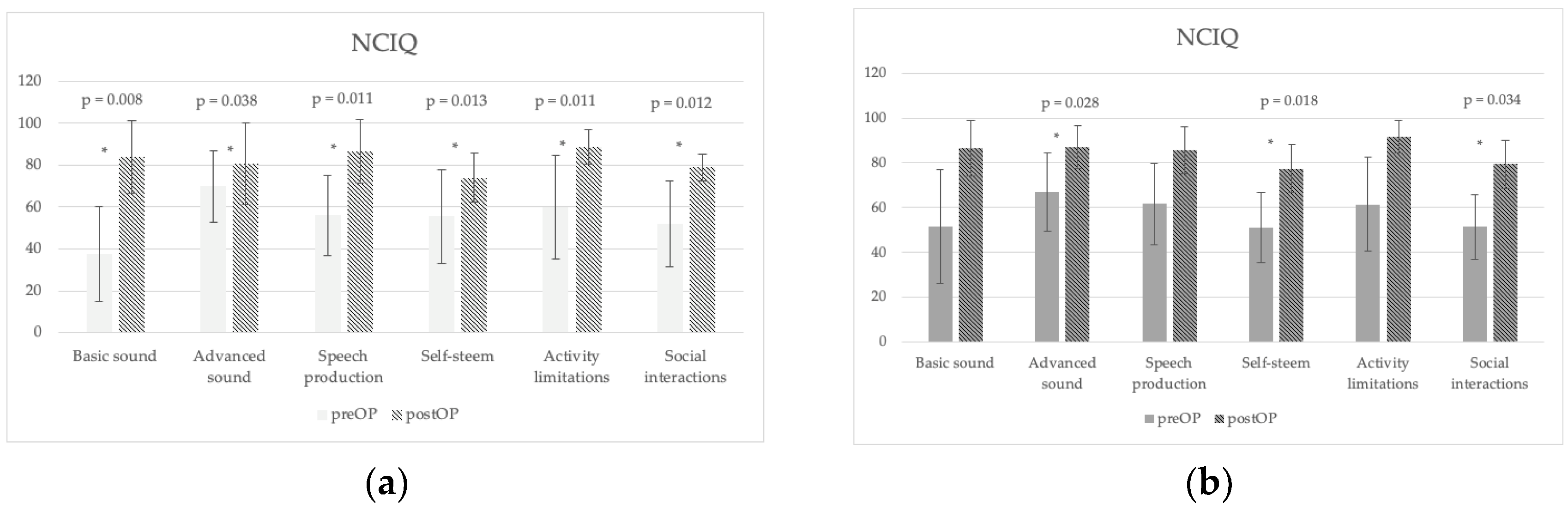
3.4. Subjective Questionnaries
3.5. Relationship between Age and Audilogical and Subjective Benefit Outcomes
4. Discussion
4.1. Audiological Outcome with the VSB
4.2. VSB and Surgical Outcomes
4.3. Effect of the VSB on Subjetive Outcomes
4.4. Limitations
4.5. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lassaletta, L.; Sánchez-Cuadrado, I.; Espinosa, J.M.; Batuecas, Á.; Cenjor, C.; Lavilla, M.J.; Cavallé, L.; Huarte, A.; Nuñez, F.; Manrique, M.; et al. Active middle ear implants. Acta Otorrinolaringol. Esp. 2019, 70, 112–118. [Google Scholar] [CrossRef]
- Rahne, T.; Skarzynski, P.H.; Hagen, R.; Radeloff, A.; Lassaletta, L.; Barbara, M.; Plontke, S.K.; Mlynski, R. A retrospective European multicenter analysis of the functional outcomes after active middle ear implant surgery using the third generation vibroplasty couplers. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Lenarz, T.; Weber, B.P.; Mack, K.F.; Battmer, R.D.; Gnadeberg, D. The Vibrant Soundbridge System: A new kind of hearing aid for sensorineural hearing loss. 1: Function and initial clinical experiences. Laryngo-Rhino-Otologie 1998, 77, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Maw, J. The Vibrant Soundbridge: A Global Overview. Otolaryngol. Clin. N. Am. 2019, 52, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Ernst, A.; Todt, I.; Wagner, J. Safety and effectiveness of the Vibrant Soundbridge in treating conductive and mixed hearing loss: A systematic review. Laryngoscope 2016, 126, 1451–1457. [Google Scholar] [CrossRef] [PubMed]
- Sprinzl, G.M.; Schoerg, P.; Muck, S.; Jesenko, M.; Speiser, S.; Ploder, M.; Edlinger, S.H.; Magele, A. Long-Term Stability and Safety of the Soundbridge Coupled to the Round Window. Laryngoscope 2021, 131, e1434–e1442. [Google Scholar] [CrossRef] [PubMed]
- United Nations; Department of Economic and Social Affairs; Population Division. World Population Prospects 2019: Highlights (ST/ESA/SER.A/423); United Nations: New York, NY, USA, 2019. [Google Scholar]
- Sprinzl, G.M.; Riechelmann, H. Current trends in treating hearing loss in elderly people: A review of the technology and treatment options—A mini-review. Gerontology 2010, 56, 351–358. [Google Scholar] [CrossRef]
- Sanchez-Cuadrado, I.; Lassaletta, L.; Perez-Mora, R.M.; Zernotti, M.; Di Gregorio, M.F.; Boccio, C.; Gavilán, J. Is there an age limit for cochlear implantation? Ann. Otol. Rhinol. Laryngol. 2013, 122, 222–228. [Google Scholar] [CrossRef]
- Brewster, K.K.; Hu, M.C.; Wall, M.M.; Brown, P.J.; Zilcha-Mano, S.; Roose, S.P.; Stein, A.; Golub, J.S.; Rutherford, B.R. Age-Related Hearing Loss, Neuropsychological Performance, and Incident Dementia in Older Adults. J. Alzheimer’s Dis. JAD 2021, 80, 855–864. [Google Scholar] [CrossRef]
- Calvino, M.; Sánchez-Cuadrado, I.; Gavilán, J.; Gutiérrez-Revilla, M.A.; Polo, R.; Lassaletta, L. Effect of cochlear implantation on cognitive decline and quality of life in younger and older adults with severe-to-profound hearing loss. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 4745–4759. [Google Scholar] [CrossRef]
- Lassaletta, L.; Calvino, M.; Sánchez-Cuadrado, I.; Pérez-Mora, R.M.; Muñoz, E.; Gavilán, J. Pros and Cons of Round Window Vibroplasty in Open Cavities: Audiological, Surgical, and Quality of Life Outcomes. Otol. Neurotol. 2015, 36, 944–952. [Google Scholar] [CrossRef] [PubMed]
- De Cárdenas, M.R.; Marrero, V. Cuaderno de Logoaudiometría; Universidad Nacional de Educación a Distancia—UNED: Madrid, Spain, 1994. [Google Scholar]
- Colletti, V.; Soli, S.D.; Carner, M.; Colletti, L. Treatment of mixed hearing losses via implantation of a vibratory transducer on the round window. Int. J. Audiol. 2006, 45, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, A.M.; Martini, A.; Prosser, S.; Giarbini, N.; Streitberger, C. Coupling the Vibrant Soundbridge to cochlea round window: Auditory results in patients with mixed hearing loss. Otol. Neurotol. 2009, 30, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Linder, T.; Schlegel, C.; DeMin, N.; van der Westhuizen, S. Active middle ear implants in patients undergoing subtotal petrosectomy: New application for the Vibrant Soundbridge device and its implication for lateral cranium base surgery. Otol. Neurotol. 2009, 30, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, A.M.; Todt, I.; Sprinzl, G.; Profant, M.; Schwab, B. Consensus statement on round window vibroplasty. Ann. Otol. Rhinol. Laryngol. 2014, 123, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Cuadrado, I.; Gavilan, J.; Perez-Mora, R.; Muñoz, E.; Lassaletta, L. Reliability and validity of the Nijmegen Cochlear Implant Questionnaire in Spanish. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 1621–1625. [Google Scholar] [CrossRef]
- Zwartenkot, J.W.; Hashemi, J.; Cremers, C.W.; Mulder, J.J.; Snik, A.F. Active middle ear implantation for patients with sensorineural hearing loss and external otitis: Long-term outcome in patient satisfaction. Otol. Neurotol. 2013, 34, 855–861. [Google Scholar] [CrossRef]
- Sanchez-Cuadrado, I.; Lassaletta, L.; Perez-Mora, R.; Muñoz, E.; Gavilan, J. Reliability and validity of the Spanish Glasgow Benefit Inventory after cochlear implant surgery in adults. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 333–336. [Google Scholar] [CrossRef]
- Calvino, M.; Gavilán, J.; Sánchez-Cuadrado, I.; Pérez-Mora, R.M.; Muñoz, E.; Lassaletta, L. Validation of the Hearing Implant Sound Quality Index (HISQUI19) to assess Spanish-speaking cochlear implant users’ auditory abilities in everyday communication situations. Acta Oto-Laryngol. 2016, 136, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.H.; Moon, Y.M.; Nam, G.S.; Bae, S.H.; Kim, S.H.; Jung, J.; Choi, J.Y. Clinical Experience of Vibroplasty With Direct Coupling to the Oval Window Without Use of a Coupler. Laryngoscope 2020, 130, e926–e932. [Google Scholar] [CrossRef]
- Busch, S.; Lenarz, T.; Maier, H. Comparison of Alternative Coupling Methods of the Vibrant Soundbridge Floating Mass Transducer. Audiol. Neuro-Otol. 2016, 21, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Song, C.I.; Cho, H.H.; Choi, B.Y.; Choi, J.Y.; Choi, J.W.; Choung, Y.H.; Chung, J.W.; Chung, W.H.; Hong, S.H.; Kim, Y.; et al. Results of Active Middle Ear Implantation in Patients With Mixed Hearing Loss After Middle Ear Surgery: A Prospective Multicenter Study (the ROMEO Study). Clin. Exp. Otorhinolaryngol. 2022, 15, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, S.; Usami, S.I.; Takahashi, H.; Kanda, Y.; Tono, T.; Doi, K.; Kumakawa, K.; Gyo, K.; Naito, Y.; Kanzaki, S.; et al. Round Window Application of an Active Middle Ear Implant: A Comparison With Hearing Aid Usage in Japan. Otol. Neurotol. 2017, 38, e145–e151. [Google Scholar] [CrossRef]
- Tysome, J.R.; Moorthy, R.; Lee, A.; Jiang, D.; O’Connor, A.F. Systematic review of middle ear implants: Do they improve hearing as much as conventional hearing AIDS? Otol. Neurotol. 2010, 31, 1369–1375. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.; Kompis, M.; Candreia, C.; Pfiffner, F.; Häusler, R.; Stieger, C. The floating mass transducer at the round window: Direct transmission or bone conduction? Hear. Res. 2010, 263, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.; Mir-Salim, P.; Zellhuber, N.; Helbig, R.; Bloching, M.; Schmidt, T.; Koscielny, S.; Dziemba, O.C.; Plontke, S.K.; Rahne, T. Influence of Floating-Mass Transducer Coupling Efficiency for Active Middle-Ear Implants on Speech Recognition. Otol. Neurotol. 2017, 38, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Marino, R.; Lampacher, P.; Dittrich, G.; Tavora-Vieira, D.; Kuthubutheen, J.; Rajan, G.P. Does Coupling and Positioning in Vibroplasty Matter? A Prospective Cohort Study. Otol. Neurotol. 2015, 36, 1223–1230. [Google Scholar] [CrossRef]
- Rajan, G.P.; Lampacher, P.; Ambett, R.; Dittrich, G.; Kuthubutheen, J.; Wood, B.; McArthur, A.; Marino, R. Impact of floating mass transducer coupling and positioning in round window vibroplasty. Otol. Neurotol. 2011, 32, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, L.; Rahne, T.; Plontke, S.K.; Oberhoffner, T.; Dahl, R.; Mlynski, R.; Dziemba, O.; Aristeidou, A.; Gadyuchko, M.; Koscielny, S.; et al. Intraoperative quantification of floating mass transducer coupling quality in active middle ear implants: A multicenter study. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 2277–2288. [Google Scholar] [CrossRef]
- Edlinger, S.H.; Hasenzagl, M.; Schoerg, P.; Muck, S.; Magele, A.; Sprinzl, G.M. Long-Term Safety and Quality of Life after Vibroplasty in Sensorineural Hearing Loss: Short/Long Incus Process Coupler. Audiol. Neuro-Otol. 2022, 27, 175–183. [Google Scholar] [CrossRef]
- Brkic, F.F.; Riss, D.; Auinger, A.; Zoerner, B.; Arnoldner, C.; Baumgartner, W.D.; Gstoettner, W.; Vyskocil, E. Long-Term Outcome of Hearing Rehabilitation With An Active Middle Ear Implant. Laryngoscope 2019, 129, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Zahnert, T.; Löwenheim, H.; Beutner, D.; Hagen, R.; Ernst, A.; Pau, H.W.; Zehlicke, T.; Kühne, H.; Friese, N.; Tropitzsch, A.; et al. Multicenter Clinical Trial of Vibroplasty Couplers to Treat Mixed/Conductive Hearing Loss: First Results. Audiol. Neuro-Otol. 2016, 21, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Kazikdas, K.C.; Onal, K.; Yildirim, N. Sensorineural hearing loss after ossicular manipulation and drill-generated acoustic trauma in type I tympanoplasty with and without mastoidectomy: A series of 51 cases. Ear Nose Throat J. 2015, 94, 378–398. [Google Scholar] [PubMed]
- Prenzler, N.K.; Gruber, L.; Lenarz, T.; Maier, H.; Schwab, B. The Impact of Two-Stage Subtotal Petrosectomy and Round Window Vibroplasty on Bone Conduction Thresholds. ORL 2018, 80, 77–84. [Google Scholar] [CrossRef]
- Short, T.G.; Campbell, D.; Frampton, C.; Chan, M.T.V.; Myles, P.S.; Corcoran, T.B.; Sessler, D.I.; Mills, G.H.; Cata, J.P.; Painter, T.; et al. Anaesthetic depth and complications after major surgery: An international, randomised controlled trial. Lancet 2019, 394, 1907–1914. [Google Scholar] [CrossRef]
- Mojallal, H.; Schwab, B.; Hinze, A.L.; Giere, T.; Lenarz, T. Retrospective audiological analysis of bone conduction versus round window vibratory stimulation in patients with mixed hearing loss. Int. J. Audiol. 2015, 54, 391–400. [Google Scholar] [CrossRef]
- Wimmer, W.; von Werdt, M.; Mantokoudis, G.; Anschuetz, L.; Kompis, M.; Caversaccio, M. Outcome prediction for Bonebridge candidates based on audiological indication criteria. Auris Nasus Larynx 2019, 46, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Atas, A.; Tutar, H.; Gunduz, B.; Bayazıt, Y.A. Vibrant SoundBridge application to middle ear windows versus conventional hearing aids: A comparative study based on international outcome inventory for hearing aids. Eur. Arch. Oto-Rhino-Laryngol. 2014, 271, 35–40. [Google Scholar] [CrossRef]
- Han, J.J.; Rhee, J.; Song, J.J.; Koo, J.W.; Choi, B.Y. Clinical predictors for satisfaction with incus vibroplasty: A preliminary study. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Brkic, F.F.; Baumgartner, W.D.; Riss, D.; Thurner, T.; Liu, D.T.; Gstöttner, W.; Vyskocil, E. Progressive Sensorineural Hearing Loss in Vibrant Soundbridge Users Requiring Cochlear Implantation. J. Pers. Med. 2022, 12, 191. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | <60 Years Old 11 | ≥60 Years Old 9 | p Value |
|---|---|---|---|
| Age (years) (mean ± SD) (range) | 45 ± 10 (24–56) | 69 ± 7 (61–79) | <0.001 |
| Gender (n) (%) | |||
| Male | 7 (64%) | 5(56%) | |
| Female | 4 (36%) | 4(44%) | |
| HL aetiology (n) (%) | |||
| Cholesteatoma | 6 (55%) | 2 (22%) | |
| Non-Cholesteatomatosus COM | 3 (27%) | 2 (22%) | |
| Previous surgery | 2 (18%) | 2 (22%) | |
| CSF leak | 0 | 1 (11%) | |
| Paraganglioma | 0 | 1 (11%) | |
| EAC stenosis | 0 | 1 (11%) | |
| PTA4BC (dB) | 28 ± 12 | 41 ± 11 | 0.018 |
| PTA4AC (dB) | 66 ± 15 | 73 ± 18 | 0.349 |
| ABG (dB) | 38 ± 10 | 32 ± 17 | 0.318 |
| SDS (%) | 19 ± 25 | 31 ± 43 | 0.297 |
| <60 Years Old | ≥60 Years Old | |
|---|---|---|
| Coupling option | ||
| Round window | 8 (73%) | 7 (78%) |
| Incus short process | 1 (9%) | 1 (11%) |
| Stapes | 2 (18%) | 1 (11%) |
| mean ± SD | ||
| PTA4BC (dB) | 33 ± 13 | 49 ± 11 |
| PTA4SF (dB) | 34 ± 7 | 42 ± 9 |
| pABG (dB) | 1 ± 10 | −6 ± 10 |
| SDS (%) | 95 ± 9 | 84 ± 14 |
| Functional gain | 32 ± 11 | 30 ± 15 |
| GBI Score | <60 Years Old Mean ± SD | ≥60 Years Old Mean ± SD | p Value |
|---|---|---|---|
| Overall | 61 ± 27 | 33 ± 24 | 0.05 |
| General subscale | 45 ± 10 | 23 ± 19 | 0.066 |
| Social subscale | 19 ± 41 | 14 ± 20 | 0.776 |
| Physical health subscale | 9 ± 35 | −8 ± 14 | 0.328 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales-Puebla, J.M.; Lassaletta, L.; Sánchez-Cuadrado, I.; Calvino, M.; Gavilán, J. Is Age a Limiting Factor for Audiological Results in Active Middle Ear Implants? J. Pers. Med. 2023, 13, 1650. https://doi.org/10.3390/jpm13121650
Morales-Puebla JM, Lassaletta L, Sánchez-Cuadrado I, Calvino M, Gavilán J. Is Age a Limiting Factor for Audiological Results in Active Middle Ear Implants? Journal of Personalized Medicine. 2023; 13(12):1650. https://doi.org/10.3390/jpm13121650
Chicago/Turabian StyleMorales-Puebla, J. Manuel, Luis Lassaletta, Isabel Sánchez-Cuadrado, Miryam Calvino, and Javier Gavilán. 2023. "Is Age a Limiting Factor for Audiological Results in Active Middle Ear Implants?" Journal of Personalized Medicine 13, no. 12: 1650. https://doi.org/10.3390/jpm13121650