
A Preliminary Study on the Meaning of Inflammatory Indexes in MS: A Neda-Based Approach
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.1.1. Participitians
2.1.2. MRI Acquisition
2.1.3. Serum Samples
2.2. Statistical Methods
3. Results
3.1. Demographic and Physical Features of the Study Group
3.2. Hemogram Parameters and Inflammation Indices
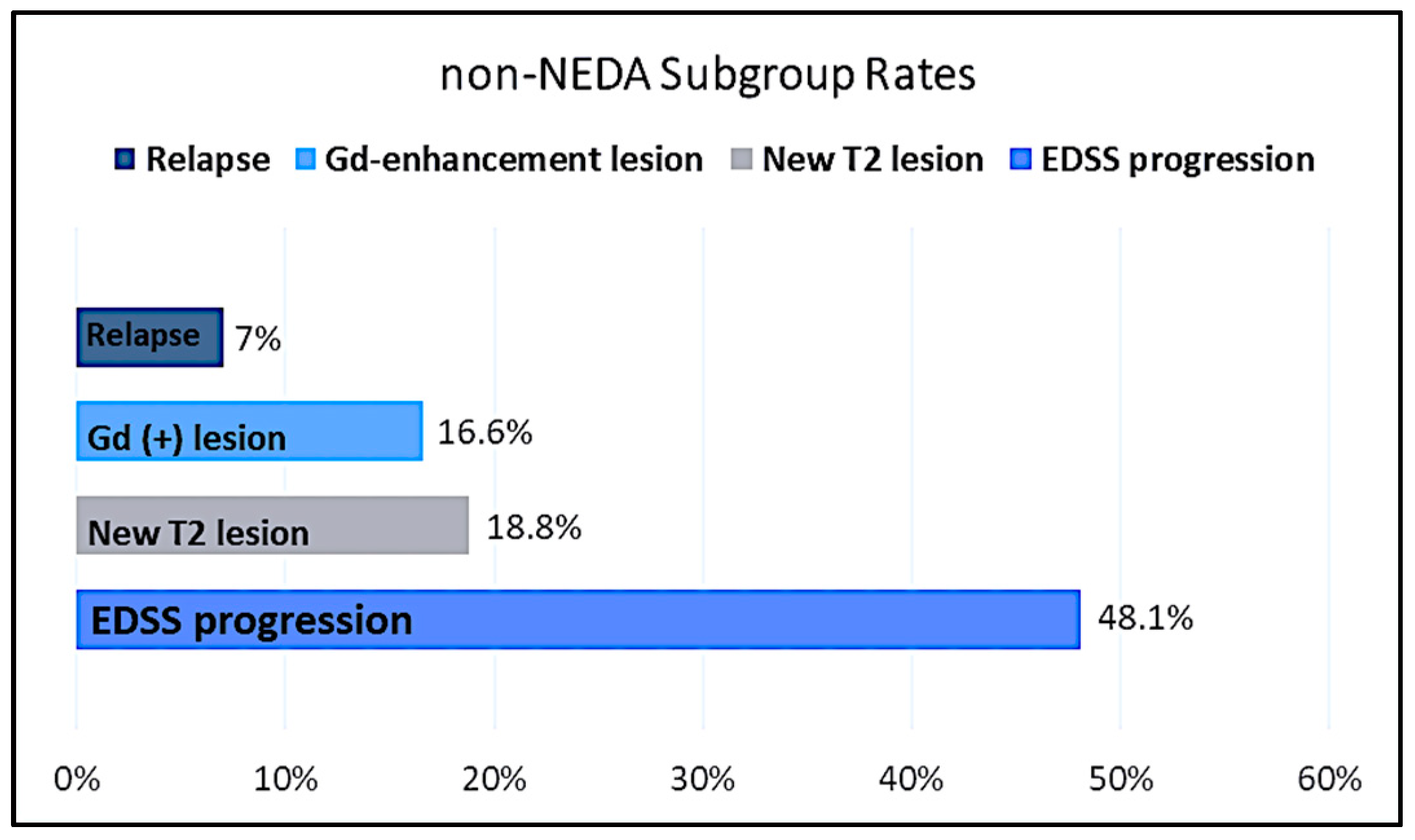
3.3. NEDA-3 Status
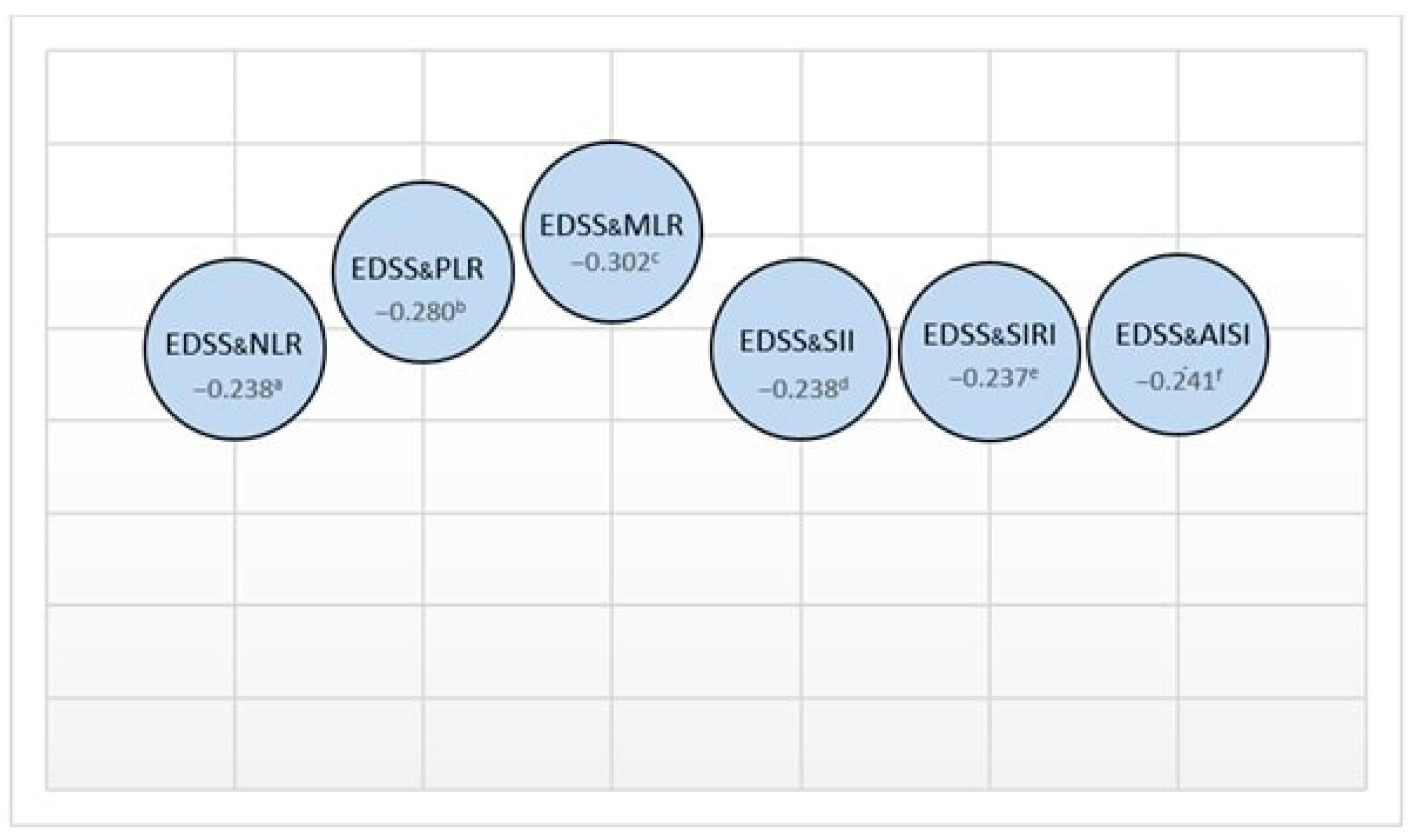
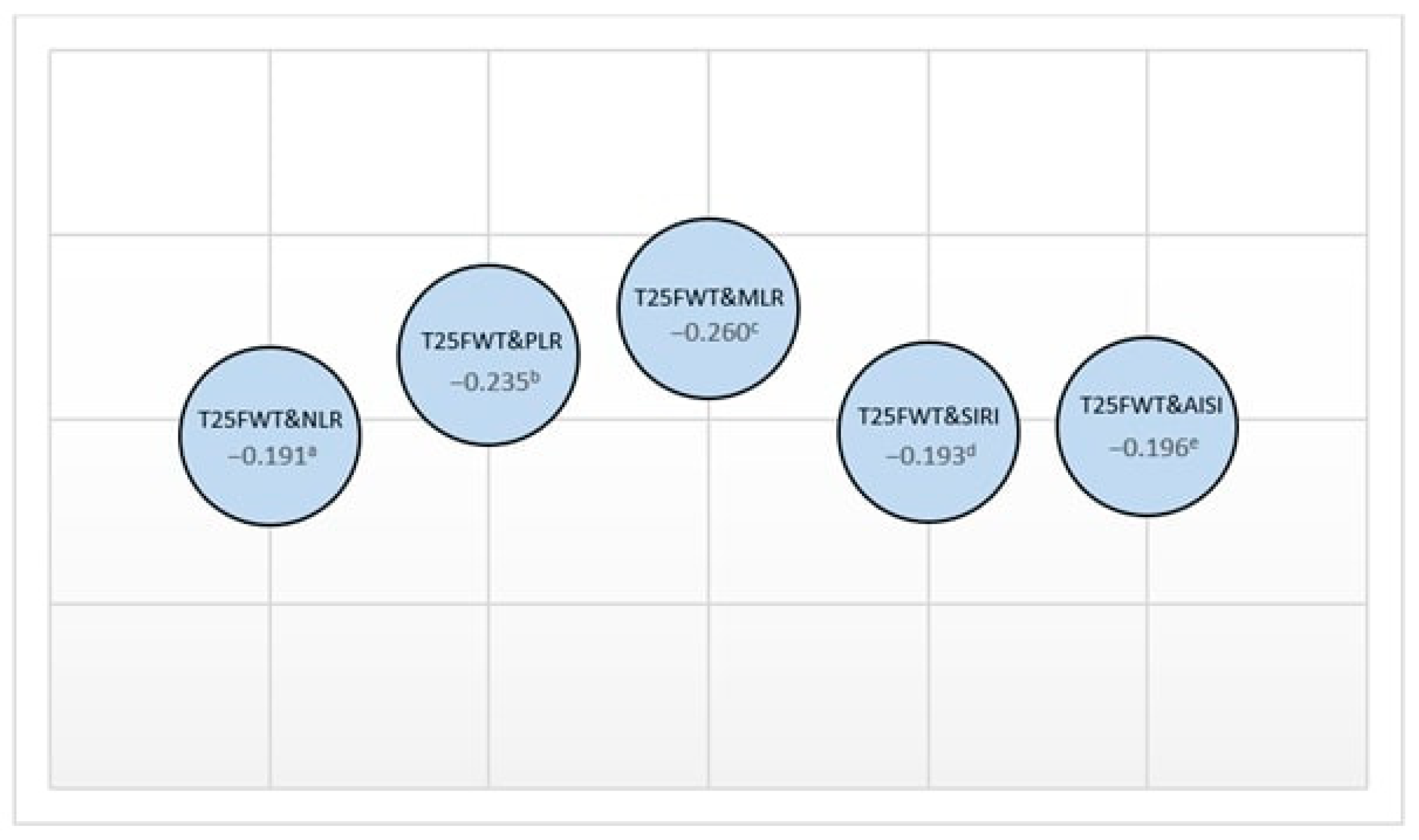
3.4. Correlation Analyses
3.5. Assessment of NEDA Status and Inflammation Indexes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dumitrescu, L.; Papathanasiou, A. Beta interferons as immunotherapy in multiple sclerosis: A new outlook on a classic drug during the COVID-19 pandemic. QJM Int. J. Med. 2021, 114, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Bittner, S.; Wiendl, H. Neuroimmunotherapies Targeting T Cells: From Pathophysiology to Therapeutic Applications. Neurotherapeutics 2016, 13, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Govindarajan, V.; de Rivero Vaccari, J.P. Role of inflammasomes in multiple sclerosis and their potential as therapeutic targets. J. Neuroinflamm. 2020, 17, 260. [Google Scholar] [CrossRef] [PubMed]
- Giovannoni, G.; Butzkueven, H. Brain health: Time matters in multiple sclerosis. Mult. Scler. Relat. Disord. 2016, 9, S5–S48. [Google Scholar] [CrossRef]
- Rush, C.A.; Heather, J. Aggressive multiple sclerosis: Proposed definition and treatment algorithm. Nat. Rev. Neurol. 2015, 11, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Parks, N.E.; Flanagan, E.P. NEDA treatment target? No evident disease activity as an actionable outcome in practice. J. Neurol. Sci. 2017, 383, 31–34. [Google Scholar] [CrossRef]
- Olsson, A.; Gustavsen, S. Neutrophil-to-lymphocyte ratio and CRP as biomarkers in multiple sclerosis: A systematic review. Acta Neurol. Scand 2021, 143, 577–586. [Google Scholar] [CrossRef]
- Hasselbalch, I.C.; Søndergaard, H.B. The neutrophil-to-lymphocyte ratio is associated with multiple sclerosis. Mult. Scler. J. Exp. Transl. Clin. 2018, 4, 2055217318813183. [Google Scholar] [CrossRef]
- Walzik, D.; Joisten, N. Transferring clinically established immune inflammation markers into exercise physiology: Focus on neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and systemic immune-inflammation index. Eur. J. Appl. Physiol. 2021, 121, 1803–1814. [Google Scholar] [CrossRef]
- Huang, W.C.; Lin, H.C. Neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio are associated with a 2-year relapse in patients with multiple sclerosis. Mult. Scler. Relat. Disord. 2022, 58, 103514. [Google Scholar] [CrossRef]
- Gokce, S.F.; Bolayr, A. The role of systemic immune inflammatory index in showing an active lesion in patients with multiple sclerosis. BMC Neurol. 2023, 23, 64. [Google Scholar] [CrossRef]
- Sacmaci, H.; Akturk, T. The predictive value of the systemic immune-inflammation index as a new prognostic marker for disability in patients with multiple sclerosis. Turk. J. Neurol. 2021, 27, 133–139. [Google Scholar] [CrossRef]
- Wei, L.; Xie, H. Prognostic value of the systemic inflammation response index in human malignancy: A meta-analysis. Medicine 2020, 99, e23486. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.K.; Wei, Q. Clinical usefulness of the lymphocyte-to-monocyte ratio and aggregate index of systemic inflammation in patients with esophageal cancer: A retrospective cohort study. Cancer Cell Int. 2023, 23, 13. [Google Scholar] [CrossRef] [PubMed]
- Solaro, C.; Cattaneo, D. Clinical correlates with 9-hole peg test in a large population of people with multiple sclerosis. Mult. Scler. Relat. Disord. 2019, 30, 1–8. [Google Scholar] [CrossRef]
- Marchesi, O.; Vizzino, C. Current perspectives on the diagnosis and management of fatigue in multiple sclerosis. Expert Rev. Neurother. 2022, 22, 681–693. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Gillies, J. Repeated forms, testing intervals, and SDMT performance in a large multiple sclerosis dataset. Mult. Scler. Relat. Disord. 2022, 68, 104375. [Google Scholar] [CrossRef]
- Jacobsen, C.; Zivadinov, R. Brain atrophy and clinical characteristics predicting SDMT performance in multiple sclerosis: A 10-year follow-up study. Mult. Scler. J. Exp. Transl. Clin. 2021, 7, 2055217321992394. [Google Scholar] [CrossRef]
- Giovannoni, G.; Tomic, D. ‘No evident disease activity’: The use of combined assessments in the management of patients with multiple sclerosis. Mult. Scler. 2017, 23, 1179–1187. [Google Scholar] [CrossRef]
- Voigt, I.; Inojosa, H. Building a monitoring matrix for the management of multiple sclerosis. Autoimmun. Rev. 2023, 22, 103358. [Google Scholar] [CrossRef]
- Ghobadi, H.; Mohammadshahi, J. Role of leukocytes and systemic inflammation indexes (NLR, PLR, MLP, dNLR, NLPR, AISI, SIR-I, and SII) on admission predicts in-hospital mortality in non-elderly and elderly COVID-19 patients. Front. Med. 2022, 9, 916453. [Google Scholar] [CrossRef] [PubMed]
- Ebrahem, W.A.; Saleh, S.A. Neutrophil to lymphocyte ratio in diagnosis of inflammatory bowel disease and correlation with disease severity assessed by ultrasound and colonoscopy. QJM Int. J. Med. 2021, 114 (Suppl. S1), hcab100-049. [Google Scholar] [CrossRef]
- He, P.; Yang, H. The diagnostic value of blood cell-derived indexes in subacute thyroiditis patients with thyrotoxicosis: A retrospective study. Ann. Transl. Med. 2022, 10, 322. [Google Scholar] [CrossRef]
- Demirci, S.; Demirci, S. The clinical significance of the neutrophil-to-lymphocyte ratio in multiple sclerosis. Int. J. Neurosci. 2016, 126, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Bisgaard, A.K.; Pihl-Jensen, G. The neutrophil-to-lymphocyte ratio as a disease activity marker in multiple sclerosis and optic neuritis. Mult. Scler. Relat. Disord. 2017, 18, 213–217. [Google Scholar] [CrossRef]
- Al-Hussain, F.; Alfallaj, M.M. Relationship between neutrophil-to-lymphocyte ratio and stress in multiple sclerosis patients. J. Clin. Diagn. Res. 2017, 11, CC01. [Google Scholar] [CrossRef] [PubMed]
- Gelibter, S.; Pisa, M.; Croese, T.; Dalla Costa, G.; Orrico, M.; Preziosa, P.; Sangalli, F.; Martinelli, V.; Furlan, R.; Filippi, M. Neutrophil-to-lymphocyte ratio: A marker of neuro-inflammation in multiple sclerosis? J. Neurol. 2021, 268, 717–723. [Google Scholar] [CrossRef]
- Saadeh, R.; Ramos, P. An Update on Laboratory-Based Diagnostic Biomarkers for Multiple Sclerosis and Beyond. Clin. Chem. 2022, 68, 1134–1150. [Google Scholar] [CrossRef]
- Giovannoni, G.; Turner, B. Is it time to target no evident disease activity (NEDA) in multiple sclerosis? Mult. Scler. Relat. Disord. 2015, 4, 329–333. [Google Scholar] [CrossRef]
- Giovannoni, G.; Bermel, R. A brief history of NEDA. Mult. Scler. Relat. Disord. 2018, 20, 228–230. [Google Scholar] [CrossRef]
- Pandit, L. No evidence of disease activity (NEDA) in multiple sclerosis-shifting the goal posts. Ann. Indian Acad. Neurol. 2019, 22, 261. [Google Scholar] [CrossRef] [PubMed]
- Prosperini, L.; Ruggieri, S. Prognostic accuracy of NEDA-3 in long-term outcomes of multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, e1059. [Google Scholar] [CrossRef] [PubMed]
- Adamczyk-Sowa, M.; Adamczyk, B. Secondary progressive multiple sclerosis—From neuropathology to definition and effective treatment. Neurol. Neurochir. Pol. 2020, 54, 384–398. [Google Scholar] [CrossRef] [PubMed]
- Haider, L.; Simeonidou, C. Multiple sclerosis deep grey matter: The relation between demyelination, neurodegeneration, inflammation and iron. J. Neurol. Neurosurg. Psychiatry 2014, 85, 1386–1395. [Google Scholar] [CrossRef]
- Reynolds, R.; Roncaroli, F. The neuropathological basis of clinical progression in multiple sclerosis. Acta Neuropathol. 2011, 122, 155–170. [Google Scholar] [CrossRef]
- Filippi, M.; Preziosa, P. Identifying progression in multiple sclerosis: New perspectives. Ann. Neurol. 2020, 88, 438–452. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Indexes | Formulas |
|---|---|
| NLR | Neutrophil/lymphocyte |
| PLR | Platelet/lymphocyte |
| MLR | Monocyte/lymphocyte |
| SII | Platelet × neutrophil/lymphocyte |
| SIRI | Neutrophil × monocyte/lymphocyte |
| AISI | Neutrophil × platelet × monocyte/lymphocyte |
| Median (Min–Max) | Mean ± SD | |
|---|---|---|
| Monocyte (/µL) | 530 (250–1340) | 569.63 ± 179.94 |
| Lymphocyte (/µL) | 1108 (114–3850) | 1206.06 ± 780.14 |
| Platelet (109/L) | 263 (134–469) | 268.38 ± 58.65 |
| Neutrophil (/µL) | 3790 (1600–9300) | 4081.11 ± 1537.32 |
| CRP (mg/dL) | 2.2 (0.4–9.9) | 2.92 ± 2.28 |
| NLR | 3.33 (1.10–42.86) | 6.22 ± 7.07 |
| PLR | 230.72 (82.67–2447.37) | 430.12 ± 493.19 |
| MLR | 0.49 (0.13–4.56) | 0.88 ± 0.94 |
| SII | 974.25 (234–11,614) | 1703.98 ± 2006.43 |
| SIRI | 1.85 (0.40–24.16) | 3.56 ± 4.16 |
| AISI | 506.10 (107.10–6135.90) | 973.56 ± 1154.85 |
| NEDA-3 (+) | NEDA-3 (−) | p | |
|---|---|---|---|
| NLR | 8.99 ± 8.77 | 3.44 ± 2.57 | <0.001 |
| PLR | 618.54 ± 610.46 | 241.69 ± 214.59 | <0.001 |
| MLR | 1.26 ± 1.14 | 0.49 ± 0.42 | <0.001 |
| SII | 2463.98 ± 2507.99 | 943.97 ± 812.67 | <0.001 |
| SIRI | 5.22 ± 5.19 | 1.90 ± 1.51 | <0.001 |
| AISI | 1426 ± 33 | 520.77 ± 459.56 | <0.001 |
| rho | p | |
|---|---|---|
| NLR and PLR | 0.876 | <0.001 |
| NLR and MLR | 0.834 | <0.001 |
| NLR and SII | 0.962 | <0.001 |
| NLR and SIRI | 0.908 | <0.001 |
| NLR and AISI | 0.887 | <0.001 |
| SII and SIRI | 0.888 | <0.001 |
| SII and AISI | 0.929 | <0.001 |
| AISI and SIRI | 0.969 | <0.001 |
| p Value | Odds Ratio (OR) | 95% CI for EXP (B) (Lower–Upper) | Accuracy | Nagelkerke R Square | Cox & Snell R Square | |
|---|---|---|---|---|---|---|
| AISI | <0.001 | 1.001 | 1.001–1.002 | 69.4% | 0.255 | 0.191 |
| SII | 0.001 | 1.001 | 1.000–1.001 | 67.6% | 0.245 | 0.184 |
| SIRI | <0.001 | 1.511 | 1.216–1.877 | 68.5% | 0.281 | 0.211 |
| DMT | Lymphocyte Values (/µL) |
|---|---|
| Interferon (n = 8) | 1145.50 ± 574.27 |
| Glatiramer acetate (n = 6) | 2061.67 ± 1207.36 |
| Teriflunomide (n = 22) | 1297.45 ± 859.62 |
| Dimethylfumarate (n = 9) | 1327.00 ± 748.84 |
| Fingolimod (n = 39) | 750.92 ± 418.83 |
| Ocrelizumab (n = 5) | 1491.40 ± 735.71 |
| Cladribine (n = 6) | 926.83 ± 442.33 |
| Natalizumab (n = 3) | 1700.00 ± 1131.37 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bunul, S.D.; Alagoz, A.N.; Piri Cinar, B.; Bunul, F.; Erdogan, S.; Efendi, H. A Preliminary Study on the Meaning of Inflammatory Indexes in MS: A Neda-Based Approach. J. Pers. Med. 2023, 13, 1537. https://doi.org/10.3390/jpm13111537
Bunul SD, Alagoz AN, Piri Cinar B, Bunul F, Erdogan S, Efendi H. A Preliminary Study on the Meaning of Inflammatory Indexes in MS: A Neda-Based Approach. Journal of Personalized Medicine. 2023; 13(11):1537. https://doi.org/10.3390/jpm13111537
Chicago/Turabian StyleBunul, Sena Destan, Aybala Neslihan Alagoz, Bilge Piri Cinar, Fatih Bunul, Seyma Erdogan, and Husnu Efendi. 2023. "A Preliminary Study on the Meaning of Inflammatory Indexes in MS: A Neda-Based Approach" Journal of Personalized Medicine 13, no. 11: 1537. https://doi.org/10.3390/jpm13111537