
Predicting Problematic Behavior in Autism Spectrum Disorder Using Medical History and Environmental Data
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort Selection and Data Inclusion Criteria
2.2. Details of Longitudinal Data Used
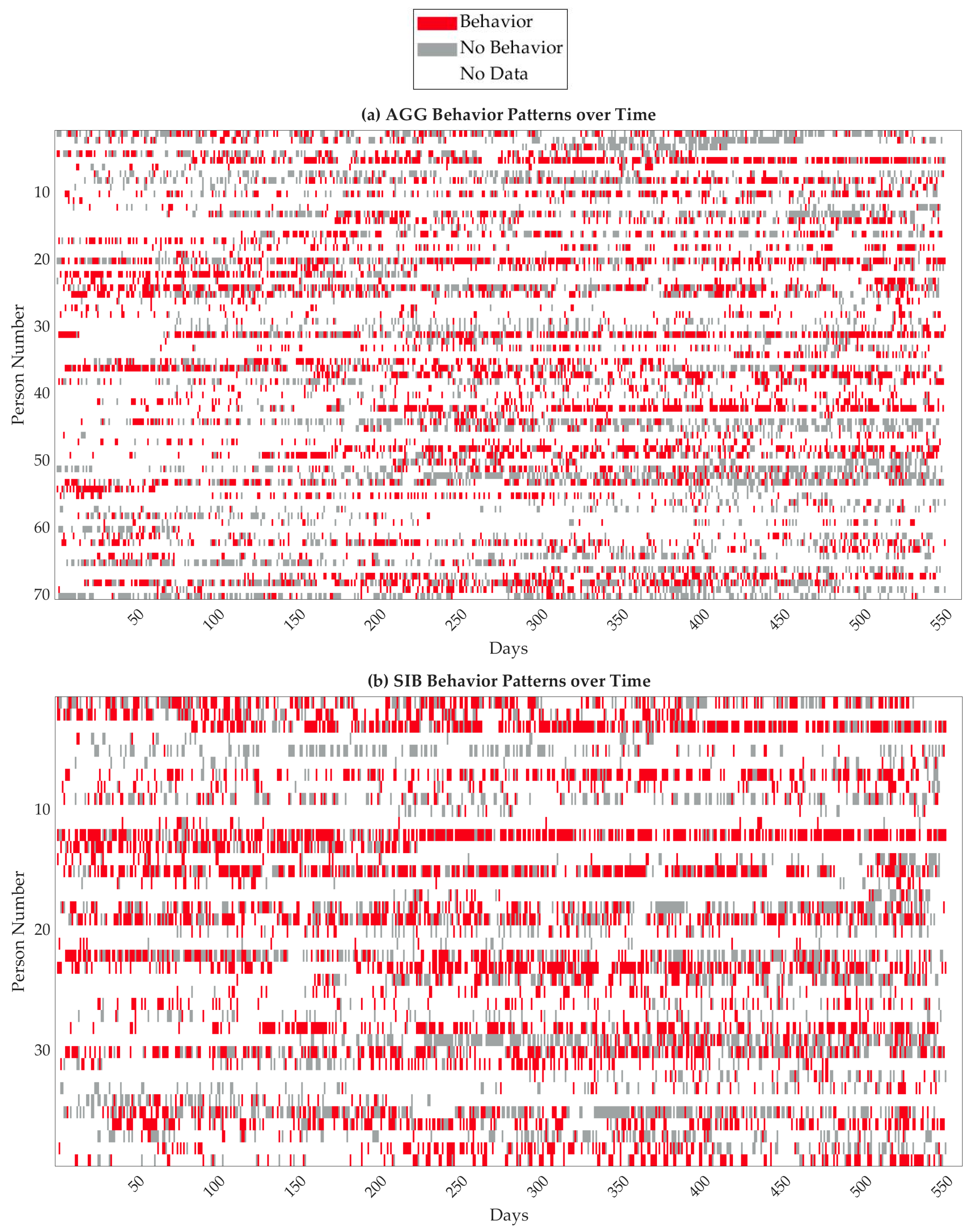
2.2.1. Data on Exhibited Behaviors
2.2.2. Sleep Variables
2.2.3. Gastrointestinal Variables
2.2.4. Environment Variables
2.2.5. Allergen
2.2.6. Weather
2.2.7. Lunar Cycle
2.3. Feature Engineering and Variable Selection
2.4. Modeling Methods, Model Validation and Model Selection
2.5. Reproducibility
3. Results
3.1. Data Pre-Processing and Results from Sensitivity Analysis and Data Reduction
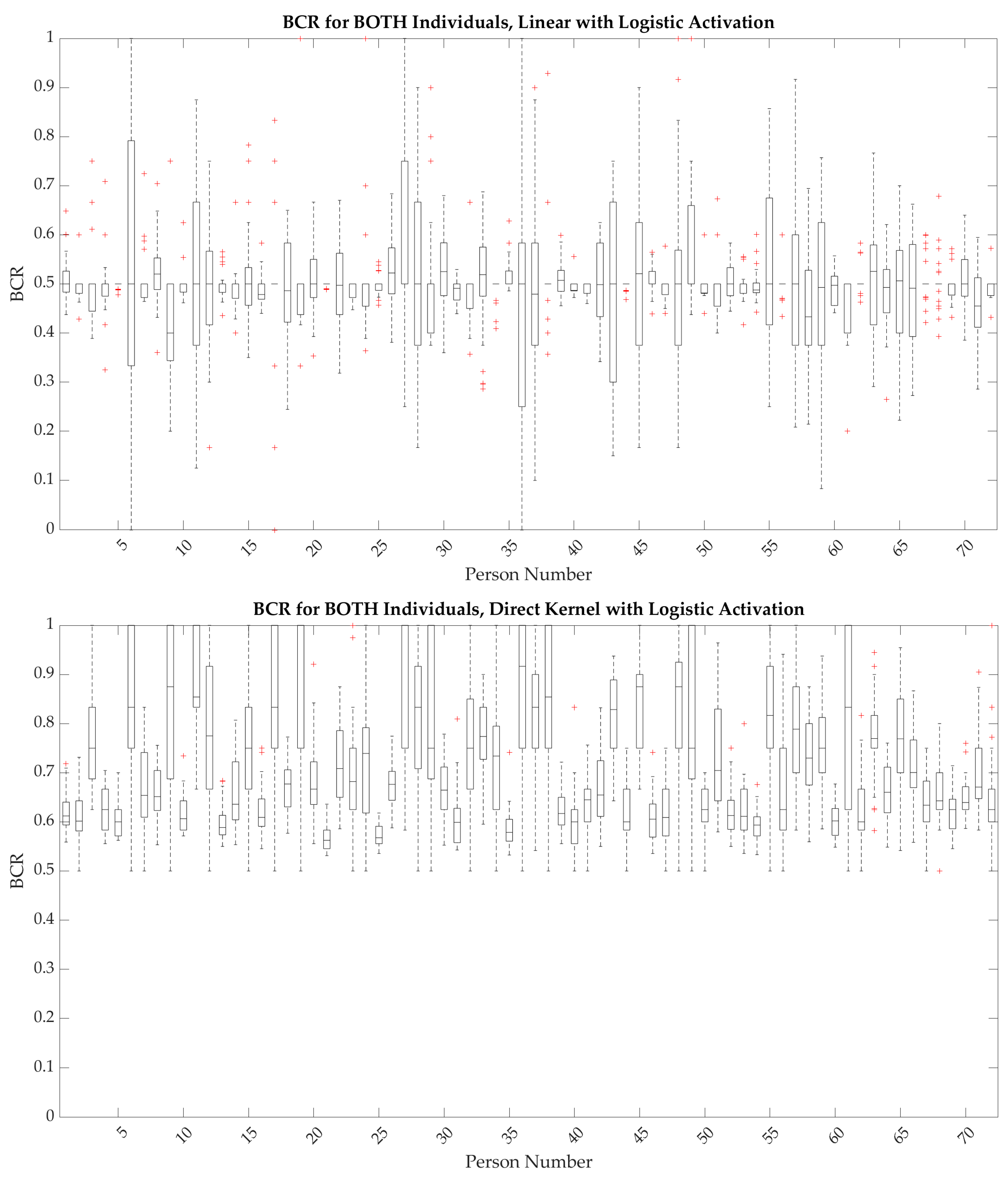
3.2. Linear Analysis Using Original Variables
3.3. Nonlinear Analysis Using Direct Kernel Transformation
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Description |
|---|---|
| Weather_TMAX | Maximum temperature (degrees F) in a day |
| Weather_TMIN | Minimum temperature (degrees F) in a day |
| Weather_PRCP | Amount of precipitation (inches) in a day |
| Weather_SNOW | Amount of snow (inches) in a day |
| Weather_SNWD | Depth of snow (inches) that day |
| Moon Rise | Time of the moon rising (percentage of 24 h, with 0 as midnight) |
| Moon Culmination | Time when the moon crosses the meridian (percentage of 24 h, with 0 as midnight) |
| Moon Set | Time of the moon setting (percentage of 24 h, with 0 as midnight) |
| Moon Altitude | The angle between the center of the moon and the horizon accounting for refraction, in degrees |
| Moon Azimuth | The angle taken between the earth at the meridian plane and the moon at the vertical plane, in degrees |
| Moon Shadow Length | Length of the shadow of the moon for a 1 m tall object, when visible (meters); when not visible, coded as 0 |
| Moon Distance | Distance from the centers of the earth and the moon in kilometers |
| Moon Phase | Percent illumination of the moon that day |
| Moon Age | Age of the moon in a range from 0 (new moon) to 1 (full moon) |
| Moon Next New | Days until the next new moon |
| Moon Next Full | Days until the next full moon |
| Allergen_Trees | Pollen counts of tree species that day |
| Allergen_Weeds | Pollen counts of weed species that day |
| Allergen_Grasses | Pollen counts of grass species that day |
| Allergen_Total | Summed pollen counts across trees, weeds, and grasses |
| Sleep_Hours | Duration of sleep in a night (hours) |
| Sleep_Interruptions | Number of night awakenings in a night |
| BM_Count | Number of BMs in a day |
| BM_Bristol_Extreme | Largest absolute Bristol difference from 3.5 (the averaged ideal Bristol scores of 3 and 4), calculated from the Bristol max or min that day; 3.5 if none (as Bristol is coded as 0 in that case) |
| BM_Bristol_Max | The maximum Bristol reading across BMs in a day; 0 if none |
| BM_Bristol_Min | The minimum Bristol reading across BMs in a day; 0 if none |
| BM_Bristol | The average Bristol reading across BMs in a day; 0 if none |
| BM_Intervention | Whether or not the individual was given some form of medication or diet change for constipation or diarrhea |
| BM_Time | Time of the latest BM that day |
| BM_Abnormal | Whether someone had constipation, diarrhea, over 3 BMs, or no BMs that day |
| BM_Constipation | Whether or not the individual had BMs with a Bristol < 3 that day, or no BM |
| BM_Diarrhea | Whether or not the individual had BMs with a Bristol >5 that day, or >3BMs |
| Menses | Whether or not the individual was menstruating that day |
References
- Maenner, M.J.; Warren, Z.; Robinson Williams, A.; Amoakohene, E.; Bakian, A.V.; Bilder, D.A.; Durkin, M.S.; Fitzgerald, R.T.; Furnier, S.M.; Hughes, M.M.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. MMWR Surveill. Summ. 2023, 72, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Faras, H.; Al Ateeqi, N.; Tidmarsh, L. Autism spectrum disorders. Ann. Saudi Med. 2010, 30, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Dominick, K.C.; Davis, N.O.; Lainhart, J.; Tager-Flusberg, H.; Folstein, S. Atypical behaviors in children with autism and children with a history of language impairment. Res. Dev. Disabil. 2007, 28, 145–162. [Google Scholar] [CrossRef] [PubMed]
- Tye, C.; Runicles, A.K.; Whitehouse, A.J.O.; Alvares, G.A. Characterizing the Interplay Between Autism Spectrum Disorder and Comorbid Medical Conditions: An Integrative Review. Front. Psychiatry 2018, 9, 751. [Google Scholar] [CrossRef]
- Vargason, T.; Grivas, G.; Hollowood-Jones, K.L.; Hahn, J. Towards a Multivariate Biomarker-Based Diagnosis of Autism Spectrum Disorder: Review and Discussion of Recent Advancements. Semin. Pediatr. Neurol. 2020, 34, 100803. [Google Scholar] [CrossRef]
- Richdale, A.L.; Prior, M.R. The sleep/wake rhythm in children with autism. Eur. Child Adolesc. Psychiatry 1995, 4, 175–186. [Google Scholar] [CrossRef]
- Leader, G.; Tuohy, E.; Chen, J.L.; Mannion, A.; Gilroy, S.P. Feeding Problems, Gastrointestinal Symptoms, Challenging Behavior and Sensory Issues in Children and Adolescents with Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 1401–1410. [Google Scholar] [CrossRef]
- Hughes, H.K.; Mills Ko, E.; Rose, D.; Ashwood, P. Immune Dysfunction and Autoimmunity as Pathological Mechanisms in Autism Spectrum Disorders. Front. Cell. Neurosci. 2018, 12, 405. [Google Scholar] [CrossRef]
- Hodgetts, S.; Nicholas, D.; Zwaigenbaum, L. Home sweet home? Families’ experiences with aggression in children with autism spectrum disorders. Focus Autism Other Dev. Disabil. 2013, 28, 166–174. [Google Scholar] [CrossRef]
- Fitzpatrick, S.E.; Srivorakiat, L.; Wink, L.K.; Pedapati, E.V.; Erickson, C.A. Aggression in autism spectrum disorder: Presentation and treatment options. Neuropsychiatr. Dis. Treat. 2016, 12, 1525–1538. [Google Scholar] [CrossRef]
- Minshawi, N.F.; Hurwitz, S.; Fodstad, J.C.; Biebl, S.; Morriss, D.H.; McDougle, C.J. The association between self-injurious behaviors and autism spectrum disorders. Psychol. Res. Behav. Manag. 2014, 7, 125–136. [Google Scholar] [CrossRef]
- Brown, C.J.; Kawahara, J.; Hamarneh, G. Connectome priors in deep neural networks to predict autism. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018. [Google Scholar]
- Cohen, S.; Fulcher, B.D.; Rajaratnam, S.M.W.; Conduit, R.; Sullivan, J.P.; St Hilaire, M.A.; Phillips, A.J.K.; Loddenkemper, T.; Kothare, S.V.; McConnell, K.; et al. Sleep patterns predictive of daytime challenging behavior in individuals with low-functioning autism. Autism Res. 2018, 11, 391–403. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Kanne, S.M.; Wodka, E.L. Physical aggression in children and adolescents with autism spectrum disorders. Res. Autism Spectr. Disord. 2013, 7, 455–465. [Google Scholar] [CrossRef]
- Kanne, S.M.; Mazurek, M.O. Aggression in Children and Adolescents with ASD: Prevalence and Risk Factors. J. Autism Dev. Disord. 2011, 41, 926–937. [Google Scholar] [CrossRef]
- Laverty, C.; Oliver, C.; Moss, J.; Nelson, L.; Richards, C. Persistence and predictors of self-injurious behaviour in autism: A ten-year prospective cohort study. Mol. Autism 2020, 11, 8. [Google Scholar] [CrossRef]
- Richards, C.; Oliver, C.; Nelson, L.; Moss, J. Self-injurious behaviour in individuals with autism spectrum disorder and intellectual disability. J. Intellect. Disabil. Res. 2012, 56, 476–489. [Google Scholar] [CrossRef] [PubMed]
- Malhi, P.; Sankhyan, N. Intentional Self Harm in Children with Autism. Indian J. Pediatr. 2021, 88, 158–160. [Google Scholar] [CrossRef]
- Matson, J.L.; Boisjoli, J.; Mahan, S. The Relation of Communication and Challenging Behaviors in Infants and Toddlers with Autism Spectrum Disorders. J. Dev. Phys. Disabil. 2009, 21, 253–261. [Google Scholar] [CrossRef]
- Duerden, E.G.; Oatley, H.K.; Mak-Fan, K.M.; McGrath, P.A.; Taylor, M.J.; Szatmari, P.; Roberts, S.W. Risk Factors Associated with Self-Injurious Behaviors in Children and Adolescents with Autism Spectrum Disorders. J. Autism Dev. Disord. 2012, 42, 2460–2470. [Google Scholar] [CrossRef] [PubMed]
- Moseley, R.L.; Gregory, N.J.; Smith, P.; Allison, C.; Baron-Cohen, S. A ‘choice’, an ‘addiction’, a way ‘out of the lost’: Exploring self-injury in autistic people without intellectual disability. Mol. Autism 2019, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Moseley, R.L.; Gregory, N.J.; Smith, P.; Allison, C.; Baron-Cohen, S. Links between self-injury and suicidality in autism. Mol. Autism 2020, 11, 14. [Google Scholar] [CrossRef] [PubMed]
- Iwata, B.A.; Pace, G.M.; Dorsey, M.F.; Zarcone, J.R.; Vollmer, T.R.; Smith, R.G.; Rodgers, T.A.; Lerman, D.C.; Shore, B.A.; Mazaleski, J.L.; et al. The functions of self-injurious behavior: An experimental-epidemiological analysis. J. Appl. Behav. Anal. 1994, 27, 215–240. [Google Scholar] [CrossRef]
- Northrup, J.B.; Goodwin, M.S.; Peura, C.B.; Chen, Q.; Taylor, B.J.; Siegel, M.S.; Mazefsky, C.A. Mapping the time course of overt emotion dysregulation, self-injurious behavior, and aggression in psychiatrically hospitalized autistic youth: A naturalistic study. Autism Res. 2022, 15, 1855–1867. [Google Scholar] [CrossRef]
- Vitale, S.R.; Schneider, H.; Gardner, L.; Alessandri, M.; Marker, C. Challenging Behavior and Parental Depression: The Effects of Everyday Stressors and Benefit Finding for Parents of Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2023, 53, 3356–3368. [Google Scholar] [CrossRef]
- Frazier, T.W.; Crowley, E.; Shih, A.; Vasudevan, V.; Karpur, A.; Uljarevic, M.; Cai, R.Y. Associations between executive functioning, challenging behavior, and quality of life in children and adolescents with and without neurodevelopmental conditions. Front. Psychol. 2022, 13, 1022700. [Google Scholar] [CrossRef]
- Nuske, H.J.; Young, A.V.; Khan, F.; Palermo, E.H.; Ajanaku, B.; Pellecchia, M.; Vivanti, G.; Mazefsky, C.A.; Brookman-Frazee, L.; McPartland, J.C.; et al. Systematic Review: Emotion Dysregulation and Challenging Behavior Interventions for Children and Adolescents with Autism with Graded Key Evidence-Based Strategy Recommendations. Eur. Child Adolesc Psychicatr. 2023. [Google Scholar] [CrossRef]
- Siegel, M.; Gabriels, R.L. Psychiatric hospital treatment of children with autism and serious behavioral disturbance. Child Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 125–142. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, R.; McGuire, B.E.; Lydon, H.K. Improving pain-related communication in children with autism spectrum disorder and intellectual disability. Paediatr. Neonatal Pain 2022, 4, 22–32. [Google Scholar] [CrossRef]
- Courtemanche, A.B.; Black, W.R. Everyday expressions of pain in children with and without autism spectrum disorder. Res. Autism Spectr. Disord. 2016, 26, 65–70. [Google Scholar] [CrossRef]
- Carr, E.G.; Owen-Deschryver, J.S. Physical illness, pain, and problem behavior in minimally verbal people with developmental disabilities. J. Autism Dev. Disord. 2007, 37, 413–424. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.; Sigafoos, J.; Lancioni, G.; Edrisinha, C.; Andrews, A. An examination of the effects of a classroom activity schedule on levels of self-injury and engagement for a child with severe autism. J. Autism Dev. Disord. 2005, 35, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Machalicek, W.; O’Reilly, M.F.; Beretvas, N.; Sigafoos, J.; Lancioni, G.E. A review of interventions to reduce challenging behavior in school settings for students with autism spectrum disorders. Res. Autism Spectr. Disord. 2007, 1, 229–246. [Google Scholar] [CrossRef]
- Heyvaert, M.; Maes, B.; Van den Noortgate, W.; Kuppens, S.; Onghena, P. A multilevel meta-analysis of single-case and small-n research on interventions for reducing challenging behavior in persons with intellectual disabilities. Res. Dev. Disabil. 2012, 33, 766–780. [Google Scholar] [CrossRef] [PubMed]
- 42 CFR 438.35. Code of Federal Regulations. National Archives. Available online: https://www.ecfr.gov/current/title-42 (accessed on 31 August 2023).
- Goodwin, M.S.; Mazefsky, C.A.; Ioannidis, S.; Erdogmus, D.; Siegel, M. Predicting aggression to others in youth with autism using a wearable biosensor. Autism Res. 2019, 12, 1286–1296. [Google Scholar] [CrossRef] [PubMed]
- Cantin-Garside, K.D.; Kong, Z.; White, S.W.; Antezana, L.; Kim, S.; Nussbaum, M.A. Detecting and Classifying Self-injurious Behavior in Autism Spectrum Disorder Using Machine Learning Techniques. J. Autism Dev. Disord. 2020, 50, 4039–4052. [Google Scholar] [CrossRef]
- Alivar, A.; Carlson, C.; Suliman, A.; Warren, S.; Prakash, P.; Thompson, D.E.; Natarajan, B. A Pilot Study on Predicting Daytime Behavior & Sleep Quality in Children with ASD. In Proceedings of the 2019 IEEE Signal Processing in Medicine and Biology Symposium (SPMB), Philadelphia, PA, USA, 7 December 2019; pp. 1–5. [Google Scholar]
- Alivar, A.; Carlson, C.; Suliman, A.; Warren, S.; Prakash, P.; Thompson, D.E.; Natarajan, B. Smart bed based daytime behavior prediction in Children with autism spectrum disorder—A Pilot Study. Med. Eng. Phys. 2020, 83, 15–25. [Google Scholar] [CrossRef]
- Carlson, C.; Suliman, A.; Alivar, A.; Prakash, P.; Thompson, D.; Natarajan, B.; Warren, S. A Pilot Study of an Unobtrusive Bed-Based Sleep Quality Monitor for Severely Disabled Autistic Children. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 4343–4346. [Google Scholar]
- Russell, G.; Mandy, W.; Elliott, D.; White, R.; Pittwood, T.; Ford, T. Selection bias on intellectual ability in autism research: A cross-sectional review and meta-analysis. Mol. Autism 2019, 10, 9. [Google Scholar] [CrossRef]
- Jack, A.; Pelphrey, K.A. Annual Research Review: Understudied populations within the autism spectrum—Current trends and future directions in neuroimaging research. J. Child Psychol. Psychiatry 2017, 58, 411–435. [Google Scholar] [CrossRef]
- Thurm, A.; Farmer, C.; Salzman, E.; Lord, C.; Bishop, S. State of the Field: Differentiating Intellectual Disability From Autism Spectrum Disorder. Front. Psychiatry 2019, 10, 526. [Google Scholar] [CrossRef]
- Stedman, A.; Taylor, B.; Erard, M.; Peura, C.; Siegel, M. Are Children Severely Affected by Autism Spectrum Disorder Underrepresented in Treatment Studies? An Analysis of the Literature. J. Autism Dev. Disord. 2019, 49, 1378–1390. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Charman, T.; Havdahl, A.; Carbone, P.; Anagnostou, E.; Boyd, B.; Carr, T.; de Vries, P.J.; Dissanayake, C.; Divan, G.; et al. The Lancet Commission on the future of care and clinical research in autism. Lancet 2022, 399, 271–334. [Google Scholar] [CrossRef] [PubMed]
- Beavers, G.A.; Iwata, B.A.; Lerman, D.C. Thirty years of research on the functional analysis of problem behavior. J. Appl. Behav. Anal. 2013, 46, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.M.; Rodriguez, B.J.; Campbell, A. Functional Behavior Assessment in Schools: Current Status and Future Directions. J. Behav. Educ. 2015, 24, 338–371. [Google Scholar] [CrossRef]
- Hagopian, L.P.; Rooker, G.W.; Jessel, J.; DeLeon, I.G. Initial functional analysis outcomes and modifications in pursuit of differentiation: A summary of 176 inpatient cases. J. Appl. Behav. Anal. 2013, 46, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Hagopian, L.P.; Rooker, G.W.; Zarcone, J.R.; Bonner, A.C.; Arevalo, A.R. Further analysis of subtypes of automatically reinforced SIB: A replication and quantitative analysis of published datasets. J. Appl. Behav. Anal. 2017, 50, 48–66. [Google Scholar] [CrossRef]
- Kennedy, C.H.; Meyer, K.A.; Knowles, T.; Shukla, S. Analyzing the multiple functions of stereotypical behavior for students with autism: Implications for assessment and treatment. J. Appl. Behav. Anal. 2000, 33, 559–571. [Google Scholar] [CrossRef]
- Day, H.M.; Horner, R.H.; O’Neill, R.E. Multiple functions of problem behaviors: Assessment and intervention. J. Appl. Behav. Anal. 1994, 27, 279–289. [Google Scholar] [CrossRef]
- Haring, T.G.; Kennedy, C.H. Contextual control of problem behavior in students with severe disabilities. J. Appl. Behav. Anal. 1990, 23, 235–243. [Google Scholar] [CrossRef]
- Smith, R.G.; Iwata, B.A.; Vollmer, T.R.; Zarcone, J.R. Experimental analysis and treatment of multiply controlled self-injury. J. Appl. Behav. Anal. 1993, 26, 183–196. [Google Scholar] [CrossRef]
- Abel, E.A.; Schwichtenberg, A.J.; Brodhead, M.T.; Christ, S.L. Sleep and Challenging Behaviors in the Context of Intensive Behavioral Intervention for Children with Autism. J. Autism Dev. Disord. 2018, 48, 3871–3884. [Google Scholar] [CrossRef]
- Goldman, S.E.; Richdale, A.L.; Clemons, T.; Malow, B.A. Parental Sleep Concerns in Autism Spectrum Disorders: Variations from Childhood to Adolescence. J. Autism Dev. Disord. 2012, 42, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Mayes, S.D.; Calhoun, S.L. Variables related to sleep problems in children with autism. Res. Autism Spectr. Disord. 2009, 3, 931–941. [Google Scholar] [CrossRef]
- Piazza, C.C.; Fisher, W.W.; Kahng, S.W. Sleep patterns in children and young adults with mental retardation and severe behavior disorders. Dev. Med. Child Neurol. 1996, 38, 335–344. [Google Scholar] [CrossRef]
- Symons, F.J.; Davis, M.L.; Thompson, T. Self-injurious behavior and sleep disturbance in adults with developmental disabilities. Res. Dev. Disabil. 2000, 21, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Saghir, Z.; Syeda, J.N.; Muhammad, A.S.; Balla Abdalla, T.H. The Amygdala, Sleep Debt, Sleep Deprivation, and the Emotion of Anger: A Possible Connection? Cureus 2018, 10, e2912. [Google Scholar] [CrossRef]
- Bauducco, S.V.; Flink, I.K.; Jansson-Fröjmark, M.; Linton, S.J. Sleep duration and patterns in adolescents: Correlates and the role of daily stressors. Sleep Health 2016, 2, 211–218. [Google Scholar] [CrossRef]
- Adams, J.B.; Johansen, L.J.; Powell, L.D.; Quig, D.; Rubin, R.A. Gastrointestinal flora and gastrointestinal status in children with autism—Comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011, 11, 22. [Google Scholar] [CrossRef]
- Maenner, M.J.; Arneson, C.L.; Levy, S.E.; Kirby, R.S.; Nicholas, J.S.; Durkin, M.S. Brief Report: Association Between Behavioral Features and Gastrointestinal Problems Among Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2012, 42, 1520–1525. [Google Scholar] [CrossRef]
- Kang, D.W.; Adams, J.B.; Gregory, A.C.; Borody, T.; Chittick, L.; Fasano, A.; Khoruts, A.; Geis, E.; Maldonado, J.; McDonough-Means, S.; et al. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: An open-label study. Microbiome 2017, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.J.; Heaton, K.W. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. 1997, 32, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Horner, R.D. The effects of an environmental “enrichment” program on the behavior of institutionalized profoundly retarded children. J. Appl. Behav. Anal. 1980, 13, 473–491. [Google Scholar] [CrossRef]
- American Academy of Allergy, Asthma & Immunology. Available online: https://www.aaaai.org/ (accessed on 1 July 2023).
- Robinson, G.S. National Allergy Bureau. The Louis Calder Center, Armonk, NY 10504. Available online: https://pollen.aaaai.org/#/station/49f7aa31-07fb-4bc0-86e8-314f6aa9c344 (accessed on 1 July 2023).
- Menne, M.J.; Durre, I.; Korzeniewski, B.; McNeill, S.; Thomas, K.; Yin, X.; Anthony, S.; Ray, R.; Vose, R.S.; Gleason, B.E.; et al. Global Historical Climatology Network-Daily (GHCN-Daily), Version 3.29; CITY:US360017; NOAA National Climatic Data Center: Asheville, NC, USA, 2012. [CrossRef]
- Menne, M.J.; Durre, I.; Vose, R.S.; Gleason, B.E.; Houston, T.G. An Overview of the Global Historical Climatology Network-Daily Database. J. Atmos. Ocean. Technol. 2012, 29, 897–910. [Google Scholar] [CrossRef]
- Bolton, M.J.; Blumberg, W.G.; Ault, L.K.; Mogil, H.M.; Hanes, S.H. Initial Evidence for Increased Weather Salience in Autism Spectrum Conditions. Weather. Clim. Soc. 2020, 12, 293–307. [Google Scholar] [CrossRef]
- VanBuskirk, S.E.; Simpson, R.L. Meteorological Variables and Behavior of Learners with Autism: An Examination of Possible Relationships. Focus Autism Other Dev. Disabil. 2013, 28, 131–137. [Google Scholar] [CrossRef]
- Cajochen, C.; Altanay-Ekici, S.; Münch, M.; Frey, S.; Knoblauch, V.; Wirz-Justice, A. Evidence that the Lunar Cycle Influences Human Sleep. Curr. Biol. 2013, 23, 1485–1488. [Google Scholar] [CrossRef]
- Hoffmann, T. MoonCalc.org. Torsten Hoffman, 2014–2022. Available online: https://www.mooncalc.org/ (accessed on 1 March 2023).
- Rise, Set, and Twilight Definitions. Astronomical Applications Department, U.S. Naval Observatory, Washington, DC 20392. Available online: https://aa.usno.navy.mil/faq/RST_defs (accessed on 1 July 2023).
- Widrow, B. An Adaptive “ADALINE” Neuron Using Chemical “Memistors”; Stanford University: Stanford, CA, USA, 1960. [Google Scholar]
- Pareto, V. Manuale di Economia Politica; Societa Editrice: Milano, Italy, 1906. [Google Scholar]
- Röösli, M.; Jüni, P.; Braun-Fahrländer, C.; Brinkhof, M.W.G.; Low, N.; Egger, M. Sleepless night, the moon is bright: Longitudinal study of lunar phase and sleep. J. Sleep Res. 2006, 15, 149–153. [Google Scholar] [CrossRef]
- Haba-Rubio, J.; Marques-Vidal, P.; Tobback, N.; Andries, D.; Preisig, M.; Kuehner, C.; Vollenweider, P.; Waeber, G.; Luca, G.; Tafti, M.; et al. Bad sleep? Don’t blame the moon! A population-based study. Sleep Med. 2015, 16, 1321–1326. [Google Scholar] [CrossRef]
- Ghaziuddin, M.; Elkins, T.E.; McNeeley, S.G.; Ghaziuddin, N. Premenstrual Syndrome in Women with Mental Handicap: A Pilot Study. Br. J. Dev. Disabil. 1993, 39, 104–107. [Google Scholar] [CrossRef]
- Carr, E.G.; Smith, C.E. Biological setting events for self-injury. Ment. Retard. Dev. Disabil. Res. Rev. 1995, 1, 94–98. [Google Scholar] [CrossRef]
- Vargason, T.; McGuinness, D.L.; Hahn, J. Gastrointestinal Symptoms and Oral Antibiotic Use in Children with Autism Spectrum Disorder: Retrospective Analysis of a Privately Insured U.S. Population. J. Autism Dev. Disord. 2019, 49, 647–659. [Google Scholar] [CrossRef]
- Fulceri, F.; Morelli, M.; Santocchi, E.; Cena, H.; Del Bianco, T.; Narzisi, A.; Calderoni, S.; Muratori, F. Gastrointestinal symptoms and behavioral problems in preschoolers with Autism Spectrum Disorder. Dig. Liver Dis. 2016, 48, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Mazefsky, C.A.; Schreiber, D.R.; Olino, T.M.; Minshew, N.J. The association between emotional and behavioral problems and gastrointestinal symptoms among children with high-functioning autism. Autism 2014, 18, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Edelson, S.M. Comparison of Autistic Individuals Who Engage in Self-Injurious Behavior, Aggression, and Both Behaviors. Pediatr. Rep. 2021, 13, 558–565. [Google Scholar] [CrossRef]
- Kennedy, C.H.; Meyer, K.A. Sleep deprivation, allergy symptoms, and negatively reinforced problem behavior. J. Appl. Behav. Anal. 1996, 29, 133–135. [Google Scholar] [CrossRef]
- Buie, T.; Campbell, D.B.; Fuchs, G.J., III; Furuta, G.T.; Levy, J.; VandeWater, J.; Whitaker, A.H.; Atkins, D.; Bauman, M.L.; Beaudet, A.L.; et al. Evaluation, Diagnosis, and Treatment of Gastrointestinal Disorders in Individuals With ASDs: A Consensus Report. Pediatrics 2010, 125, S1–S18. [Google Scholar] [CrossRef] [PubMed]
- Bergmeir, C.; Benítez, J.M. On the use of cross-validation for time series predictor evaluation. Inf. Sci. 2012, 191, 192–213. [Google Scholar] [CrossRef]











| Cohort | Sex (Male; Female) | Age Range |
|---|---|---|
| AGG | 59; 11 | 9.63–18.81 |
| SIB | 32; 7 | 11.00–18.81 |
| BOTH | 59; 13 | 9.63–18.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferina, J.; Kruger, M.; Kruger, U.; Ryan, D.; Anderson, C.; Foster, J.; Hamlin, T.; Hahn, J. Predicting Problematic Behavior in Autism Spectrum Disorder Using Medical History and Environmental Data. J. Pers. Med. 2023, 13, 1513. https://doi.org/10.3390/jpm13101513
Ferina J, Kruger M, Kruger U, Ryan D, Anderson C, Foster J, Hamlin T, Hahn J. Predicting Problematic Behavior in Autism Spectrum Disorder Using Medical History and Environmental Data. Journal of Personalized Medicine. 2023; 13(10):1513. https://doi.org/10.3390/jpm13101513
Chicago/Turabian StyleFerina, Jennifer, Melanie Kruger, Uwe Kruger, Daniel Ryan, Conor Anderson, Jenny Foster, Theresa Hamlin, and Juergen Hahn. 2023. "Predicting Problematic Behavior in Autism Spectrum Disorder Using Medical History and Environmental Data" Journal of Personalized Medicine 13, no. 10: 1513. https://doi.org/10.3390/jpm13101513