
Surgical Technique of Central and Over-the-Top Full-Endoscopic Decompression of the Cervical Spine: A Technical Note

 , , and
, , and
Abstract
:1. Introduction
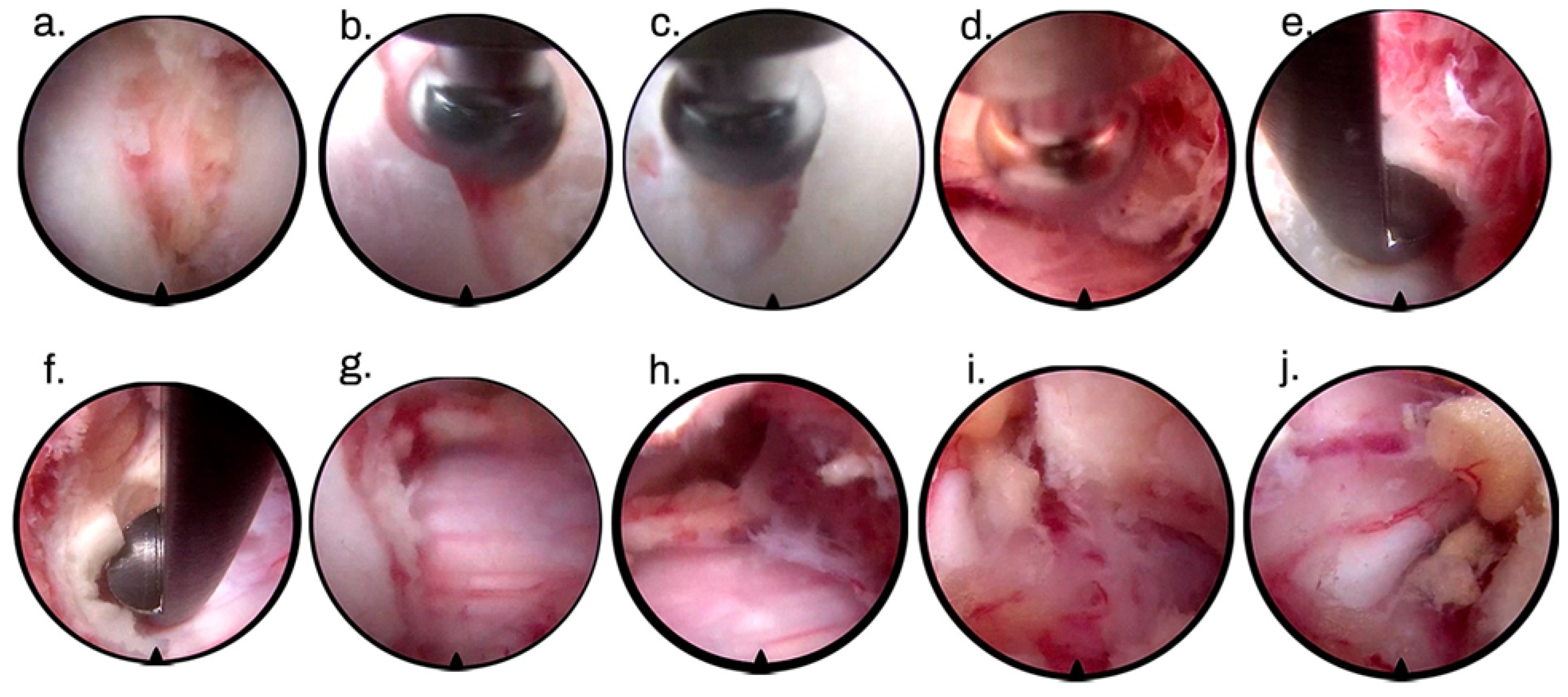
2. Surgical Technique
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Full-endoscopic cervical posterior foraminotomy for the operation of lateral disc herniations using 5.9-mm endoscopes: A prospective, randomized, controlled study. Spine 2008, 33, 940–948. [Google Scholar] [CrossRef]
- Gatam, A.R.; Gatam, L.; Phedy; Mahadhipta, H.; Luthfi, O.; Ajiantoro; Husin, S.; Aprilya, D. Full Endoscopic Posterior Cervical Foraminotomy in Management of Foraminal Disc Herniation and Foraminal Stenosis. Orthop. Res. Rev. 2022, 14, 1–7. [Google Scholar] [CrossRef]
- Foley, K.T.; Smith, M.M. Microendoscopic Discectomy. Tech. Neurosurg. 1997, 3, 301–307. [Google Scholar]
- Yeung, A.T. The Evolution and Advancement of Endoscopic Foraminal Surgery: One Surgeon’s Experience Incorporating Adjunctive Techologies. SAS J. 2007, 1, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Wirth, F.; Bergamaschi, E.C.Q.A.; Forti, F.S.; Bergamaschi, J.P.M. Development of Indications for Endoscopic Spine Surgery: An Overview. Int. J. Transl. Med. 2023, 3, 321–333. [Google Scholar]
- Carr, D.A.; Abecassis, I.J.; Hofstetter, C.P. Full endoscopic unilateral laminotomy for bilateral decompression of the cervical spine: Surgical technique and early experience. J. Spine Surg. 2020, 6, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Gibson, J.N.A.; Subramanian, A.S.; Scott, C.E.H. A randomised controlled trial of transforaminal endoscopic discectomy vs. microdiscectomy. Eur. Spine J. 2017, 26, 847–856. [Google Scholar] [CrossRef]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: A prospective, randomized, controlled study. Spine 2008, 33, 931–939. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, L.; Dong, J.; Xie, P.; Liu, B.; Wang, Q.; Chen, R.; Feng, F.; Yang, B.; Shu, T.; et al. Percutaneous transforaminal endoscopic discectomy compared with microendoscopic discectomy for lumbar disc herniation: 1-year results of an ongoing randomized controlled trial. J. Neurosurg. Spine 2018, 28, 300–310. [Google Scholar] [CrossRef]
- McGrath, L.B.; White-Dzuro, G.A.; Hofstetter, C.P. Comparison of clinical outcomes following minimally invasive or lumbar endoscopic unilateral laminotomy for bilateral decompression. J. Neurosurg. Spine 2019, 30, 491–499. [Google Scholar] [CrossRef]
- Wan, Q.; Zhang, D.; Li, S.; Liu, W.; Wu, X.; Ji, Z.; Ru, B.; Cai, W. Posterior percutaneous full-endoscopic cervical discectomy under local anesthesia for cervical radiculopathy due to soft-disc herniation: A preliminary clinical study. J. Neurosurg. Spine 2018, 29, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Liu, K.; Chu, L.; Chen, L.; Deng, Z. Posterior percutaneous endoscopic cervical discectomy through lamina-hole approach for cervical intervertebral disc herniation. Int. J. Neurosci. 2019, 129, 627–634. [Google Scholar] [CrossRef]
- Ruan, W.; Feng, F.; Liu, Z.; Xie, J.; Cai, L.; Ping, A. Comparison of percutaneous endoscopic lumbar discectomy versus open lumbar microdiscectomy for lumbar disc herniation: A meta-analysis. Int. J. Surg. 2016, 31, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Wang, F.; Hong, X.; Wang, Y.T.; Bao, J.P.; Liu, L.; Wang, X.H.; Xie, Z.Y.; Wu, X.T. Comparison of percutaneous endoscopic lumbar discectomy versus microendoscopic discectomy for the treatment of lumbar disc herniation: A meta-analysis. Int. Orthop. 2019, 43, 923–937. [Google Scholar] [CrossRef] [PubMed]
- Qin, R.; Liu, B.; Hao, J.; Zhou, P.; Yao, Y.; Zhang, F.; Chen, X. Percutaneous Endoscopic Lumbar Discectomy Versus Posterior Open Lumbar Microdiscectomy for the Treatment of Symptomatic Lumbar Disc Herniation: A Systemic Review and Meta-Analysis. World Neurosurg. 2018, 120, 352–362. [Google Scholar] [CrossRef]
- Liu, X.; Yuan, S.; Tian, Y.; Wang, L.; Gong, L.; Zheng, Y.; Li, J. Comparison of percutaneous endoscopic transforaminal discectomy, microendoscopic discectomy, and microdiscectomy for symptomatic lumbar disc herniation: Minimum 2-year follow-up results. J. Neurosurg. Spine 2018, 28, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Oezdemir, S.; Komp, M.; Hahn, P.; Ruetten, S. Decompression for cervical disc herniation using the full-endoscopic anterior technique. Oper. Orthop. Traumatol. 2019, 31 (Suppl. S1), 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ruetten, S.; Komp, M.; Merk, H.; Godolias, G. A new full-endoscopic technique for cervical posterior foraminotomy in the treatment of lateral disc herniations using 6.9-mm endoscopes: Prospective 2-year results of 87 patients. Minim. Invasive Neurosurg. 2007, 50, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.T.; Carleton-Bland, N.P.; Lee, M.K.; Jackson, R.; Clark, S.R.; Wilby, M.J. Comparison of clinical outcomes in anterior cervical discectomy versus foraminotomy for brachialgia. Br. J. Neurosurg. 2019, 33, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Keum, H.J.; Shin, S.H. Percutaneous Endoscopic Cervical Discectomy Versus Anterior Cervical Discectomy and Fusion: A Comparative Cohort Study with a Five-Year Follow-Up. J. Clin. Med. 2020, 9, 371. [Google Scholar] [CrossRef]
- MacDowall, A.; Heary, R.F.; Holy, M.; Lindhagen, L.; Olerud, C. Posterior foraminotomy versus anterior decompression and fusion in patients with cervical degenerative disc disease with radiculopathy: Up to 5 years of outcome from the national Swedish Spine Register. J. Neurosurg. Spine 2019, 32, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Cheung, J.P.Y.; Luk, K.D.K. Complications of Anterior and Posterior Cervical Spine Surgery. Asian Spine J. 2016, 10, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Sahai, N.; Changoor, S.; Dunn, C.J.; Sinha, K.; Hwang, K.S.; Faloon, M.; Emami, A. Minimally Invasive Posterior Cervical Foraminotomy as an Alternative to Anterior Cervical Discectomy and Fusion for Unilateral Cervical Radiculopathy: A Systematic Review and Meta-analysis. Spine 2019, 44, 1731–1739. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, S.; Brooks, N.P. Posterior Endoscopic Cervical Foraminotomy. Neurosurg. Clin. N. Am. 2020, 31, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Yu, K.X.; Chu, L.; Chen, L.; Shi, L.; Deng, Z.L. A Novel Posterior Trench Approach Involving Percutaneous Endoscopic Cervical Discectomy for Central Cervical Intervertebral Disc Herniation. Clin. Spine Surg. 2019, 32, 10–17. [Google Scholar] [CrossRef]
- Skovrlj, B.; Gologorsky, Y.; Haque, R.; Fessler, R.G.; Qureshi, S.A. Complications, outcomes, and need for fusion after minimally invasive posterior cervical foraminotomy and microdiscectomy. Spine J. 2014, 14, 2405–2411. [Google Scholar] [CrossRef] [PubMed]
- Jagannathan, J.; Sherman, J.H.; Szabo, T.; Shaffrey, C.I.; Jane, J.A. The posterior cervical foraminotomy in the treatment of cervical disc/osteophyte disease: A single-surgeon experience with a minimum of 5 years’ clinical and radiographic follow-up. J. Neurosurg. Spine 2009, 10, 347–356. [Google Scholar] [CrossRef]
- Won, S.J.; Kim, C.H.; Chung, C.K.; Choi, Y.; Park, S.B.; Moon, J.H.; Heo, W.; Kim, S.M. Clinical Outcomes of Single-level Posterior Percutaneous Endoscopic Cervical Foraminotomy for Patients with Less Cervical Lordosis. J. Minim. Invasive Spine Surg. Tech. 2016, 1, 11–17. [Google Scholar] [CrossRef]
- Yuchi, C.X.; Sun, G.; Chen, C.; Liu, G.; Zhao, D.; Yang, H.; Xu, B.; Deng, S.; Ma, X.; Du, C.F.; et al. Comparison of the Biomechanical Changes After Percutaneous Full-Endoscopic Anterior Cervical Discectomy versus Posterior Cervical Foraminotomy at C5-C6: A Finite Element-Based Study. World Neurosurg. 2019, 128, e905–e911. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.; Chu, B.; Kuo, C.C.; Leasure, J.M.; Ames, C.; Kondrashov, D. Changes in foraminal area with anterior decompression versus keyhole foraminotomy in the cervical spine: A biomechanical investigation. J. Neurosurg. Spine 2017, 27, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Choi, M.; Ryu, D.S.; Choi, I.; Kim, C.H.; Kim, H.S.; Sohn, M.J. Efficacy and Safety of Full-endoscopic Decompression via Interlaminar Approach for Central or Lateral Recess Spinal Stenosis of the Lumbar Spine: A Meta-analysis. Spine 2018, 43, 1756–1764. [Google Scholar] [CrossRef] [PubMed]
- Xie, P.; Feng, F.; Chen, Z.; He, L.; Yang, B.; Chen, R.; Wu, W.; Liu, B.; Dong, J.; Shu, T.; et al. Percutaneous transforaminal full endoscopic decompression for the treatment of lumbar spinal stenosis. BMC Musculoskelet. Disord. 2020, 21, 546. [Google Scholar] [CrossRef] [PubMed]
- Bergamaschi, J.P.M.; Teixeira, K.O.; Soares, T.Q.; Araújo, F.F.; Depieri, G.V.; Lugão, A.F.; Assis, R.R.; Graciano, R.S.; Sandon, L.H.D.; Bergamaschi, E.C.Q.; et al. Extraforaminal Full-Endoscopic Approach for the Treatment of Lateral Compressive Diseases of the Lumbar Spine. J. Pers. Med. 2023, 13, 453. [Google Scholar] [CrossRef] [PubMed]
- Spetzger, U.; Bertalanffy, H.; Naujokat, C.; von Keyserlingk, D.G.; Gilsbach, J.M. Unilateral laminotomy for bilateral decompression of lumbar spinal stenosis. Part I: Anatomical and surgical considerations. Acta Neurochir. 1997, 139, 392–396. [Google Scholar] [CrossRef]
- Spetzger, U.; Bertalanffy, H.; Reinges, M.H.; Gilsbach, J.M. Unilateral laminotomy for bilateral decompression of lumbar spinal stenosis. Part II: Clinical experiences. Acta Neurochir. 1997, 139, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Bresnahan, L.; Ogden, A.T.; Natarajan, R.N.; Fessler, R.G. A biomechanical evaluation of graded posterior element removal for treatment of lumbar stenosis: Comparison of a minimally invasive approach with two standard laminectomy techniques. Spine 2009, 34, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ruetten, S.; Hahn, P.; Oezdemir, S.; Baraliakos, X.; Merk, H.; Godolias, G.; Komp, M. Full-endoscopic uniportal decompression in disc herniations and stenosis of the thoracic spine using the interlaminar, extraforaminal, or transthoracic retropleural approach. J. Neurosurg. Spine 2018, 29, 157–168. [Google Scholar] [CrossRef]
- Bae, J.; Lee, S.H.; Wagner, R.; Shen, J.; Telfeian, A.E. Full Endoscopic Surgery for Thoracic Pathology: Next Step after Mastering Lumbar and Cervical Endoscopic Spine Surgery? Biomed. Res. Int. 2022, 2022, 11–13. [Google Scholar] [CrossRef]
- Gibson, R.D.S.; Wagner, R.; Gibson, J.N.A. Full endoscopic surgery for thoracic pathology: An assessment of supportive evidence. EFORT Open Rev. 2021, 6, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Hussain, I.; Schmidt, F.A.; Kirnaz, S.; Wipplinger, C.; Schwartz, T.H.; Härtl, R. MIS approaches in the cervical spine. J Spine Surg. 2019, 5 (Suppl. S1), S74–S83. [Google Scholar] [CrossRef]
- Alimi, M.; Hofstetter, C.P.; Pyo, S.Y.; Paulo, D.; Härtl, R. Minimally invasive laminectomy for lumbar spinal stenosis in patients with and without preoperative spondylolisthesis: Clinical outcome and reoperation rates. J. Neurosurg. Spine 2015, 22, 339–352. [Google Scholar] [CrossRef] [PubMed]
- Thomé, C.; Zevgaridis, D.; Leheta, O.; Bäzner, H.; Pöckler-Schöniger, C.; Wöhrle, J.; Schmiedek, P. Outcome after less-invasive decompression of lumbar spinal stenosis: A randomized comparison of unilateral laminotomy, bilateral laminotomy, and laminectomy. J. Neurosurg. Spine 2005, 3, 129–141. [Google Scholar] [CrossRef]
- Zhang, Y.; Lv, N.; He, F.; Pi, B.; Liu, H.; Chen, A.C.; Yang, H.; Liu, M.; Zhu, X. Comparison of cervical disc arthroplasty and anterior cervical discectomy and fusion for the treatment of cervical disc degenerative diseases on the basis of more than 60 months of follow-up: A systematic review and meta-analysis. BMC Neurol. 2020, 20, 143. [Google Scholar] [CrossRef]
- Geck, M.J.; Eismont, F.J. Surgical options for the treatment of cervical spondylotic myelopathy. Orthop. Clin. N. Am. 2002, 33, 329–348. [Google Scholar] [CrossRef] [PubMed]
- Bakhsheshian, J.; Mehta, V.A.; Liu, J.C. Current Diagnosis and Management of Cervical Spondylotic Myelopathy. Glob. Spine J. 2017, 7, 572–586. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, J.H.; DeCastro, I.; McDonnell, D.E. Minimally invasive spine technology and minimally invasive spine surgery: A historical review. Neurosurg. Focus. 2009, 27, E9. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.B.; Ma, Y.J.; Ma, H.J.; Zhang, X.Y.; Zhou, H.G. Clinical Efficacy of Posterior Percutaneous Endoscopic Unilateral Laminotomy with Bilateral Decompression for Symptomatic Cervical Spondylotic Myelopathy. Orthop. Surg. 2022, 14, 876–884. [Google Scholar] [CrossRef]
- Chang, C.J.; Liu, Y.F.; Hsiao, Y.M.; Chang, W.L.; Hsu, C.C.; Liu, K.C.; Huang, Y.H.; Yeh, M.L.; Lin, C.L. Full endoscopic spine surgery for cervical spondylotic myelopathy: A systematic review. World Neurosurg. 2023, 175, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Rao, R.D.; Gourab, K.; David, K.S. Operative treatment of cervical spondylotic myelopathy. J. Bone Joint Surg. Am. 2006, 88, 1619–1640. [Google Scholar] [CrossRef] [PubMed]
- Ban, D.; Liu, Y.; Cao, T.; Feng, S. Safety of outpatient anterior cervical discectomy and fusion: A systematic review and meta-analysis. Eur. J. Med. Res. 2016, 21, 34. [Google Scholar] [CrossRef] [PubMed]
- Cook, C.; Roman, M.; Stewart, K.M.; Leithe, L.G.; Isaacs, R. Reliability and diagnostic accuracy of clinical special tests for myelopathy in patients seen for cervical dysfunction. J. Orthop. Sports Phys. Ther. 2009, 39, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Young, W.F. Cervical spondylotic myelopathy: A common cause of spinal cord dysfunction in older persons. Am. Fam. Physician 2000, 62, 1064–1070. [Google Scholar] [PubMed]
- Asher, A.L.; Devin, C.J.; Kerezoudis, P.; Chotai, S.; Nian, H.; Harrell, F.E.J.; Sivaganesan, A.; McGirt, M.; Archer, K.R.; Foley, K.T.; et al. Comparison of Outcomes Following Anterior vs. Posterior Fusion Surgery for Patients with Degenerative Cervical Myelopathy: An Analysis from Quality Outcomes Database. Neurosurgery 2019, 84, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, H.; Maeno, K.; Uno, K.; Kakutani, K.; Nishida, K.; Sumi, M. Outcomes of surgical intervention for cervical spondylotic myelopathy accompanying local kyphosis (comparison between laminoplasty alone and posterior reconstruction surgery using the screw-rod system). Eur. Spine J. 2014, 23, 341–346. [Google Scholar] [CrossRef]
- Choi, G.; Pophale, C.S.; Patel, B.; Uniyal, P. Endoscopic Spine Surgery. J. Korean Neurosurg. Soc. 2017, 60, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Ju, C., II; Lee, S.M. Complications and Management of Endoscopic Spinal Surgery. Neurospine 2023, 20, 56–77. [Google Scholar] [CrossRef]
- Sclafani, J.A.; Kim, C.W. Complications Associated With the Initial Learning Curve of Minimally Invasive Spine Surgery: A Systematic Review. Clin. Orthop. Relat. Res. 2014, 472, 1711–1717. [Google Scholar] [CrossRef]
- Lv, J.; Mei, J.; Feng, X.; Tian, X.; Sun, L. Clinical efficacy and safety of posterior minimally invasive surgery in cervical spondylosis: A systematic review. J. Orthop. Surg. Res. 2022, 17, 389. [Google Scholar] [CrossRef]
- Lee, C.W.; Yoon, K.J.; Kim, S.W. Percutaneous Endoscopic Decompression in Lumbar Canal and Lateral Recess Stenosis—The Surgical Learning Curve. Neurospine 2019, 16, 63–71. [Google Scholar] [CrossRef]
- Tong, Y.; Huang, Z.; Hu, C.; Fan, Z.; Bian, F.; Yang, F.; Zhao, C. A comparison study of posterior cervical percutaneous endoscopic ventral bony decompression and simple dorsal decompression treatment in cervical spondylotic radiculopathy caused by cervical foraminal and/or lateral spinal stenosis: A clinical retrospect. BMC Musculoskelet. Disord. 2020, 21, 290. [Google Scholar] [CrossRef]
- Liu, L.; Li, Q.; Ao, J.; Du, Q.; Xin, Z.J.; Liao, W.B. Posterior Percutaneous Endoscopic Technique Through Bilateral Translaminar Osseous Channels for Thoracic Spinal Stenosis Caused by Ossification of the Ligamentum Flavum Combined with Disk Herniation at the T10–11 Level: A Technical Note. World Neurosurg. 2020, 133, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Siepe, C.J.; Sauer, D.; Mayer, H.M. Full endoscopic, bilateral over-the-top decompression for lumbar spinal stenosis. Eur. Spine J. 2018, 27 (Suppl. S4), 563–565. [Google Scholar] [CrossRef]
- Komp, M.; Hahn, P.; Oezdemir, S.; Giannakopoulos, A.; Heikenfeld, R.; Kasch, R.; Merk, H.; Godolias, G.; Ruetten, S. Bilateral spinal decompression of lumbar central stenosis with the full-endoscopic interlaminar versus microsurgical laminotomy technique: A prospective, randomized, controlled study. Pain. Physician 2015, 18, 61–70. [Google Scholar] [CrossRef] [PubMed]
- An, B.; Li, X.C.; Zhou, C.P.; Wang, B.S.; Gao, H.R.; Ma, H.J.; He, Y.; Zhou, H.G.; Yang, H.J.; Qian, J.X. Percutaneous full endoscopic posterior decompression of thoracic myelopathy caused by ossification of the ligamentum flavum. Eur. Spine J. 2019, 28, 492–501. [Google Scholar] [CrossRef]
- Boukebir, M.A.; Berlin, C.D.; Ramirez, R.N.; Heiland, T.; Schöller, K.; Rawanduzy, C.; Kirnaz, S.; Jada, A.; Härtl, R. Ten-Step Minimally Invasive Spine Lumbar Decompression and Dural Repair through Tubular Retractors. Oper. Neurosurg. 2017, 13, 232–245. [Google Scholar] [CrossRef] [PubMed]
- Siepe, C.J.; Bridts, A.L.; Ayman, M.; Sauer, D.; Mehren, C. Full-endoscopic bilateral over-the-top decompression in lumbar central stenosis: Surgical technique and outcomes. Eur. Spine J. 2023, 32, 2918–2923. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Radiographic Parameters
|
Clinical Parameters
|
Anatomical Parameters
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bergamaschi, J.P.M.; Brito, M.B.S.d.; Araújo, F.F.d.; Graciano, R.S.; Utino, E.T.; Lewandrowski, K.-U.; Wirth, F. Surgical Technique of Central and Over-the-Top Full-Endoscopic Decompression of the Cervical Spine: A Technical Note. J. Pers. Med. 2023, 13, 1508. https://doi.org/10.3390/jpm13101508
Bergamaschi JPM, Brito MBSd, Araújo FFd, Graciano RS, Utino ET, Lewandrowski K-U, Wirth F. Surgical Technique of Central and Over-the-Top Full-Endoscopic Decompression of the Cervical Spine: A Technical Note. Journal of Personalized Medicine. 2023; 13(10):1508. https://doi.org/10.3390/jpm13101508
Chicago/Turabian StyleBergamaschi, João Paulo Machado, Marcelo Botelho Soares de Brito, Fernando Flores de Araújo, Ricardo Squiapati Graciano, Edgar Takao Utino, Kai-Uwe Lewandrowski, and Fernanda Wirth. 2023. "Surgical Technique of Central and Over-the-Top Full-Endoscopic Decompression of the Cervical Spine: A Technical Note" Journal of Personalized Medicine 13, no. 10: 1508. https://doi.org/10.3390/jpm13101508