
Prognostic Nomogram Combining Preoperative Neutrophil to Lymphocyte Ratio and Clinicopathologic Features for Gastric Cancer Patients after Distal Radical Gastrectomy: Based on Propensity Score Matching
 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Population
2.2. Data Collection
2.3. Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Basic Clinical Characteristics
3.2. Biomarker Selection
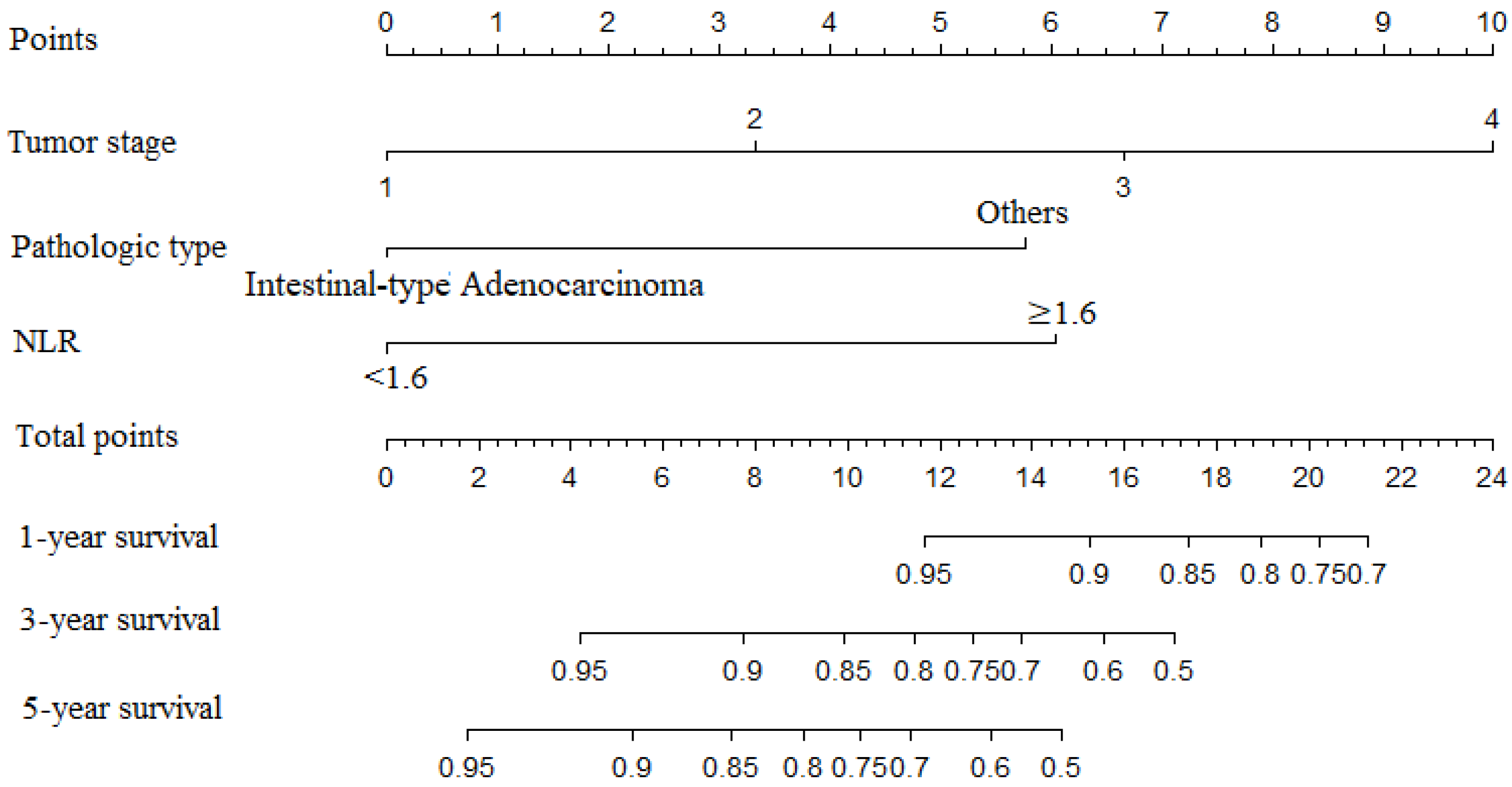
3.3. Development of the Prediction Model
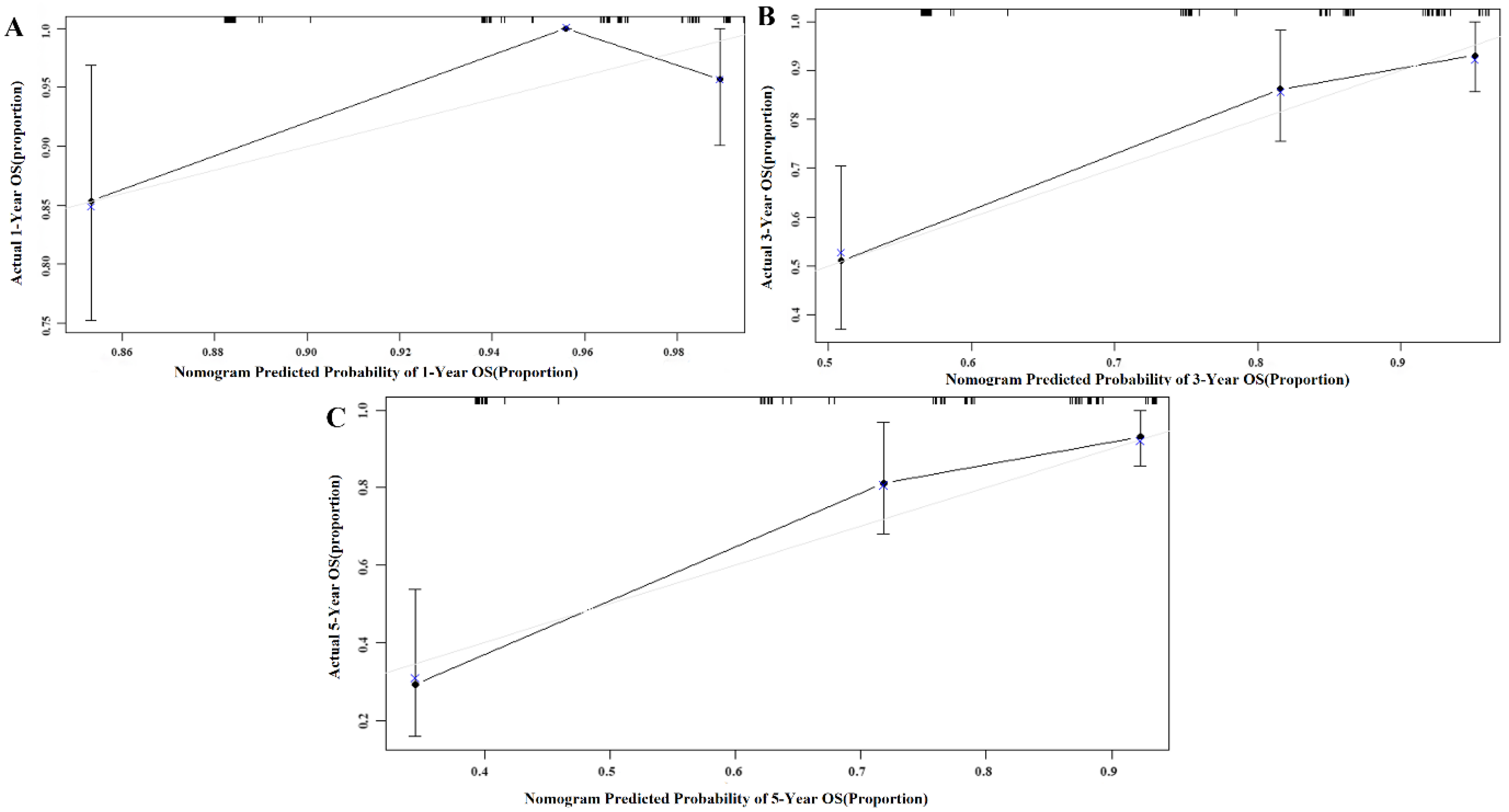
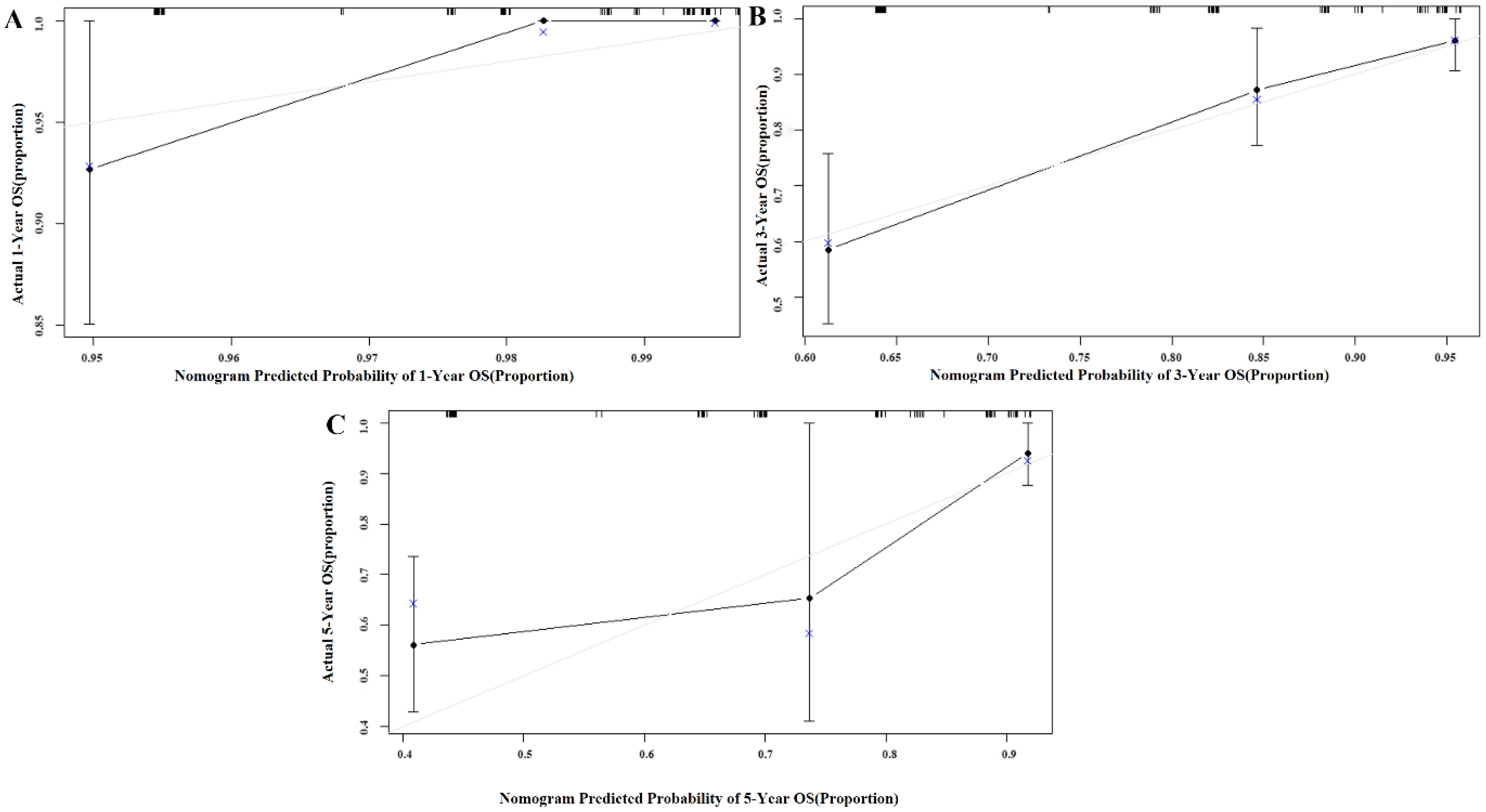
3.4. Internal and External Validation of the Nomogram Model
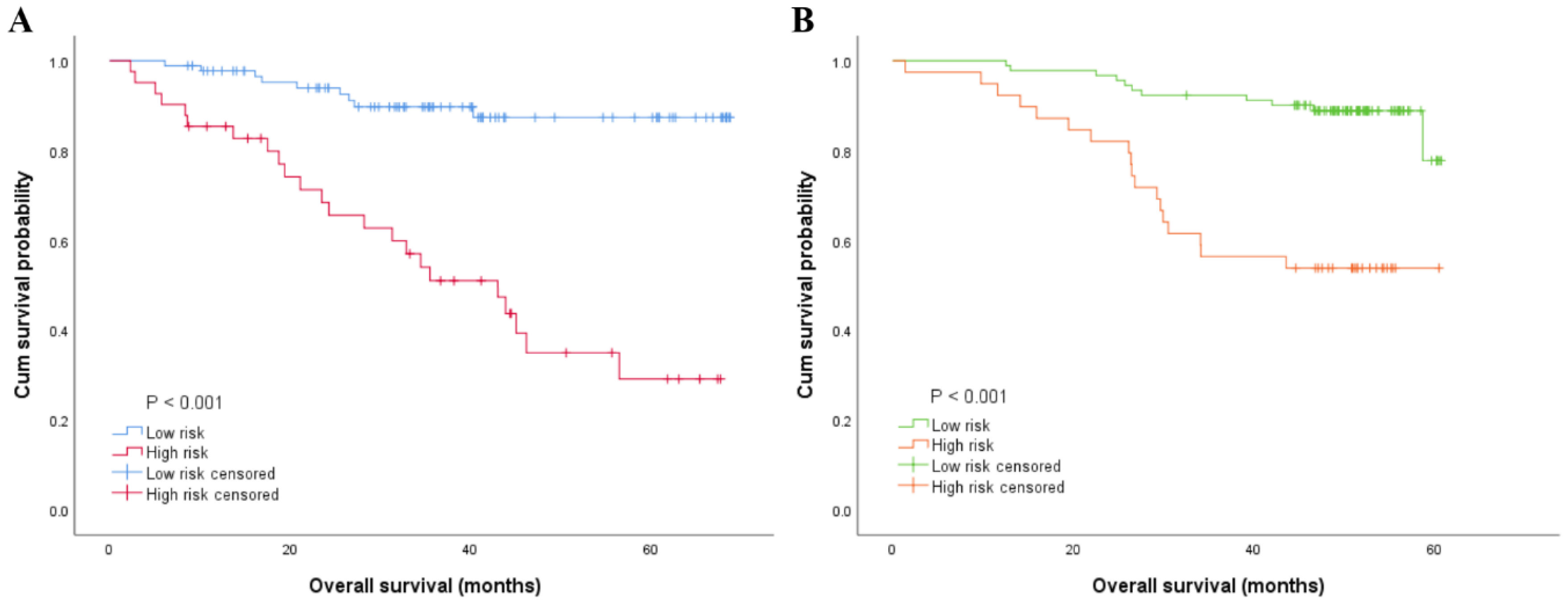
3.5. Risk Stratification of OS by the Nomogram Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hanahan, D.; Weinberg, R.A. Hallmarks of Cancer: The Next Generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, D.D.; Fuentes, E.; Quraishi, S.A.; Cropano, C.; Kaafarani, H.; Lee, J.; King, D.R.; DeMoya, M.; Fagenholz, P.; Butler, K.; et al. Adequate Nutrition May Get You Home: Effect of Caloric/Protein Deficits on the Discharge Destination of Critically Ill Surgical Patients. JPEN J. Parenter Enter. Nutr. 2016, 40, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Neeman, E.; Sharon, E.; Ben-Eliyahu, S. Exploiting the Critical Perioperative Period to Improve Long-Term Cancer Outcomes. Nat. Rev. Clin. Oncol. 2015, 12, 213–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gustafsson, U.O.; Oppelstrup, H.; Thorell, A.; Nygren, J.; Ljungqvist, O. Adherence to the Eras Protocol Is Associated with 5-Year Survival after Colorectal Cancer Surgery: A Retrospective Cohort Study. World J. Surg. 2016, 40, 1741–1747. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.; Deng, J.Y.; Liu, Y.; Ke, B.; Liu, H.G.; Liang, H. The Role of Preoperative Neutrophil-Lymphocyte and Platelet-Lymphocyte Ratio in Patients after Radical Resection for Gastric Cancer. Biomarkers 2014, 19, 444–451. [Google Scholar] [CrossRef]
- Nozoe, T.; Ninomiya, M.; Maeda, T.; Matsukuma, A.; Nakashima, H.; Ezaki, T. Prognostic Nutritional Index: A Tool to Predict the Biological Aggressiveness of Gastric Carcinoma. Surg. Today 2010, 40, 440–443. [Google Scholar] [CrossRef]
- Chan, J.C.; Chan, D.L.; Diakos, C.I.; Engel, A.; Pavlakis, N.; Gill, A.; Clarke, S.J. The Lymphocyte-to-Monocyte Ratio Is a Superior Predictor of Overall Survival in Comparison to Established Biomarkers of Resectable Colorectal Cancer. Ann. Surg. 2017, 265, 539–546. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Zhou, Y.; Xu, Y.; Zhu, H.Y.; Shi, Y.Q. Low Pretreatment Serum Globulin May Predict Favorable Prognosis for Gastric Cancer Patients. Tumour Biol. 2016, 37, 3905–3911. [Google Scholar] [CrossRef]
- Ishizuka, M.; Nagata, H.; Takagi, K.; Iwasaki, Y.; Shibuya, N.; Kubota, K. Clinical Significance of the C-Reactive Protein to Albumin Ratio for Survival after Surgery for Colorectal Cancer. Ann. Surg. Oncol. 2016, 23, 900–907. [Google Scholar] [CrossRef]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic Criteria for Malnutrition—An Espen Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. A Comparison of Inflammation-Based Prognostic Scores in Patients with Cancer. A Glasgow Inflammation Outcome Study. Eur. J. Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef]
- Cheema, F.N.; Abraham, N.S.; Berger, D.H.; Albo, D.; Taffet, G.E.; Naik, A.D. Novel Approaches to Perioperative Assessment and Intervention May Improve Long-Term Outcomes after Colorectal Cancer Resection in Older Adults. Ann. Surg. 2011, 253, 867–874. [Google Scholar] [CrossRef]
- Eo, W.K.; Chang, H.J.; Suh, J.; Ahn, J.; Shin, J.; Hur, J.Y.; Kim, G.Y.; Lee, S.; Park, S.; Lee, S. The Prognostic Nutritional Index Predicts Survival and Identifies Aggressiveness of Gastric Cancer. Nutr. Cancer 2015, 67, 1260–1267. [Google Scholar] [CrossRef]
- Sun, K.Y.; Xu, J.B.; Chen, S.L.; Yuan, Y.J.; Wu, H.; Peng, J.J.; Chen, C.Q.; Guo, P.; Hao, Y.T.; He, Y.L. Novel Immunological and Nutritional-Based Prognostic Index for Gastric Cancer. World J. Gastroenterol. 2015, 21, 5961–5971. [Google Scholar] [CrossRef]
- Chen, X.-L.; Xue, L.; Wang, W.; Chen, H.-N.; Zhang, W.-H.; Liu, K.; Chen, X.-Z.; Yang, K.; Zhang, B.; Chen, Z.-X.; et al. Prognostic Significance of the Combination of Preoperative Hemoglobin, Albumin, Lymphocyte and Platelet in Patients with Gastric Carcinoma a Retrospective Cohort Study. Oncotarget 2015, 6, 41370–41382. [Google Scholar] [CrossRef]
- Liu, X.; Meltzer, S. Gastric Cancer in the Era of Precision Medicine. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 348–358. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.P.; Xie, F.; Liu, L.; Sun, Y.; Li, L.; Tang, L.; Liao, X.; Xu, H.; Chen, L.; Lai, S.; et al. Re-Evaluation of 6th Edition of Ajcc Staging System for Nasopharyngeal Carcinoma and Proposed Improvement Based on Magnetic Resonance Imaging. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1326–1334. [Google Scholar] [CrossRef]
- Cetinkunar, S.; Guzel, H.; Gokce, I.E.; Erdem, H.; Gulkan, S.; Aktimur, R.; Kucuk, B.; Imamoglu, I.; Kargici, H. High Levels of Platelet/Lymphocyte Ratio Are Associated with Metastatic Gastric Cancer. JBOUN 2015, 20, 78–83. [Google Scholar]
- Lee, S.; Oh, S.Y.; Kim, S.H.; Lee, J.H.; Kim, M.C.; Kim, K.H.; Kim, H.-J. Prognostic Significance of Neutrophil Lymphocyte Ratio and Platelet Lymphocyte Ratio in Advanced Gastric Cancer Patients Treated with Folfox Chemotherapy. BMC Cancer 2013, 13, 350. [Google Scholar] [CrossRef] [Green Version]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Ohtani, H.; Iseki, Y.; Ikeya, T.; Sugano, K.; Hirakawa, K. The Pretreatment Albumin to Globulin Ratio Predicts Chemotherapeutic Outcomes in Patients with Unresectable Metastatic Colorectal Cancer. BMC Cancer 2015, 15, 347. [Google Scholar] [CrossRef] [Green Version]
- Park, S.; Park, S.; Lee, S.H.; Suh, B.; Ock, C.Y.; Keam, B.; Kim, T.M.; Kim, D.W.; Kim, Y.W.; Heo, D.S. Pretreatment Albumin-to-Globulin Ratio as a Predictive Marker for Tyrosine Kinase Inhibitor in Non-Small Cell Lung Cancer. Cancer Biomark 2016, 16, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shao, Y.; Yao, H.; Zhuang, Q.; Wang, K.; Xing, Z.; Xu, X.; He, X.; Xu, R. Preoperative Albumin to Globulin Ratio Predicts Survival in Clear Cell Renal Cell Carcinoma Patients. Oncotarget 2017, 8, 48291–48302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.Z.; Li, F.; Xu, Z.K.; Chen, X.; Sun, B.; Cao, J.W.; Liu, Y.G. Preoperative Albumin-to-Globulin Ratio and Prognostic Nutrition Index Predict Prognosis for Glioblastoma. Oncol. Targets Ther. 2017, 10, 725–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohri, Y.; Inoue, Y.; Tanaka, K.; Hiro, J.; Uchida, K.; Kusunoki, M. Prognostic Nutritional Index Predicts Postoperative Outcome in Colorectal Cancer. World J. Surg. 2013, 37, 2688–2692. [Google Scholar] [CrossRef] [PubMed]
- Crumley, A.B.; Stuart, R.C.; McKernan, M.; McMillan, D.C. Is Hypoalbuminemia an Independent Prognostic Factor in Patients with Gastric Cancer? World J. Surg. 2010, 34, 2393–2398. [Google Scholar] [CrossRef]
- Azab, B.; Kedia, S.; Shah, N.; Vonfrolio, S.; Lu, W.; Naboush, A.; Mohammed, F.; Bloom, S.W. The Value of the Pretreatment Albumin/Globulin Ratio in Predicting the Long-Term Survival in Colorectal Cancer. Int. J. Colorectal. Dis. 2013, 28, 1629–1636. [Google Scholar] [CrossRef]
- Jalali, A.; Alvarez-Iglesias, A.; Roshan, D.; Newell, J. Visualising Statistical Models Using Dynamic Nomograms. PLoS ONE 2019, 14, e0225253. [Google Scholar] [CrossRef]
- Talebi, A.; Borumandnia, N.; Doosti, H.; Abbasi, S.; Pourhoseingholi, M.A.; Agah, S.; Tabaeian, S.P. Development of Web-Based Dynamic Nomogram to Predict Survival in Patients with Gastric Cancer: A Population-Based Study. Sci. Rep. 2022, 12, 4580. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, D. Nomogram for Predicting Survival in Advanced Gastric Cancer after Neoadjuvant Chemotherapy and Radical Surgery. Gastroenterol. Res. Pract. 2021, 2021, 2923700. [Google Scholar] [CrossRef]
- Eom, B.W.; Ryu, K.W.; Nam, B.H.; Park, Y.; Lee, H.J.; Kim, M.C.; Cho, G.S.; Kim, C.Y.; Ryu, S.W.; Shin, D.W.; et al. Survival Nomogram for Curatively Resected Korean Gastric Cancer Patients: Multicenter Retrospective Analysis with External Validation. PLoS ONE 2015, 10, e0119671. [Google Scholar] [CrossRef]
- Huang, Y.Q.; Liang, C.; He, L.; Tian, J.; Liang, C.; Chen, X.; Ma, Z.; Liu, Z. Development and Validation of a Radiomics Nomogram for Preoperative Prediction of Lymph Node Metastasis in Colorectal Cancer. J. Clin. Oncol. 2016, 34, 2157–2164. [Google Scholar] [CrossRef]
- Narita, Y.; Kadowaki, S.; Oze, I.; Kito, Y.; Kawakami, T.; Machida, N.; Taniguchi, H.; Ura, T.; Ando, M.; Ito, S.; et al. Establishment and Validation of Prognostic Nomograms in First-Line Metastatic Gastric Cancer Patients. J. Gastrointest Oncol. 2018, 9, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Pinato, D.J.; North, B.; Sharma, R. A Novel, Externally Validated Inflammation-Based Prognostic Algorithm in Hepatocellular Carcinoma: The Prognostic Nutritional Index (Pni). Br. J. Cancer 2012, 106, 1439–1445. [Google Scholar] [CrossRef] [Green Version]
- Schwegler, I.; von Holzen, A.; Gutzwiller, J.P.; Schlumpf, R.; Mühlebach, S.; Stanga, Z. Nutritional Risk Is a Clinical Predictor of Postoperative Mortality and Morbidity in Surgery for Colorectal Cancer. Br. J. Surg. 2010, 97, 92–97. [Google Scholar] [CrossRef]
- Migita, K.; Takayama, T.; Saeki, K.; Matsumoto, S.; Wakatsuki, K.; Enomoto, K.; Tanaka, T.; Ito, M.; Kurumatani, N.; Nakajima, Y. The Prognostic Nutritional Index Predicts Long-Term Outcomes of Gastric Cancer Patients Independent of Tumor Stage. Ann. Surg. Oncol. 2013, 20, 2647–2654. [Google Scholar] [CrossRef]
- Kao, S.C.; Pavlakis, N.; Harvie, R.; Vardy, J.L.; Boyer, M.J.; van Zandwijk, N.; Clarke, S.J. High Blood Neutrophil-to-Lymphocyte Ratio Is an Indicator of Poor Prognosis in Malignant Mesothelioma Patients Undergoing Systemic Therapy. Clin. Cancer Res. 2010, 16, 5805–5813. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Huang, D. The Value of the Systematic Inflammation-Based Glasgow Prognostic Score in Patients with Gastric Cancer: A Literature Review. J. Cancer Res. Ther. 2014, 10, 799–804. [Google Scholar] [CrossRef]
- Pan, Q.X.; Su, Z.J.; Zhang, J.H.; Wang, C.R.; Ke, S.Y. A Comparison of the Prognostic Value of Preoperative Inflammation-Based Scores and Tnm Stage in Patients with Gastric Cancer. Oncol. Targets Ther. 2015, 8, 1375–1385. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and Cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Xu, J.; Zhong, Y.; Jing, D.; Wu, Z. Preoperative Enteral Immunonutrition Improves Postoperative Outcome in Patients with Gastrointestinal Cancer. World J. Surg. 2006, 30, 1284–1289. [Google Scholar] [CrossRef]
- Soeters, P.B.; Reijven, P.L.; van Bokhorst-de van der Schueren, M.A.; Schols, J.M.; Halfens, R.J.; Meijers, J.M.; van Gemert, W.G. A Rational Approach to Nutritional Assessment. Clin. Nutr. 2008, 27, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Arends, J. The Causes and Consequences of Cancer-Associated Malnutrition. Eur. J. Oncol. Nurs. 2005, 9, S51–S63. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, T.; Matsumoto, S.; Teramukai, S.; Ishiwata, R.; Nagai, Y.; Fukushima, M. The Baseline Ratio of Neutrophils to Lymphocytes Is Associated with Patient Prognosis in Advanced Gastric Cancer. Oncology 2007, 73, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Takiguchi, N.; Kainuma, O.; Soda, H.; Ikeda, A.; Cho, A.; Miyazaki, A.; Gunji, H.; Yamamoto, H.; Nagata, M. High Preoperative Neutrophil-Lymphocyte Ratio Predicts Poor Survival in Patients with Gastric Cancer. Gastric Cancer 2010, 13, 170–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, M.R.; Park, Y.K.; Jeong, O.; Seon, J.W.; Ryu, S.Y.; Kim, D.Y.; Kim, Y.J. Elevated Preoperative Neutrophil to Lymphocyte Ratio Predicts Poor Survival Following Resection in Late Stage Gastric Cancer. J. Surg. Oncol. 2011, 104, 504–510. [Google Scholar] [CrossRef]
- Miyamoto, R.; Inagawa, S.; Sano, N.; Tadano, S.; Adachi, S.; Yamamoto, M. The Neutrophil-to-Lymphocyte Ratio (Nlr) Predicts Short-Term and Long-Term Outcomes in Gastric Cancer Patients. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2018, 44, 607–612. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Raw Data | After Propensity-Matching | |||||
|---|---|---|---|---|---|---|
| Characteristics | Primary Cohort | Validation Cohort | p Value | Primary Cohort | Validation Cohort | p Value |
| No. of patients | 389 | 133 | 130 | 130 | ||
| Age (years) | 0.970 | 0.535 | ||||
| ≥60 | 204 | 70 | 66 | 69 | ||
| ˂60 | 185 | 63 | 64 | 61 | ||
| Gender | 0.759 | 0.075 | ||||
| Male | 263 | 88 | 99 | 86 | ||
| Female | 126 | 45 | 31 | 44 | ||
| Tumor size (cm) | 0.503 | 0.615 | ||||
| ≥3 | 238 | 77 | 78 | 74 | ||
| ˂3 | 151 | 56 | 52 | 56 | ||
| Tumor stage | 0.046 | 0.293 | ||||
| T1 | 109 | 38 | 33 | 38 | ||
| T2 | 65 | 25 | 24 | 25 | ||
| T3 | 82 | 14 | 25 | 14 | ||
| T4 | 133 | 56 | 48 | 53 | ||
| Node stage | 0.489 | 0.826 | ||||
| N0 | 190 | 65 | 63 | 63 | ||
| N1 | 58 | 20 | 21 | 20 | ||
| N2 | 61 | 27 | 22 | 27 | ||
| N3 | 80 | 21 | 24 | 20 | ||
| Metastasis stage | 0.445 | 1.000 | ||||
| M0 | 388 | 132 | 130 | 129 | ||
| M1 | 1 | 1 | 0 | 1 | ||
| Clinical stage | 0.436 | 0.588 | ||||
| Ⅰ | 144 | 47 | 48 | 47 | ||
| Ⅱ | 92 | 38 | 30 | 36 | ||
| Ⅲ | 152 | 47 | 52 | 46 | ||
| Ⅳ | 1 | 1 | 0 | 1 | ||
| Borrmann type | 0.034 | 0.457 | ||||
| Ⅰ | 38 | 15 | 10 | 15 | ||
| Ⅱ | 108 | 20 | 28 | 20 | ||
| Ⅲ | 189 | 76 | 71 | 76 | ||
| Ⅳ | 54 | 22 | 21 | 19 | ||
| * Pathological type | 0.470 | 0.586 | ||||
| Intestinal-type adenocarcinoma | 323 | 114 | 114 | 111 | ||
| Others | 66 | 19 | 16 | 19 | ||
| Histological grade | <0.001 | 0.791 | ||||
| Well | 193 | 92 | 87 | 89 | ||
| Moderately-poor | 196 | 41 | 43 | 41 | ||
| OS status | 0.865 | 0.661 | ||||
| Survived | 304 | 103 | 98 | 101 | ||
| Dead | 85 | 30 | 32 | 29 | ||
| NLR | 0.085 | 0.653 | ||||
| Median (P25, P75) | 1.93 (1.43, 2.61) | 1.78 (1.28, 2.58) | 1.80 (1.32, 2.33) | 1.78 (1.27, 2.60) | ||
| PLR | 0.047 | 0.992 | ||||
| Median (P25, P75) | 132.50 (101.00, 178.61) | 121.74 (93.55, 154.75) | 122.47 (91.88, 166.20) | 121.00 (93.29, 156.25) | ||
| PNI | 0.250 | 0.970 | ||||
| Median (P25, P75) | 52.00 (47.00, 55.50) | 53.00 (48.00, 56.50) | 53.00 (47.38, 57.00) | 53.00 (48.00, 56.50) | ||
| AGR | 0.916 | 0.636 | ||||
| Median (P25, P75) | 1.64 (1.43, 1.77) | 1.62 (1.46, 1.76) | 1.64 (1.41, 1.77) | 1.62 (1.46, 1.76) | ||
| Characteristics | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| No. of patients | ||||
| Age (years) | ||||
| ˂60 | 1 | |||
| ≥60 | 1.754 (0.864–3.561) | 0.120 | ||
| Gender | ||||
| Male | 1 | |||
| Female | 0.833 (0.385–1.801) | 0.642 | ||
| Tumor size (cm) | ||||
| ˂3 | 1 | |||
| ≥3 | 1.751 (0.810–3.787) | 0.154 | ||
| Tumor stage | ||||
| T1 | 1 | 1 | ||
| T2 | 0.696 (0.116–4.188) | 0.693 | 0.616 (0.101–3.771) | 0.601 |
| T3 | 1.471 (0.297–7.295) | 0.637 | 1.076 (0.216–5.356) | 0.929 |
| T4 | 5.186 (1.558–17.270) | 0.007 | 4.084 (1.188–14.041) | 0.026 |
| Node stage | ||||
| N0 | 1 | |||
| N1 | 2.295 (0.700–7.523) | 0.170 | ||
| N2 | 6.592 (2.430–17.880) | ˂0.001 | ||
| N3 | 4.783 (1.738–13.163) | 0.002 | ||
| Borrmann type | ||||
| Ⅰ | 1 | |||
| Ⅱ | 0.643 (0.153–2.701) | 0.547 | ||
| Ⅲ | 0.793 (0.232–2.708) | 0.711 | ||
| Ⅳ | 1.193 (0.308–4.619) | 0.798 | ||
| * Pathological type | ||||
| Intestinal-type Adenocarcinoma | 1 | 1 | ||
| Others | 2.872 (1.235–6.680) | 0.014 | 3.398 (1.427–8.089) | 0.006 |
| Histological grade | ||||
| Well | 1 | |||
| Moderately-poor | 1.319 (0.644–2.702) | 0.450 | ||
| NLR | ||||
| ˂1.6 | 1 | 1 | ||
| ≥1.6 | 4.673 (1.794–12.168) | 0.002 | 3.396 (1.283–8.988) | 0.014 |
| PLR | ||||
| ˂92.9 | 1 | |||
| ≥92.9 | 2.505 (0.961–6.528) | 0.060 | ||
| PNI | ||||
| ≥48 | 1 | |||
| ˂48 | 2.307 (1.177–4.641) | 0.019 | ||
| AGR | ||||
| ≥1.4 | 1 | |||
| ˂1.4 | 2.169 (1.060–4.439) | 0.034 |
| Primary Cohort | Validation Cohort | |||
|---|---|---|---|---|
| C-Index | 95% CI | C-Index | 95% CI | |
| Nomogram | 0.753 | 0.642–0.833 | 0.748 | 0.638–0.827 |
| TNM stage | 0.689 | 0.583–0.766 | 0.727 | 0.632–0.788 |
| Groups | OS (Mean ± SD) | 1-Year (%) | 3-Year (%) | 5-Year (%) | |
|---|---|---|---|---|---|
| Primary cohort | Low-Risk | 63.026 ± 1.816 | 97.7 | 89.7 | 87.4 |
| High-Risk | 39.674 ± 3.811 | 85.4 | 51.0 | 29.2 | |
| Validation cohort | Low-Risk | 56.904 ± 1.151 | 98.9 | 92.3 | 77.7 |
| High-Risk | 43.647 ± 3.115 | 92.3 | 56.4 | 53.8 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Wang, C.; Wang, H.; Yang, C.; Cheng, X.; Li, W. Prognostic Nomogram Combining Preoperative Neutrophil to Lymphocyte Ratio and Clinicopathologic Features for Gastric Cancer Patients after Distal Radical Gastrectomy: Based on Propensity Score Matching. J. Pers. Med. 2023, 13, 86. https://doi.org/10.3390/jpm13010086
Liu Y, Wang C, Wang H, Yang C, Cheng X, Li W. Prognostic Nomogram Combining Preoperative Neutrophil to Lymphocyte Ratio and Clinicopathologic Features for Gastric Cancer Patients after Distal Radical Gastrectomy: Based on Propensity Score Matching. Journal of Personalized Medicine. 2023; 13(1):86. https://doi.org/10.3390/jpm13010086
Chicago/Turabian StyleLiu, Yi, Chuandong Wang, Huan Wang, Changshun Yang, Xuefei Cheng, and Weihua Li. 2023. "Prognostic Nomogram Combining Preoperative Neutrophil to Lymphocyte Ratio and Clinicopathologic Features for Gastric Cancer Patients after Distal Radical Gastrectomy: Based on Propensity Score Matching" Journal of Personalized Medicine 13, no. 1: 86. https://doi.org/10.3390/jpm13010086