
Comparison of Pedicled Adductor Longus and Pedicled Sartorius Flap in Inguinal Reconstruction, a Fresh Cadaver Study

Abstract
:1. Introduction
2. Materials and Methods
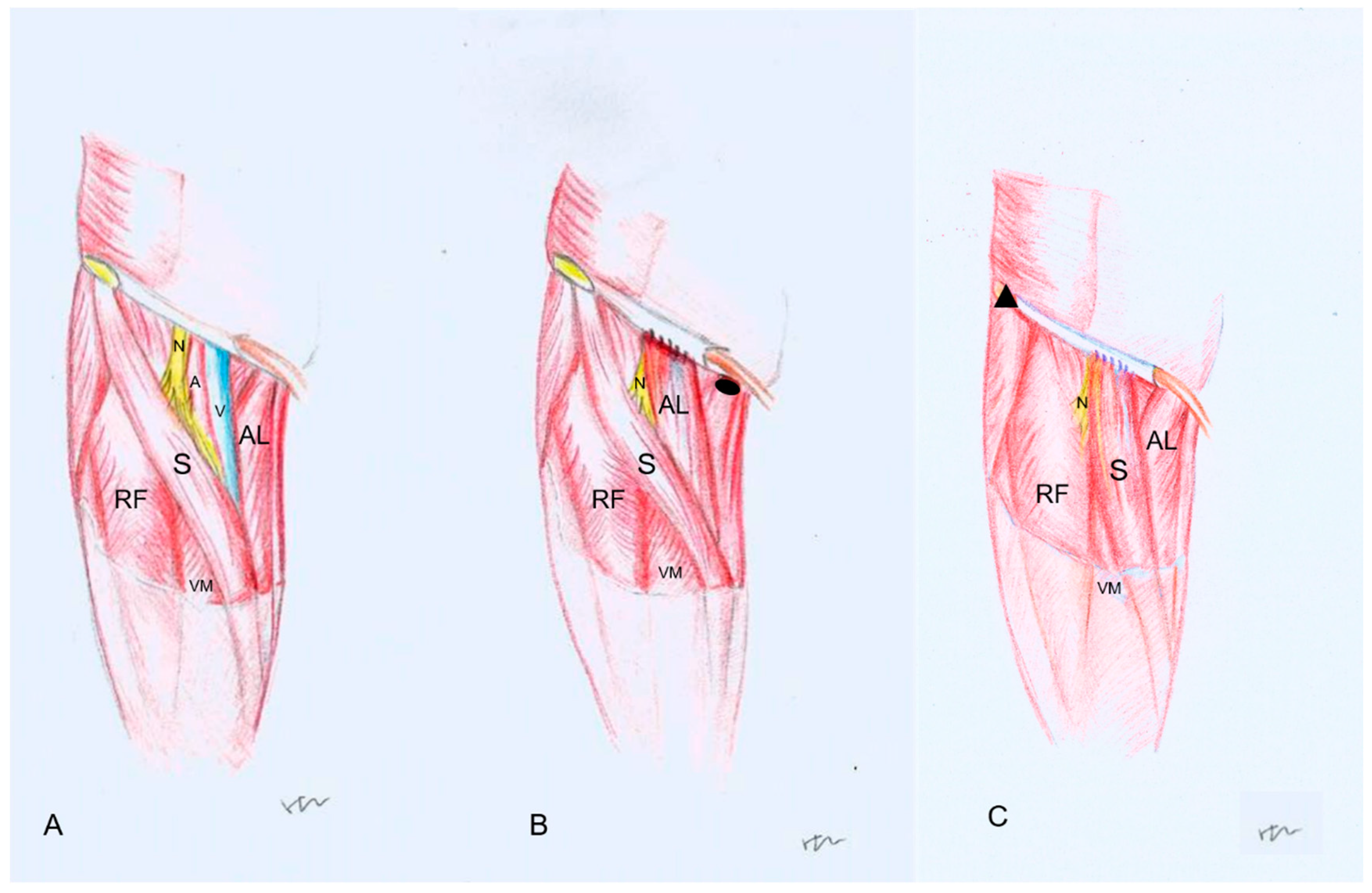
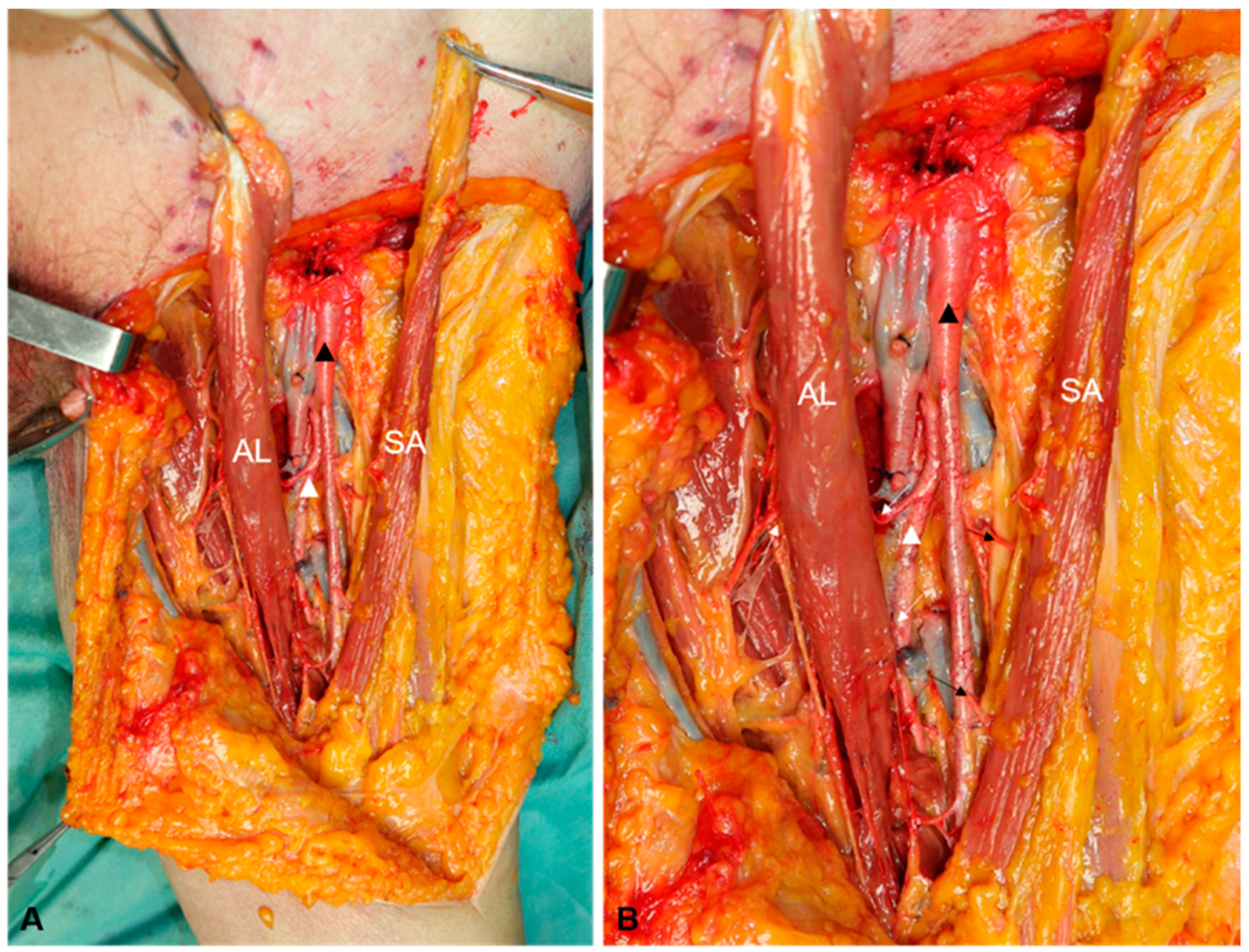
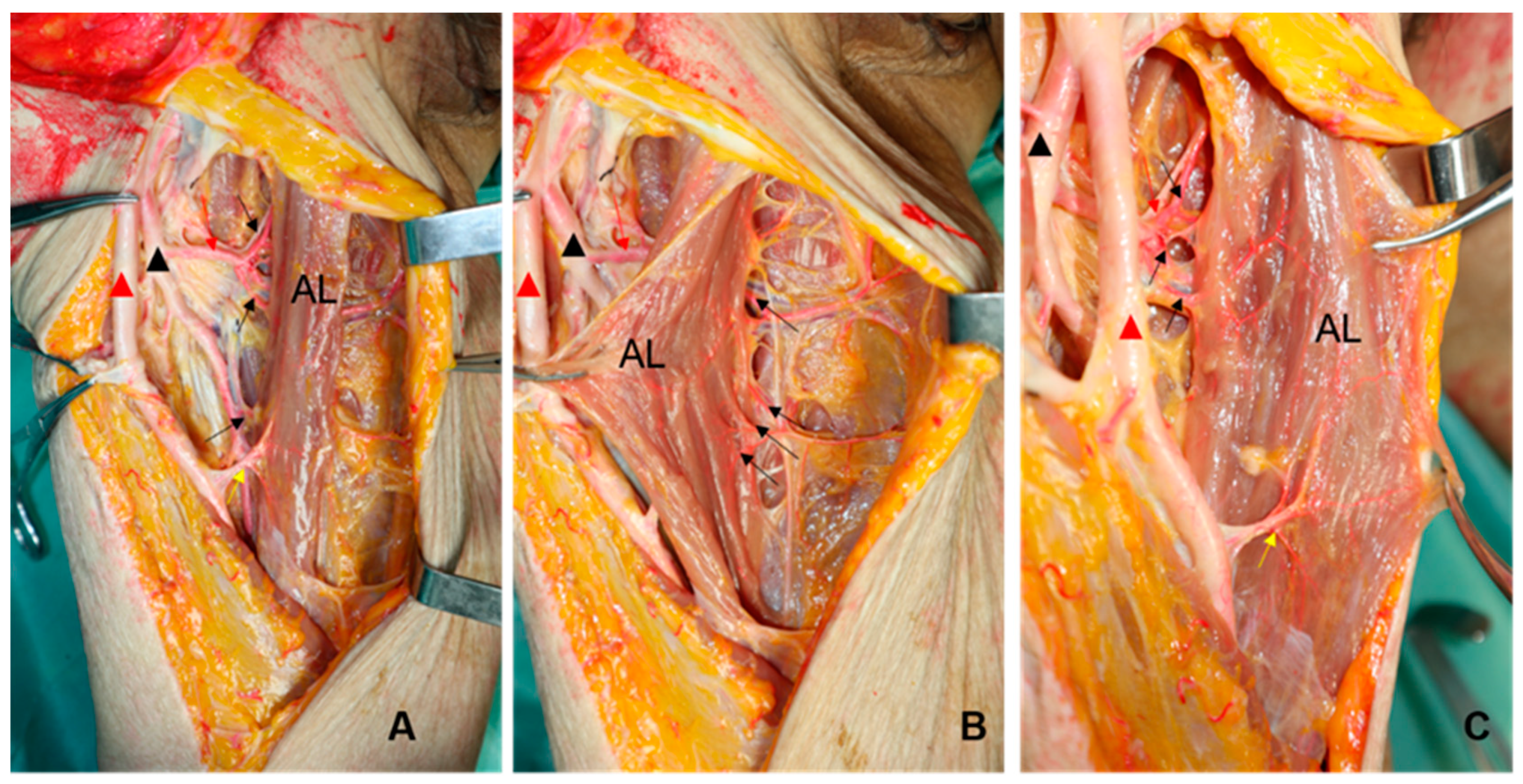
The Procedures of the Pedicled Adductor Longus Flap and the Pedicled Sartorius Flap
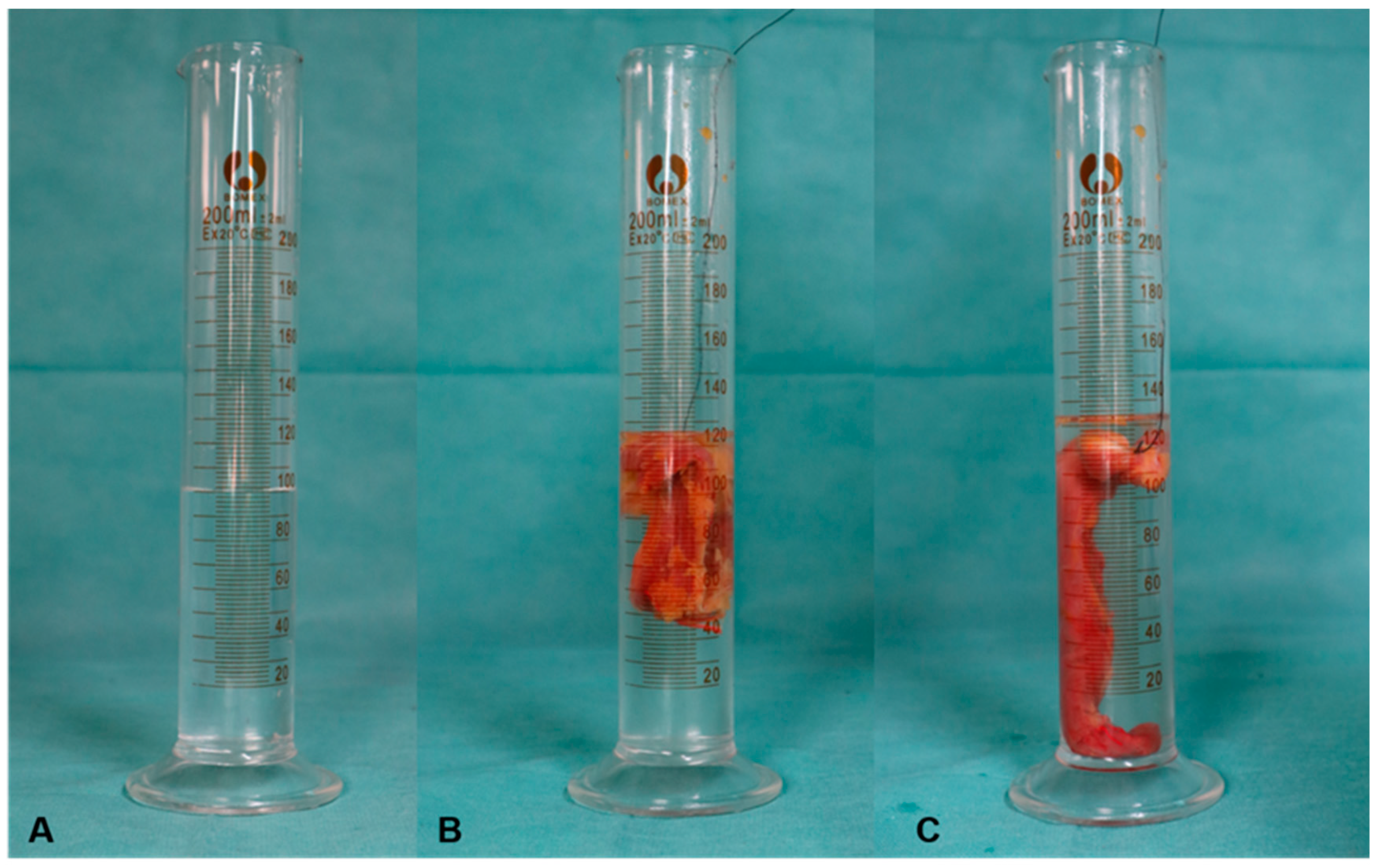
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bandyk, D.F. Vascular surgical site infection: Risk factors and preventive measures. Semin. Vasc. Surg. 2008, 21, 119–123. [Google Scholar] [CrossRef]
- Lee, E.S.; Santilli, S.M.; Olson, M.M.; Kuskowski, M.A.; Lee, J.T. Wound infection after infrainguinal bypass operations: Multivariate analysis of putative risk factors. Surg. Infect. 2000, 1, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.L.; Brahmanandam, S.; Bandyk, D.F.; Belkin, M.; Clowes, A.W.; Moneta, G.L.; Conte, M.S. Female gender and oral anticoagulants are associated with wound complications in lower extremity vein bypass: An analysis of1404 operations for critical limb ischemia. J. Vasc. Surg. 2007, 46, 1191–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, K.C.; Bartek, S.; Kuntz, K.M.; Anninos, E.; Skillman, J.J. Prospective study of wound complications in continuous infrainguinal incisions after lower limb arterial reconstruction: Incidence, risk factors, and cost. Surgery 1996, 119, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Brewer, M.B.; Ochoa, C.J.; Woo, K.; Wartman, S.M.; Nikolian, V.; Han, S.; Weaver, F.A.; Rowe, V.L. Sartorius Muscle Flaps for Vascular Groin Wound Complications. Am. Surg. 2015, 81, 1163–1169. [Google Scholar] [CrossRef]
- Johnson, J.A.; Cogbill, T.H.; Strutt, P.J.; Gundersen, A.L. Wound Complications after Infrainguinal Bypass. Arch. Surg. 1988, 123, 859–862. [Google Scholar] [CrossRef]
- Kuy, S.; Dua, A.; Desai, S.; Dua, A.; Patel, B.; Tondravi, N.; Seabrook, G.R.; Brown, K.R.; Lewis, B.D.; Lee, C.; et al. Surgical Site Infections after Lower Extremity Revascularization Procedures Involving Groin Incisions. Ann. Vasc. Surg. 2013, 28, 53–58. [Google Scholar] [CrossRef]
- Parikh, P.P.; Rubio, G.A.; Patel, K.; Gupta, K.; Jones, K.; Rey, J.; Robinson, H. Transverse versus Longitudinal Incisions for Femoral Artery Exposure in Treating Patients with Peripheral Vascular Disease. Ann. Vasc. Surg. 2018, 47, 143–148. [Google Scholar] [CrossRef]
- Audu, C.O.; Columbo, J.A.; Sun, S.J.; Perri, J.L.; Goodney, P.P.; Stone, D.H.; Nolan, B.W.; Suckow, B.D. Variation in timing and type of groin wound complications highlights the need for uniform reporting standards. J. Vasc. Surg. 2019, 69, 532–543. [Google Scholar] [CrossRef]
- Fischer, J.P.; Nelson, J.A.; Mirzabeigi, M.N.; Wang, G.J.; Foley, P.J.; Wu, L.C.; Woo, E.Y.; Kanchwala, S. Prophylactic muscle flaps in vascular surgery. J. Vasc. Surg. 2012, 55, 1081–1086. [Google Scholar] [CrossRef]
- Shermak, M.A.; Yee, K.; Wong, L.; Jones, C.E.; Wong, J. Surgical Management of Groin Lymphatic Complications after Arterial Bypass Surgery. Plast. Reconstr. Surg. 2005, 115, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Illig, K.A.; Alkon, J.E.; Smith, A.; Rhodes, J.M.; Keefer, A.; Doyle, A.; Serletti, J.; Shortell, C.K.; Davies, M.G.; Green, R.M. Rotational Muscle Flap Closure for Acute Groin Wound Infections Following Vascular Surgery. Ann. Vasc. Surg. 2004, 18, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Herrera, F.A.; Kohanzadeh, S.; Nasseri, Y.; Kansal, N.; Owens, E.L.; Bodor, R. Management of Vascular Graft Infections with Soft Tissue Flap Coverage: Improving Limb Salvage Rates–A Veterans Affairs Experience. Am. Surg. 2009, 75, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Sörelius, K.; Schiraldi, L.; Giordano, S.; Oranges, C.M.; Raffoul, W.; Di Summa, P.G. Reconstructive Surgery of Inguinal Defects: A Systematic Literature Review of Surgical Etiology and Reconstructive Technique. In Vivo 2018, 33, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Li, Z.; Li, J.; Zhu, L.; Ibrahim, Y. The Pedicled Flap of Adductor Longus, a New Technique for Inguinal Reconstruction. Front. Surg. 2021, 8, 639893. [Google Scholar] [CrossRef]
- Murthy, V.; Gopinath, K.S. Reconstruction of groin defects following radical inguinal lymphadenectomy: An evidence based review. Indian J. Surg. Oncol. 2012, 3, 130–138. [Google Scholar] [CrossRef] [Green Version]
- LoGiudice, J.A.; Haberman, K.; Sanger, J.R. The anterolateral thigh flap for groin and lower abdominal defects: A better alternative to the rectus abdominis flap. Plast. Reconstr. Surg. 2014, 133, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Nahai, F.; Hill, L.H.; Hester, R.T. Experiences with the Tensor Fascia Lata Flap. Plast. Reconstr. Surg. 1979, 63, 788–799. [Google Scholar] [CrossRef]
- Ali, A.T.; Rueda, M.; Desikan, S.; Moursi, M.M.; An, R.; Spencer, H.; Rueda, S.; Eidt, J.F. Outcomes after retroflexed gracilis muscle flap for vascular infections in the groin. J. Vasc. Surg. 2016, 64, 452–457. [Google Scholar] [CrossRef]
- Armstrong, P.A.; Back, M.R.; Bandyk, D.F.; Johnson, B.L.; Shames, M.L. Selective application of sartorius muscle flaps and aggressive staged surgical debridement can influence long-term outcomes of complex prosthetic graft infections. J. Vasc. Surg. 2007, 46, 71–78. [Google Scholar] [CrossRef]
- Chateau, F.; Duisit, J.; Lengel, B.; Vanwijck, R. Techniques for coverage of infected vascular grafts in the groin. Acta Chir. Belg. 2010, 110, 487–491. [Google Scholar] [CrossRef] [PubMed]
- De Santis, F.; Chaves Brait, C.M.; Caravelli, G.; Pompei, S.; Di Cintio, V. Salvage of infected vascular graft via ‘perivascular venous banding’ technique coupled with rectus abdominis myocutaneous muscle flap transposition. Vascular 2013, 21, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Ducic, I.; Dayan, J.H.; Attinger, C.E.; Curry, P. Complex perineal and groin wound reconstruction using the extended dissection technique of the gracilis flap. Plast. Reconstr. Surg. 2008, 122, 472–478. [Google Scholar] [CrossRef]
- Baronofsky, I.D. Technique of inguinal node dissection. Surgery. 1948, 24, 555–567. [Google Scholar] [PubMed]
- Buckland, A.; Pan, W.R.; Dhar, S.; Edwards, G.; Rozen, W.M.; Ashton, M.W.; Taylor, G.I. Neurovascular Anatomy of Sartorius Muscle Flaps: Implications for Local Transposition and Facial Reanimation. Plast. Reconstr. Surg. 2009, 123, 44–54. [Google Scholar] [CrossRef]
- Manjunath, K.N.; Venkatesh, M.S.; Shivaprasad, A. Distal major pedicle of sartorius muscle flap: Anatomical study and its clinical implications. Indian J. Plast. Surg. 2018, 51, 040–045. [Google Scholar] [CrossRef] [Green Version]
- Mardini, S.; Tsai, F.-C.; Wei, F.-C. The thigh as a model for free style free flaps. Clin. Plast. Surg. 2003, 30, 473–480. [Google Scholar] [CrossRef]
- Wei, F.-C.; Mardini, S. Free-Style Free Flaps. Plast. Reconstr. Surg. 2004, 114, 910–916. [Google Scholar] [CrossRef]
- Lattimore, C.M.; Meneveau, M.O.; Marsh, K.M.; Shada, A.L.; Slingluff, C.L.; Dengel, L.T. A Novel Fascial Flap Technique After Inguinal Complete Lymph Node Dissection for Melanoma. J. Surg. Res. 2022, 278, 356–363. [Google Scholar] [CrossRef]
- Siddharth, P.; Smith, N.L.; Mason, R.A.; Giron, F. Variational anatomy of the deep femoral artery. Anat. Rec. 1985, 212, 206–209. [Google Scholar] [CrossRef]
- Kalinin, R.E.; Suchkov, I.A.; Klimentova, A.; Shanaev, I.N. Clinical anatomy of deep femoral vessels in the area of femoral triangle. Angiol. Vasc. Surg. 2021, 27, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Garg, K. Front of the thigh. In Chaurasia BD. BD Chaurasia’s Human Anatomy (Regional and Applied Dissection and Clinical), 5th ed.; CBS Publishers and Distributors Pvt Ltd: New Delhi, India, 2010; Volume 2, pp. 51–55. [Google Scholar]
- Williams, P.L. Gray’s Anatomy, 38th ed.; Churchill Livingstone: London, UK, 1995; pp. 870–871. [Google Scholar]
- Benninghoff. Makroskopische und mikroskopische Anatomie des Menschen; Urban & Schwarzenberg: Munchen, Wien, Baltimore, Germany, 1985; pp. 356–357. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Sex | Age | Cause of Death | Left-Side (mL) | Right-Side (mL) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Volume of ALF | Volume of SAF | Volume Difference | Ratio of SAF/ALF | Volume of ALF | Volume of SAF | Volume Difference | Ratio of SAF/ALF | ||||
| 1 | M | 61 | EC 1 | 32 | 20 | 12 | 0.63 | 40 | 25 | 15 | 0.63 |
| 2 | F | 75 | CI 2 | 34 | 26 | 8 | 0.76 | 38 | 24 | 14 | 0.63 |
| 3 | F | 65 | EC 1 | 46 | 35 | 11 | 0.76 | 49 | 34 | 15 | 0.69 |
| 4 | M | 51 | CH 3 | 120 | 84 | 36 | 0.70 | 130 | 89 | 41 | 0.68 |
| 5 | M | 54 | CI 1 | 30 | 21 | 9 | 0.70 | 53 | 38 | 15 | 0.72 |
| 6 | M | 74 | CI 1 | 52 | 39 | 13 | 0.75 | 32 | 23 | 9 | 0.72 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; Li, Z.; Li, J.; Zhu, B.; Xu, Q. Comparison of Pedicled Adductor Longus and Pedicled Sartorius Flap in Inguinal Reconstruction, a Fresh Cadaver Study. J. Pers. Med. 2023, 13, 143. https://doi.org/10.3390/jpm13010143
Zhang H, Li Z, Li J, Zhu B, Xu Q. Comparison of Pedicled Adductor Longus and Pedicled Sartorius Flap in Inguinal Reconstruction, a Fresh Cadaver Study. Journal of Personalized Medicine. 2023; 13(1):143. https://doi.org/10.3390/jpm13010143
Chicago/Turabian StyleZhang, Hong, Zhenfeng Li, Jianmin Li, Binghong Zhu, and Qingjia Xu. 2023. "Comparison of Pedicled Adductor Longus and Pedicled Sartorius Flap in Inguinal Reconstruction, a Fresh Cadaver Study" Journal of Personalized Medicine 13, no. 1: 143. https://doi.org/10.3390/jpm13010143