
Assessment of the Accuracy of Two Different Dynamic Navigation System Registration Methods for Dental Implant Placement in the Posterior Area: An In Vitro Study


Abstract
:1. Introduction
2. Materials and Methods
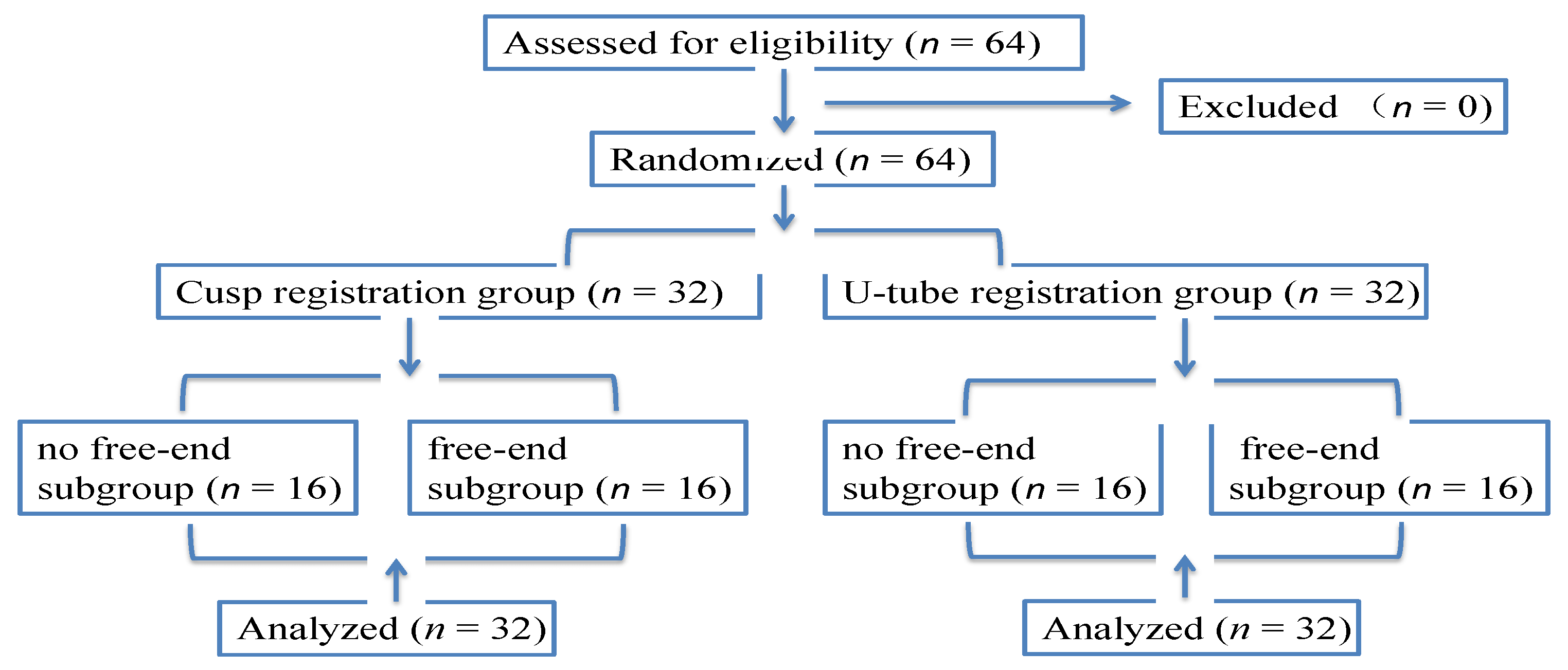
2.1. Study Design
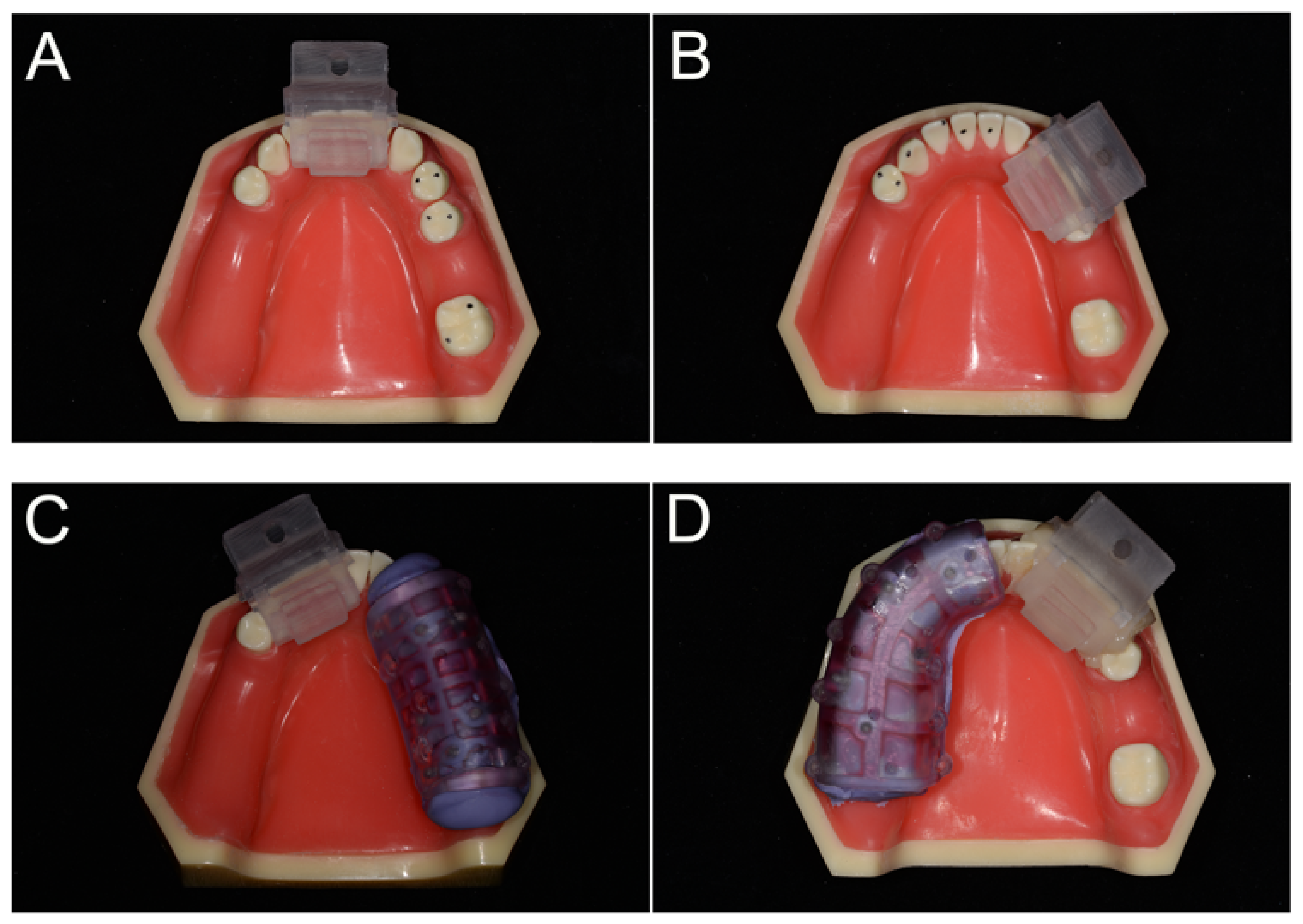
2.2. Model Preparation
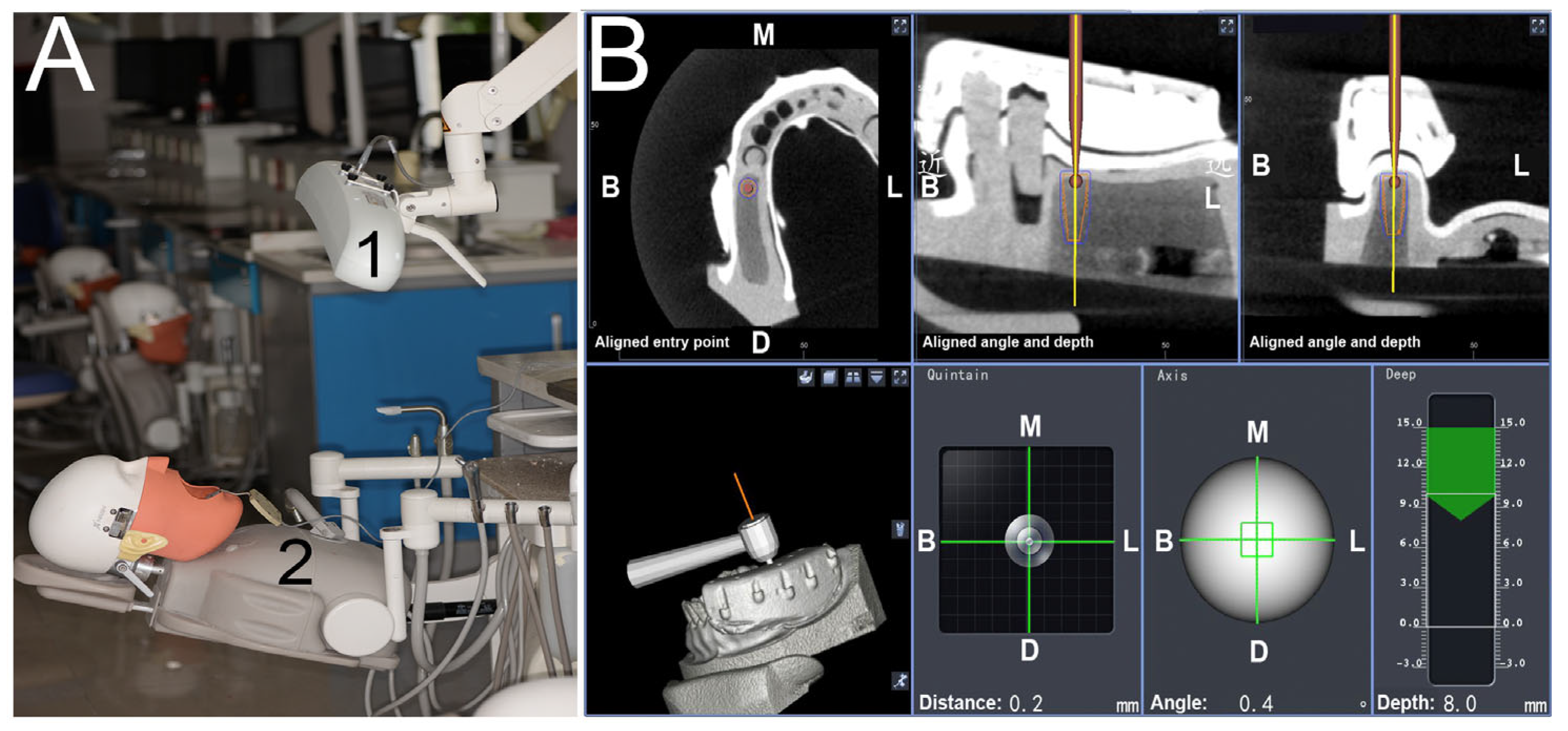
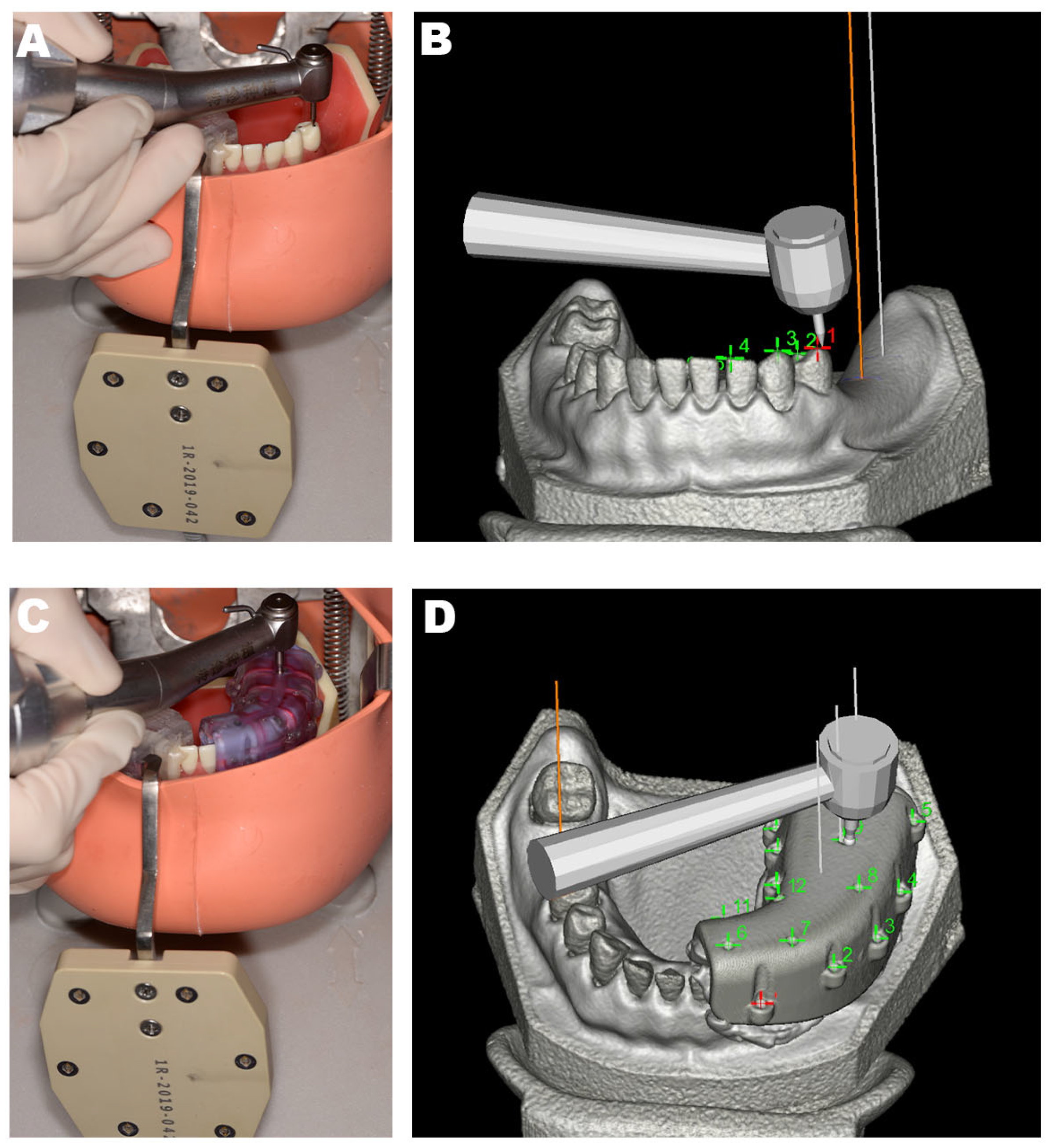
2.3. Treatment Preparation and Surgical Procedures
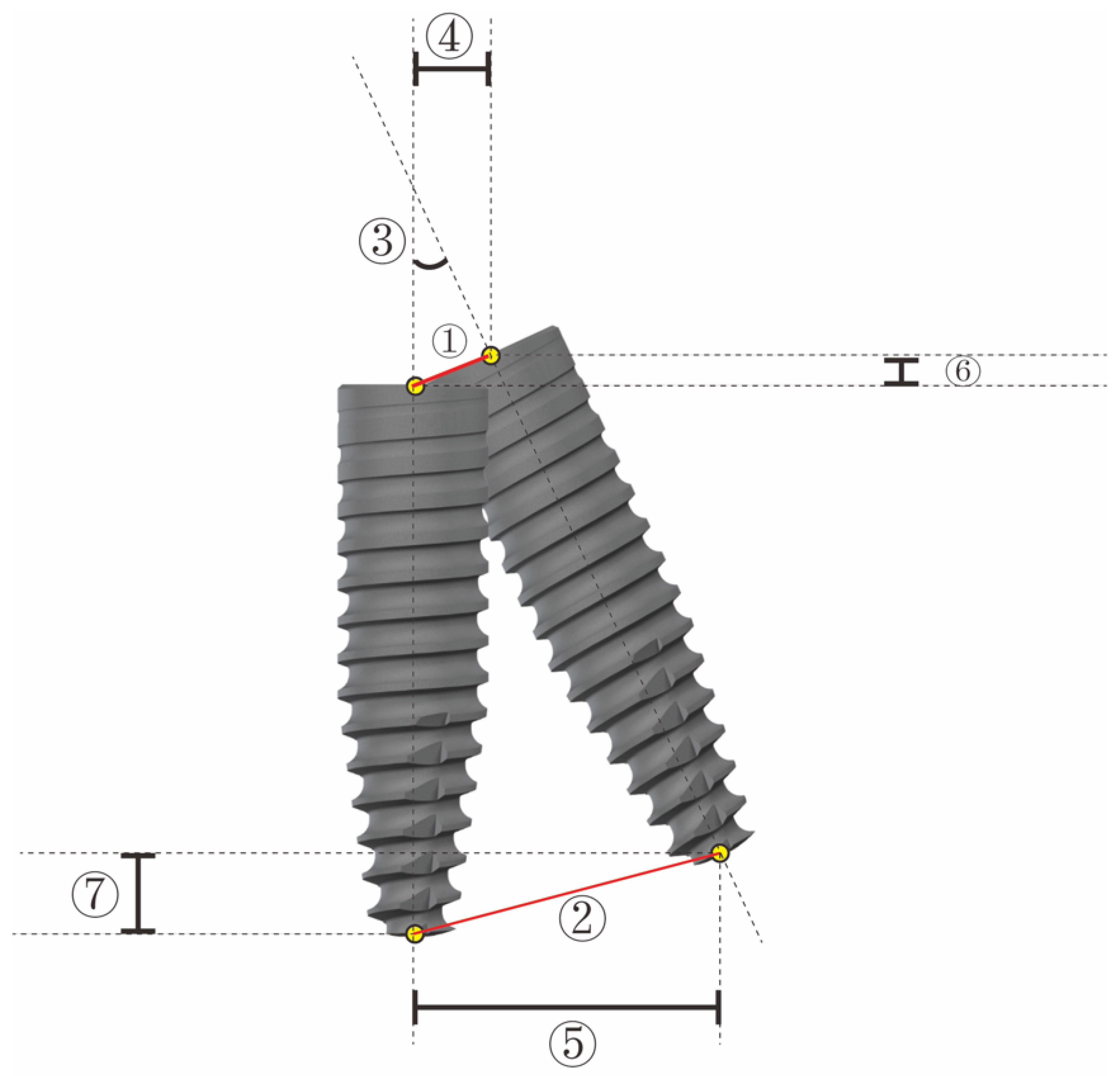
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buser, D.; Janner, S.F.; Wittneben, J.G.; Bragger, U.; Ramseier, C.A.; Salvi, G.E. 10-year survival and success rates of 511 titanium implants with a sandblasted and acid-etched surface: A retrospective study in 303 partially edentulous patients. Clin. Implant Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int. J. Oral Maxillofac. Implant. 2004, 19, 43–61. [Google Scholar]
- Reda, R.; Zanza, A.; Cicconetti, A.; Bhandi, S.; Guarnieri, R.; Testarelli, L.; Di Nardo, D. A Systematic Review of Cementation Techniques to Minimize Cement Excess in Cement-Retained Implant Restorations. Methods Protoc. 2022, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, R.; Zanza, A.; D’Angelo, M.; Di Nardo, D.; Del Giudice, A.; Mazzoni, A.; Reda, R.; Testarelli, L. Correlation between Peri-Implant Marginal Bone Loss Progression and Peri-Implant Sulcular Fluid Levels of Metalloproteinase-8. J. Pers. Med. 2022, 12, 58. [Google Scholar] [CrossRef]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant Placement Accuracy Using Dynamic Navigation. Int. J. Oral Maxillofac. Implants 2017, 32, 92–99. [Google Scholar] [CrossRef]
- D’haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2020 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Kaewsiri, D.; Panmekiate, S.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. The accuracy of static vs. dynamic computer-assisted implant surgery in single tooth space: A randomized controlled trial. Clin. Oral Implants Res. 2019, 30, 505–514. [Google Scholar] [CrossRef]
- Eggers, G.; Mühling, J.; Marmulla, R. Image-to-patient registration techniques in head surgery. Int. J. Oral Maxillofac. Surg. 2006, 35, 1081–1095. [Google Scholar] [CrossRef]
- Xiaojun, C.; Ming, Y.; Yanping, L.; Chengtao, W. Image guided oral implantology and its application IN the placement of zygoma implants. Comput. Methods Programs Biomed. 2009, 93, 162–273. [Google Scholar] [CrossRef]
- Sinikovic, B.; Kramer, F.J.; Swennen, G.; Lubbers, H.T.; Dempf, R. Reconstruction of orbital wall defects with calcium phosphatecement: Clinical and histological indings in a sheep model. Int. J. Oral Maxillofac. Surg. 2007, 36, 54–61. [Google Scholar] [CrossRef]
- Gellrich, N.C.; Schramm, A.; Hammer, B.; Rojas, S.; Cufi, D.; Lagreze, W.; Schmelzeisen, R. Computer-assisted secondary reconstruction of unilateral posttraumatic orbital deformity. Plast. Reconstr. Surg. 2002, 110, 1417–1429. [Google Scholar]
- Hardy, S.M.; Melroy, C.; White, D.R.; Dubin, M.; Senior, B. A comparison of computeraided surgery registration methods for endoscopic sinus surgery. Am. J. Rhinol. 2006, 20, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Westendorff, C.; Leitner, C.; Bartz, D.; Reinert, S. Validation of 3D-lasersurface registration for image-guided craniomaxillofacial surgery. J. Craniomaxillofac. Surg. 2005, 33, 13–18. [Google Scholar] [CrossRef]
- Marmulla, R.; Muhling, J.; Eggers, G.; Hassfeld, S. Markerless patient registration. A new technique for image-guided surgery of the lateral base of the skull. HNO 2005, 53, 148–154. [Google Scholar]
- Marmulla, R.; Eggers, G.; Muhling, J. Laser surface registration for lateral skull base surgery. Minim. Invasive Neurosurg. 2005, 48, 181–185. [Google Scholar] [CrossRef]
- Grevers, G.; Leunig, A.; Klemens, A.; Hagedorn, H. CAS of the paranasal sinuses etechnology and clinical experience with the vector-vision-compact-system in 102 patients. Laryngorhinootologie 2002, 81, 476–483. [Google Scholar] [CrossRef]
- Swennen, G.R.J.; Schutyser, F.; Hausamen, J.E. Three-Dimensional Cephalometry. A Color Atlas and Manual; Springer: Berlin/Heidelberg, Germany; New York, NY, USA, 2006. [Google Scholar]
- Stefanelli, L.V.; De Groot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a dynamic dental implant navigation system in a private practice. Int. J. Oral Maxillofac. Implants 2019, 34, 205–213. [Google Scholar] [CrossRef]
- Emery, R.W.; Merritt, S.A.; Lank, K.; Gibbs, J.D. Accuracy of dynamic navigation for dental implant placement-model-based evaluation. J. Oral Implantol. 2016, 42, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.K.; Yuh, D.Y.; Huang, R.Y.; Fu, E.; Tsai, C.F.; Chiang, C.Y. Accuracy of implant placement with a navigation system, a laboratory guide, and freehand drilling. Int. J. Oral Maxillofac. Implants 2018, 33, 1213–1218. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W.; Cullum, D.R.; Sheikh, A. Implant placement is more accurate using dynamic navigation. J. Oral Maxillofac. Surg. 2017, 75, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Jorba-García, A.; Figueiredo, R.; González-Barnadas, A.; Camps-Font, O.; Valmaseda-Castellón, E. Accuracy and the role of experience in dynamic computer guided dental implant surgery: An in-vitro study. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, 332. [Google Scholar] [CrossRef] [PubMed]
- Krithikadatta, J.; Gopikrishna, V.; Datta, M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef] [PubMed]
- Stefanelli, L.V.; Mandelaris, G.A.; DeGroot, B.S.; Di Carlo, S. Accuracy of a Novel Trace-Registration Method for Dynamic Navigation Surgery. Int. J. Periodontics Restor. Dent. 2020, 40, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Pellegrino, G.; Ferri, A.; Prati, C.; Gandolfi, M.G.; Marchetti, C. Dynamic navigation in implant dentistry: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implants. 2021, 36, 121–140. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Q.; Zhang, J. Role of dynamic navigation systems in enhancing the accuracy of implant placement: A systematic review and meta-analysis of clinical studies. J. Oral Maxillofac. Surg. 2021, 79, 2061–2070. [Google Scholar] [CrossRef]
- Farley, N.; Kennedy, K.; McGlumphy, E.; Clelland, N. Split-Mouth Comparison of the Accuracy of Computer-Generated and Conventional Surgical Guides. Int. J. Oral Maxillofac. Implants 2013, 28, 563–572. [Google Scholar] [CrossRef]
- Kramer, F.J.; Baethge, C.; Swennen, G.; Rosahl, S. Navigated vs. conventional implant insertion for maxillary single tooth replacement. Clin. Oral Implants Res. 2005, 16, 60–68. [Google Scholar] [CrossRef]
- Ruppin, J.; Popovic, A.; Strauss, M.; Stoll, C. Evaluation of the accuracy of three different computer-aided surgery systems in dental implantology: Optical tracking vs. stereolithographic. splint systems. Clin. Oral Implants Res. 2008, 19, 709–716. [Google Scholar]
- Somogyi-Ganss, E.; Holmes, H.I.; Jokstad, A. Accuracy of a novel prototype dynamic computer-assisted surgery system. Clin. Oral Implants Res. 2015, 26, 882–890. [Google Scholar] [CrossRef]
- Maló, P.; Rangert, B.; Nobre, M. All-on-4 immediate-function concept with Brånemark System implants for completely edentulous maxillae: A 1-year retrospective clinical study. Clin. Implant Dent. Relat. Res. 2005, 7 (Suppl. 1), 88–94. [Google Scholar] [CrossRef] [PubMed]
- Mandelaris, G.A.; Stefanelli, L.V.; De Groot, B.S. Dynamic Navigation for Surgical Implant Placement: Overview of Technology, Key Concepts, and a Case Report. Compend. Contin. Educ. Dent. 2018, 39, 614–621. [Google Scholar] [PubMed]
- Brief, J.; Edinger, D.; Hassfeld, S.; Eggers, G. Accuracy of image guided implantology. Clin. Oral Implants Res. 2005, 16, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Mischkowski, R.A.; Zinser, M.J.; Neugebauer, J.; Kübler, A.C.; Zöller, J.E. Comparison of static and dynamic computer-assisted guidance methods in implantology. Int. J. Comput. Dent. 2006, 9, 23–35. [Google Scholar] [PubMed]
- Jung, R.E.; Schneider, D.; Ganeles, J. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral. Maxillofac. Implants 2009, 24, 92–109. [Google Scholar]
- Gillot, L.; Cannas, B.; Friberg, B.L.; Vrielinck, L.; Rohner, D.; Pettersson, A. Accuracy of virtually planned and conventionally placed implants in edentulous cadaver maxillae and mandibles: A preliminary report. J. Prosthet. Dent. 2014, 112, 798–804. [Google Scholar] [CrossRef]
- Widmann, G. Image-guided surgery and medical robotics in the cranial area. Biomed. Imaging Interv. J. 2007, 3, 11. [Google Scholar] [CrossRef] [Green Version]
- Widmann, G.; Bale, R.J. Accuracy in computer-aided implant surgery—A review. Int. J. Oral Maxillofac. Implants 2006, 21, 305–313. [Google Scholar]
- Widmann, G.; Stoffner, R.; Schullian, P.; Bale, R.J. Comparison of the Accuracy of Invasive and Noninvasive Registration Methods for Image-Guided Oral Implant Surgery. Int. J. Oral Maxillofac. Implants 2010, 25, 491–498. [Google Scholar]
- Luebbers, H.T.; Messmer, P.; Obwegeser, J.A.; Matthews, F. Comparison of different registration methods for surgical navigation in cranio-maxillofacial surgery. J. Craniomaxillofac. Surg. 2008, 36, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Ma, F.; Sun, F.; Wei, T.; Ma, Y. Comparison of the accuracy of two different dynamic navigation system registration methods for dental implant placement: A retrospective study. Clin. Implant Dent. Relat. Res. 2022, 24, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Ewers, R.; Schicho, K.; Undt, G.; Wanschitz, F.; Truppe, M.; Wagner, A. Basic research and 12 years of clinical experience in computer-assisted navigation technology: A review. Int. J. Oral Maxillofac. Surg. 2005, 34, 1–8. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Enrolled | Cusp | U-Tube | p Value | |
|---|---|---|---|---|
| N | 64 | 32 | 32 | |
| Angular deviation (°) | 1.970 ± 1.042 | 2.118 ± 0.940 | 1.823 ± 0.999 | 0.141 |
| Entry deviation (mm) | 1.089 ± 0.515 | 1.172 ± 0.469 | 1.006 ± 0.567 | 0.320 |
| Apex deviation (mm) | 1.174 ± 0.531 | 1.23 ± 0.520 | 1.119 ± 0.561 | 0.126 |
| EH (mm) | 0.582 ± 0.358 | 0.554 ± 0.340 | 0.609 ± 0.378 | 0.544 |
| AH (mm) | 0.824 ± 0.429 | 0.738 ± 0.406 | 0.909 ± 0.442 | 0.112 |
| ED (mm) | 0.731 ± 0.529 | 0.780 ± 0.493 | 0.683 ± 0.583 | 0.476 |
| AD (mm) | 0.750 ± 0.574 | 0.791 ± 0.491 | 0.707 ± 0.660 | 0.567 |
| Cusp | U-tube | |||
|---|---|---|---|---|
| Without Distal-Extension Absence (n = 16) | Distal-Extension Absence (n = 16) | Without Distal-Extension Absence (n = 16) | Distal-Extension Absence (n = 16) | |
| Angular deviation (°) | 1.957 ± 0.941 | 2.278 ± 0.941 | 1.675 ± 1.066 | 1.971 ± 1.265 |
| p value | 0.724 | 0.515 | ||
| Entry deviation (mm) | 1.186 ± 0.512 | 1.158 ± 0.469 | 0.787 ± 0.459 | 1.224 ± 0.592 |
| p value | 0.323 | 0.026 * | ||
| Apex deviation (mm) | 1.260 ± 0.510 | 1.120 ± 0.544 | 0.868 ± 0.443 | 1.369 ± 0.567 |
| p value | 1 | 0.012 * | ||
| EH (mm) | 0.513 ± 0.242 | 0.595 ± 0.422 | 0.544 ± 0.269 | 0.685 ± 0.458 |
| p value | 0.505 | 0.263 | ||
| AH (mm) | 0.663 ± 0.330 | 0.813 ± 0.468 | 0.895 ± 0.306 | 1.023 ± 0.530 |
| p value | 0.301 | 0.145 | ||
| ED (mm) | 0.819 ± 0.574 | 0.741 ± 0.412 | 0.491 ± 0.400 | 0.875 ± 0.581 |
| p value | 0.663 | 0.061 | ||
| AD (mm) | 0.832 ± 0.568 | 0.751 ± 0.416 | 0.494 ± 0.401 | 0.921 ± 0.802 |
| p value | 0.648 | 0.067 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, T.; Ma, F.; Sun, F.; Ma, Y. Assessment of the Accuracy of Two Different Dynamic Navigation System Registration Methods for Dental Implant Placement in the Posterior Area: An In Vitro Study. J. Pers. Med. 2023, 13, 139. https://doi.org/10.3390/jpm13010139
Wei T, Ma F, Sun F, Ma Y. Assessment of the Accuracy of Two Different Dynamic Navigation System Registration Methods for Dental Implant Placement in the Posterior Area: An In Vitro Study. Journal of Personalized Medicine. 2023; 13(1):139. https://doi.org/10.3390/jpm13010139
Chicago/Turabian StyleWei, Tai, Feifei Ma, Feng Sun, and Yu Ma. 2023. "Assessment of the Accuracy of Two Different Dynamic Navigation System Registration Methods for Dental Implant Placement in the Posterior Area: An In Vitro Study" Journal of Personalized Medicine 13, no. 1: 139. https://doi.org/10.3390/jpm13010139