
Non-Typical Clinical Presentation of COVID-19 Patients in Association with Disease Severity and Length of Hospital Stay

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
- Age between 15 and 85 years old.
- Saturation of Oxygen above 94% in room air (FiO2:21%).
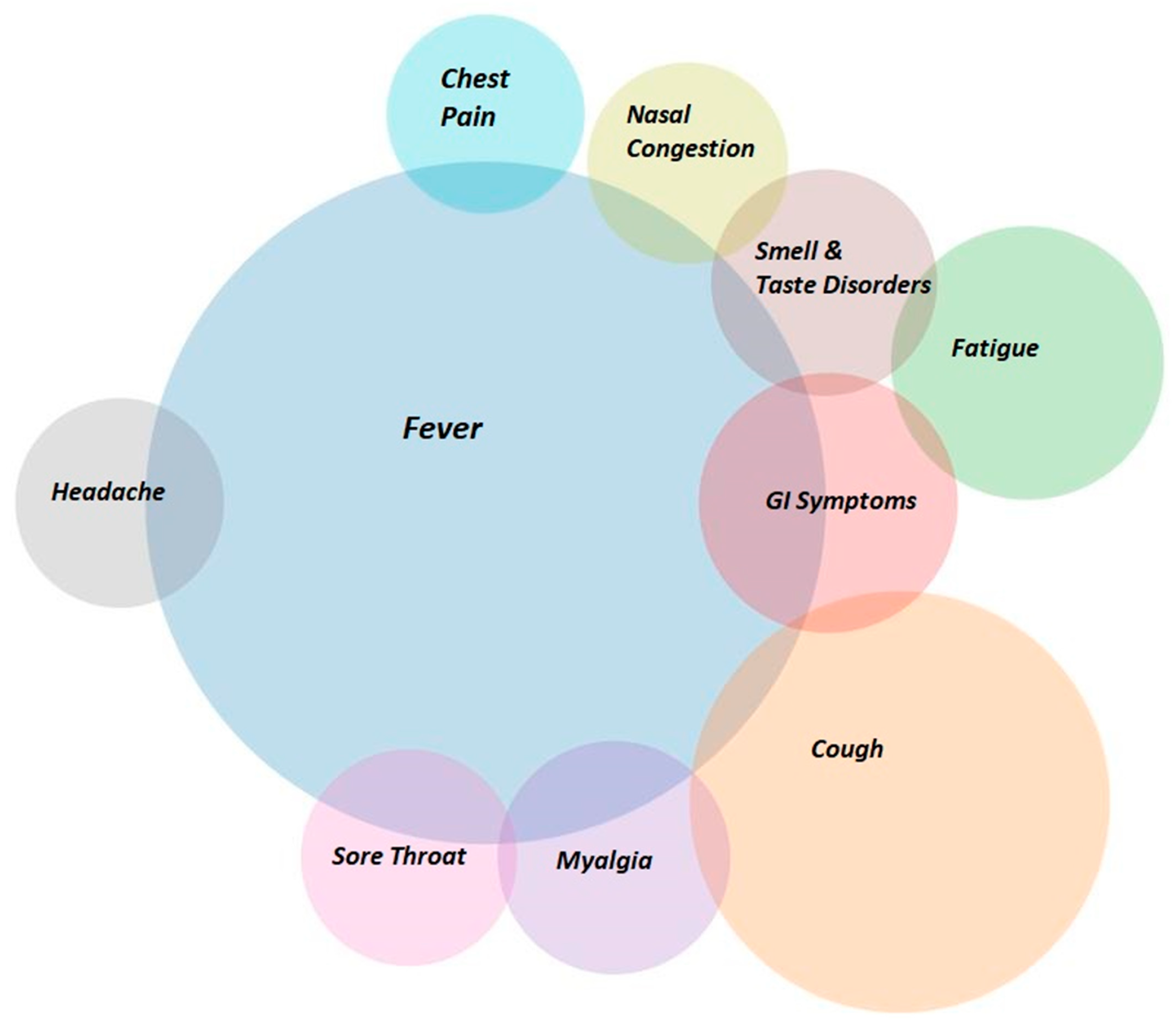
- Symptoms including headache, smell and taste disorders, abdominal pain, diarrhea, vomiting, myalgia, or common respiratory infection symptoms (fever, cough, shortness of breath, fatigue).
- Respiratory Rate (R-R) < 20 per minute.
- Positive nasopharyngeal swab test for SARS-CoV-2 (RT-PCR or POC-PCR).
- Exclusion criteria:
- Age <15 years old or >85 years old.
- Oxygen saturation (SatO2) <94% in room air.
- Respiratory Rate RR > 20.
- Negative nasopharyngeal swab test for SARS-CoV-2 (RT-PCR or POC-PCR).
- Asymptomatic patients.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. Available online: http://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 12 February 2020).
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; Marder, E.P.; Raz, K.M.; Felix, S.E.B.; Tie, Y.; Fullerton, K.E. Coronavirus Disease 2019 Case Surveillance—United States, January 22–May 30, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 759–765. [Google Scholar] [CrossRef]
- Alimohamadi, Y.; Sepandi, M.; Taghdir, M.; Hosamirudsari, H. Determine the most common clinical symptoms in COVID-19 patients: A systematic review and meta-analysis. J. Prev. Med. Hyg. 2020, 61, E304–E312. [Google Scholar]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_3 (accessed on 12 February 2020).
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20,133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kompaniyets, L.; Goodman, A.B.; Belay, B.; Freedman, D.S.; Sucosky, M.S.; Lange, S.J.; Gundlapalli, A.V.; Boehmer, T.K.; Blanck, H.M. Body Mass Index and Risk for COVID-19-Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death—United States, March–December 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Zhang, D.; Xu, J.; Chen, Z.; Yang, T.; Zhao, P.; Chen, G.; Cheng, G.; Wang, Y.; Bi, J.; et al. Prediction for Progression Risk in Patients With COVID-19 Pneumonia: The CALL Score. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 1393–1399. [Google Scholar] [CrossRef] [Green Version]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.K.; Harrison, E.M.; Ho, A.; Docherty, A.B.; Knight, S.R.; van Smeden, M.; Abubakar, I.; Lipman, M.; Quartagno, M.; Pius, R.; et al. Development and validation of the ISARIC 4C Deterioration model for adults hospitalised with COVID-19: A prospective cohort study. Lancet Respir. Med. 2021, 9, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Valdes, A.M.; Freidin, M.B.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Ganesh, S.; Varsavsky, T.; Cardoso, M.J.; El-Sayed Moustafa, J.S.; et al. Real-time tracking of self-reported symptoms to predict potential COVID-19. Nat. Med. 2020, 26, 1037–1040. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Lee, K.A.; Ni Lochlainn, M.; Varsavsky, T.; Murray, B.; Graham, M.S.; Menni, C.; Modat, M.; Bowyer, R.C.E.; Nguyen, L.H.; et al. Symptom clusters in COVID-19: A potential clinical prediction tool from the COVID Symptom Study app. Sci. Adv. 2021, 7, eabd4177. [Google Scholar] [CrossRef]
- Pullen, M.F.; Skipper, C.P.; Hullsiek, K.H.; Bangdiwala, A.S.; Pastick, K.A.; Okafor, E.C.; Lofgren, S.M.; Rajasingham, R.; Engen, N.W.; Galdys, A.; et al. Symptoms of COVID-19 Outpatients in the United States. Open Forum Infect. Dis. 2020, 7, ofaa271. [Google Scholar] [CrossRef] [PubMed]
- Dixon, B.E.; Wools-Kaloustian, K.K.; Fadel, W.F.; Duszynski, T.J.; Yiannoutsos, C.; Halverson, P.K.; Menachemi, N. Symptoms and symptom clusters associated with SARS-CoV-2 infection in community-based populations: Results from a statewide epidemiological study. PloS ONE 2021, 16, e0241875. [Google Scholar] [CrossRef]
- Al Mutair, A.; Alhumaid, S.; Alhuqbani, W.N.; Zaidi AR, Z.; Alkoraisi, S.; Al-Subaie, M.F.; AlHindi, A.M.; Abogosh, A.K.; Alrasheed, A.K.; Alsharafi, A.A.; et al. Clinical, epidemiological, and laboratory characteristics of mild-to-moderate COVID-19 patients in Saudi Arabia: An observational cohort study. Eur. J. Med. Res. 2020, 25, 61. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Qu, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Zeleke, A.J.; Moscato, S.; Miglio, R.; Chiari, L. Length of Stay Analysis of COVID-19 Hospitalizations Using a Count Regression Model and Quantile Regression: A Study in Bologna, Italy. Int. J. Environ. Res. Public Health 2022, 19, 2224. [Google Scholar] [CrossRef]
- Birhanu, A.; Merga, B.T.; Ayana, G.M.; Alemu, A.; Negash, B.; Dessie, Y. Factors associated with prolonged length of hospital stay among COVID-19 cases admitted to the largest treatment center in Eastern Ethiopia. SAGE Open Med. 2022, 10, 20503121211070366. [Google Scholar] [CrossRef]
- Thiruvengadam, G.; Lakshmi, M.; Ramanujam, R. A Study of Factors Affecting the Length of Hospital Stay of COVID-19 Patients by Cox-Proportional Hazard Model in a South Indian Tertiary Care Hospital. J. Prim. Care Community Health 2021, 12, 21501327211000231. [Google Scholar] [CrossRef]
- Vekaria, B.; Overton, C.; Wiśniowski, A.; Ahmad, S.; Aparicio-Castro, A.; Curran-Sebastian, J.; Eddleston, J.; Hanley, N.A.; House, T.; Kim, J.; et al. Hospital length of stay for COVID-19 patients: Data-driven methods for forward planning. BMC Infect Dis. 2021, 21, 700. [Google Scholar] [CrossRef] [PubMed]
- Rees, E.M.; Nightingale, E.S.; Jafari, Y.; Waterlow, N.R.; Clifford, S.; Pearson, C.A.B.; CMMID Working Group; Jombart, T.; Procter, S.R.; Knight, G.M. COVID-19 length of hospital stay: A systematic review and data synthesis. BMC Med. 2020, 18, 270. [Google Scholar] [CrossRef]
- International Severe Acute Respiratory and Emerging Infections Consortium (ISARIC). COVID-19 Report. 2020. Available online: https://media.tghn.org/medialibrary/2020/04/ISARIC_Data_Platform_COVID-%19_Report_8APR20.pdf (accessed on 8 April 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Hannawi, S.; Hannawi, H.; Bin Naeem, K.; Elemam, N.M.; Hachim, M.Y.; Hachim, I.Y.; Darwish, A.S.; Al Salmi, I. Clinical and Laboratory Profile of Hospitalized Symptomatic COVID-19 Patients: Case Series Study From the First COVID-19 Center in the UAE. Front. Cell. Infect. Microbiol. 2021, 11, 632965. [Google Scholar] [CrossRef]
- Delavari, A.; Asgari, S.; Alimohamadi, Y.; Vosoogh-Moghaddam, A.; Sadeghi, A.; Shahrousvand, S.; Zakeri, A.; Moradzadeh, R.; Akbarpour, S. xsGastrointestinal symptoms are associated with a lower risk of hospitalization and mortality and Outcomes in COVID-19. BMC Gastroenterol 2022, 22, 119. [Google Scholar] [CrossRef] [PubMed]
- Ghayda, R.; Lee, J.; Lee, J.; Kim, D.; Lee, K.; Hong, S.; Han, Y.; Kim, J.; Yang, J.; Kronbichler, A.; et al. Correlations of Clinical and Laboratory Characteristics of COVID-19: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 5026. [Google Scholar] [CrossRef]
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or Moderate COVID-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef]
- ISARIC Clinical Characterisation Group. COVID-19 symptoms at hospital admission vary with age and sex: Results from the ISARIC prospective multinational observational study. Infection 2021, 49, 889–905. [Google Scholar] [CrossRef]
- Ghimire, S.; Sharma, S.; Patel, A.; Budhathoki, R.; Chakinala, R.; Khan, H.; Lincoln, M.; Georgeston, M. Diarrhea Is Associated with Increased Severity of Disease in COVID-19: Systemic Review and Metaanalysis. SN Compr. Clin. Med. 2021, 3, 28–35. [Google Scholar] [CrossRef]
- Comoglu, Ş.; Öztürk, S.; Kant, A.; Arslan, M.; Karakoc, H.N.; Yılmaz, G. Evaluation of Diarrhea in Patients with COVID-19. Dig. Dis. 2021, 39, 622–625. [Google Scholar] [CrossRef]
- Ramachandran, P.; Onukogu, I.; Ghanta, S.; Gajendran, M.; Perisetti, A.; Goyal, H.; Aggarwal, A. Gastrointestinal Symptoms and Outcomes in Hospitalized Coronavirus Disease 2019 Patients. Dig. Dis. 2020, 38, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, Y.; Zhang, Y.; Liu, Y.; Liu, Y. Are gastrointestinal symptoms associated with higher risk of Mortality in COVID-19 patients? A systematic review and meta-analysis. BMC Gastroenterol. 2022, 22, 106. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.-C.; Bouabdallaoui, N.; L’Allier, P.L.; Gaudet, D.; Shah, B.; Pillinger, M.H.; Lopez-Sendon, J.; da Luz, P.; Verret, L.; Audet, S.; et al. Colchicine for community-treated patients with COVID-19 (COLCORONA): A phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial. Lancet Respir. Med. 2021, 9, 924–932. [Google Scholar] [CrossRef] [PubMed]
- The Expert Committee of the Ministry of Health. The Task Force for the Therapeutic Guidelines for the Treatment of Patients with COVID-19 Infection. Initial Assessment of the Severity of the Disease in Primary Care at Home, in Private Practice and in Emergency Departments. (Hellenic National Public Health Organization—EODY). Available online: https://eody.gov.gr/wp-content/uploads/2021/03/COVID-19-therapeutikos-algorithmos-20210222.pdf (accessed on 20 March 2021).
- Hellenic Society of Internal Medicine, Patient with COVID-19 (SARS-COV 2 Infection) Management at Home. Available online: https://www.isathens.gr/images/eggrafa/EEEswtPath-diaxerisi-katoikon-asthenous-me-COVID19.pdf (accessed on 8 February 2021).
- AbuRuz, S.; Al-Azayzih, A.; ZainAlAbdin, S.; Beiram, R.; Al Hajjar, M. Clinical characteristics and risk factors for mortality among COVID-19 hospitalized patients in UAE: Does ethnic origin have an impact. PLoS ONE 2022, 17, e0264547. [Google Scholar] [CrossRef]
- Abayomi, A.; Odukoya, O.; Osibogun, A.; Wright, O.; Adebayo, B.; Balogun, M.; Abdus-Salam, I.; Bowale, A.; Mutiu, B.; Saka, B.; et al. Presenting Symptoms and Predictors of Poor Outcomes Among 2184 Patients with COVID-19 in Lagos State, Nigeria. Int. J. Infect. Dis. 2021, 102, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Keeley, P.; Buchanan, D.; Carolan, C.; Pivodic, L.; Tavabie, S.; Noble, S. Symptom burden and clinical profile of COVID-19 deaths: A rapid systematic review and evidence summary. BMJ Support. Palliat. Care 2020, 10, 381–384. [Google Scholar] [CrossRef]
- Jain, V.; Yuan, J.-M. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: A systematic review and meta-analysis. Int. J. Public Health 2020, 65, 533–546. [Google Scholar] [CrossRef]
- Zhao, Z.; Chen, A.; Hou, W.; Graham, J.M.; Li, H.; Richman, P.S.; Thode, H.C.; Singer, A.J.; Duong, T.Q. Prediction model and risk scores of ICU admission and mortality in COVID-19. PLoS ONE 2020, 15, e0236618. [Google Scholar] [CrossRef]
- Pouw, N.; van de Maat, J.; Veerman, K.; Oever, J.T.; Janssen, N.; Abbink, E.; Reijers, M.; de Mast, Q.; Hoefsloot, W.; van Crevel, R.; et al. Clinical characteristics and outcomes of 952 hospitalized COVID-19 patients in The Netherlands: A retrospective cohort study. PLoS ONE 2021, 16, e0248713. [Google Scholar] [CrossRef]
- Argenziano, M.G.; Bruce, S.L.; Slater, C.L.; Tiao, J.R.; Baldwin, M.R.; Barr, R.G.; Chang, B.P.; Chau, K.H.; Choi, J.J.; Gavin, N.; et al. Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: Retrospective case series. BMJ 2020, 369, m1996. [Google Scholar] [CrossRef]
- de Souza, F.S.H.; Hojo-Souza, N.S.; Batista, B.D.D.O.; da Silva, C.M.; Guidoni, D.L. On the analysis of mortality risk factors for hospitalized COVID-19 patients: A data-driven study using the major Brazilian database. PLoS ONE 2021, 16, e0248580. [Google Scholar] [CrossRef] [PubMed]
- He, X.; Cheng, X.; Feng, X.; Wan, H.; Chen, S.; Xiong, M. Clinical Symptom Differences Between Mild and Severe COVID-19 Patients in China: A Meta-Analysis. Front. Public Health 2021, 8, 561264. [Google Scholar] [CrossRef]
- Lenfant, C. Chest pain of cardiac and noncardiac origin. Metabolism 2010, 59 (Suppl. 1), S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Weng, L.M.; Su, X.; Wang, X.Q. Pain Symptoms in Patients with Coronavirus Disease (COVID-19): A Literature Review. J. Pain Res. 2021, 14, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.I.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, L.; Jin, H.; Wang, M.; Hu, Y.; Chen, S.; He, Q.; Chang, J.; Hong, C.; Zhou, Y.; Wang, D.; et al. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020, 77, 683–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arentz, M.; Yim, E.; Klaff, L.; Lokhandwala, S.; Riedo, F.X.; Chong, M.; Lee, M. Characteristics and Outcomes of 21 Critically Ill Patients With COVID-19 in Washington State. JAMA 2020, 323, 1612–1614. [Google Scholar] [CrossRef] [Green Version]
- Cao, J.; Tu, W.-J.; Cheng, W.; Yu, L.; Liu, Y.-K.; Hu, X.; Liu, Q. Clinical Features and Short-term Outcomes of 102 Patients with Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 748–755. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Oxley, T.J.; Mocco, J.; Majidi, S.; Kellner, C.P.; Shoirah, H.; Singh, I.P.; De Leacy, R.A.; Shigematsu, T.; Ladner, T.R.; Yaeger, K.A.; et al. Large-Vessel Stroke as a Presenting Feature of COVID-19 in the Young. N. Engl. J. Med. 2020, 382, e60. [Google Scholar] [CrossRef]
- Merkler, A.E.; Parikh, N.S.; Mir, S.; Gupta, A.; Kamel, H.; Lin, E.; Lantos, J.; Schenck, E.J.; Goyal, P.; Bruce, S.S.; et al. Risk of Ischemic Stroke in Patients With Coronavirus Disease 2019 (COVID-19) vs Patients With Influenza. JAMA Neurol. 2020, 77, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Xue, L.; Legido-Quigley, H.; Khan, M.; Wu, H.; Peng, X.; Li, X.; Li, P. Understanding factors influencing the length of hospital stay among non-severe COVID-19 patients: A retrospective cohort study in a Fangcang shelter hospital. PLoS ONE 2020, 15, e0240959. [Google Scholar] [CrossRef] [PubMed]
- Guo:, A.; Lu, J.; Tan, H.; Kuang, Z.; Luo, Y.; Yang, T.; Xu, J.; Yu, J.; Wen, C.; Shen, A. Risk factors on admission associated with hospital length of stay in patients with COVID-19: A retrospective cohort study. Sci. Rep. 2021, 11, 7310. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N | % | |
|---|---|---|
| Male | 349 | 61.3 |
| Female | 220 | 38.7 |
| Age, (standard deviation) | 42.25 (15.37) | |
| Fever | 435 | 76.3 |
| Cough | 166 | 29.1 |
| Shortness of Breath | 29 | 5.1 |
| Fatigue | 70 | 12.3 |
| Nasal Congestion/Rhinorrhoea | 38 | 6.7 |
| Sore Throat | 44 | 7.7 |
| Chest Pain | 37 | 6.5 |
| Smell and Taste Disorders | 48 | 8.4 |
| Headache | 41 | 7.2 |
| Myalgia | 51 | 8.9 |
| GI Disorders | 63 | 11.1 |
| Rash | 1 | 0.2 |
| Other | 32 | 5.6 |
| Joint Pain | 16 | 50.0 |
| Hematuria-Dysuria | 2 | 6.3 |
| Heart Palpitations | 1 | 3.1 |
| Flank Pain | 1 | 3.1 |
| Anorexia | 1 | 3.1 |
| Impaired consciousness | 1 | 3.1 |
| Conjunctivitis | 1 | 3.1 |
| Dizziness and Vertigo | 1 | 3.1 |
| Hoarseness | 1 | 3.1 |
| Syncope | 2 | 6.3 |
| Xerostomia | 1 | 3.1 |
| Pre-syncope | 3 | 9.4 |
| Earache | 1 | 3.1 |
| Typical | 499 | 87.5 |
| Atypical | 286 | 50.2 |
| Admission | 188 | 33.0 |
| Death | 5 | 0.9 |
| ICU Admission | 13 | 2.3 |
| Length of Hospital Stay, (standard deviation) | 9.53 (8.99) |
| Non-Typical | |||||
|---|---|---|---|---|---|
| No | Yes | X2 | p | ||
| Admission | Yes | 112 (39.4%) | 76 (26.6%) | 10.67 | 0.001 |
| Death | Yes | 3 (1.1%) | 2 (0.7%) | 0.209 | 0.685 |
| ICU a Admission | Yes | 10 (3.5%) | 3 (1%) | 3.908 | 0.048 |
| Admission | ||||
|---|---|---|---|---|
| No | Yes | X2 124.234 | p < 0.001 | |
| Fever | 262 (60.2%) | 173 (39.8%) | ||
| Cough | 85 (51.2%) | 81 (48.8%) | ||
| Shortness of breath | 13 (44.8%) | 16 (55.2%) | ||
| Fatigue | 34 (48.6%) | 36 (51.4%) | ||
| Nasal congestion and Rhinorrhea | 35 (92.1%) | 3 (7.9%) | ||
| Sore Throat | 37 (84.1%) | 7 (15.9%) | ||
| Chest pain | 19 (51.4%) | 18 (48.6%) | ||
| Smell and taste disorders | 40 (83.3%) | 8 (16.7%) | ||
| Headache | 30 (73.2%) | 11 (26.8%) | ||
| Myalgia | 42 (82.4%) | 9 (17.6%) | ||
| GI Symptoms a | 35 (55.6%) | 28 (44.4%) | ||
| Rash | 1 (100%) | 0 (0%) | ||
| Other | 23 (71.9%) | 9 (28.1%) | ||
| Variable | Odds Ratio | p-Value |
|---|---|---|
| Fever | 6.64 [3.47;12.7] | 0.0001 |
| Cough | 2.82 [1.85;4.3] | 0.0001 |
| Shortness of Breath | 2.64 [1.05;6.62] | 0.0384 |
| Fatigue | 3.09 [1.71;5.58] | 0.000176 |
| Nasal Congestion/Rhinorrhea | 0.415 [0.117;1.48] | 0.175 |
| Sore Throat | 0.466 [0.185;1.17] | 0.105 |
| Chest Pain | 2.1 [0.978;4.51] | 0.0571 |
| Smell and Taste Disorders | 0.558 [0.231;1.35] | 0.196 |
| Headache | 0.821 [0.377;1.79] | 0.618 |
| Myalgia | 0.484 [0.215;1.09] | 0.0795 |
| GI Disorders | 2.05 [1.13;3.72] | 0.0176 |
| Other | 1.57 [0.64;3.86] | 0.324 |
| Fever | ||||
|---|---|---|---|---|
| No (N = 15) | Yes (N = 173) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (3–9) | 7 (5–12) | −1.294 | 0.196 |
| Cough | ||||
| No (N = 107) | Yes (N = 81) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (5–12) | 8 (4–12) | −0.319 | 0.750 |
| Shortness of Breath | ||||
| No (N = 172) | Yes (N = 16) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (4.25–12) | 8 (4–14.5) | −0.043 | 0.965 |
| Fatigue | ||||
| No (N = 152) | Yes (N = 36) | Mann–Whitney | p | |
| Length of Stay (days) | 8 (4.25–12) | 7 (4–12) | −0.372 | 0.710 |
| Sore throat | ||||
| No (N = 181) | Yes (N = 7) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (4.5–12) | 8 (3–12) | −0.500 | 0.617 |
| Chest Pain | ||||
| No (N = 170) | Yes (N = 18) | Mann–Whitney | p | |
| Length of Stay (days) | 8 (5–12) | 5.5 (4–8.25) | −1.420 | 0.155 |
| Smell and Taste Disorders | ||||
| No (N = 180) | Yes (N = 8) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (4–12) | 9.5 (8–11.5) | −1.082 | 0.279 |
| Headache | ||||
| No (N = 177) | Yes (N = 11) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (4–12) | 7 (6–11) | −0.195 | 0.846 |
| Myalgia | ||||
| No (N = 179) | Yes (N = 9) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (4–12) | 6 (4–14.5) | −0.072 | 0.942 |
| GI symptoms | ||||
| No (N = 160) | Yes (N = 28) | Mann–Whitney | p | |
| Length of Stay (days) | 8 (4.25–12) | 6.5 (4–9.75) | −0.985 | 0.325 |
| Other | ||||
| No (N = 179) | Yes (N = 9) | Mann–Whitney | p | |
| Length of Stay (days) | 7 (4–12) | 9 (5.5–9) | −0.334 | 0.739 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skourtis, A.; Ekmektzoglou, K.; Xanthos, T.; Stouraitou, S.; Iacovidou, N. Non-Typical Clinical Presentation of COVID-19 Patients in Association with Disease Severity and Length of Hospital Stay. J. Pers. Med. 2023, 13, 132. https://doi.org/10.3390/jpm13010132
Skourtis A, Ekmektzoglou K, Xanthos T, Stouraitou S, Iacovidou N. Non-Typical Clinical Presentation of COVID-19 Patients in Association with Disease Severity and Length of Hospital Stay. Journal of Personalized Medicine. 2023; 13(1):132. https://doi.org/10.3390/jpm13010132
Chicago/Turabian StyleSkourtis, Alexandros, Konstantinos Ekmektzoglou, Theodoros Xanthos, Stella Stouraitou, and Nicoletta Iacovidou. 2023. "Non-Typical Clinical Presentation of COVID-19 Patients in Association with Disease Severity and Length of Hospital Stay" Journal of Personalized Medicine 13, no. 1: 132. https://doi.org/10.3390/jpm13010132