
Comprehensive Analysis of Clinicopathological and Molecular Features to Predict Anti-PD-1-Based Therapy Efficacy in Patients with Advanced Gastric Signet Ring Cell Carcinoma

Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Molecular Characteristics
2.3. Assessment and Statistical Analysis
3. Results
3.1. Patients’ Characteristics
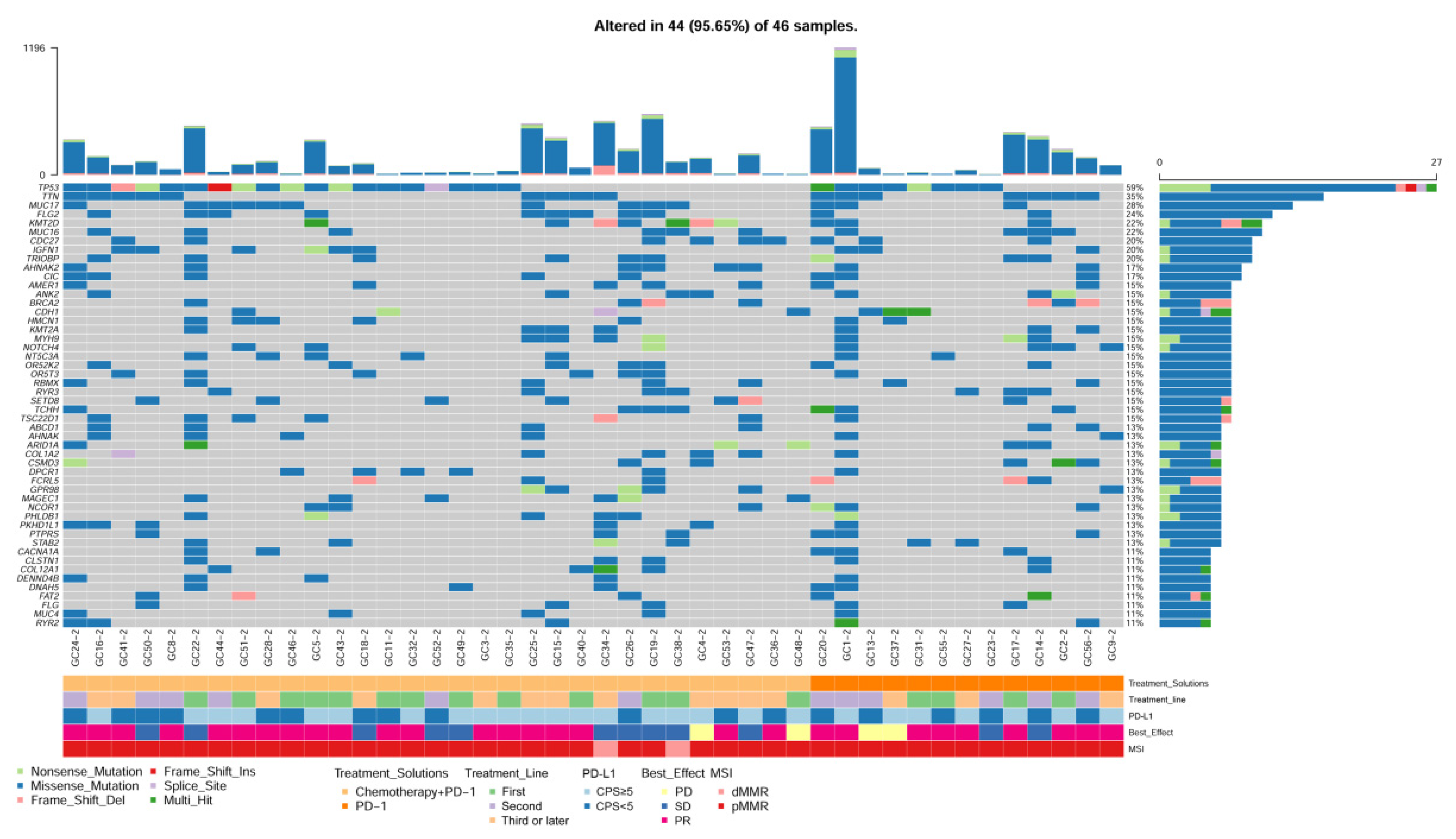
3.2. Molecular Alteration in Primary and Metastatic Tissues
3.3. Clinicopathological and Molecular Characteristics Associated with Anti-PD-1 Response in SRCC
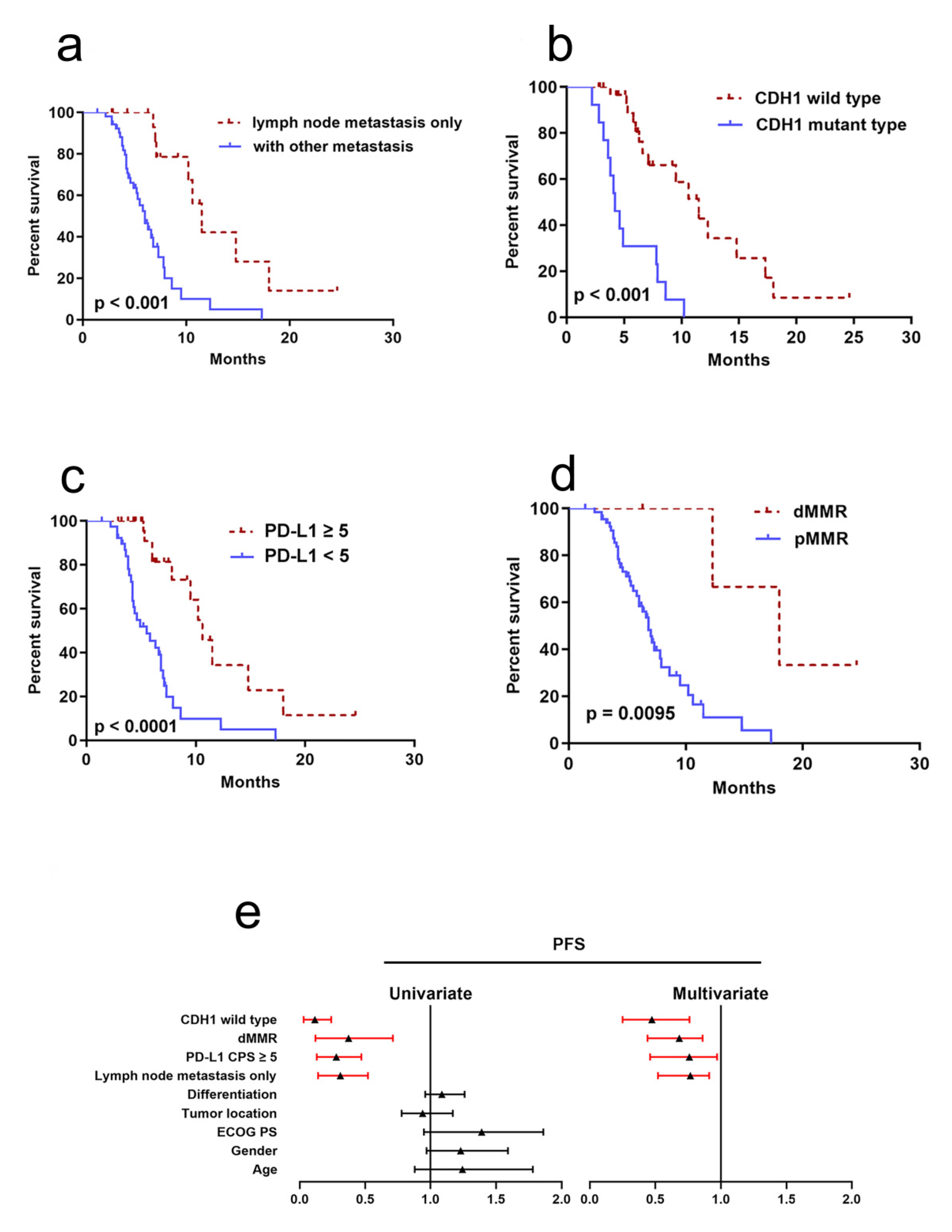
3.4. Clinicopathological and Molecular Factors to Predict PFS
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.D.; Grothe, W.; Haerting, J.; Kleber, G.; Grothey, A.; Fleig, W.E. Chemotherapy in advanced gastric cancer: A systematic review and meta-analysis based on aggregate data. J. Clin. Oncol. 2006, 24, 2903–2909. [Google Scholar] [CrossRef] [PubMed]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Tomasek, J.; Yong, C.J.; Dumitru, F.; Passalacqua, R.; Goswami, C.; Safran, H.; Dos Santos, L.V.; Aprile, G.; Ferry, D.R.; et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2014, 383, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.G.; Wang, Z.N.; Sun, Z.; Liu, F.N.; Yu, M.; Xu, H.M. Clinicopathologic characteristics and prognosis of signet ring cell carcinoma of the stomach: Results from a Chinese mono-institutional study. J. Surg. Oncol. 2011, 103, 700–703. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Cai, H.; Sheng, W.; Yu, L.; Long, Z.; Shi, Y.; Wang, Y. Clinicopathological Characteristics and Survival Outcomes of Primary Signet Ring Cell Carcinoma in the Stomach: Retrospective Analysis of Single Center Database. PLoS ONE 2015, 10, e0144420. [Google Scholar] [CrossRef]
- Adachi, Y.; Yasuda, K.; Inomata, M.; Sato, K.; Shiraishi, N.; Kitano, S. Pathology and prognosis of gastric carcinoma: Well versus poorly differentiated type. Cancer 2000, 89, 1418–1424. [Google Scholar] [CrossRef]
- Kunz, P.L.; Gubens, M.; Fisher, G.A.; Ford, J.M.; Lichtensztajn, D.Y.; Clarke, C.A. Long-term survivors of gastric cancer: A California population-based study. J. Clin. Oncol. 2012, 30, 3507–3515. [Google Scholar] [CrossRef]
- Jin, S.; Xu, B.; Yu, L.; Fu, Y.; Wu, H.; Fan, X.; Wei, J.; Liu, B. The PD-1, PD-L1 expression and CD3+ T cell infiltration in relation to outcome in advanced gastric signet-ring cell carcinoma, representing a potential biomarker for immunotherapy. Oncotarget 2017, 8, 38850–38862. [Google Scholar] [CrossRef] [Green Version]
- Vinay, D.S.; Ryan, E.P.; Pawelec, G.; Talib, W.H.; Stagg, J.; Elkord, E.; Lichtor, T.; Decker, W.K.; Whelan, R.L.; Kumara, H.; et al. Immune evasion in cancer: Mechanistic basis and therapeutic strategies. Semin. Cancer Biol. 2015, 35, S185–S198. [Google Scholar] [CrossRef]
- Spranger, S. Mechanisms of tumor escape in the context of the T-cell-inflamed and the non-T-cell-inflamed tumor microenvironment. Int. Immunol. 2016, 28, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Wu, A.A.; Drake, V.; Huang, H.S.; Chiu, S.; Zheng, L. Reprogramming the tumor microenvironment: Tumor-induced immunosuppressive factors paralyze T cells. Oncoimmunology 2015, 4, e1016700. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, N.A.; Mazieres, J.; Planchard, D.; Stinchcombe, T.E.; Dy, G.K.; Antonia, S.J.; Horn, L.; Lena, H.; Minenza, E.; Mennecier, B.; et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): A phase 2, single-arm trial. Lancet Oncol. 2015, 16, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Ansell, S.M.; Lesokhin, A.M.; Borrello, I.; Halwani, A.; Scott, E.C.; Gutierrez, M.; Schuster, S.J.; Millenson, M.M.; Cattry, D.; Freeman, G.J.; et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin’s lymphoma. N. Engl. J. Med. 2015, 372, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Kang, Y.K.; Boku, N.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Doi, T.; Jang, R.W.; Muro, K.; Satoh, T.; Machado, M.; Sun, W.; Jalal, S.I.; Shah, M.A.; Metges, J.P.; et al. Safety and Efficacy of Pembrolizumab Monotherapy in Patients With Previously Treated Advanced Gastric and Gastroesophageal Junction Cancer: Phase 2 Clinical KEYNOTE-059 Trial. JAMA Oncol. 2018, 4, e180013. [Google Scholar] [CrossRef]
- Shitara, K.; Ozguroglu, M.; Bang, Y.J.; Di Bartolomeo, M.; Mandala, M.; Ryu, M.H.; Fornaro, L.; Olesinski, T.; Caglevic, C.; Chung, H.C.; et al. Pembrolizumab versus paclitaxel for previously treated, advanced gastric or gastro-oesophageal junction cancer (KEYNOTE-061): A randomised, open-label, controlled, phase 3 trial. Lancet 2018, 392, 123–133. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.M.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat. Med. 2018, 24, 1449–1458. [Google Scholar] [CrossRef]
- Wang, D.S.; Yang, H.; Liu, X.Y.; Chen, Z.G.; Wang, Y.; Fong, W.P.; Hu, M.T.; Zheng, Y.C.; Zheng, Y.; Li, B.K.; et al. Dynamic monitoring of circulating tumor DNA to predict prognosis and efficacy of adjuvant chemotherapy after resection of colorectal liver metastases. Theranostics 2021, 11, 7018–7028. [Google Scholar] [CrossRef]
- Zhao, S.; Lv, L.; Zheng, K.; Tian, Y.; Zheng, J.C.; Jiang, C.G. Prognosis and Biological Behavior of Gastric Signet-Ring Cell Carcinoma Better or Worse: A Meta-Analysis. Front. Oncol. 2021, 11, 603070. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Gao, Y.; Qi, C.; Yuan, X.; Li, J.; Xu, Q.; Luo, C.; Chen, L.; Zhuo, W.; Xu, Z.; et al. Clinicopathological Characteristics and Prognosis of Signet Ring Gastric Cancer: A Population-Based Study. Front. Oncol. 2021, 11, 580545. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research, N. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakiuchi, M.; Nishizawa, T.; Ueda, H.; Gotoh, K.; Tanaka, A.; Hayashi, A.; Yamamoto, S.; Tatsuno, K.; Katoh, H.; Watanabe, Y.; et al. Recurrent gain-of-function mutations of RHOA in diffuse-type gastric carcinoma. Nat. Genet. 2014, 46, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.S.; Kim, K.M.; Ting, J.C.; Yu, K.; Fu, J.; Liu, S.; Cristescu, R.; Nebozhyn, M.; Gong, L.; Yue, Y.G.; et al. Genomic landscape and genetic heterogeneity in gastric adenocarcinoma revealed by whole-genome sequencing. Nat. Commun. 2014, 5, 5477. [Google Scholar] [CrossRef] [Green Version]
- Shu, Y.; Zhang, W.; Hou, Q.; Zhao, L.; Zhang, S.; Zhou, J.; Song, X.; Zhang, Y.; Jiang, D.; Chen, X.; et al. Prognostic significance of frequent CLDN18-ARHGAP26/6 fusion in gastric signet-ring cell cancer. Nat. Commun. 2018, 9, 2447. [Google Scholar] [CrossRef] [Green Version]
- Wang, F.; Wei, X.L.; Wang, F.H.; Xu, N.; Shen, L.; Dai, G.H.; Yuan, X.L.; Chen, Y.; Yang, S.J.; Shi, J.H.; et al. Safety, efficacy and tumor mutational burden as a biomarker of overall survival benefit in chemo-refractory gastric cancer treated with toripalimab, a PD-1 antibody in phase Ib/II clinical trial NCT02915432. Ann. Oncol. 2019, 30, 1479–1486. [Google Scholar] [CrossRef] [Green Version]
- Davis, A.A.; Patel, V.G. The role of PD-L1 expression as a predictive biomarker: An analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 278. [Google Scholar] [CrossRef]
- Shitara, K.; Van Cutsem, E.; Bang, Y.J.; Fuchs, C.; Wyrwicz, L.; Lee, K.W.; Kudaba, I.; Garrido, M.; Chung, H.C.; Lee, J.; et al. Efficacy and Safety of Pembrolizumab or Pembrolizumab Plus Chemotherapy vs Chemotherapy Alone for Patients With First-line, Advanced Gastric Cancer: The KEYNOTE-062 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1571–1580. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Bendell, J.; Calvo, E.; Kim, J.W.; Ascierto, P.A.; Sharma, P.; Ott, P.A.; Peltola, K.; Jaeger, D.; Evans, J.; et al. CheckMate-032 Study: Efficacy and Safety of Nivolumab and Nivolumab Plus Ipilimumab in Patients With Metastatic Esophagogastric Cancer. J. Clin. Oncol. 2018, 36, 2836–2844. [Google Scholar] [CrossRef]
- Bang, Y.J.; Ruiz, E.Y.; Van Cutsem, E.; Lee, K.W.; Wyrwicz, L.; Schenker, M.; Alsina, M.; Ryu, M.H.; Chung, H.C.; Evesque, L.; et al. Phase III, randomised trial of avelumab versus physician’s choice of chemotherapy as third-line treatment of patients with advanced gastric or gastro-oesophageal junction cancer: Primary analysis of JAVELIN Gastric 300. Ann. Oncol. 2018, 29, 2052–2060. [Google Scholar] [CrossRef]
- Mishima, S.; Kawazoe, A.; Nakamura, Y.; Sasaki, A.; Kotani, D.; Kuboki, Y.; Bando, H.; Kojima, T.; Doi, T.; Ohtsu, A.; et al. Clinicopathological and molecular features of responders to nivolumab for patients with advanced gastric cancer. J. Immunother. Cancer 2019, 7, 24. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Xie, T.; Wang, Z.; Tong, S.; Zhao, X.; Zhao, F.; Cai, J.; Wei, X.; Peng, Z.; Shen, L. Efficacy and predictive biomarkers of immunotherapy in Epstein-Barr virus-associated gastric cancer. J. Immunother. Cancer 2022, 10, e004080. [Google Scholar] [CrossRef]
- Mitchell, K.G.; Negrao, M.V.; Parra, E.R.; Li, J.; Zhang, J.; Dejima, H.; Vaporciyan, A.A.; Swisher, S.G.; Weissferdt, A.; Antonoff, M.B.; et al. Lymphovascular Invasion Is Associated With Mutational Burden and PD-L1 in Resected Lung Cancer. Ann. Thorac. Surg. 2020, 109, 358–366. [Google Scholar] [CrossRef]
- Puccini, A.; Poorman, K.; Catalano, F.; Seeber, A.; Goldberg, R.M.; Salem, M.E.; Shields, A.F.; Berger, M.D.; Battaglin, F.; Tokunaga, R.; et al. Molecular profiling of signet-ring-cell carcinoma (SRCC) from the stomach and colon reveals potential new therapeutic targets. Oncogene 2022, 41, 3455–3460. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Yoshihiro, T.; Ariyama, H.; Ito, M.; Nakano, M.; Semba, Y.; Nogami, J.; Tsuchihashi, K.; Yamauchi, T.; Ueno, S.; et al. Potential therapeutic targets discovery by transcriptome analysis of an in vitro human gastric signet ring carcinoma model. Gastric Cancer 2022, 25, 862–878. [Google Scholar] [CrossRef]
- Wei, Y.; Li, Y.; Du, Q.; Peng, X.; Jin, J.; Guo, H.; Li, Y.; Li, Q. Effects of Clinicopathological Characteristics on the Survival of Patients Treated with PD-1/PD-L1 Inhibitor Monotherapy or Combination Therapy for Advanced Cancer: A Systemic Review and Meta-Analysis. J. Immunol. Res. 2020, 2020, 5269787. [Google Scholar] [CrossRef]
- Huemer, F.; Lang, D.; Westphal, T.; Gampenrieder, S.P.; Hutarew, G.; Weiss, L.; Hackl, H.; Lamprecht, B.; Rinnerthaler, G.; Greil, R. Baseline Absolute Lymphocyte Count and ECOG Performance Score Are Associated with Survival in Advanced Non-Small Cell Lung Cancer Undergoing PD-1/PD-L1 Blockade. J. Clin. Med. 2019, 8, 1014. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N = 71 | All | Responder | Non-Responder | ORR | p-Value | |
|---|---|---|---|---|---|---|
| Age | <65 | 34 | 15 | 19 | 44.1% | 0.702 |
| ≥65 | 37 | 18 | 19 | 48.6% | ||
| Gender | Male | 47 | 20 | 27 | 42.5% | 0.353 |
| Female | 24 | 13 | 11 | 54.1% | ||
| ECOG PS | 0 | 21 | 16 | 5 | 76.1% | 0.001 |
| ≥1 | 50 | 17 | 33 | 34.0% | ||
| Primary tumor location | EGJ/Cardia | 11 | 4 | 7 | 36.3% | 0.622 |
| Body | 32 | 17 | 15 | 53.1% | ||
| Antrum | 24 | 11 | 13 | 45.8% | ||
| Unknown | 4 | 1 | 3 | 25.0% | ||
| Differentiation | Moderately | 2 | 1 | 1 | 50.0% | 0.674 |
| Poorly | 65 | 31 | 34 | 48.4% | ||
| Unknown | 4 | 1 | 3 | 25.0% | ||
| Lauren classification | Intestinal | 0 | 0 | 0 | - | 0.317 |
| Diffuse | 64 | 31 | 33 | 48.4% | ||
| Mixed | 7 | 2 | 5 | 28.5% | ||
| Previous gastrectomy | Yes | 8 | 3 | 5 | 37.5% | 0.589 |
| No | 63 | 30 | 33 | 47.6% | ||
| Lymph node metastasis only | Yes | 18 | 14 | 4 | 77.7% | 0.002 |
| No | 53 | 19 | 34 | 35.8% |
| Characteristics | Detected | Responder | Non-Responder | ORR | p-Value | |
|---|---|---|---|---|---|---|
| PD-L1 CPS | ≥5 | 40 | 15 | 25 | 37.5% | 0.085 |
| <5 | 31 | 18 | 13 | 58.0% | ||
| HER-2+ | Yes | 5 | 4 | 1 | 80.0% | 0.119 |
| No | 66 | 29 | 37 | 43.9% | ||
| dMMR | Yes | 4 | 4 | 0 | 100.0% | 0.027 |
| No | 67 | 29 | 38 | 43.2% | ||
| EBV+ | Yes | 4 | 3 | 1 | 75.0% | 0.197 |
| No | 55 | 23 | 32 | 41.8% | ||
| TMB | ≥10 | 9 | 6 | 3 | 66.6% | 0.494 |
| <10 | 37 | 20 | 17 | 54.0% | ||
| TP53 mutation | Yes | 24 | 13 | 11 | 54.1% | 0.736 |
| No | 22 | 13 | 9 | 59.0% | ||
| PIK3CA mutation | Yes | 7 | 3 | 4 | 42.8% | 0.428 |
| No | 39 | 23 | 16 | 58.9% | ||
| CDH1 mutation | Yes | 13 | 6 | 7 | 46.1% | 0.373 |
| No | 33 | 20 | 13 | 60.6% | ||
| MET mutation | Yes | 3 | 1 | 2 | 33.3% | 0.402 |
| No | 43 | 25 | 18 | 58.1% | ||
| KRAS mutation | Yes | 4 | 2 | 2 | 50.0% | 0.783 |
| No | 42 | 24 | 18 | 57.1% | ||
| FGFR amplification | Yes | 2 | 1 | 1 | 50.0% | 0.849 |
| No | 44 | 25 | 19 | 56.8% | ||
| MYC amplification | Yes | 5 | 3 | 2 | 60.0% | 0.868 |
| No | 41 | 23 | 18 | 56.0% | ||
| ERBB2 amplification | Yes | 4 | 1 | 3 | 25.0% | 0.183 |
| No | 42 | 25 | 17 | 59.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Y.; Chen, N.; Huang, R.-Z.; Chen, D.-L. Comprehensive Analysis of Clinicopathological and Molecular Features to Predict Anti-PD-1-Based Therapy Efficacy in Patients with Advanced Gastric Signet Ring Cell Carcinoma. J. Pers. Med. 2023, 13, 115. https://doi.org/10.3390/jpm13010115
Hu Y, Chen N, Huang R-Z, Chen D-L. Comprehensive Analysis of Clinicopathological and Molecular Features to Predict Anti-PD-1-Based Therapy Efficacy in Patients with Advanced Gastric Signet Ring Cell Carcinoma. Journal of Personalized Medicine. 2023; 13(1):115. https://doi.org/10.3390/jpm13010115
Chicago/Turabian StyleHu, Yan, Nuo Chen, Ren-Ze Huang, and Dong-Liang Chen. 2023. "Comprehensive Analysis of Clinicopathological and Molecular Features to Predict Anti-PD-1-Based Therapy Efficacy in Patients with Advanced Gastric Signet Ring Cell Carcinoma" Journal of Personalized Medicine 13, no. 1: 115. https://doi.org/10.3390/jpm13010115