
Adequacy of Disease Control by Supraomohyoid Neck Dissection in cT1/T2 Tongue Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Selection
2.2. Diagnostic Work-Up, Treatment Policy, and Follow-Up
2.3. Survival Analysis
3. Results
3.1. Patients, Disease, and Treatment Characteristics
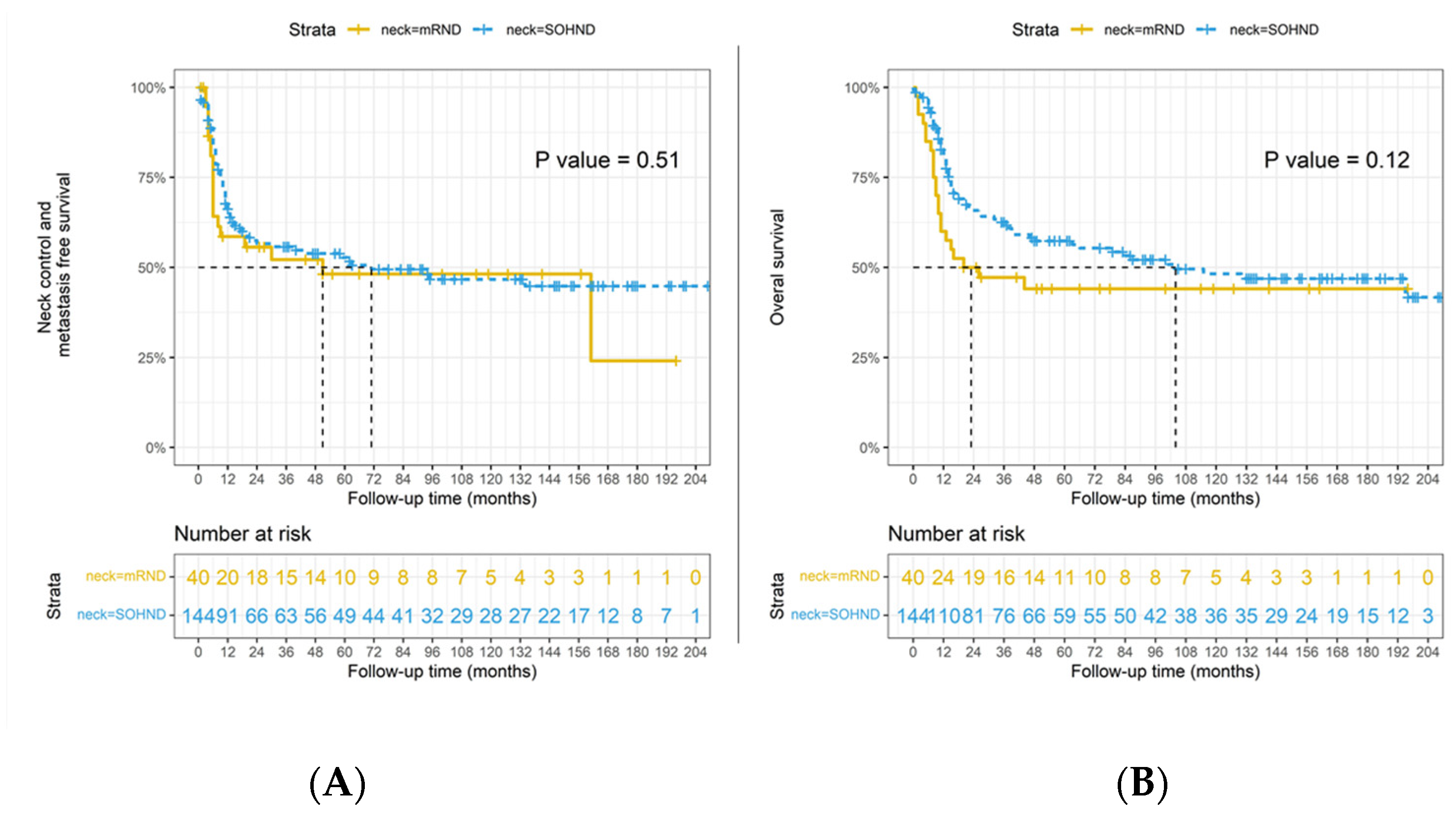
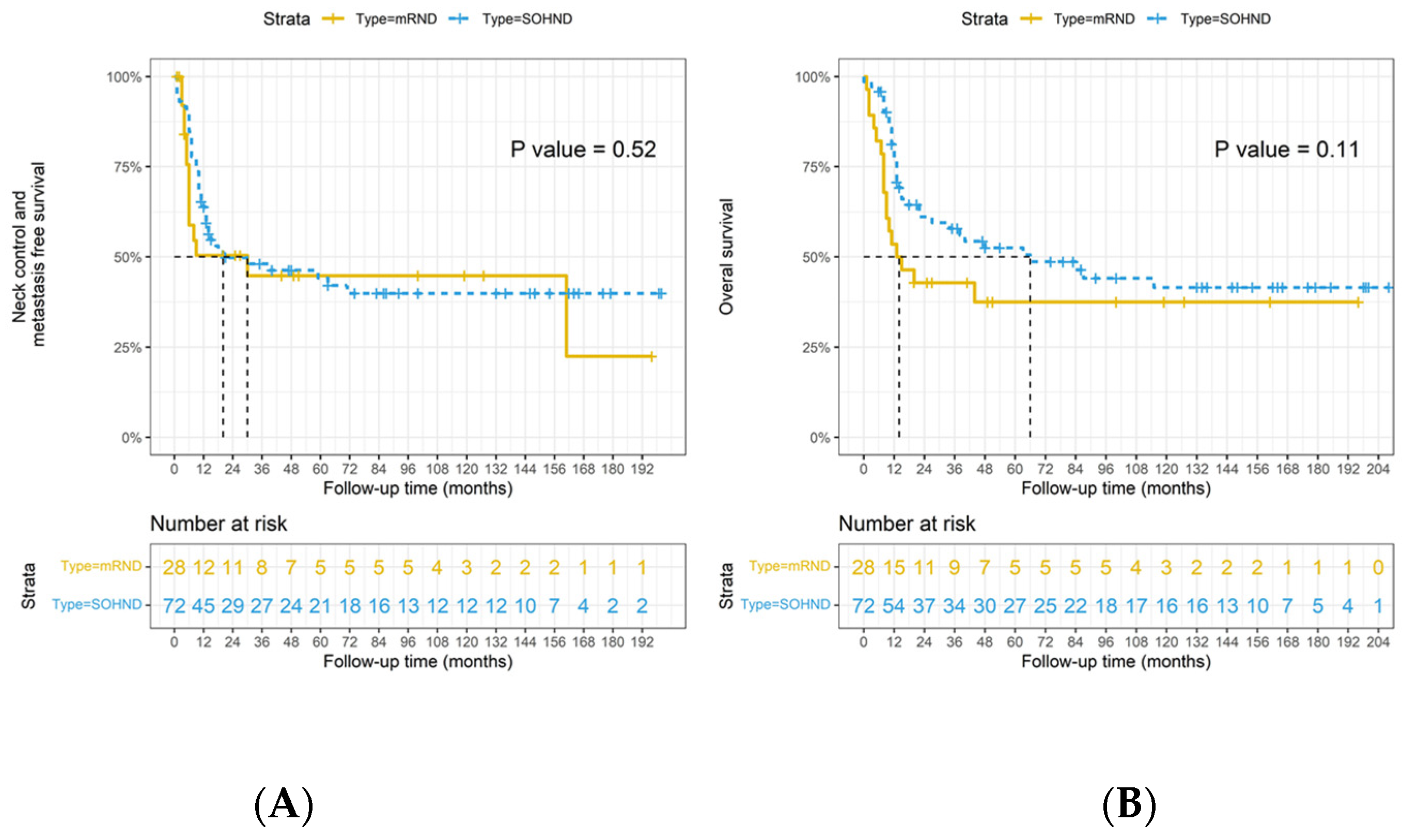
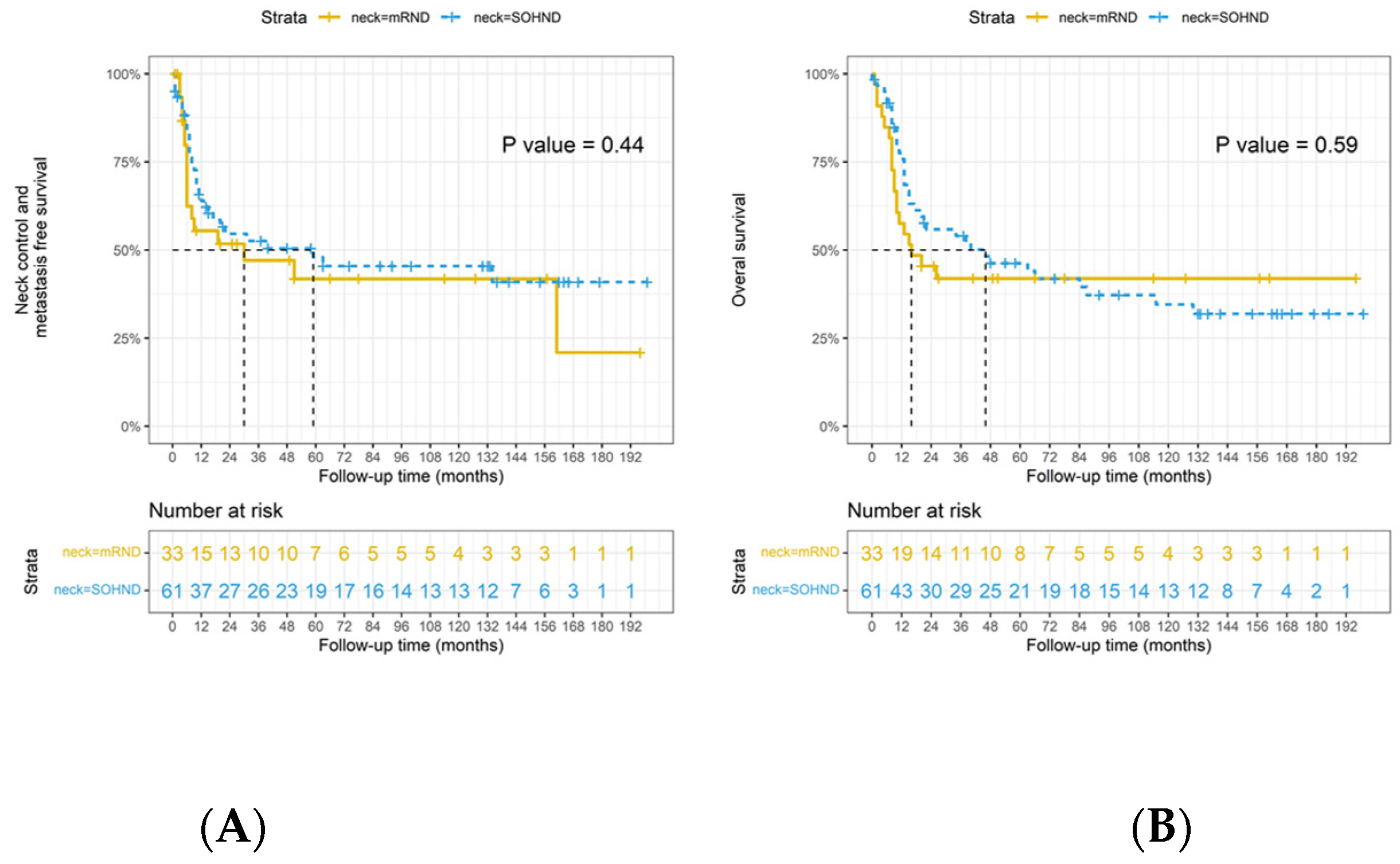
3.2. Survival Analysis by Type on Neck Dissection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, B.; Salama, A.M.; Valero, C.; Yuan, A.; Khimraj, A.; Saliba, M.; Zanoni, D.K.; Ganly, I.; Patel, S.G.; Katabi, N.; et al. The prognostic role of histologic grade, worst pattern of invasion, and tumor budding in early oral tongue squamous cell carcinoma: A comparative study. Virchows Arch. Int. J. Pathol. 2021, 47, 597–606. [Google Scholar] [CrossRef]
- Tsai, T.Y.; Iandelli, A.; Marchi, F.; Huang, Y.; Tai, S.F.; Hung, S.Y.; Kao, H.K.; Chang, K.P. The Prognostic Value of Lymph Node Burden in Oral Cavity Cancer: Systematic Review and Meta-Analysis. Laryngoscope 2021, 132, 88–95. [Google Scholar] [CrossRef]
- Zanoni, D.; Montero, P.; Migliacci, J.; Shah, J.; Ganly, I.; Patel, S.G. Survival outcomes after treatment of cancer of the oral cavity (1985–2015). Oral Oncol. 2020, 90, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, D.; Thankappan, K.; Battoo, A.J.; Rajapurkar, M.; Kuriakose, M.A.; Iyer, S. Isolated skip nodal metastasis is rare in T1 and T2 oral tongue squamous cell carcinoma. Otolaryngol. Head Neck Surg. Off. J. Am. Acad. Otolaryngol. Head Neck Surg. 2012, 147, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Henley, S.J.; Ward, E.M.; Scott, S.; Anderson, R.N.; Firth, A.U.; Thomas, C.C.; Islami, F.; Weir, H.K.; Lewis, D.R.; Sherman, R.L.; et al. Annual Report to the Nation on the Status of Cancer, Part I: National Cancer Statistics. Cancer 2020, 126, 2225–2249. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Forastiere, A.A. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin. Proc. 2016, 91, 386–396. [Google Scholar] [CrossRef]
- American Joint Committee on Cancer. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Lee, H.; Roh, J.L.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Number of positive lymph nodes better predicts survival for oral cavity cancer. J. Surg. Oncol. 2019, 119, 675–682. [Google Scholar] [CrossRef]
- Ebrahimi, A.; Gupta, R.; Luk, P.; Low, T.H.H.; McDowell, L.; Magarey, M.J.; Smith, P.N.; Perriman, D.M.; Schulte, K.M.; Veness, M.; et al. Number of nodal metastases and the American Joint Committee on cancer staging of head and neck cutaneous squamous cell carcinoma: A multicenter study. Oral Oncol. 2020, 111, 104855. [Google Scholar] [CrossRef] [PubMed]
- Subramaniam, N.; Balasubramanian, D.; Kumar, N.; Murthy, S.; Vijayan, S.N.; Nambiar, A.; Vidhyadharan, S.; Thankappan, K.; Iyer, S. Lymph node staging systems in oral squamous cell carcinoma: A comparative analysis. Oral Oncol. 2019, 97, 92–98. [Google Scholar] [CrossRef]
- Balasubramanian, D.; Vijayan, S.; Nambiar, A.; Mattavelli, D. Predictive nomograms for oral tongue squamous cell carcinoma applying the American Joint Committee on Cancer/Union Internationale Contre le Cancer 8th edition staging system. Head Neck 2021, 43, 1043–1055. [Google Scholar] [CrossRef]
- Mattavelli, D.; Ferrari, M.; Taboni, S.; Morello, R.; Paderno, A.; Rampinelli, V.; Del Bon, F.; Lombardi, D.; Grammatica, A.; Bossi, P.; et al. The 8th TNM classification for oral squamous cell carcinoma: What is gained, what is lost, and what is missing. Oral Oncol. 2020, 111, 104937. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Strong, E.; Spiro, R.H.; Vikram, B. Surgical grand rounds. Neck dissection: Current status and future possibilities. Clin. Bull. 1981, 11, 25–33. [Google Scholar] [PubMed]
- Satgunaseelan, L.; Allanson, B.M.; Asher, R.; Reddy, R.; Low, H.T.; Veness, M.; Iyer, N.G.; Smee, R.I.; Palme, C.E.; Gupta, R.; et al. The incidence of squamous cell carcinoma of the oral tongue is rising in young non-smoking women: An international multi-institutional analysis. Oral Oncol. 2020, 110, 104875. [Google Scholar] [CrossRef]
- Lindberg, R. Distribution of cervical lymph node metastases from squamous cell carcinoma of the upper respiratory and digestive tracts. Cancer 1972, 29, 1446–1449. [Google Scholar] [CrossRef]
- Choi, K.Y.; Park, S.C.; Kim, J.H.; Lee, D.J. The occult nodal metastasis rate of early tongue cancer (T1-T2): A protocol for a systematic review and meta-analysis. Medicine 2021, 100, e24327. [Google Scholar] [CrossRef]
- Chatterjee, D.; Bansal, V.; Malik, V.; Bhagat, R.; Punia, R.S.; Handa, U. Tumor Budding and Worse Pattern of Invasion Can Predict Nodal Metastasis in Oral Cancers and Associated with Poor Survival in Early-Stage Tumors. Ear Nose Throat J. 2019, 98, E112–E119. [Google Scholar] [CrossRef]
- Ahlberg, A.; Nikolaidis, P.; Engström, T.; Gunnarsson, K.; Johansson, H.; Sharp, L.; Laurell, G. Morbidity of supraomohyoidal and modified radical neck dissection combined with radiotherapy for head and neck cancer: A prospective longitudinal study. Head Neck 2012, 34, 66–72. [Google Scholar] [CrossRef]
- Popescu, B.; Berteşteanu, S.V.G.; Grigore, R.; Scăunaşu, R.; Popescu, C.R. Functional implications of radical neck dissection and the impact on the quality of life for patients with head and neck neoplasia. J. Med. Life 2012, 5, 410–413. [Google Scholar]
- Terrell, J.E.; Welsh, D.E.; Bradford, C.R.; Chepeha, D.B.; Esclamado, R.M.; Hogikyan, N.D.; Wolf, G.T. Pain, quality of life, and spinal accessory nerve status after neck dissection. Laryngoscope 2000, 110, 620–626. [Google Scholar] [CrossRef]
- Huang, S.F.; Kang, C.J.; Lin, C.Y.; Fan, K.H.; Yen, T.C.; Wang, H.M.; Chen, I.H.; Liao, C.T.; Cheng, A.J.; Chang, J.T.C. Neck treatment of patients with early stage oral tongue cancer: Comparison between observation, supraomohyoid dissection, and extended dissection. Cancer 2008, 112, 1066–1075. [Google Scholar] [CrossRef]
- Flach, G.B.; Tenhagen, M.; de Bree, R.; Brakenhoff, R.H.; van der Waal, I.; Bloemena, E.; Kuik, D.J.; Castelijns, J.A.; Leemans, C.R. Outcome of patients with early stage oral cancer managed by an observation strategy towards the N0 neck using ultrasound guided fine needle aspiration cytology: No survival difference as compared to elective neck dissection. Oral Oncol. 2013, 49, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, L.P.; Sanabria, A. Elective neck dissection in oral carcinoma: A critical review of the evidence. Acta Otorhinolaryngol. Ital. 2007, 27, 113–117. [Google Scholar] [PubMed]
- Kowalski, L.P.; Carvalho, A.L. Feasibility of supraomohyoid neck dissection in N1 and N2a oral cancer patients. Head Neck 2002, 24, 921–924. [Google Scholar] [CrossRef] [PubMed]
- Andersen, P.E.; Warren, F.; Spiro, J.; Burningham, A.; Wong, R.; Wax, M.K.; Shah, J.P.; Cohen, J.I. Results of selective neck dissection in management of the node-positive neck. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 1180–1184. [Google Scholar] [CrossRef]
- Patel, R.S.; Clark, J.R.; Gao, K.; O’Brien, C.J. Effectiveness of selective neck dissection in the treatment of the clinically positive neck. Head Neck 2008, 30, 1231–1236. [Google Scholar] [CrossRef]
- Byers, R.M.; Weber, R.S.; Andrews, T.; McGill, D.; Kare, R.; Wolf, P. Frequency and therapeutic implications of “skip metastases” in the neck from squamous carcinoma of the oral tongue. Head Neck 1997, 19, 14–19. [Google Scholar] [CrossRef]
- Lin, C.Y.; Fan, K.H.; Lee, L.Y.; Hsueh, C.; Yang, L.Y.; Ng, S.H.; Wang, H.M.; Hsieh, C.H.; Lin, C.H.; Tsao, C.K.; et al. Precision Adjuvant Therapy Based on Detailed Pathologic Risk Factors for Resected Oral Cavity Squamous Cell Carcinoma: Long-Term Outcome Comparison of CGMH and NCCN Guidelines. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 916–925. [Google Scholar] [CrossRef]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- R Core Team. The R Project for Statistical Computing. 2021. Available online: https://www.R-project.org/ (accessed on 27 August 2022).
- Therneau, T.M. A Package for Survival Analysis in R. R Package Version 3.4-0. 2022. Available online: https://CRAN.R-project.org/package=survival (accessed on 27 August 2022).
- Therneau, T.M.; Grambsch, P.M. Modeling Survival Data: Extending the Cox Model, 1st ed.; Springer: New York, NY, USA, 2000. [Google Scholar] [CrossRef]
- Kassambra, A.; Kosinski, M.; Biecek, P.; Fabian, S. Drawing Survival Curves Using “ggplot2”. R Package Version 0.4.9. 2021. Available online: https://CRAN.R-project.org/package=survminer (accessed on 27 August 2022).
- de Bree, R.; van den Brekel, M.W.M. Elective neck dissection versus observation in the clinically node negative neck in early oral cancer: Do we have the answer yet? Oral Oncol. 2015, 51, 963–965. [Google Scholar] [CrossRef]
- Ferlito, A.; Rinaldo, A.; Silver, C.E.; Shah, J.P.; Suárez, C.; Medina, J.E.; Kowalski, L.P.; Johnson, J.T.; Strome, M.; Rodrigo, J.P.; et al. Neck dissection: Then and now. Auris Nasus Larynx 2006, 33, 365–374. [Google Scholar] [CrossRef]
- Ewing, M.; Martin, H. Disability following radical neck dissection; an assessment based on the postoperative evaluation of 100 patients. Cancer 1952, 5, 873–883. [Google Scholar] [CrossRef]
- Gane, E.M.; Michaleff, Z.A.; Cottrell, M.A.; McPhail, S.M.; Hatton, A.L.; Panizza, B.J.; O’Leary, S.P. Prevalence, incidence, and risk factors for shoulder and neck dysfunction after neck dissection: A systematic review. Eur. J. Surg. Oncol. 2017, 43, 1199–1218. [Google Scholar] [CrossRef] [PubMed]
- Ferlito, A.; Rinaldo, A. Osvaldo Suárez: Often-forgotten father of functional neck dissection (in the non-Spanish-speaking literature). Laryngoscope 2004, 114, 1177–1178. [Google Scholar] [CrossRef] [PubMed]
- Gavilán, C.; Gavilán, J. Five-year results of functional neck dissection for cancer of the larynx. Arch. Otolaryngol. Head Neck Surg. 1989, 115, 1193–1196. [Google Scholar] [CrossRef] [PubMed]
- Bocca, E.; Pignataro, O.; Oldini, C.; Cappa, C. Functional neck dissection: An evaluation and review of 843 cases. Laryngoscope 1984, 94, 942–945. [Google Scholar] [CrossRef]
- Nibu, K.I.; Ebihara, Y.; Ebihara, M.; Kawabata, K.; Onitsuka, T.; Fujii, T.; Saikawa, M. Quality of life after neck dissection: A multicenter longitudinal study by the Japanese Clinical Study Group on Standardization of Treatment for Lymph Node Metastasis of Head and Neck Cancer. Int. J. Clin. Oncol. 2010, 15, 33–38. [Google Scholar] [CrossRef]
- D’Cruz, A.K.; Vaish, R.; Kapre, N.; Dandekar, M.; Gupta, S.; Hawaldar, R.; Agarwal, J.P.; Pantvaidya, G.; Chaukar, D.; Deshmukh, A.; et al. Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer. N. Engl. J. Med. 2015, 373, 521–529. [Google Scholar] [CrossRef]
- Iype, E.M.; Sebastian, P.; Mathew, A.; Balagopal, P.G.; Varghese, B.T.; Thomas, S. The role of selective neck dissection (I-III) in the treatment of node negative (N0) neck in oral cancer. Oral Oncol. 2008, 44, 1134–1138. [Google Scholar] [CrossRef]
- Abu-Ghanem, S.; Yehuda, M.; Carmel, N.N.; Leshno, M.; Abergel, A.; Gutfeld, O.; Fliss, D.M. Elective Neck Dissection vs Observation in Early-Stage Squamous Cell Carcinoma of the Oral Tongue With No Clinically Apparent Lymph Node Metastasis in the Neck: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 857–865. [Google Scholar] [CrossRef]
- Kolli, V.R.; Datta, R.V.; Orner, J.B.; Hicks, W.L.; Loree, T.R. The role of supraomohyoid neck dissection in patients with positive nodes. Arch. Otolaryngol. Head Neck Surg. 2000, 126, 413–416. [Google Scholar] [CrossRef] [Green Version]
- Byers, R.M. Modified neck dissection. A study of 967 cases from 1970 to 1980. Am. J. Surg. 1985, 150, 414–421. [Google Scholar] [CrossRef]
- Byers, R.M.; Wolf, P.F.; Ballantyne, A.J. Rationale for elective modified neck dissection. Head Neck Surg. 1988, 10, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.C.; Koo, B.S.; Lee, J.S.; Choi, E.C. Level V lymph node dissection in oral and oropharyngeal carcinoma patients with clinically node-positive neck: Is it absolutely necessary? Laryngoscope 2006, 116, 1232–1235. [Google Scholar] [CrossRef] [PubMed]
- Jayasuriya, N.S.S.; Mannapperuma, N.T.; Siriwardana, S.; Attygalla, A.M.; DeSilva, S.; Jinadasa, H.; Ekanayaka, R.; Dias, D.K.; Wadusinghearachi, S.; Perera, I. Incidence of metastasis to level V lymph nodes in clinically positive necks among Sri Lankan patients with oral squamous cell carcinoma. Br. J. Oral Maxillofac. Surg. 2021, 59, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Battoo, A.J.; Hedne, N.; Ahmad, S.Z.; Thankappan, K.; Iyer, S.; Kuriakose, M.A. Selective neck dissection is effective in N1/N2 nodal stage oral cavity squamous cell carcinoma. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2013, 71, 636–643. [Google Scholar] [CrossRef]
- Subramaniam, N.; Balasubramanian, D.; Murthy, S.; Thankappan, K.; Iyer, S. European Journal of Surgical Oncology Predictors of loco-regional control in stage I/II oral squamous cell carcinoma classi fi ed by AJCC 8th edition. Eur. J. Surg. Oncol. 2019, 45, 2126–2130. [Google Scholar] [CrossRef]
- Larson, A.R.; Kemmer, J.; Formeister, E.; El-Sayed, I.; Ha, P.; George, J.; Ryan, W.; Chan, E.; Heaton, C. Beyond Depth of Invasion: Adverse Pathologic Tumor Features in Early Oral Tongue Squamous Cell Carcinoma. Laryngoscope 2020, 130, 1715–1720. [Google Scholar] [CrossRef]
- Ho, A.S.; Kim, S.; Tighiouart, M.; Gudino, C.; Mita, A.; Scher, K.S.; Laury, A.; Prasad, R.; Shiao, S.L.; Van Eyk, J.E.; et al. Metastatic lymph node burden and survival in oral cavity cancer. J. Clin. Oncol. 2017, 35, 3601–3609. [Google Scholar] [CrossRef]
- Choi, Y.; Bin-Manie, M.; Roh, J.L.; Cho, K.J.; Lee, Y.S.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Metastatic lymph node burden predictive of survival in patients undergoing primary surgery for laryngeal and hypopharyngeal cancer. J. Cancer Res. Clin. Oncol. 2019, 145, 2565–2572. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | (%) | pN0 | (%) | pN+ | (%) | p | |
|---|---|---|---|---|---|---|---|---|
| cT stage | T1 | 256 | 45.3 | 215 | 56.4 | 41 | 22.3 | <0.001 |
| T2 | 309 | 54.7 | 151 | 43.6 | 107 | 77.7 | ||
| cN stage | N0 | 381 | 67.4 | - | - | - | - | - |
| N1 | 84 | 14.9 | - | - | - | - | - | |
| N2b | 90 | 15.9 | - | - | - | - | - | |
| N2c | 10 | 1.8 | - | - | - | - | - | |
| pT stage | T1 | 175 | 31.0 | 158 | 41. | 17 | 9.2 | <0.001 |
| T2 | 199 | 35.2 | 139 | 36.5 | 60 | 32.6 | ||
| T3 | 191 | 33.8 | 84 | 22.0 | 107 | 58.2 | ||
| pN stage | N0 | 381 | 67.4 | - | - | - | - | - |
| N1 | 59 | 10.4 | - | - | - | - | - | |
| N2b | 30 | 5.3 | - | - | - | - | - | |
| N2c | 1 | 0.2 | - | - | - | - | - | |
| N3b | 94 | 16.6 | - | - | - | - | - | |
| Grading | Well | 177 | 31.3 | 141 | 37.0 | 36 | 19.6 | <0.001 |
| Moderate | 331 | 58.6 | 215 | 56.4 | 116 | 63.0 | ||
| Poor | 57 | 10.1 | 25 | 6.6 | 32 | 17.4 | ||
| PNI | No | 388 | 68.7 | 290 | 76.1 | 98 | 53.3 | <0.001 |
| Yes | 177 | 31.3 | 91 | 23.9 | 86 | 46.7 | ||
| VI | No | - | - | - | - | - | - | - |
| Yes | - | - | - | - | - | - | - | |
| LI | No | 541 | 95.8 | 377 | 99.0 | 164 | 89.1 | <0.001 |
| yes | 24 | 4.2 | 4 | 1.0 | 20 | 10.9 | ||
| AJCC 7th Ed. pN Status | SOHND (%) | mRND (%) | AJCC 8th Ed. pN Status | SOHND (%) | mRND (%) | p | |
|---|---|---|---|---|---|---|---|
| pN0 | 381 (67.4) | 357 (71.3) | 24 (37.5) | 381 (67.4) | 357 (71.3) | 24 (37.5) | <0.001 |
| pN1 | 84 (14.9) | 72 (14.4) | 12 (18.8) | 59 (10.4) | 55 (11.0) | 4 (6.2) | |
| pN2a | 25 (4.4) | 17 (3.4) | 8 (12.5) | ||||
| pN2b | 90 (15.9) | 66 (13.2) | 24 (37.5) | 30 (5.3) | 27 (5.4) | 3 (4.7) | |
| pN2c | 10 (1.8) | 6 (1.2) | 4 (6.3) | 1 (0.2) | 1 (0.2) | 0 (0.0) | |
| pN3b | 69 (12.2) | 44 (8.8) | 25 (36.2) | ||||
| Total | 501 (100.0) | 64 (100.0) | 501 (100.0) | 64 (100.0) |
| All | SOHND (%) | mRND (%) | p | |
|---|---|---|---|---|
| ENE− | 31 | 28 (38.90) | 3 (10.70) | <0.001 |
| ENE+ | 69 | 44 (61.10) | 25 (89.30) | |
| Total | 100 | 72 | 28 |
| DFS | OS | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | HR (95% C.I.) | p | HR (95% C.I.) | p | HR (95% C.I.) | p | HR (95% C.I.) | p |
| Age | ||||||||
| <50 years old | Ref | 0.037 | Ref | Ref | ||||
| ≥50 years old | 0.735 (0.550–0.982) | 0.737 (0.548–0.991) | 0.043 | 0.984 (0.715–1.354) | 0.921 | |||
| Primary tumor status | ||||||||
| pT1 | Ref | Ref | - | Ref | Ref | - | ||
| pT2 | 1.489 (1.018–2.179) | 0.040 | 1.144 (0.766–1.707) | 0.511 | 2.862 (1.696–4.829) | <0.001 | 2.245 (1.310–3.848) | 0.003 |
| pT3 | 2.261 (1.569–3.258) | <0.001 | 1.417 (0.933–2.151) | 0.102 | 5.032 (3.052–8.298) | <0.001 | 2.910 (1.691–5.007) | <0.001 |
| Lymph node metastasis | ||||||||
| pN (−) ENE(−) | Ref | Ref | - | Ref | Ref | - | ||
| pN (+) ENE(−) | 2.045(1.420–2.945) | <0.001 | 1.603 (1.085–2.369) | 0.018 | 2.632(1.732–4.000) | <0.001 | 2.001 (1.294–3.094) | <0.001 |
| pN (+) ENE(+) | 2.743(1.947–3.865) | <0.001 | 2.034 (1.381–2.995) | <0.001 | 5.491(3.828–7.876) | <0.001 | 3.756 (2.510–5.622) | <0.001 |
| Type of neck dissection | ||||||||
| SOHND | Ref | Ref | - | Ref | Ref | - | ||
| mRND | 1.624(1.094–2.411) | 0.016 | 1.188 (0.783–1.802) | 0.418 | 2.471 (1.673–3.649) | <0.001 | 1.348 (0.887–2.048) | 0.162 |
| Tumor cell differentiation | ||||||||
| Well/Moderate | Ref | - | Ref | |||||
| Poor | 1.683 (1.113–2.545) | 0.014 | 1.275 (0.824–1.973) | 0.275 | 1.212 (0.722–2.034) | 0.468 | ||
| PNI | ||||||||
| No | Ref | <0.001 | Ref | - | Ref | Ref | ||
| Yes | 1.816(1.363–2.419) | 1.398 (1.023–1.910) | 0.035 | 1.644 (1.190–2.271) | 0.003 | 1.006 (0.714–1.417) | 0.972 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iandelli, A.; Marchi, F.; Chen, A.-C.; Young, C.-K.; Liao, C.-T.; Tsao, C.-K.; Kang, C.-J.; Wang, H.-M.; Chang, T.-C.J.; Huang, S.-F. Adequacy of Disease Control by Supraomohyoid Neck Dissection in cT1/T2 Tongue Cancer. J. Pers. Med. 2022, 12, 1535. https://doi.org/10.3390/jpm12091535
Iandelli A, Marchi F, Chen A-C, Young C-K, Liao C-T, Tsao C-K, Kang C-J, Wang H-M, Chang T-CJ, Huang S-F. Adequacy of Disease Control by Supraomohyoid Neck Dissection in cT1/T2 Tongue Cancer. Journal of Personalized Medicine. 2022; 12(9):1535. https://doi.org/10.3390/jpm12091535
Chicago/Turabian StyleIandelli, Andrea, Filippo Marchi, An-Chieh Chen, Chi-Kuan Young, Chun-Ta Liao, Chung-Kan Tsao, Chung-Jan Kang, Hung-Ming Wang, Tung-Chieh Joseph Chang, and Shiang-Fu Huang. 2022. "Adequacy of Disease Control by Supraomohyoid Neck Dissection in cT1/T2 Tongue Cancer" Journal of Personalized Medicine 12, no. 9: 1535. https://doi.org/10.3390/jpm12091535