
Surgery for T4 Colorectal Cancer in Older Patients: Determinants of Outcomes
 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Patients and Methods
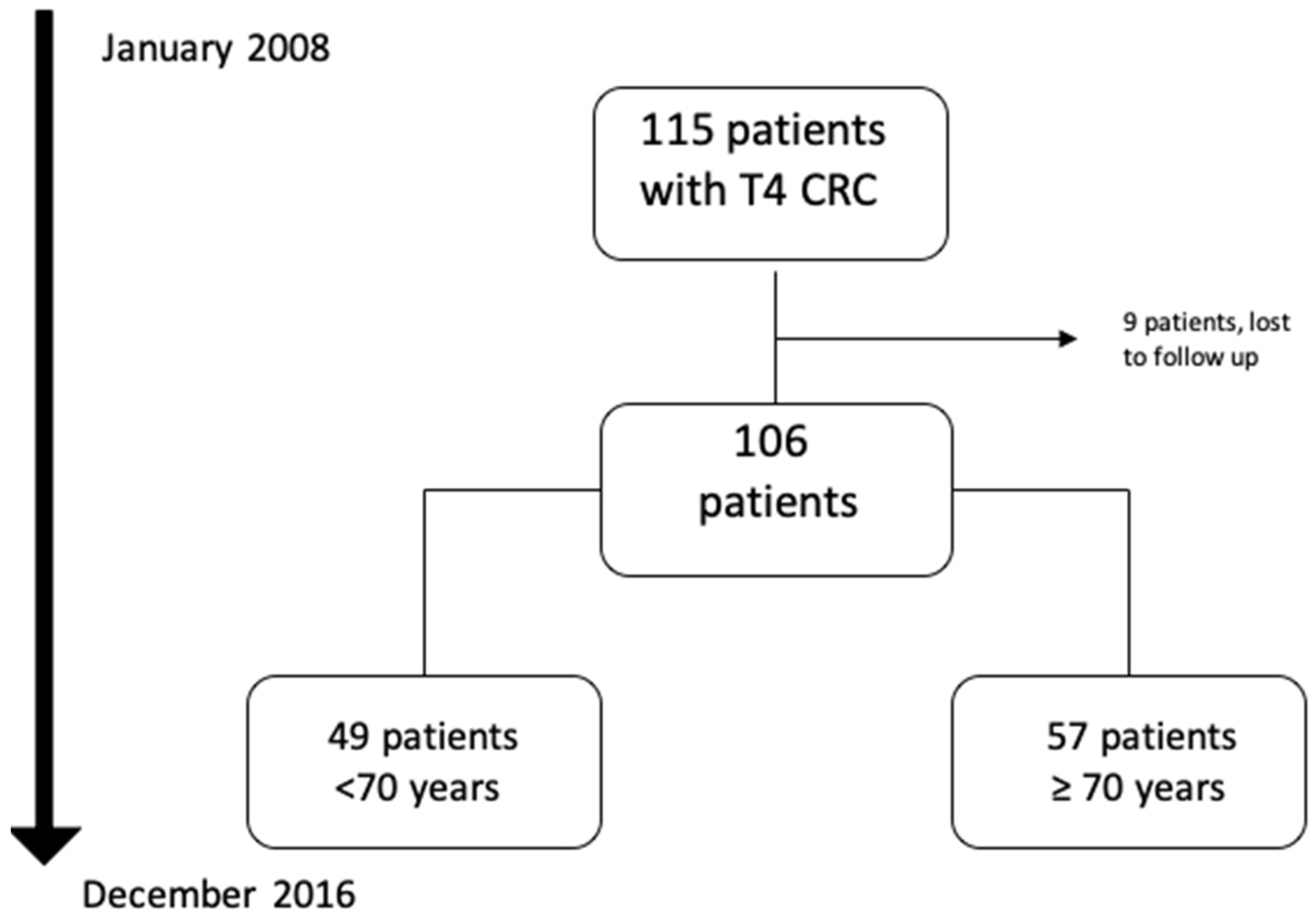
2.1. Patients and Data Collection
2.2. Investigations and Treatment Strategies
2.3. Follow-Up
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Itatani, Y.; Kawada, K.; Sakai, Y. Treatment of Elderly Patients with Colorectal Cancer. BioMed Res. Int. 2018, 2018, 2176056. [Google Scholar] [CrossRef]
- Adeleke, S.; Haslam, A.; Choy, A.; Diaz-Cano, S.; Galante, J.R.; Mikropoulos, C.; Boussios, S. Microsatellite instability testing in colorectal patients with Lynch syndrome: Lessons learned from a case report and how to avoid such pitfalls. Pers. Med. 2022, 19, 277–286. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Ueno, H.; Mochizuki, H.; Akagi, Y.; Kusumi, T.; Yamada, K.; Ikegami, M.; Kawachi, H.; Kameoka, S.; Ohkura, Y.; Masaki, T.; et al. Optimal colorectal cancer staging criteria in TNM classification. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1519–1526. [Google Scholar] [CrossRef]
- Gao, P.; Song, Y.; Wang, Z.; Xu, Y.; Tong, L.; Sun, J.; Yu, M.; Xu, H. Is the prediction of prognosis not improved by the seventh edition of the TNM classification for colorectal cancer? Analysis of the surveillance, epidemiology, and end results (SEER) database. BMC Cancer 2013, 13, 123. [Google Scholar] [CrossRef]
- Aapro, M.S.; Köhne, C.-H.; Cohen, H.J.; Extermann, M. Never too old? Age should not be a barrier to enrollment in cancer clinical trials. Oncologist 2005, 10, 198–204. [Google Scholar] [CrossRef]
- Townsley, C.; Pond, G.R.; Peloza, B.; Kok, J.; Naidoo, K.; Dale, D.; Herbert, C.; Holowaty, E.; Straus, S.; Siu, L.L. Analysis of treatment practices for elderly cancer patients in Ontario, Canada. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 3802–3810. [Google Scholar] [CrossRef]
- Colorectal Cancer Collaborative Group. Surgery for colorectal cancer in elderly patients: A systematic review. Lancet 2000, 356, 968–974. [Google Scholar] [CrossRef]
- Blood Pressure Lowering Treatment Trialists’ Collaboration; Ying, A.; Arima, H.; Czernichow, S.; Woodward, M.; Huxley, R.; Turnbull, F.; Perkovic, V.; Neal, B. Effects of blood pressure lowering on cardiovascular risk according to baseline body-mass index: A meta-analysis of randomised trials. Lancet 2015, 385, 867–874. [Google Scholar] [CrossRef]
- Eveno, C.; Lefevre, J.H.; Svrcek, M.; Bennis, M.; Chafai, N.; Tiret, E.; Parc, Y. Oncologic results after multivisceral resection of clinical T4 tumors. Surgery 2014, 156, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, G.; Cherqui, D.; Geller, D.A.; Buell, J.F.; Kaneko, H.; Han, H.S.; Asbun, H.; O’Rourke, N.; Tanabe, M.; Koffron, A.J.; et al. Recommendations for laparoscopic liver resection: A report from the second international consensus conference held in Morioka. Ann. Surg. 2015, 261, 619–629. [Google Scholar] [CrossRef]
- Papamichael, D.; Audisio, R.A.; Glimelius, B.; de Gramont, A.; Glynne-Jones, R.; Haller, D.; Köhne, C.-H.; Rostoft, S.; Lemmens, V.; Mitry, E.; et al. Treatment of colorectal cancer in older patients: International Society of Geriatric Oncology (SIOG) consensus recommendations 2013. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 463–476. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D.; ESMO Guidelines Working Group. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2014, 25 (Suppl. 3), iii1–iii9. [Google Scholar] [CrossRef]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Rahbari, N.N.; Weitz, J.; Hohenberger, W.; Heald, R.J.; Moran, B.; Ulrich, A.; Holm, T.; Wong, W.D.; Tiret, E.; Moriya, Y.; et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the International Study Group of Rectal Cancer. Surgery 2010, 147, 339–351. [Google Scholar] [CrossRef]
- Slankamenac, K.; Graf, R.; Barkun, J.; Puhan, M.A.; Clavien, P.-A. The comprehensive complication index: A novel continuous scale to measure surgical morbidity. Ann. Surg. 2013, 258, 1–7. [Google Scholar] [CrossRef]
- Pohar, M.; Stare, J. Making relative survival analysis relatively easy. Comput. Biol. Med. 2007, 37, 1741–1749. [Google Scholar] [CrossRef]
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D.; ESMO Guidelines Committee. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- Biondi, A.; Vacante, M.; Ambrosino, I.; Cristaldi, E.; Pietrapertosa, G.; Basile, F. Role of surgery for colorectal cancer in the elderly. World J. Gastrointest. Surg. 2016, 8, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Parent, P.; Cohen, R.; Rassy, E.; Svrcek, M.; Taieb, J.; André, T.; Turpin, A. A comprehensive overview of promising biomarkers in stage II colorectal cancer. Cancer Treat. Rev. 2020, 88, 102059. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Ozturk, M.A.; Moschetta, M.; Karathanasi, A.; Zakynthinakis-Kyriakou, N.; Katsanos, K.H.; Christodoulou, D.K.; Pavlidis, N. The Developing Story of Predictive Biomarkers in Colorectal Cancer. J. Pers. Med. 2019, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.H.; Johnson, D.S.; Hemmings, D.; Hsu, A.; Imai, T.; Tominaga, G.T. Assessing the quality of colorectal cancer staging: Documenting the process in improving the staging of node-negative colorectal cancer. Arch. Surg. 2005, 140, 881–886; discussion 886–887. [Google Scholar] [CrossRef]
- Takano, S.; Kato, J.; Yamamoto, H.; Shiode, J.; Nasu, J.; Kawamoto, H.; Okada, H.; Shiratori, Y. Identification of risk factors for lymph node metastasis of colorectal cancer. Hepatogastroenterology 2007, 54, 746–750. [Google Scholar]
- Grossmann, I.; Klaase, J.M.; Avenarius, J.K.; de Hingh, I.H.; Mastboom, W.J.; Wiggers, T. The strengths and limitations of routine staging before treatment with abdominal CT in colorectal cancer. BMC Cancer 2011, 11, 433. [Google Scholar] [CrossRef]
- Gezen, C.; Kement, M.; Altuntas, Y.E.; Okkabaz, N.; Seker, M.; Vural, S.; Gumus, M.; Oncel, M. Results after multivisceral resections of locally advanced colorectal cancers: An analysis on clinical and pathological t4 tumors. World J. Surg. Oncol. 2012, 10, 39. [Google Scholar] [CrossRef]
- Engelmann, B.E.; Loft, A.; Kjær, A.; Nielsen, H.J.; Berthelsen, A.K.; Binderup, T.; Brinch, K.; Brünner, N.; Gerds, T.A.; Høyer-Hansen, G.; et al. Positron emission tomography/computed tomography for optimized colon cancer staging and follow up. Scand. J. Gastroenterol. 2014, 49, 191–201. [Google Scholar] [CrossRef]
- Rosati, G.; Lonardi, S.; Galli, F.; Di Bartolomeo, M.; Ronzoni, M.; Zampino, M.G.; Banzi, M.; Zaniboni, A.; Pasini, F.; Bozzarelli, S.; et al. Oxaliplatin plus fluoropyrimidines as adjuvant therapy for colon cancer in older patients: A subgroup analysis from the TOSCA trial. Eur. J. Cancer 2021, 148, 190–201. [Google Scholar] [CrossRef]
- Seishima, R.; Okabayashi, K.; Hasegawa, H.; Tsuruta, M.; Shigeta, K.; Matsui, S.; Yamada, T.; Kitagawa, Y. Is laparoscopic colorectal surgery beneficial for elderly patients? A systematic review and meta-analysis. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2015, 19, 756–765. [Google Scholar] [CrossRef]
- Peltrini, R.; Imperatore, N.; Carannante, F.; Cuccurullo, D.; Capolupo, G.T.; Bracale, U.; Caricato, M.; Corcione, F. Age and comorbidities do not affect short-term outcomes after laparoscopic rectal cancer resection in elderly patients. A multi-institutional cohort study in 287 patients. Updates Surg. 2021, 73, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Kiran, R.P.; Pokala, N.; Dudrick, S.J. Long-term outcome after operative intervention for rectal cancer in patients aged over 80 years: Analysis of 9,501 patients. Dis. Colon Rectum 2007, 50, 604–610. [Google Scholar] [CrossRef]
- Devon, K.M.; Vergara-Fernandez, O.; Victor, J.C.; McLeod, R.S. Colorectal cancer surgery in elderly patients: Presentation, treatment, and outcomes. Dis. Colon Rectum 2009, 52, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Yap, R.; Oliva, K.; Wilkins, S.; McMurrick, P.J. Colorectal Cancer Surgery in the Very Elderly: Nonagenarians. Dis. Colon Rectum 2016, 59, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Lund, C.M.; Vistisen, K.K.; Dehlendorff, C.; Rønholt, F.; Johansen, J.S.; Nielsen, D.L. The effect of geriatric intervention in frail elderly patients receiving chemotherapy for colorectal cancer: A randomized trial (GERICO). BMC Cancer 2017, 17, 448. [Google Scholar] [CrossRef]
- Eamer, G.; Taheri, A.; Chen, S.S.; Daviduck, Q.; Chambers, T.; Shi, X.; Khadaroo, R.G. Comprehensive geriatric assessment for older people admitted to a surgical service. Cochrane Database Syst. Rev. 2018, 1, CD012485. [Google Scholar] [CrossRef] [PubMed]
- Saripella, A.; Wasef, S.; Nagappa, M.; Riazi, S.; Englesakis, M.; Wong, J.; Chung, F. Effects of comprehensive geriatric care models on postoperative outcomes in geriatric surgical patients: A systematic review and meta-analysis. BMC Anesthesiol. 2021, 21, 127. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Baseline Characteristics | Total n = 106 | Patients Aged 50–69 Years N = 49 (46.2%) | Patients Aged ≥ 70 Years N = 57 (53.8%) | p-Value | |
|---|---|---|---|---|---|
| Age (years) | Median | 71.5 | 58 | 80 | <0.001 |
| IQR | 21 | 9 | 11 | ||
| Gender | Male | 44 (41.5) | 30 (28.3) | 14 (13.2) | <0.001 |
| Female | 62 (58.5) | 19 (17.9) | 43 (40.5) | ||
| American Society of Anaesthesiologists score | <2 | 78 (73.6) | 39 (36.7) | 39 (36.7) | 0.193 |
| ≥3 | 28 (26.4) | 10 (9.4) | 18 (16.9) | ||
| Comorbidities | Cardiovascular | 42 (39.6) | 14 (13.2) | 28 (26.4) | 0.031 |
| Pulmonary | 16 (15.1) | 6 (5.6) | 10 (9.4) | 0.447 | |
| Diabetes | 19 (17.9) | 7 (6.6) | 12 (11.3) | 0.365 | |
| Localization | Rectum | 19 (17.9) | 10 (9.4) | 9 (8.4) | 0.536 |
| Colon | 87 (82.1) | 39 (36.7) | 48 (45.2) | ||
| Specified localization | Rectum | 19 (17.9) | 10 (9.4) | 9 (8.4) | 0.296 |
| Right colon | 39 (36.4) | 17 (16) | 22 (20.7) | ||
| Transverse colon | 7(6.2) | 3 (2.8) | 4 (3.7) | ||
| Left colon | 42(39.5) | 21(19.8) | 21(19.8) | ||
| Lymph node | N+ | 57(53.7) | 25(23.5) | 32(30.1) | 0.389 |
| N− | 46(46.3) | 25(23.5) | 21(19.8) | ||
| Synchronous metastasis | Stage IVA (liver only) | 18 (16.9) | 10 (9.4) | 8 (7.5) | 0.383 |
| Stage IVA (lung only) | 4 (3.7) | 3 (2.8) | 1 (0.9) | 0.334 | |
| Stage IVB | 5 (4.7) | 4 (3.7) | 1 (0.9) | 0.179 | |
| Serum carcinoembryonic antigen (µ/L) | Median | 8.5 | 7 | 12 | <0.001 |
| IQR | 29 | 29 | 29 | ||
| Treatment Modality | Total n = 106 | Patients Aged 50–69 Years N = 49 (46.2%) | Patients Aged ≥ 70 Years N = 57 (53.8%) | p-Value | |
|---|---|---|---|---|---|
| Neoadjuvant radiotherapy or chemotherapy | 17 (16.1) | 9 (8.5) | 8 (7.5) | 0.546 | |
| Operative setting | Elective surgery | 85 (80.2) | 40 (37.7) | 45 (42.4) | 0.729 |
| Urgent surgery | 21 (19.8) | 9 (8.5) | 12 (11.3) | ||
| Surgical procedure | Segmental resection | 81 (76.4) | 37 (34.9) | 44 (41.5) | 0.836 |
| Anterior resection | 13 (12.3) | 6 (5.6) | 7 (6.6) | ||
| Hartmann’s procedure | 6 (5.7) | 2 (1.9) | 4 (3.8) | ||
| Abdominoperineal resection | 2 (1.9) | 1 (0.9) | 1 (0.9) | ||
| Surgical approach | Open surgery | 74 (69.8) | 33 (31.1) | 41 (38.6) | 0.608 |
| Laparoscopic | 32 (30.2) | 16 (15) | 16 (15) | ||
| Associated resection | None | 67 (63.2) | 30 (28.3) | 37 (34.9) | 0.679 |
| 1 organ | 23 (21.7) | 10 (9.4) | 13 (12.2) | ||
| ≥2 organs | 16 (15.1) | 9 (8.4) | 7 (6.6) | ||
| Synchronous liver resection | 11 (10.4) | 8 (7.5) | 3 (2.8) | 0.063 | |
| Stoma | 22 (21.7) | 10 (9.4) | 12 (11.3) | 0.969 | |
| Lymph node involvement | 59 (55.7) | 25 (23.5) | 34 (32) | 0.372 | |
| Surgical margins status | R0 | 98 (92.5) | 46 (43.3) | 52 (49) | 0.723 |
| R1 | 8 (7.5) | 3 (2.8) | 5 (4.7) | ||
| Adjuvant chemotherapy | 63 (59.4) | 36 (33.9) | 27 (25.4) | 0.006 | |
| Delay from surgery to chemotherapy, days | Mean | 37 | 34 | 40 | <0.001 |
| Complications | Patients Aged 50–69 Years n = 49 (46.2%) | Patients Aged ≥70 Years n = 57 (53.8%) | p-Value | |
|---|---|---|---|---|
| Clavien–Dindo grade III–IV | 3 (2.8) | 9 (8.5) | 0.117 | |
| Comprehensive complication index | Median | 8.7 | 0 | 0.697 |
| IQR | 20.9 | 8.7 | ||
| Complications/patient ≥ 1 | 25 (23.5) | 22 (20.7) | 0.199 | |
| Anastomotic leakage | 1 (0.9) | 5 (4.7) | 0.213 | |
| Other infectious complications | Pelvic abscess | 1 (0.9) | 0 (0) | 0.462 |
| Intra-abdominal abscess | 2 (1.9) | 4 (3.8) | 0.684 | |
| Urinary infection | 1 (0.9) | 2 (1.9) | 1.000 | |
| Wound infection | 4 (3.8) | 6 (5.7) | 0.749 | |
| Non-infectious complications | Ileus | 7 (6.6) | 11 (10.3) | 0.476 |
| Pulmonary failure/pleuresia | 2 (1.9) | 1 (0.9) | 0.594 | |
| Intra-abdominal bleeding | 1 (0.9) | 0 (0) | 0.430 | |
| Cardiac complications | 1 (0.9) | 1 (0.9) | 1.000 |
| Variable | HR [95% CI] | p-Value |
|---|---|---|
| Age more than 70 years (vs. less than 70 years) | 1.030 [1–1.061] | 0.048 |
| Male sex (vs. Female) | 0.664 [0.324–1.361] | 0.264 |
| BMI ≥ 30 kg/m2 (vs. < 30) | 0.756 [0.230–2.483] | 0.645 |
| ASA ≥ 2 (vs. < 2) | 0.632 [0.241–1.658] | 0.351 |
| Elevated CEA (vs. low CEA) | 1.16 [0.558–2.411] | 0.690 |
| Colon (vs. rectum) | 0.921 [0.379–2.239] | 0.856 |
| Synchronous liver metastases (vs. no synchronous metastases) | 0.839 [0.255–2.757] | 0.008 |
| Neoadjuvant treatment (vs. no neoadjuvant treatment) | 0.964 [0.338–2.752] | 0.945 |
| Emergent surgery (vs. elective) | 1.422 [0638–3.168] | 0.389 |
| Laparoscopic approach (vs. open) | 0.382 [0.147–0.995] | 0.049 |
| Multiple organ resection (vs. no resection) | 1.074 [0.524–2.2] | 0.845 |
| Synchronous liver resection (vs. no synchronous liver resection) | 0.839 [0.255–2.757] | 0.772 |
| N+ status (vs. N0 status) | 1.517 [0.740–3.108] | 0.255 |
| R1 margins (vs. R0 margins) | 3.754 [1.273–11.07] | 0.017 |
| Postoperative complications (vs. no postoperative complications) | 1.393 [0.692–2.802] | 0.353 |
| Grade III–IV complications (vs. no major complications) | 0.964 [0.294–3.166] | 0.952 |
| CCI Score | 0.990 [0.9631.018] | 0.476 |
| Adjuvant chemotherapy (vs. no adjuvant chemotherapy) | 0.936 [0.431–2.031] | 0.867 |
| Variable | HR [95% CI] | p-Value |
|---|---|---|
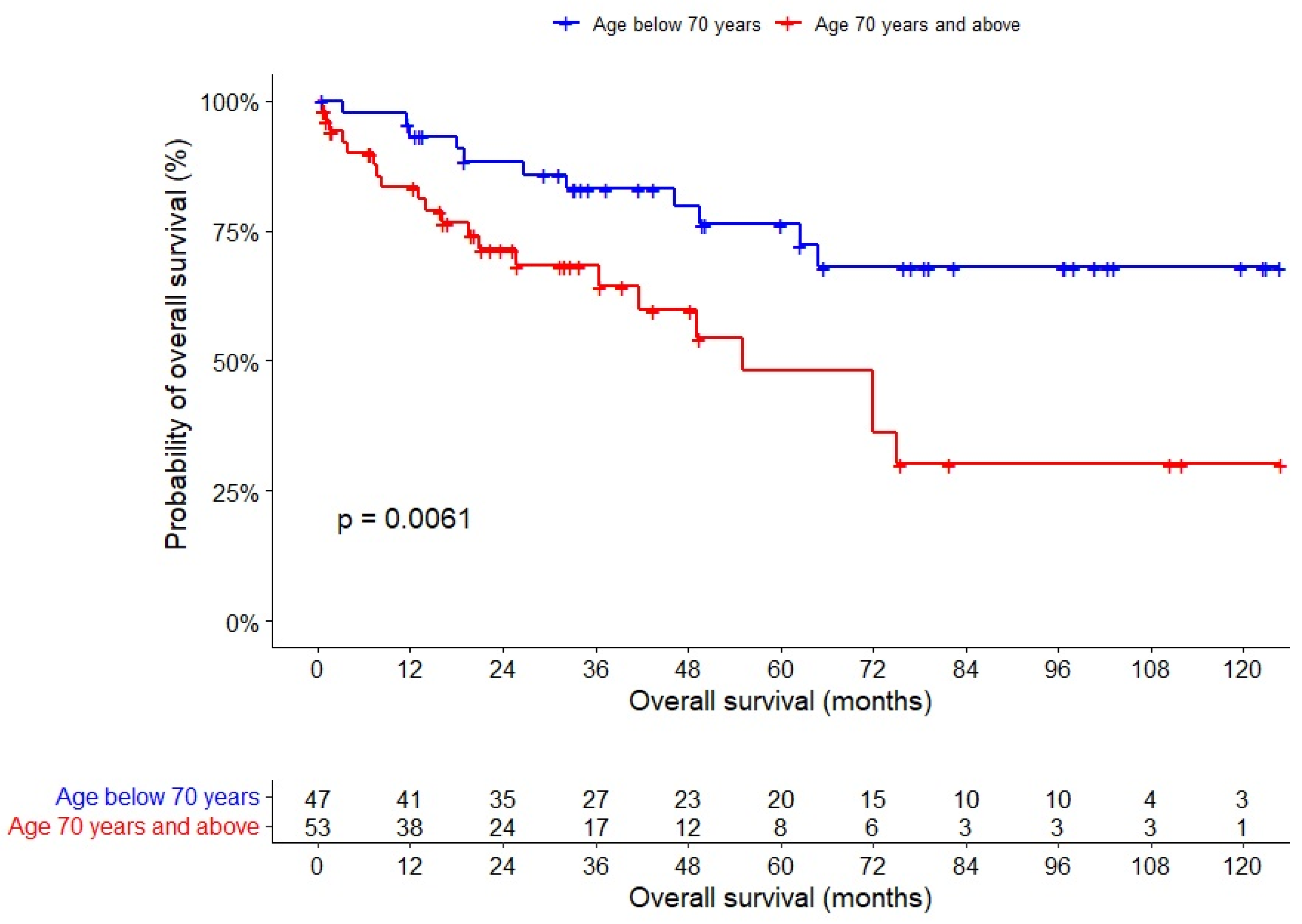
| Age more than 70 years (vs. less than 70 years) | 3.322 [1.491–7.398] | 0.003 |
| Synchronous liver metastasis | 2.633 [1.102–6.286] | 0.004 |
| Laparoscopic approach (vs. open) | 0.506 [0.224–1.115] | 0.078 |
| R1 margins (vs. R0 margins) | 3.043 [0.964–9.603] | 0.058 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osseis, M.; Nehmeh, W.A.; Rassy, N.; Derienne, J.; Noun, R.; Salloum, C.; Rassy, E.; Boussios, S.; Azoulay, D. Surgery for T4 Colorectal Cancer in Older Patients: Determinants of Outcomes. J. Pers. Med. 2022, 12, 1534. https://doi.org/10.3390/jpm12091534
Osseis M, Nehmeh WA, Rassy N, Derienne J, Noun R, Salloum C, Rassy E, Boussios S, Azoulay D. Surgery for T4 Colorectal Cancer in Older Patients: Determinants of Outcomes. Journal of Personalized Medicine. 2022; 12(9):1534. https://doi.org/10.3390/jpm12091534
Chicago/Turabian StyleOsseis, Michael, William A Nehmeh, Nathalie Rassy, Joseph Derienne, Roger Noun, Chady Salloum, Elie Rassy, Stergios Boussios, and Daniel Azoulay. 2022. "Surgery for T4 Colorectal Cancer in Older Patients: Determinants of Outcomes" Journal of Personalized Medicine 12, no. 9: 1534. https://doi.org/10.3390/jpm12091534