
Treatment of Distal Radius Fractures with Bridging External Fixator with Optional Percutaneous K-Wires: What Are the Right Indications for Patient Age, Gender, Dominant Limb and Injury Pattern?

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
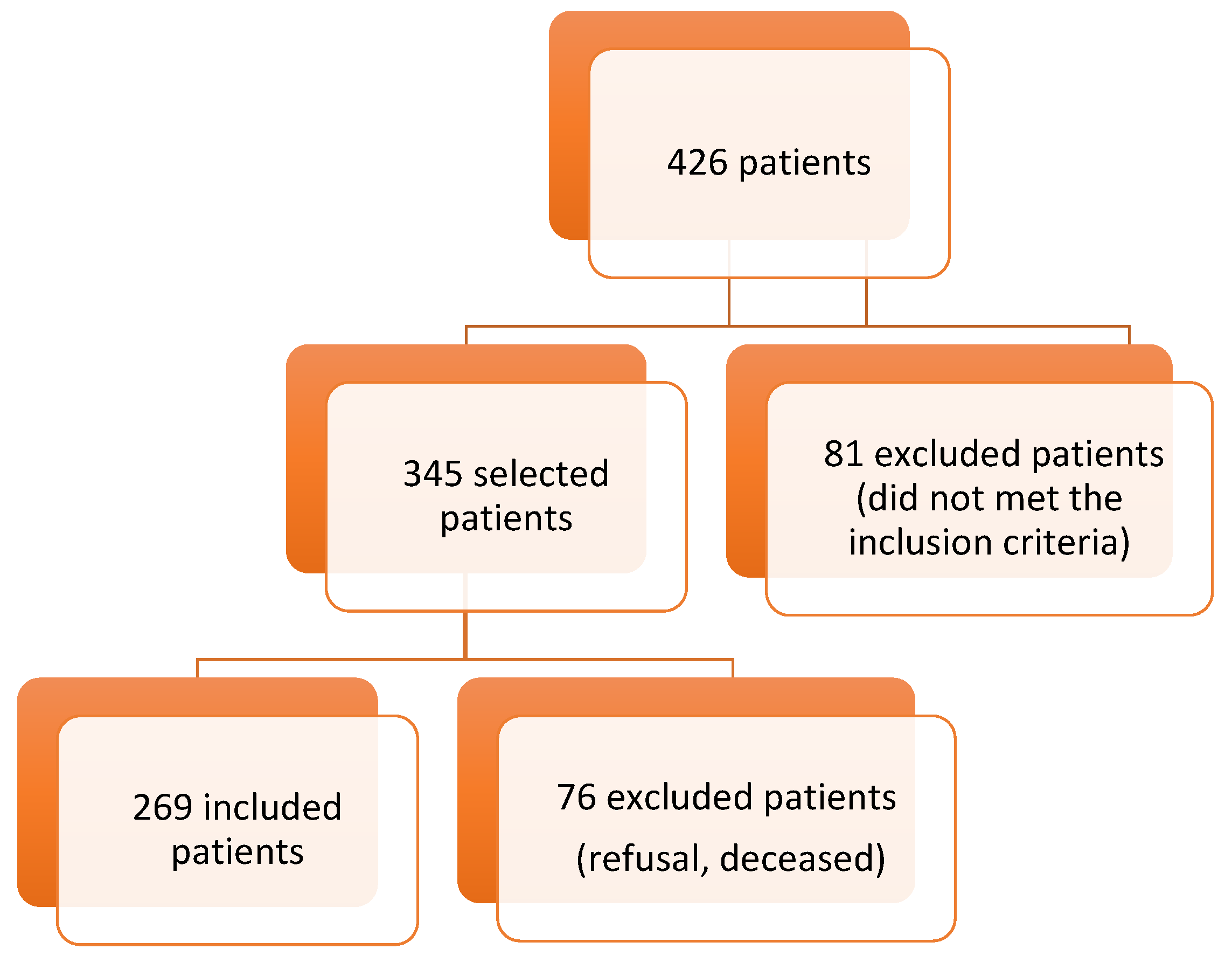
2.1. Patients
2.2. Ethics
2.3. Inclusion and Exclusion Criteria
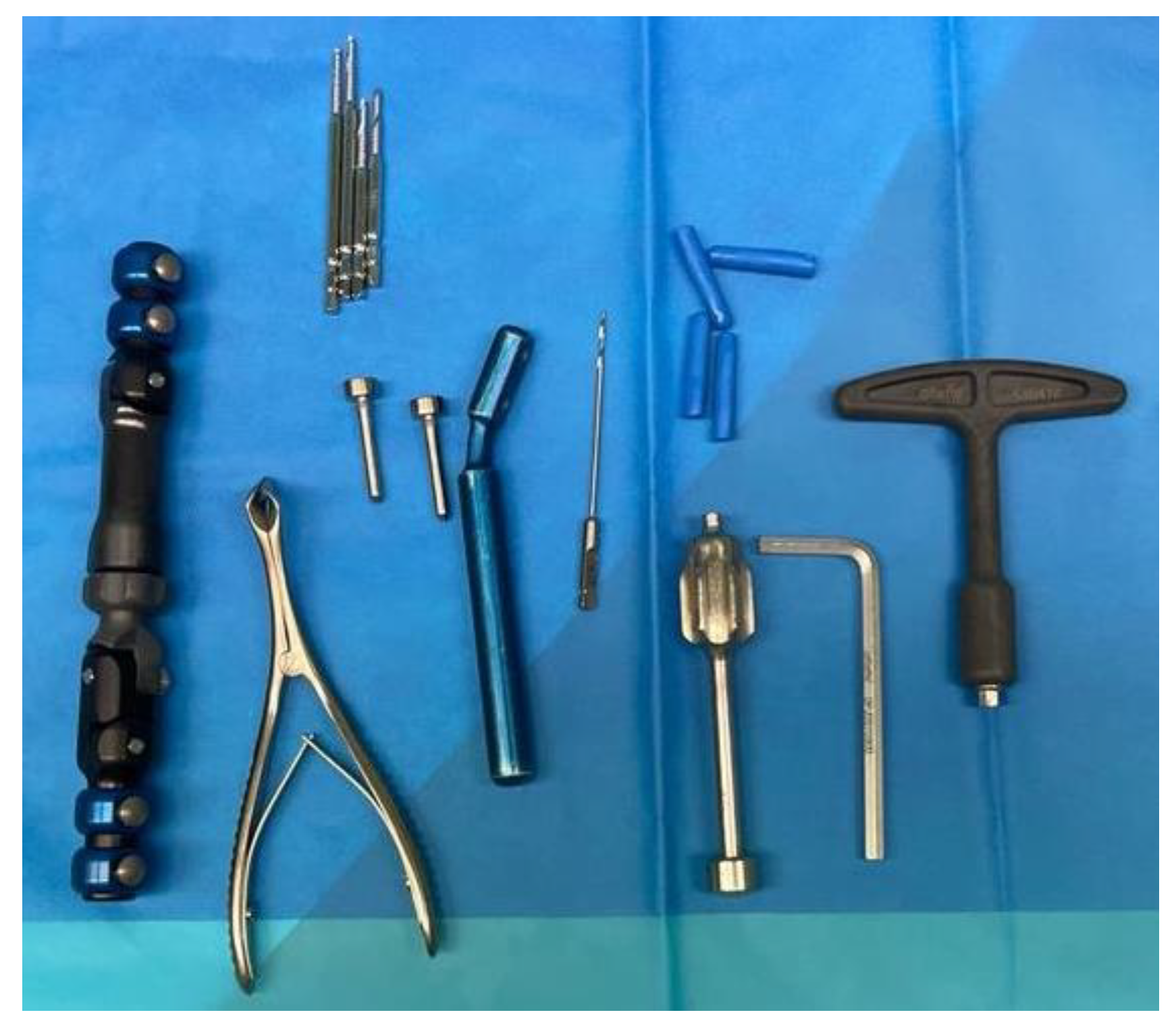
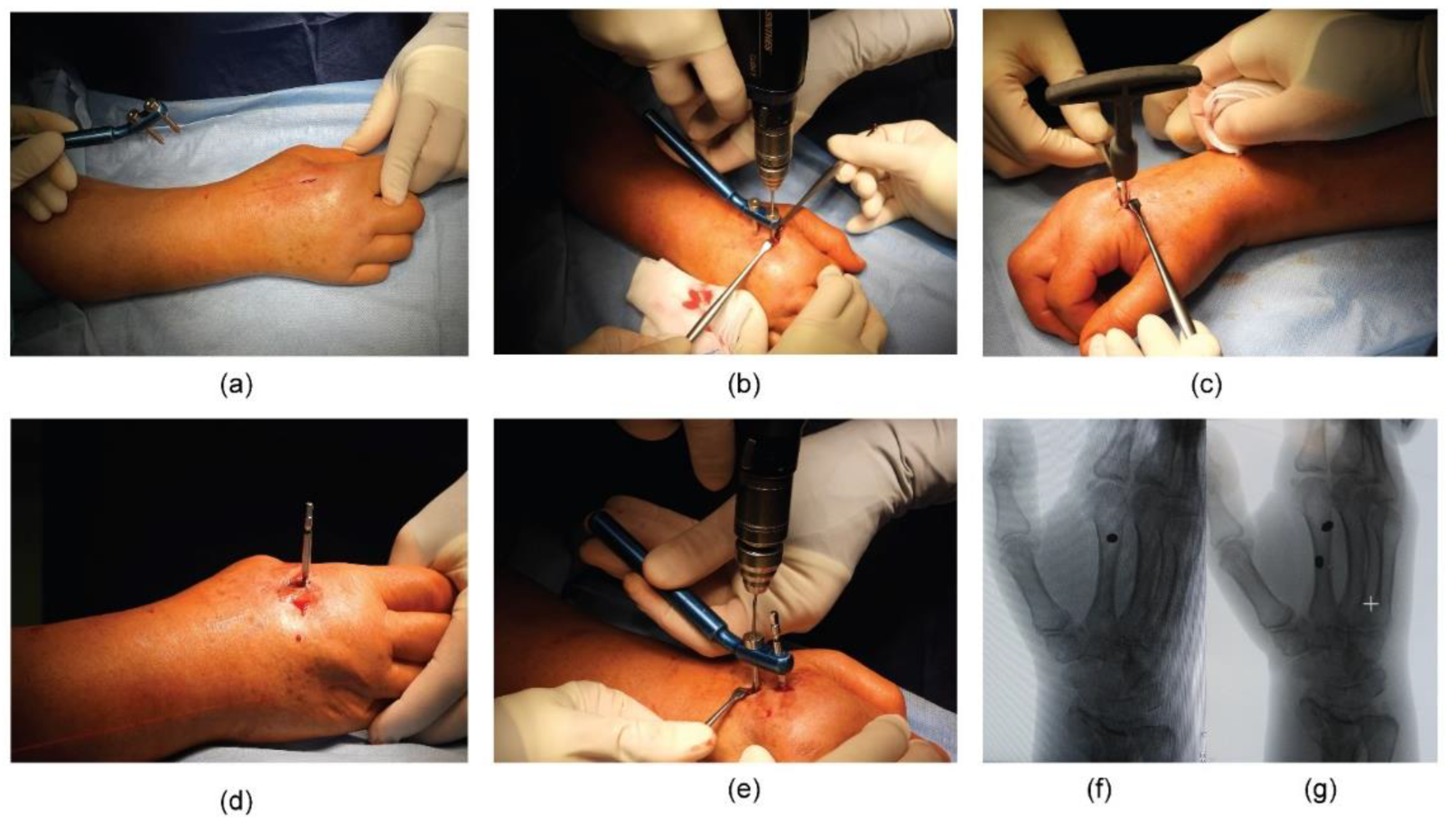
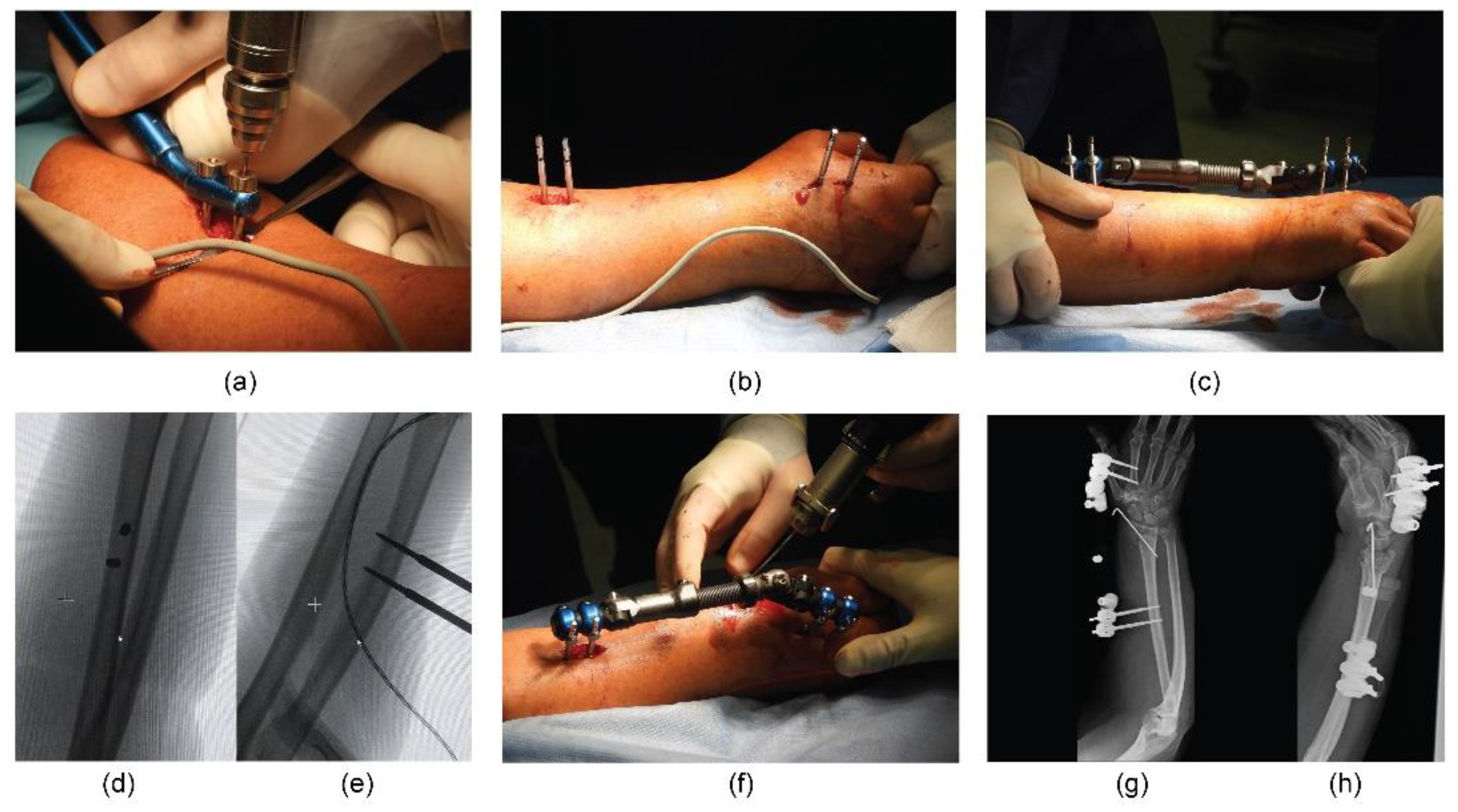
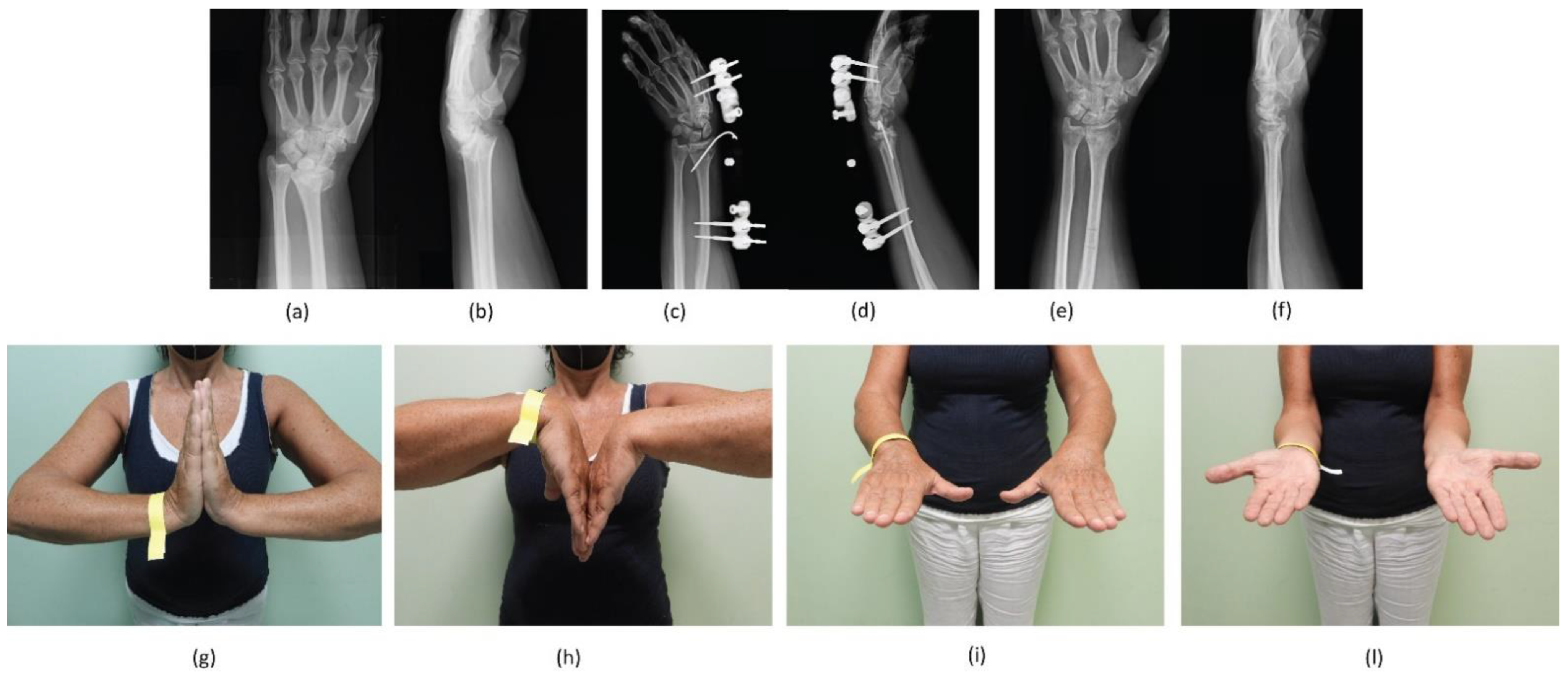
2.4. Surgical Percutaneous Techniques
2.5. Post-Operative Protocol of Both Procedures
2.6. Patient Assessment
- (1)
- BEF group;
- (2)
- BEF + KWs group.
2.7. Statistical Analysis
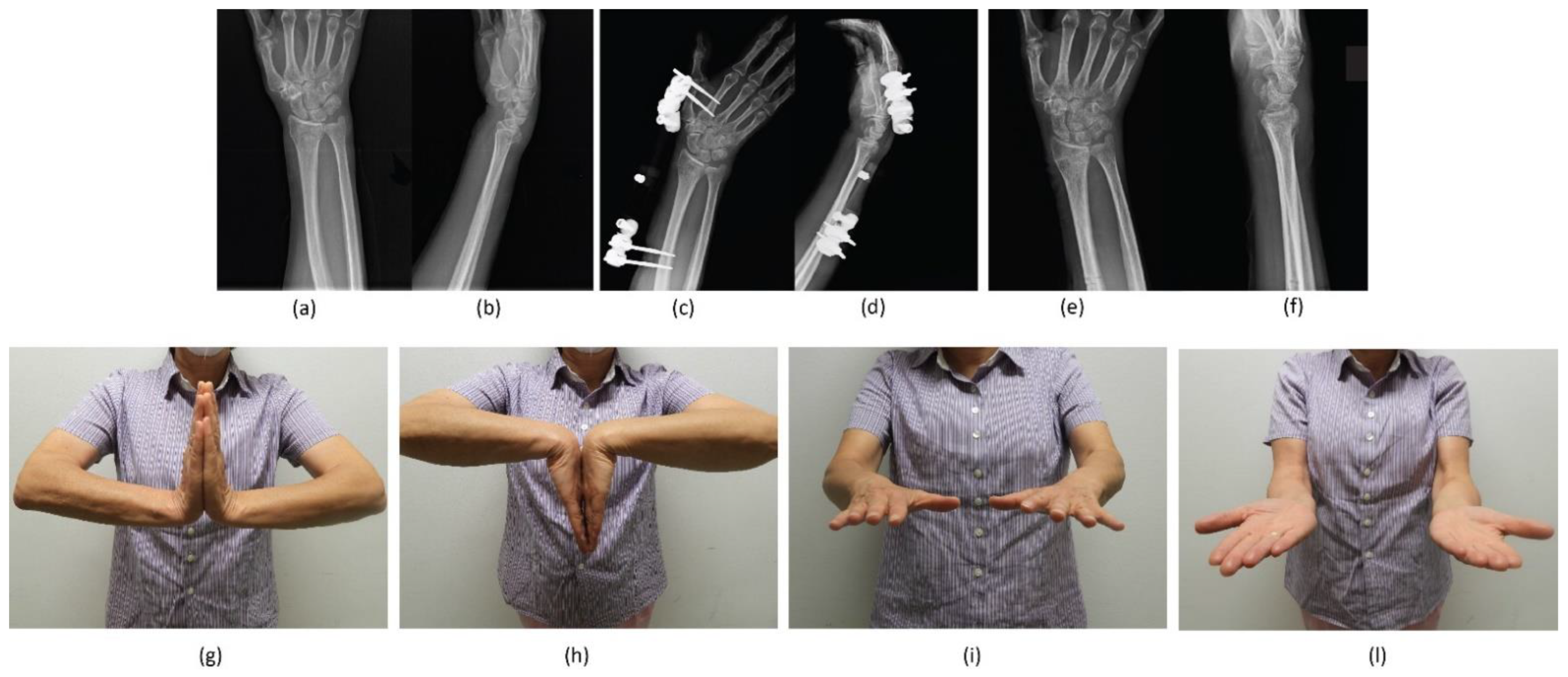
3. Results
3.1. Patient Data
3.2. Complications
3.3. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nellans, K.W.; Kowalski, E.; Chung, K.C. The epidemiology of distal radius fractures. Hand Clin. 2012, 28, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Singer, B.R.; McLauchlan, G.J.; Robinson, C.M.; Christie, J. Epidemiology of fractures in 15,000 adults: The influence of age and gender. J. Bone Joint Surg. Br. 1998, 80, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Schuit, S.C.; van der Klift, M.; Weel, A.E.; de Laet, C.E.; Burger, H.; Seeman, E.; Hofman, A.; Uitterlinden, A.G.; van Leeuwen, J.P.; Pols, H.A. Fracture incidence and association with bone mineral density in elderly men and women: The Rotterdam Study. Bone 2004, 34, 195–202. [Google Scholar] [CrossRef]
- Court-Brown, C.M.; Caesar, B. Epidemiology of adult fractures: A review. Injury 2006, 37, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Meena, S.; Sharma, P.; Sambharia, A.K.; Dawar, A. Fractures of Distal Radius: An Overview. J. Fam. Med. Prim. Care 2014, 3, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Tagliapietra, J.; Zonta, F.; Belluzzi, E.; Bragazzi, N.L.; Ruggieri, P. Predictors of early failure of the cannulated screw system in patients, 65 years and older, with non-displaced femoral neck fractures. Aging Clin. Exp. Res. 2020, 32, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Krämer, S.; Meyer, H.; O’Loughlin, P.F.; Vaske, B.; Krettek, C.; Gaulke, R. The incidence of ulnocarpal complaints after distal radial fracture in relation to the fracture of the ulnar styloid. J. Hand Surg. (Eur. Vol. ) 2012, 38, 710–717. [Google Scholar] [CrossRef]
- May, M.M.; Lawton, J.N.; Blazar, P.E. Ulnar styloid fractures associated with distal radius fractures: Incidence and implications for distal radioulnar joint instability. J. Hand Surg. 2002, 27, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, C.; Biz, C. Plating in diaphyseal fractures of the forearm. Acta Biomed. 2014, 84, 202–211. [Google Scholar]
- MacIntyre, N.J.; Dewan, N. Epidemiology of distal radius fractures and factors predicting risk and prognosis. J. Hand Ther. 2016, 29, 136–145. [Google Scholar] [CrossRef]
- Levin, L.S.; Rozell, J.C.; Pulos, N. Distal Radius Fractures in the Elderly. JAAOS J. Am. Acad. Orthop. Surg. 2017, 25, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.; Wu, F.; Chen, H.; Jiang, C.; Wang, T.; Han, P.; Chai, Y. Early hybrid nonbridging external fixation of unstable distal radius fractures in patients aged ≥50 years. J. Int. Med. Res. 2020, 48, 0300060519879562. [Google Scholar] [CrossRef] [PubMed]
- Bäcker, H.C.; Thiele, K.; Wu, C.H.; Moroder, P.; Stöckle, U.; Braun, K.F. Distal Radius Fracture with Ipsilateral Elbow Dislocation: A Rare but Challenging Injury. J. Pers. Med. 2022, 12, 1097. [Google Scholar] [CrossRef] [PubMed]
- Biz, C.; Crimì, A.; Belluzzi, E.; Maschio, N.; Baracco, R.; Volpin, A.; Ruggieri, P. Conservative Versus Surgical Management of Elbow Medial Ulnar Collateral Ligament Injury: A Systematic Review. Orthop. Surg. 2019, 11, 974–984. [Google Scholar] [CrossRef]
- Buckley, R.E. AO Principles of Fracture Management; Thieme Medical Publishers: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Young, B.T.; Rayan, G.M. Outcome following nonoperative treatment of displaced distal radius fractures in low-demand patients older than 60 years. J. Hand Surg. 2000, 25, 19–28. [Google Scholar] [CrossRef]
- Synn, A.J.; Makhni, E.C.; Makhni, M.C.; Rozental, T.D.; Day, C.S. Distal Radius Fractures in Older Patients: Is Anatomic Reduction Necessary? Clin. Orthop. Relat. Res. 2009, 467, 1612–1620. [Google Scholar] [CrossRef]
- Obert, L.; Rey, P.B.; Uhring, J.; Gasse, N.; Rochet, S.; Lepage, D.; Serre, A.; Garbuio, P. Fixation of distal radius fractures in adults: A review. Orthop. Traumatol. Surg. Res. 2013, 99, 216–234. [Google Scholar] [CrossRef]
- Handoll, H.H.G.; Madhok, R. From evidence to best practice in the management of fractures of the distal radius in adults: Working towards a research agenda. BMC Musculoskelet. Disord. 2003, 4, 27. [Google Scholar] [CrossRef]
- Padegimas, E.M.; Ilyas, A.M. Distal radius fractures: Emergency department evaluation and management. Orthop. Clin. N. Am. 2015, 46, 259–270. [Google Scholar] [CrossRef]
- Mellstrand Navarro, C.; Ahrengart, L.; Törnqvist, H.; Ponzer, S. Volar Locking Plate or External Fixation with Optional Addition of K-Wires for Dorsally Displaced Distal Radius Fractures: A Randomized Controlled Study. J. Orthop. Trauma 2016, 30, 217–224. [Google Scholar] [CrossRef]
- Liu, Y.; Bai, Y.M. Efficacy of non-bridging external fixation in treating distal radius fractures. Orthop. Surg. 2020, 12, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Pathak, S.; Sandhu, H.; Bagtharia, P.; Kumar, N.; Bajwa, R.S.; Pruthi, V.; Chawla, J.S. Prospective randomized study comparing the external fixator and volar locking plate in intraarticular distal radius fractures: Which is better? Cureus 2020, 12, e6849. [Google Scholar] [CrossRef]
- Li, J.; Rai, S.; Tang, X.; Ze, R.; Liu, R.; Hong, P. Fixation of delayed distal radial fracture involving metaphyseal diaphyseal junction in adolescents: A comparative study of crossed Kirschner-wiring and non-bridging external fixator. BMC Musculoskelet. Disord. 2020, 21, 365. [Google Scholar] [CrossRef] [PubMed]
- Marsh, J.L.; Slongo, T.F.; Agel, J.; Broderick, J.S.; Creevey, W.; DeCoster, T.A.; Prokuski, L.; Sirkin, M.S.; Ziran, B.; Henley, B.; et al. Fracture and dislocation classification compendium—2007: Orthopaedic Trauma Association classification, database and outcomes committee. J. Orthop. Trauma 2007, 21, S1–S133. [Google Scholar] [CrossRef] [PubMed]
- Padulo, J.; Oliva, F.; Frizziero, A.; Maffulli, N. Basic principles and recommendations in clinical and field science research. Muscles Ligaments Tendons J. 2013, 3, 250–252. [Google Scholar]
- Leixnering, M.; Rosenauer, R.; Pezzei, C.; Jurkowitsch, J.; Beer, T.; Keuchel, T.; Simon, D.; Hausner, T.; Quadlbauer, S. Indications, surgical approach, reduction, and stabilization techniques of distal radius fractures. Arch. Orthop. Trauma Surg. 2020, 140, 611–621. [Google Scholar] [CrossRef]
- Walenkamp, M.M.; Vos, L.M.; Strackee, S.D.; Goslings, J.C.; Schep, N.W. The Unstable Distal Radius Fracture-How Do We Define It? A Systematic Review. J. Wrist Surg. 2015, 4, 307–316. [Google Scholar] [CrossRef]
- Gou, Q.; Xiong, X.; Cao, D.; He, Y.; Li, X. Volar locking plate versus external fixation for unstable distal radius fractures: A systematic review and meta-analysis based on randomized controlled trials. BMC Musculoskelet. Disord. 2021, 22, 433. [Google Scholar] [CrossRef]
- Fairplay, T.; Atzei, A.; Corradi, M.; Luchetti, R.; Cozzolino, R.; Schoenhuber, R. Cross-cultural adaptation and validation of the Italian version of the patient-rated wrist/hand evaluation questionnaire. J. Hand Surg. (Eur. Vol.) 2012, 37, 863–870. [Google Scholar] [CrossRef]
- Beaton, D.E.; Wright, J.G.; Katz, J.N. Development of the QuickDASH: Comparison of three item-reduction approaches. J. Bone Jt. Surgery. Am. Vol. 2005, 87, 1038–1046. [Google Scholar] [CrossRef]
- Firth, D. Bias reduction of maximum likelihood estimates. Biometrika 1993, 80, 27–38. [Google Scholar] [CrossRef]
- Kosmidis, I. brglm2: Bias Reduction in Generalized Linear Models. Available online: https://CRAN.R-project.org/package=brglm2 (accessed on 28 June 2022).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]
- Chhabra, A.B.; Yildirim, B. Adult Distal Radius Fracture Management. JAAOS J. Am. Acad. Orthop. Surg. 2021, 29, e1105–e1116. [Google Scholar] [CrossRef]
- Rüedi, T.P.; Murphy, W.M.; Colton, C.L.; Fackelman, G.E.; Harder, Y. AO Principles of Fracture Management; Thieme: Stuttgart, Germany, 2000. [Google Scholar]
- Patterson, M. Apley’s Concise System of Orthopaedics and Fractures 3rd edn). Ann. R. Coll. Surg. Engl. 2006, 88, 425–426. [Google Scholar] [CrossRef]
- Chen, N.C.; Jupiter, J.B. Management of distal radial fractures. J. Bone Jt. Surgery. Am. Vol. 2007, 89, 2051–2062. [Google Scholar] [CrossRef]
- Walenkamp, M.M.; Bentohami, A.; Beerekamp, M.S.; Peters, R.W.; van der Heiden, R.; Goslings, J.C.; Schep, N.W. Functional outcome in patients with unstable distal radius fractures, volar locking plate versus external fixation: A meta-analysis. Strateg. Trauma Limb Reconstr. 2013, 8, 67–75. [Google Scholar] [CrossRef]
- Hammer, O.L.; Clementsen, S.; Hast, J.; Šaltytė Benth, J.; Madsen, J.E.; Randsborg, P.H. Volar Locking Plates Versus Augmented External Fixation of Intra-Articular Distal Radial Fractures: Functional Results from a Randomized Controlled Trial. J. Bone Jt. Surgery. Am. Vol. 2019, 101, 311–321. [Google Scholar] [CrossRef]
- Xie, M.; Cao, Y.; Cai, X.; Shao, Z.; Nie, K.; Xiong, L. The Effect of a PEEK Material-Based External Fixator in the Treatment of Distal Radius Fractures with Non-Transarticular External Fixation. Orthop. Surg. 2021, 13, 90–97. [Google Scholar] [CrossRef]
- Luokkala, T.; Laitinen, M.K.; Hevonkorpi, T.P.; Raittio, L.; Mattila, V.M.; Launonen, A.P. Distal radius fractures in the elderly population. EFORT Open Rev. 2020, 5, 361–370. [Google Scholar] [CrossRef]
- Vakhshori, V.; Rounds, A.D.; Heckmann, N.; Azad, A.; Intravia, J.M.; Rosario, S.; Stevanovic, M.; Ghiassi, A. The Declining Use of Wrist-Spanning External Fixators. Hand (N Y) 2020, 15, 255–263. [Google Scholar] [CrossRef]
- Tang, J.B. Distal Radius Fracture: Diagnosis, Treatment, and Controversies. Clin. Plast. Surg. 2014, 41, 481–499. [Google Scholar] [CrossRef]
- Rectenwald, J.P.; Bentley, K.A.; Murray, P.M.; Saha, S. Strain as a Function of Time in Extrinsic Wrist Ligaments Tensioned Through External Fixation. Hand (N Y) 2018, 13, 60–64. [Google Scholar] [CrossRef] [Green Version]
- Fu, Y.C.; Chien, S.H.; Huang, P.J.; Chen, S.K.; Tien, Y.C.; Lin, G.T.; Wang, G.J. Use of an external fixation combined with the buttress-maintain pinning method in treating comminuted distal radius fractures in osteoporotic patients. J. Trauma 2006, 60, 330–333. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, Y.; Mao, Z.; Zhang, L.; Li, H.; Yan, H.; Liu, X.; Tang, P. Volar locking plate versus external fixation for the treatment of unstable distal radial fractures: A meta-analysis of randomized controlled trials. J. Surg. Res. 2015, 193, 324–333. [Google Scholar] [CrossRef]
- Walenkamp, M.M.J.; Mulders, M.A.M.; Goslings, J.C.; Westert, G.P.; Schep, N.W.L. Analysis of variation in the surgical treatment of patients with distal radial fractures in the Netherlands. J. Hand Surg. Eur. Vol. 2017, 42, 39–44. [Google Scholar] [CrossRef]
- Gummesson, C.; Atroshi, I.; Ekdahl, C. The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: Longitudinal construct validity and measuring self-rated health change after surgery. BMC Musculoskelet. Disord. 2003, 4, 11. [Google Scholar] [CrossRef]
- Lee, S.J.; Park, J.W.; Kang, B.J.; Lee, J.I. Clinical and radiologic factors affecting functional outcomes after volar locking plate fixation of dorsal angulated distal radius fractures. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2016, 21, 619–624. [Google Scholar] [CrossRef]
- Capo, J.T.; Rossy, W.; Henry, P.; Maurer, R.J.; Naidu, S.; Chen, L. External fixation of distal radius fractures: Effect of distraction and duration. J. Hand Surg. 2009, 34, 1605–1611. [Google Scholar] [CrossRef]
- Anderson, J.T.; Lucas, G.L.; Buhr, B.R. Complications of treating distal radius fractures with external fixation: A community experience. Iowa Orthop. J. 2004, 24, 53–59. [Google Scholar]
- Ma, C.; Deng, Q.; Pu, H.; Cheng, X.; Kan, Y.; Yang, J.; Yusufu, A.; Cao, L. External fixation is more suitable for intra-articular fractures of the distal radius in elderly patients. Bone Res. 2016, 4, 16017. [Google Scholar] [CrossRef]
- Sanders, R.A.; Keppel, F.L.; Waldrop, J.I. External fixation of distal radial fractures: Results and complications. J. Hand Surg. 1991, 16, 385–391. [Google Scholar] [CrossRef]
- Weber, S.C.; Szabo, R.M. Severely comminuted distal radial fracture as an unsolved problem: Complications associated with external fixation and pins and plaster techniques. J. Hand Surg. 1986, 11, 157–165. [Google Scholar] [CrossRef]
- Xie, X.; Xie, X.; Qin, H.; Shen, L.; Zhang, C. Comparison of internal and external fixation of distal radius fractures. Acta Orthop. 2013, 84, 286–291. [Google Scholar] [CrossRef] [Green Version]
- Edwards, G.S., Jr. Intra-articular fractures of the distal part of the radius treated with the small AO external fixator. J. Bone Jt. Surgery. Am. Vol. 1991, 73, 1241–1250. [Google Scholar] [CrossRef]
- Dienst, M.; Wozasek, G.E.; Seligson, D. Dynamic external fixation for distal radius fractures. Clin. Orthop. Relat. Res. 1997, 338, 160–171. [Google Scholar] [CrossRef]
- Horesh, Z.; Volpin, G.; Hoerer, D.; Stein, H. The surgical treatment of severe comminuted intraarticular fractures of the distal radius with the small AO external fixation device. A prospective three-and-one-half-year follow-up study. Clin. Orthop. Relat. Res. 1991, 263, 147–153. [Google Scholar] [CrossRef]
- Raskin, K.B.; Melone, C.P., Jr. Unstable articular fractures of the distal radius. Comparative techniques of ligamentotaxis. Orthop. Clin. N. Am. 1993, 24, 275–286. [Google Scholar] [CrossRef]
- Gelberman, R.H.; Szabo, R.M.; Mortensen, W.W. Carpal tunnel pressures and wrist position in patients with colles’ fractures. J. Trauma 1984, 24, 747–749. [Google Scholar] [CrossRef]
- Hertel, R.; Ballmer, F. Complications of external fixation of the wrist. Injury 1994, 25 (Suppl. S4), S-d39-43. [Google Scholar] [CrossRef]
- Burke, E.F.; Singer, R.M. Treatment of comminuted distal radius with the use of an internal distraction plate. Tech. Hand Up. Extrem. Surg. 1998, 2, 248–252. [Google Scholar] [CrossRef]
- Dicpinigaitis, P.; Wolinsky, P.; Hiebert, R.; Egol, K.; Koval, K.; Tejwani, N. Can external fixation maintain reduction after distal radius fractures? J. Trauma 2004, 57, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Jorge-Mora, A.A.; Cecilia-López, D.; Rodríguez-Vega, V.; Suárez-Arias, L.; Andrés-Esteban, E.; Porras-Moreno, M.; Resines-Erasun, C. Comparison between external fixators and fixed-angle volar-locking plates in the treatment of distal radius fractures. J. Hand Microsurg. 2012, 4, 50–54. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.J.; Wartinbee, D.A.; Riboh, J.; Miller, M.; Leversedge, F.J.; Ruch, D.S. Analysis of the complications of palmar plating versus external fixation for fractures of the distal radius. J. Hand Surg. 2011, 36, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Williksen, J.H.; Frihagen, F.; Hellund, J.C.; Kvernmo, H.D.; Husby, T. Volar locking plates versus external fixation and adjuvant pin fixation in unstable distal radius fractures: A randomized, controlled study. J. Hand Surg. 2013, 38, 1469–1476. [Google Scholar] [CrossRef]
- Maccagnano, G.; Noia, G.; Vicenti, G.; Coviello, M.; Pesce, V.; Moretti, B. A Prospective Observational Clinical and Radiological Study of a Modular Bridging External Fixator for Unstable Distal Radius Fractures. Malays Orthop. J. 2021, 15, 108–114. [Google Scholar] [CrossRef]
- Mishra, R.K.; Sharma, B.P.; Kumar, A.; Sherawat, R. A comparative study of variable angle volar plate and bridging external fixator with K-wire augmentation in comminuted distal radius fractures. Chin. J. Traumatol. 2021, 24, 301–305. [Google Scholar] [CrossRef]
- Aita, M.A.; Rodrigues, F.L.; Alves, K.; de Oliveira, R.K.; Ruggiero, G.M.; Rodrigues, L.M.R. Bridging versus Nonbridging Dynamic External Fixation of Unstable Distal Radius Fractures in the Elderly with Polytrauma: A Randomized Study. J. Wrist Surg. 2019, 8, 408–415. [Google Scholar] [CrossRef]
- Ring, D.; Jupiter, J.B. Treatment of osteoporotic distal radius fractures. Osteoporos. Int. 2005, 16, S80–S84. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Patients (n = 269) |
|---|---|
| Age | 65.55 ± 15.27 |
| Sex | |
| Female | 202 (75.1%) |
| Male | 67 (24.9%) |
| PRWHE | 12.18 ± 15.75 |
| QuickDASH | 13.13 ± 15.86 |
| Side | |
| Dominant | 106 (39.4%) |
| Non-dominant | 163 (60.6%) |
| AO classification (23) | |
| A2 | 48 (17.8%) |
| A3 | 39 (14.5%) |
| B1 | 2 (0.7%) |
| B3 | 1 (0.4%) |
| C1 | 50 (18.6%) |
| C2 | 82 (30.5%) |
| C3 | 47 (17.5%) |
| Variable | BEF (194 Patients) | BEF + KWs (75 Patients) | p-Value |
|---|---|---|---|
| Age | 65.83 ± 15.24 | 64.81 ± 15.44 | 0.59 |
| Sex | 0.57 | ||
| Female | 148 (76.3%) | 54 (72%) | |
| Male | 46 (23.7%) | 21 (28%) | |
| PRWHE | 14.59 ± 17.04 | 5.88 ± 9.20 | <0.001 |
| QuickDASH | 15.30 ± 17.10 | 7.50 ± 10.16 | <0.001 |
| Side | 0.57 | ||
| Dominant | 79 (40.7%) | 27 (36%) | |
| Non-dominant | 115 (59.3%) | 48 (64%) | |
| AO classification (23) | 0.007 | ||
| A2 | 41 (21.1%) | 7 (9.3%) | |
| A3 | 30 (15.5%) | 9 (12.0%) | |
| B1 | 0 (0%) | 2 (2.7%) | |
| B3 | 1 (0.5%) | 0 (0%) | |
| C1 | 40 (20.6%) | 10 (13.3%) | |
| C2 | 53 (27.3%) | 29 (38.7%) | |
| C3 | 29 (14.9%) | 18 (24.0%) |
| Variable | Estimate | Standard Error | Z Value | p-Value |
|---|---|---|---|---|
| Intercept | −0.377 | 0.436 | −0.866 | 0.386 |
| pp | −0.976 | 1.739 | −0.561 | 0.575 |
| BEF + KWs | −0.385 | 0.165 | −2.334 | 0.020 |
| Dominant side | 0.275 | 0.133 | 2.065 | 0.039 |
| Age | −0.018 | 0.004 | −4.004 | <0.001 |
| 23-A3 | −0.310 | 0.254 | −1.224 | 0.220 |
| 23-B | −0.173 | 0.955 | −0.181 | 0.856 |
| 23-C1 | −0.002 | 0.214 | −0.010 | 0.992 |
| 23-C2 | 0.006 | 0.386 | 0.017 | 0.986 |
| 23-C3 | 0.182 | 0.439 | 0.416 | 0.677 |
| BEF + KWs and dominant side | −0.410 | 0.266 | −1.545 | 0.122 |
| Phi coefficients | ||||
| Intercept | 0.186 | 0439 | 0.425 | 0.671 |
| Age | 0.014 | 0.006 | 2.551 | 0.011 |
| pp | 2.168 | 0.888 | 2.441 | 0.015 |
| Variable | Estimate | Standard Error | Z Value | p-Value |
|---|---|---|---|---|
| Intercept | −0.378 | 0.433 | −0.874 | 0.382 |
| pp | 0.211 | 1.735 | 0.122 | 0.903 |
| BEF + KWs | −0.249 | 0.165 | −1.516 | 0.129 |
| Dominant side | 0.354 | 0.133 | 2.664 | 0.008 |
| Age | −0.020 | 0.004 | −4.544 | <0.001 |
| 23-A3 | −0.362 | 0.251 | −1.447 | 0.148 |
| 23-B | −0.616 | 0.960 | −0.641 | 0.521 |
| 23-C1 | −0.156 | 0.211 | −0.740 | 0.459 |
| 23-C2 | −0.263 | 0.385 | −0.682 | 0.495 |
| 23-C3 | −0.120 | 0.438 | −0.273 | 0.785 |
| BEF + KWs and dominant side | −0.468 | 0.264 | −1.775 | 0.076 |
| Phi coefficients | ||||
| Intercept | −0.012 | 0.430 | −0.029 | 0.977 |
| Age | 1.546 | 0.876 | 1.764 | 0.078 |
| pp | 0.020 | 0.006 | 3.586 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biz, C.; Cerchiaro, M.; Belluzzi, E.; Bortolato, E.; Rossin, A.; Berizzi, A.; Ruggieri, P. Treatment of Distal Radius Fractures with Bridging External Fixator with Optional Percutaneous K-Wires: What Are the Right Indications for Patient Age, Gender, Dominant Limb and Injury Pattern? J. Pers. Med. 2022, 12, 1532. https://doi.org/10.3390/jpm12091532
Biz C, Cerchiaro M, Belluzzi E, Bortolato E, Rossin A, Berizzi A, Ruggieri P. Treatment of Distal Radius Fractures with Bridging External Fixator with Optional Percutaneous K-Wires: What Are the Right Indications for Patient Age, Gender, Dominant Limb and Injury Pattern? Journal of Personalized Medicine. 2022; 12(9):1532. https://doi.org/10.3390/jpm12091532
Chicago/Turabian StyleBiz, Carlo, Mariachiara Cerchiaro, Elisa Belluzzi, Elena Bortolato, Alessandro Rossin, Antonio Berizzi, and Pietro Ruggieri. 2022. "Treatment of Distal Radius Fractures with Bridging External Fixator with Optional Percutaneous K-Wires: What Are the Right Indications for Patient Age, Gender, Dominant Limb and Injury Pattern?" Journal of Personalized Medicine 12, no. 9: 1532. https://doi.org/10.3390/jpm12091532