
Direct-Acting Antivirals for HCV Treatment in Decompensated Liver Cirrhosis Patients: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
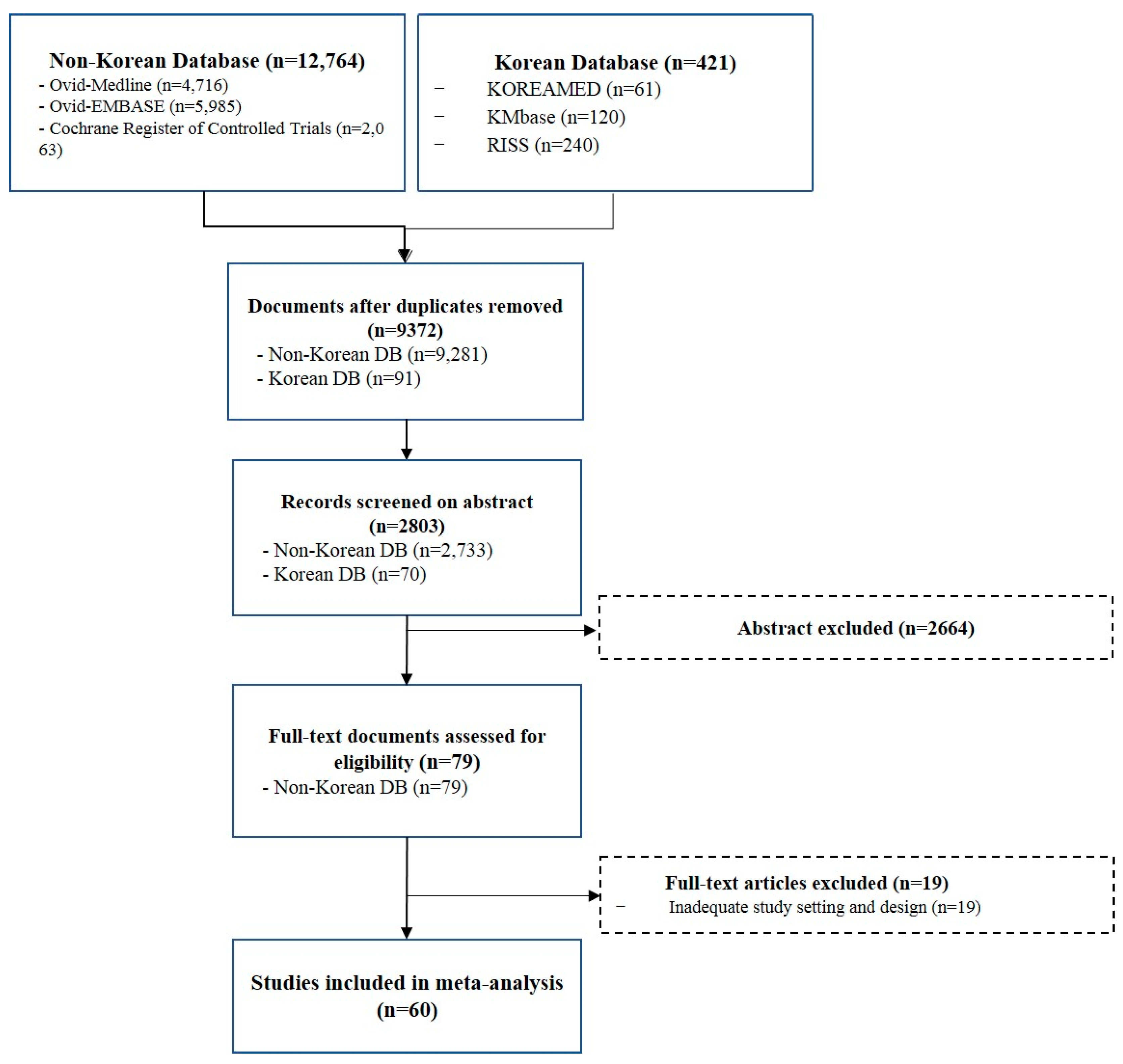
2.1. Data Sources and Searches
2.2. Definition
2.3. Study Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Risk of Bias Graph
3.3. Efficacy and Safety of DAA in DC Patients
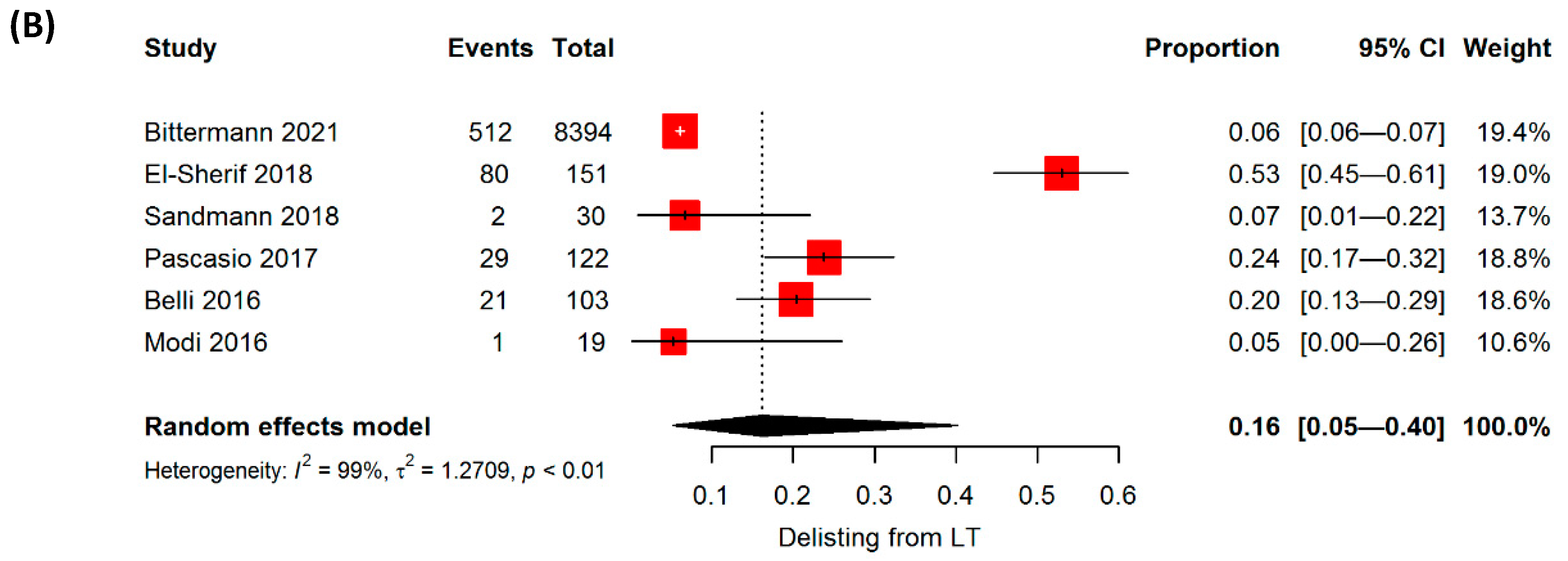
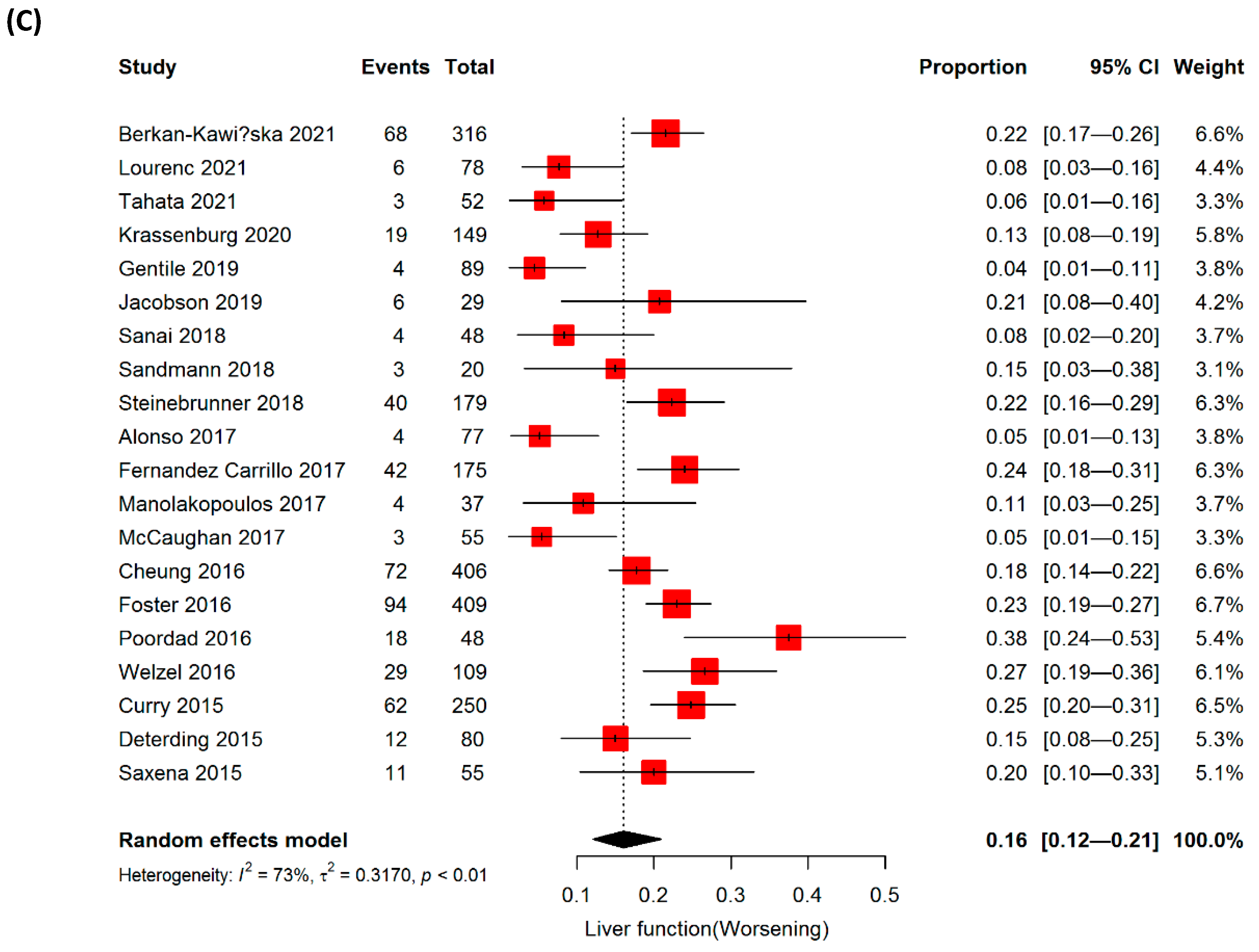
3.4. Improvement in Liver Functions and Delisting from Liver Transplantation
3.5. Efficacy and Safety of PI-based DAA in DC Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Global Hepatitis Report, 2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Korean Association for the Study of the Liver. 2021 Hepatitis C Factsheet; Korean Association for the Study of the Liver: Seoul, Korea, 2021. [Google Scholar]
- McDonald, S.A.; Innes, H.A.; Aspinall, E.; Hayes, P.C.; Alavi, M.; Valerio, H.; Goldberg, D.J.; Hutchinson, S.J. Prognosis of 1169 hepatitis C chronically infected patients with decompensated cirrhosis in the predirect-acting antiviral era. J. Viral Hepat. 2017, 24, 295–303. [Google Scholar] [CrossRef]
- Molnar, A.O.; Sood, M.M. Predicting in a predicament: Stroke and hemorrhage risk prediction in dialysis patients with atrial fibrillation. Semin. Dial. 2018, 31, 37–47. [Google Scholar] [CrossRef]
- Curry, M.P.; O’Leary, J.G.; Bzowej, N.; Muir, A.J.; Korenblat, K.M.; Fenkel, J.M.; Reddy, K.R.; Lawitz, E.; Flamm, S.L.; Schiano, T.; et al. Sofosbuvir and velpatasvir for HCV in patients with decompensated cirrhosis. N. Engl. J. Med. 2015, 373, 2618–2628. [Google Scholar] [CrossRef] [PubMed]
- Nahon, P.; Bourcier, V.; Layese, R.; Audureau, E.; Cagnot, C.; Marcellin, P.; Guyader, D.; Fontaine, H.; Larrey, D.; De Ledinghen, V.; et al. Eradication of hepatitis c virus infection in patients with cirrhosis reduces risk of liver and non-liver complications. Gastroenterology 2017, 152, 142–156. [Google Scholar] [CrossRef] [PubMed]
- Bachofner, J.A.; Valli, P.V.; Kroger, A.; Bergamin, I.; Kunzler, P.; Baserga, A.; Braun, D.; Seifert, B.; Moncsek, A.; Fehr, J.; et al. Direct antiviral agent treatment of chronic hepatitis C results in rapid regression of transient elastography and fibrosis markers fibrosis-4 score and aspartate aminotransferase-platelet ratio index. Liver Int. 2017, 37, 369–376. [Google Scholar] [CrossRef]
- Krassenburg, L.A.P.; Maan, R.; Ramji, A.; Manns, M.P.; Cornberg, M.; Wedemeyer, H.; de Knegt, R.J.; Hansen, B.E.; Janssen, H.L.A.; de Man, R.A.; et al. Clinical outcomes following DAA therapy in patients with HCV-related cirrhosis depend on disease severity. J. Hepatol. 2021, 74, 1053–1063. [Google Scholar] [CrossRef]
- Charlton, M.; Everson, G.T.; Flamm, S.L.; Kumar, P.; Landis, C.; Brown, R.S.; Fried, M.W.; Terrault, N.A.; O’Leary, J.G.; Vargas, H.E.; et al. Ledipasvir and sofosbuvir plus ribavirin for treatment of HCV infection in patients with advanced liver disease. Gastroenterology 2015, 149, 649–659. [Google Scholar] [CrossRef]
- Lawitz, E.; Sulkowski, M.S.; Ghalib, R.; Rodriguez-Torres, M.; Younossi, Z.M.; Corregidor, A.; DeJesus, E.; Pearlman, B.; Rabinovitz, M.; Gitlin, N.; et al. Simeprevir plus sofosbuvir, with or without ribavirin, to treat chronic infection with hepatitis C virus genotype 1 in non-responders to pegylated interferon and ribavirin and treatment-naive patients: The COSMOS randomised study. Lancet 2014, 384, 1756–1765. [Google Scholar] [CrossRef]
- FDA. FDA Drug Safety Communication: FDA Warns of Serious Liver Injury Risk with Hepatitis C Treatments Viekira Pak and Technivie; FDA: Silver Spring, MD, USA, 2015. [Google Scholar]
- Zuckerman, E.; Ashkenasi, E.; Kovalev, Y.; Weitzman, E.; Tur-Kaspa, R.; Brown, M.; Cohen, M.; Saadi, T.; Baruch, Y.; Carlebach, M.; et al. The real world Israeli experience of treating chronic hepatitis C genotype 1 patients with advanced fibrosis with parataprevir/ritonavir/ombitasvir, dasabuvir with or without ribavirin: A large, multi-center cohort. J. Hepatol. 2016, 64, S137. [Google Scholar] [CrossRef]
- Lawitz, E.; Poordad, F.; Gutierrez, J.A.; Kakuda, T.N.; Picchio, G.; Beets, G.; Vandevoorde, A.; Van Remoortere, P.; Jacquemyn, B.; Luo, D.; et al. Simeprevir, daclatasvir and sofosbuvir for hepatitis C virus-infected patients with decompensated liver disease. J. Viral Hepat. 2017, 24, 287–294. [Google Scholar] [CrossRef]
- Lawitz, E.; Poordad, F.; Gutierrez, J.A.; Beumont, M.; Beets, G.; Vandevoorde, A.; Remoortere, P.V.; Luo, D.; Vijgen, L.; Eygen, V.V.; et al. Simeprevir, daclatasvir, and sofosbuvir for hepatitis C virus-infected patients: Long-term follow-up results from the open-label, Phase II IMPACT study. Health Sci. Rep. 2020, 3, e145. [Google Scholar] [CrossRef] [PubMed]
- Torgersen, J.; Newcomb, C.W.; Carbonari, D.M.; Rentsch, C.T.; Park, L.S.; Mezochow, A.; Mehta, R.L.; Buchwalder, L.; Tate, J.P.; Bräu, N.; et al. Protease inhibitor-based direct-acting antivirals are associated with increased risk of aminotransferase elevations but not hepatic dysfunction or decompensation. J. Hepatol. 2021, 75, 1312–1322. [Google Scholar] [CrossRef] [PubMed]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: The PRISMA-DTA statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Venick, R.S.; Farmer, D.G.; Soto, J.R.; Vargas, J.; Yersiz, H.; Kaldas, F.M.; Agopian, V.G.; Hiatt, J.R.; McDiarmid, S.V.; Busuttil, R.W. One thousand pediatric liver transplants during thirty years: Lessons learned. J. Am. Coll. Surg. 2018, 226, 355–366. [Google Scholar] [CrossRef]
- Afdhal, N.; Everson, G.T.; Calleja, J.L.; McCaughan, G.W.; Bosch, J.; Brainard, D.M.; McHutchison, J.G.; De-Oertel, S.; An, D.; Charlton, M.; et al. Effect of viral suppression on hepatic venous pressure gradient in hepatitis C with cirrhosis and portal hypertension. J. Viral. Hepat. 2017, 24, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S.; Riveiro-Barciela, M.; Fernandez, I.; Rincon, D.; Real, Y.; Llerena, S.; Gea, F.; Olveira, A.; Fernandez-Carrillo, C.; Polo, B.; et al. Effectiveness and safety of sofosbuvir-based regimens plus an NS5A inhibitor for patients with HCV genotype 3 infection and cirrhosis. Results of a multicenter real-life cohort. J. Viral. Hepat. 2017, 24, 304–311. [Google Scholar] [CrossRef]
- Backus, L.I.; Belperio, P.S.; Shahoumian, T.A.; Loomis, T.P.; Mole, L.A. Comparative effectiveness of ledipasvir/sofosbuvir +/− ribavirin vs. ombitasvir/paritaprevir/ritonavir + dasabuvir +/− ribavirin in 6961 genotype 1 patients treated in routine medical practice. Aliment. Pharmacol. Ther. 2016, 44, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Berkan-Kawinska, A.; Piekarska, A.; Janczewska, E.; Lorenc, B.; Tudrujek-Zdunek, M.; Tomasiewicz, K.; Berak, H.; Horban, A.; Zarebska-Michaluk, D.; Pabjan, P.; et al. Real-world effectiveness and safety of direct-acting antivirals in patients with cirrhosis and history of hepatic decompensation: Epi-Ter2 Study. Liver Int. 2021, 41, 1789–1801. [Google Scholar] [CrossRef]
- Calleja, J.L.; Crespo, J.; Rincon, D.; Ruiz-Antoran, B.; Fernandez, I.; Perello, C.; Gea, F.; Lens, S.; Garcia-Samaniego, J.; Sacristan, B.; et al. Effectiveness, safety and clinical outcomes of direct-acting antiviral therapy in HCV genotype 1 infection: Results from a Spanish real-world cohort. J. Hepatol. 2017, 66, 1138–1148. [Google Scholar] [CrossRef]
- Calvaruso, V.; Craxi, A. Hepatic benefits of HCV cure. J. Hepatol. 2020, 73, 1548–1556. [Google Scholar] [CrossRef]
- Fernandez Carrillo, C.; Lens, S.; Llop, E.; Pascasio, J.M.; Crespo, J.; Arenas, J.; Fernandez, I.; Baliellas, C.; Carrion, J.A.; de la Mata, M.; et al. Treatment of hepatitis C virus infection in patients with cirrhosis and predictive value of model for end-stage liver disease: Analysis of data from the Hepa-C registry. Hepatology 2017, 65, 1810–1822. [Google Scholar] [CrossRef]
- Chatterjee, J.G.; Konar, A.; Bhattacharya, S. Outcome of decompensated hepatitis C cirrhosis with DAA—A tertiary care experience from Kolkata. J. Gastroenterol. Hepatol. 2019, 34, 121. [Google Scholar]
- Cheung, M.C.M.; Walker, A.J.; Hudson, B.E.; Verma, S.; McLauchlan, J.; Mutimer, D.J.; Brown, A.; Gelson, W.T.H.; MacDonald, D.C.; Agarwal, K.; et al. Outcomes after successful direct-acting antiviral therapy for patients with chronic hepatitis C and decompensated cirrhosis. J. Hepatol. 2016, 65, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Deterding, K.; Honer Zu Siederdissen, C.; Port, K.; Solbach, P.; Sollik, L.; Kirschner, J.; Mix, C.; Cornberg, J.; Worzala, D.; Mix, H.; et al. Improvement of liver function parameters in advanced HCV-associated liver cirrhosis by IFN-free antiviral therapies. Aliment. Pharmacol. Ther. 2015, 42, 889–901. [Google Scholar] [CrossRef] [PubMed]
- Garg, G.; Dixit, V.K.; Shukla, S.K.; Singh, S.K.; Sachan, S.; Tiwari, A.; Yadav, V.K.; Yadav, D.P. Impact of Direct Acting Antiviral Drugs in Treatment Naive HCV Cirrhosis on Fibrosis and Severity of Liver Disease: A Real Life Experience from a Tertiary Care Center of North India. J. Clin. Exp. Hepatol. 2018, 8, 241–249. [Google Scholar] [CrossRef]
- Goel, A.; Bhargava, R.; Rai, P.; Aggarwal, R. Treatment of chronic genotype-3 hepatitis C virus infection using direct-acting antiviral agents: An Indian experience. Indian J. Gastroenterol. 2017, 36, 227–234. [Google Scholar] [CrossRef]
- Gupta, S.; Rout, G.; Patel, A.H.; Mahanta, M.; Kalra, N.; Sahu, P.; Sethia, R.; Agarwal, A.; Ranjan, G.; Kedia, S.; et al. Efficacy of generic oral directly acting agents in patients with hepatitis C virus infection. J. Viral. Hepat. 2018, 25, 771–778. [Google Scholar] [CrossRef]
- Moussa, M.; Ibrahim, H.; Sakr, A. Response and safety of treatment of chronic hepatitis C by direct-acting antiviral drugs in patients with Child B-related cirrhosis. Menoufia Med. J. 2021, 34. [Google Scholar] [CrossRef]
- Jacobson, I.M.; Poordad, F.; Firpi-Morell, R.; Everson, G.T.; Verna, E.C.; Bhanja, S.; Hwang, P.; Caro, L.; Robertson, M.; Charles, E.D.; et al. Elbasvir/Grazoprevir in People With Hepatitis C Genotype 1 Infection and Child-Pugh Class B Cirrhosis: The C-SALT Study. Clin. Transl. Gastroenterol. 2019, 10, e00007. [Google Scholar] [CrossRef]
- Kumada, T.; Toyoda, H.; Yasuda, S.; Tada, T.; Tanaka, J.; Chayama, K.; Johnson, P.J.; Irving, W.L. Comparison of the Prognosis of Decompensated Cirrhosis in Patients with and Without Eradication of Hepatitis C Virus. Infect. Dis. Ther. 2021, 10, 1001–1013. [Google Scholar] [CrossRef]
- Kwo, P.; Fried, M.W.; Reddy, K.R.; Soldevila-Pico, C.; Khemichian, S.; Darling, J.; Zamor, P.J.; Napoli, A.A.; Anduze-Faris, B.; Brown, R.S., Jr. Daclatasvir and sofosbuvir treatment of decompensated liver disease or post-liver transplant hepatitis C virus recurrence in patients with advanced liver disease/cirrhosis in a real-world cohort. Hepatol. Commun. 2018, 2, 354–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lens, S.; Fernandez, I.; Rodriguez-Tajes, S.; Hontangas, V.; Vergara, M.; Forne, M.; Calleja, J.L.; Diago, M.; Llaneras, J.; Llerena, S.; et al. Interferon-Free Therapy in Elderly Patients With Advanced Liver Disease. Am. J. Gastroenterol. 2017, 112, 1400–1409. [Google Scholar] [CrossRef]
- Lens, S.; Baiges, A.; Alvarado-Tapias, E.; LLop, E.; Martinez, J.; Fortea, J.I.; Ibanez-Samaniego, L.; Marino, Z.; Rodriguez-Tajes, S.; Gallego, A.; et al. Clinical outcome and hemodynamic changes following HCV eradication with oral antiviral therapy in patients with clinically significant portal hypertension. J. Hepatol. 2020, 73, 1415–1424. [Google Scholar] [CrossRef]
- Lim, J.K.; Liapakis, A.M.; Shiffman, M.L.; Lok, A.S.; Zeuzem, S.; Terrault, N.A.; Park, J.S.; Landis, C.S.; Hassan, M.; Gallant, J.; et al. Safety and Effectiveness of Ledipasvir and Sofosbuvir, With or Without Ribavirin, in Treatment-Experienced Patients With Genotype 1 Hepatitis C Virus Infection and Cirrhosis. Clin. Gastroenterol. Hepatol. 2018, 16, 1811–1819. [Google Scholar] [CrossRef] [PubMed]
- Lobato, C.M.O.; Codes, L.; Silva, G.F.; Souza, A.F.M.; Coelho, H.S.M.; Pedroso, M.L.A.; Parise, E.R.; Lima, L.; Borba, L.A.; Evangelista, A.S.; et al. Direct antiviral therapy for treatment of hepatitis C: A real-world study from Brazil. Ann. Hepatol. 2019, 18, 849–854. [Google Scholar] [CrossRef]
- Maan, R.; van Tilborg, M.; Deterding, K.; Ramji, A.; van der Meer, A.J.; Wong, F.; Fung, S.; Sherman, M.; Manns, M.P.; Cornberg, M.; et al. Safety and Effectiveness of Direct-Acting Antiviral Agents for Treatment of Patients With Chronic Hepatitis C Virus Infection and Cirrhosis. Clin. Gastroenterol. Hepatol. 2016, 14, 1821–1830. [Google Scholar] [CrossRef] [PubMed]
- Macken, L.; Gelson, W.; Priest, M.; Abouda, G.; Barclay, S.; Fraser, A.; Healy, B.; Irving, W.; Verma, S. Efficacy of direct-acting antivirals: UK real-world data from a well-characterised predominantly cirrhotic HCV cohort. J. Med. Virol. 2019, 91, 1979–1988. [Google Scholar] [CrossRef]
- Mandorfer, M.; Kozbial, K.; Schwabl, P.; Freissmuth, C.; Schwarzer, R.; Stern, R.; Chromy, D.; Stattermayer, A.F.; Reiberger, T.; Beinhardt, S.; et al. Sustained virologic response to interferon-free therapies ameliorates HCV-induced portal hypertension. J. Hepatol. 2016, 65, 692–699. [Google Scholar] [CrossRef]
- Mangia, A.; Lawitz, E.; Gane, E.; Conway, B.; Ruane, P.; Abergel, A.; McNabb, B.; Osinusi, A.; Chen, F.; Dvory-Sobol, H.; et al. Long-term follow-up of patients with chronic HCV infection and compensated or decompensated cirrhosis following treatment with sofosbuvir-based regimens. J. Hepatol. 2018, 68, S67–S68. [Google Scholar] [CrossRef]
- Mazzarelli, C.; Considine, A.; Childs, K.; Carey, I.; Manini, M.A.; Suddle, A.; Dusheiko, G.; Agarwal, K.; Cannon, M.D. Efficacy and Tolerability of Direct-Acting Antivirals for Hepatitis C in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 1339–1345. [Google Scholar] [CrossRef]
- Papatheodoridi, M.; Dalekos, G.N.; Goulis, J.; Manolakopoulos, S.; Triantos, C.; Zachou, K.; Koukoufiki, A.; Kappaourikou, A.; Zetaisimopoulos, K.; Tausoulas, C.; et al. Prioritization for interferon-free regimens and potential drug interactions of current direct-acting anti-hepatitis C agents in routine clinical practice. Ann. Gastroenterol. 2017, 30, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Pascasio, J.M.; Vinaixa, C.; Ferrer, M.T.; Colmenero, J.; Rubin, A.; Castells, L.; Manzano, M.L.; Lorente, S.; Testillano, M.; Xiol, X.; et al. Clinical outcomes of patients undergoing antiviral therapy while awaiting liver transplantation. J. Hepatol. 2017, 67, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Poordad, F.; Schiff, E.R.; Vierling, J.M.; Landis, C.; Fontana, R.J.; Yang, R.; McPhee, F.; Hughes, E.A.; Noviello, S.; Swenson, E.S. Daclatasvir with sofosbuvir and ribavirin for hepatitis C virus infection with advanced cirrhosis or post-liver transplantation recurrence. Hepatology 2016, 63, 1493–1505. [Google Scholar] [CrossRef]
- Ridruejo, E.; Cheinquer, H.; Marciano, S.; Mendizabal, M.; Pinero, F.; Wolff, F.H.; de Araujo, A.; Coelho Borges, S.; Kliemann, D.; Fleck, A.; et al. B.A.R.C.O.S. (Brazilian Argentine Hepatitis C Collaborative Observational Study): Effectiveness and clinical outcomes of HCV treatment with daclatasvir and sofosbuvir with or without ribavirin. J. Viral. Hepat. 2019, 26, 1200–1209. [Google Scholar] [CrossRef] [PubMed]
- Sanai, F.M.; Altraif, I.H.; Alswat, K.; AlZanbagi, A.; Babatin, M.A.; AlMousa, A.; Almutairi, N.H.; Aljawad, M.S.; Alghamdi, A.S.; Aljumah, A.A.; et al. Real life efficacy of ledipasvir/sofosbuvir in hepatitis C genotype 4-infected patients with advanced liver fibrosis and decompensated cirrhosis. J. Infect. 2018, 76, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Saxena, V.; Nyberg, L.; Pauly, M.; Dasgupta, A.; Nyberg, A.; Piasecki, B.; Winston, B.; Redd, J.; Ready, J.; Terrault, N.A. Safety and Efficacy of Simeprevir/Sofosbuvir in Hepatitis C-Infected Patients With Compensated and Decompensated Cirrhosis. Hepatology 2015, 62, 715–725. [Google Scholar] [CrossRef]
- Shiffman, M.L.; James, A.M.; Long, A.G.; Alexander, P.C. Treatment of chronic HCV with sofosbuvir and simeprevir in patients with cirrhosis and contraindications to interferon and/or ribavirin. Am. J. Gastroenterol. 2015, 110, 1179–1185. [Google Scholar] [CrossRef]
- Steinebrunner, N.; Stein, K.; Sandig, C.; Bruckner, T.; Stremmel, W.; Pathil, A. Predictors of functional benefit of hepatitis C therapy in a ‘real-life’ cohort. World J. Gastroenterol. 2018, 24, 852–861. [Google Scholar] [CrossRef]
- Tahata, Y.; Hikita, H.; Mochida, S.; Kawada, N.; Enomoto, N.; Ido, A.; Yoshiji, H.; Miki, D.; Hiasa, Y.; Takikawa, Y.; et al. Sofosbuvir plus velpatasvir treatment for hepatitis C virus in patients with decompensated cirrhosis: A Japanese real-world multicenter study. J. Gastroenterol. 2021, 56, 67–77. [Google Scholar] [CrossRef]
- Terrault, N.A.; Zeuzem, S.; Di Bisceglie, A.M.; Lim, J.K.; Pockros, P.J.; Frazier, L.M.; Kuo, A.; Lok, A.S.; Shiffman, M.L.; Ben Ari, Z.; et al. Effectiveness of Ledipasvir-Sofosbuvir Combination in Patients with Hepatitis C Virus Infection and Factors Associated With Sustained Virologic Response. Gastroenterology 2016, 151, 1131–1140. [Google Scholar] [CrossRef]
- Tmu, N.; Kumar, A.; Sharma, P.; Singla, V.; Bansal, N.; Arora, A. Results of Sofosbuvir Plus Ribavirin in Patients With Hepatitis C Related Decompensated Cirrhosis. J. Clin. Exp. Hepatol. 2019, 9, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Verna, E.C.; Morelli, G.; Terrault, N.A.; Lok, A.S.; Lim, J.K.; Di Bisceglie, A.M.; Zeuzem, S.; Landis, C.S.; Kwo, P.; Hassan, M.; et al. DAA therapy and long-term hepatic function in advanced/decompensated cirrhosis: Real-world experience from HCV-TARGET cohort. J. Hepatol. 2020, 73, 540–548. [Google Scholar] [CrossRef]
- Wei, J.; Mei, Y.; Li, J.; Yuan, J.; Yang, X.; Xu, Z.; Lin, G.; Zhang, J.; Zhao, Z.; Zhang, X. Efficacy and safety of direct-acting antiviral agent regimens in a real-world cohort of adult Chinese patients with chronic hepatitis C virus infection. Liver Res. 2020, 4, 101–107. [Google Scholar] [CrossRef]
- Welzel, T.M.; Petersen, J.; Herzer, K.; Ferenci, P.; Gschwantler, M.; Wedemeyer, H.; Berg, T.; Spengler, U.; Weiland, O.; van der Valk, M.; et al. Daclatasvir plus sofosbuvir, with or without ribavirin, achieved high sustained virological response rates in patients with HCV infection and advanced liver disease in a real-world cohort. Gut 2016, 65, 1861–1870. [Google Scholar] [CrossRef] [PubMed]
- Belli, L.S.; Berenguer, M.; Cortesi, P.A.; Strazzabosco, M.; Rockenschaub, S.R.; Martini, S.; Morelli, C.; Donato, F.; Volpes, R.; Pageaux, G.P.; et al. Delisting of liver transplant candidates with chronic hepatitis C after viral eradication: A European study. J. Hepatol. 2016, 65, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Belli, L.S.; Perricone, G.; Adam, R.; Cortesi, P.A.; Strazzabosco, M.; Facchetti, R.; Karam, V.; Salizzoni, M.; Andujar, R.L.; Fondevila, C.; et al. Impact of DAAs on liver transplantation: Major effects on the evolution of indications and results. An ELITA study based on the ELTR registry. J. Hepatol. 2018, 69, 810–817. [Google Scholar] [CrossRef]
- Bittermann, T.; Reddy, K.R. In the Era of Direct-Acting Antivirals, Liver Transplant Delisting Due to Clinical Improvement for Hepatitis C Remains Infrequent. Clin. Gastroenterol. Hepatol. 2021, 19, 2389–2397.e2. [Google Scholar] [CrossRef]
- Curry, M.P.G.E.; Manns, M.; McCaughan, G.; Peck-Radosavljevic, M.; Van Vlierberghe, H.; Denning, J.; Brainard, D.M.; McHutchison, J.G.; Kumar, P. LDV/SOF+RBV in HCV patients with decompensated cirrhosis or liver transplantation: Data from the SOLAR-1 and-2 trials. Transplantation 2016, 100, S77–S262. [Google Scholar] [CrossRef]
- Debnath, P.; Chandnani, S.; Rathi, P.; Nair, S.; Junare, P.; Udgirkar, S.; Singh, A.; Contractor, Q. A new model to predict response to direct-acting antiviral therapy in decompensated cirrhotics due to hepatitis C virus. Clin. Exp. Hepatol. 2020, 6, 253–262. [Google Scholar] [CrossRef]
- El-Sherif, O.; Jiang, Z.G.; Tapper, E.B.; Huang, K.C.; Zhong, A.; Osinusi, A.; Charlton, M.; Manns, M.; Afdhal, N.H.; Mukamal, K.; et al. Baseline Factors Associated With Improvements in Decompensated Cirrhosis After Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection. Gastroenterology 2018, 154, 2111–2121.e8. [Google Scholar] [CrossRef]
- Flemming, J.A.; Kim, W.R.; Brosgart, C.L.; Terrault, N.A. Reduction in liver transplant wait-listing in the era of direct-acting antiviral therapy. Hepatology 2017, 65, 804–812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, I.; Scotto, R.; Coppola, C.; Staiano, L.; Amoruso, D.C.; De Simone, T.; Portunato, F.; De Pascalis, S.; Martini, S.; Macera, M.; et al. Treatment with direct-acting antivirals improves the clinical outcome in patients with HCV-related decompensated cirrhosis: Results from an Italian real-life cohort (Liver Network Activity-LINA cohort). Hepatol. Int. 2019, 13, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Hanafy, A.S.; Bassiony, M.A.; Basha, M.A.A. Management of HCV-related decompensated cirrhosis with direct-acting antiviral agents: Who should be treated? Hepatol. Int. 2019, 13, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Lourenco, M.S.; Zitelli, P.M.Y.; Cunha-Silva, M.; Oliveira, A.I.N.; Lima, R.G.R.; Souza, E.O.; Oliveira, C.P.; Seva-Pereira, T.; Carrilho, F.J.; Pessoa, M.G.; et al. Early liver function improvement following successful treatment of chronic hepatitis C in patients with decompensated cirrhosis: A real-life study. Clinics 2021, 76, e3186. [Google Scholar] [CrossRef]
- Manolakopoulos, S.; Akriviadis, E.; Vlachogiannakos, J.; Papageorgiou, M.V.; Kapatais, A.; Oikonomopoulou, M.; Papatheodoridis, G.V. The impact of direct acting antivirals (DAAs) in patients with decompensated liver disease (DLD) due to chronic hepatitis C (CHC). heraclis-a multicenter greek real world study. Hepatology 2017, 66, 838A–839A. [Google Scholar]
- McCaughan, G.W.; Thwaites, P.A.; Roberts, S.K.; Strasser, S.I.; Mitchell, J.; Morales, B.; Mason, S.; Gow, P.; Wigg, A.; Tallis, C.; et al. Sofosbuvir and daclatasvir therapy in patients with hepatitis C-related advanced decompensated liver disease (MELD >/= 15). Aliment. Pharmacol. Ther. 2018, 47, 401–411. [Google Scholar] [CrossRef]
- Modi, A.A.; Nazario, H.; Trotter, J.F.; Gautam, M.; Weinstein, J.; Mantry, P.; Barnes, M.; Habib, A.; McAfee, J.; Teachenor, O.; et al. Safety and efficacy of simeprevir plus sofosbuvir with or without ribavirin in patients with decompensated genotype 1 hepatitis C cirrhosis. Liver Transpl. 2016, 22, 281–286. [Google Scholar] [CrossRef]
- Essa, M.; Sabry, A.; Abdelsameea, E.; Tharwa, E.S.; Salama, M. Impact of new direct-acting antiviral drugs on hepatitis C virus-related decompensated liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2019, 31, 53–58. [Google Scholar] [CrossRef]
- Sandmann, L.; Dorge, P.; Wranke, A.; Vermehren, J.; Welzel, T.M.; Berg, C.P.; Grottenthaler, J.M.; Weiss, K.H.; Langel, J.; Sterneck, M.; et al. Treatment strategies for patients with decompensated liver cirrhosis due to hepatitis C virus infection eligible for liver transplantation: Real-life data from five German transplant centers. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1049–1056. [Google Scholar] [CrossRef]
- Yu, M.L.; Chuang, W.L. Treatment of chronic hepatitis C in Asia: When East meets West. J. Gastroenterol. Hepatol. 2009, 24, 336–345. [Google Scholar] [CrossRef]
- Feld, J.J.; Jacobson, I.M.; Hézode, C.; Asselah, T.; Ruane, P.J.; Gruener, N.; Abergel, A.; Mangia, A.; Lai, C.L.; Chan, H.L.; et al. Sofosbuvir and velpatasvir for HCV genotype 1, 2, 4, 5, and 6 Infection. N. Engl. J. Med. 2015, 373, 2599–2607. [Google Scholar] [CrossRef] [PubMed]
- Asselah, T.; Bourgeois, S.; Pianko, S.; Zeuzem, S.; Sulkowski, M.; Foster, G.R.; Han, L.; McNally, J.; Osinusi, A.; Brainard, D.M.; et al. Sofosbuvir/velpatasvir in patients with hepatitis C virus genotypes 1-6 and compensated cirrhosis or advanced fibrosis. Liver Int. 2018, 38, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Zignego, A.L.; Monti, M.; Gragnani, L. Sofosbuvir/Velpatasvir for the treatment of Hepatitis C Virus infection. Acta Biomed. 2018, 89, 321–331. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Location | Publication Type | Study Design | Total Patients | Age (Years) | Gender (Male) | Prior Treatment (%) | CC | DC | GT | DAA | PI-Based (≥20%) | FU Period | References * |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Afdhal, 2017 | Worldwide | Original | Prospective | 50 | 55 (43–69) | 76% | 68% | 18 | 32 | 1–4 | SOF/RBV | No | NA | [18] |
| Alonso, 2017 | Spain | Original | Retrospective | 208 | 55 ± 8 | 82% | 47% | 166 | 42 | 3 | SOF/LDV ± RBV, SOF/DCV ± RBV | No | 12 wks | [19] |
| Backus, 2016 | China | Original | Retrospective | 6542 | 61.4 ± 6.2 (24.5–90.8) | 96% | 24% | 6333 | 209 | 1 | LDV/SOF ± RBV, PTV/r/DSV/RBV | No | NA | [20] |
| Berkan-Kawińska, 2021 | Europe | Original | Prospective | 2713 | 59 (50–65) | 54% | 41% | 2397 | 316 | 1–6 | LDV/SOF ± RBV, OBV/PTV/r ± DSV ± RBV, GRZ/EBR ± RBV, GLE/PIB, SOF/VEL ± RBV, SOF/DCV/RBV, SOF/IFN/RBV, SOF/RBV, ASV/DCV | Yes | At least 12 wks | [21] |
| Calleja, 2017 | Spain | Original | Retrospective | 3325 | 59.5 (21–87) | 55% | 45% | 2362 | 136 | 1 | OMV/PTV/r + DSV ± RBV, SOF/LDV ± RBV | No | 24 or 36 wks | [22] |
| Calvaruso, 2018 | Italy | Original | Prospective | 2249 | 65.4 ± 10.7 | 57% | 56% | 2035 | 214 | 1–4 | SOF/RBV, SOF/LDV ± RBV, SOF/DCV ± RBV, SOF/SIM ± RBV, OBV/PTV/r ± RBV, OBV/PTV/r/DSV ± RBV | No | 14 (6–24) mo | [23] |
| Carrillo, 2017 | Spain | Original | Retrospective | 739 | 55 (36–80) | 67% | 60% | 564 | 175 | 1/3 | SOF/SIM, SOF/DCV, SOF/LDV OBV/PTV/r/DSV, SIM/DCV | Yes | 12 wks | [24] |
| Chatterjee, 2019 | India | Abstract | Prospective | 50 | 55 | 62% | 28% | 21 | 29 | 1/3 | SOF/LDV/DCV, SOF/VEL ± RBV | No | 2 yrs | [25] |
| Cheung, 2016 | UK | Original | Prospective | 406 | 54 (28–79) | NA | NA | 70 | 406 | 1/3 | SOF/LDV ± RBV, SOF/DCV ± RBV | No | 15 mo | [26] |
| Deterding, 2015 | Germany | Original | Prospective | 80 | 57 ± 9 (range 38–79) | 59% | 68% | 45 | 34 | 1–4 | SOF/RBV 56, SOF/SIM ± RBV, SOF/DCV ± RBV | NA | 12 wks | [27] |
| Garg, 2018 | India | Original | Prospective | 63 | 47.2 ± 11.51 (32–75) | 56% | 0 | 33 | 30 | 3 | SOF/LDV ± RBV | No | 15 mo | [28] |
| Goel, 2017 | India | Original | Prospective | 160 | 45 (18–75) | 39% | 10% | 31 (CHC79) | 51 | 3 | SOF/RBV, SOF/DCV, SOF/DCV/RBV | No | 12/24 wks | [29] |
| Gupta, 2018 | India | Original | Prospective | 490 | 38.9 ± 12.7 | 57% | 12% | 120 (CHC339) | 31 | 1–4 | SOF/RBV, SOF/RBV/IFN, SOF/DCV, SOF/DCV/RBV | No | 12 wks | [30] |
| Ibrahim, 2021 | Egypt | Original | Retrospective | 601 | 50.54 ± 12.82 | 37% | 18% | 275 | 326 | 4 | DAA | NA | 12 wks | [31] |
| Jacobson, 2019 | USA | Original | Prospective | 40 | 58.3 ± 7 | 57% | 37% | 10 | 30 | 1 | EBR/GZR | Yes | 12 wks | [32] |
| Krassenburg, 2020 | Worldwide | Original | Retrospective | 868 | 59 (54–65) | 64% | 12% | 719 | 149 | 1–6 | NS3/4 NS5A NS3/4 NS5B NS3/4 NS5A/B NS5B NS5A/B | No | 28 (IQR 20–36) | [8] |
| Kumada, 2021 | UK and Japan | Original | Prospective | 364 | 54 (48–59) | 72% | 0 | 50 | 314 | 1–4 | LDV/SOF ± RBV, SOF/DCV ± RBV | No | 1.75 (0.71–3.05) yrs | [33] |
| Kwo, 2018 | USA | Original | Retrospective | 77 | 61 (34–79) | 78% | 56% | 63 | 14 | 1–3 | DCV/SOF ± RBV | No | 24 wks | [34] |
| Lens, 2017 | Spain | Original | Retrospective | 922 | 72 (65–90) | 58% | 48% | 746 | 176 | 1–4 | SOF/RBV, LDV/SOF ± RBV, SOF/SIM ± RBV, DCV ± RBV, DCV/SIM ± RBV, PTV/OBV/RBV, OBV/PTV/DSV ± RBV | NA | 12 wks | [35] |
| Lens, 2020 | Spain | Original | Prospective | 226 | 60 (53–69) | 53% | NA | 179 | 47 | 1–5 | LDV/SOF ± RBV, SOF/SIM ± RBV SOF/DCV ± RBV | NA | 24, 96 wks | [36] |
| Lim, 2018 | USA | Original | Prospective | 634 | >65 (153 (24%) | 66% | 100% | 383 | 251 | 1 | LDV/SOF ± RBV | No | 12 wks | [37] |
| Lobato, 2019 | Brazil | Original | Prospective | 3939 | 58 ± 10 | 60% | NA | 3703 | 236 | 1–6 | SOF/DCV, SOF/SIM, SOF/LDV, OBV/PTV/r/DSV ± RBV, SOF/RBV/PEG-IFN | NA | 12, 24 mo | [38] |
| Maan, 2016 | Worldwide | Original | Retrospective | 433 | 57.8 ± 8.7 | 64% | 65% | 319 | 114 | 1–5 | PI, DAA/RBV | Yes | 12 wks | [39] |
| Macken, 2019 | UK | Original | Prospective | 1448 | 54 (47–60) | 73% | 41% | 1344 | 104 | 1/3 | OBV/PTV/r/DSV ± RBV SOF/LDV ± RBV, SOF/DCV ± RBV, SOF/PEG/RBV | NA | 12 wks | [40] |
| Mandorfer, 2016 | Austria | Original | Retrospective | 120 | 52.6 ± 1.2 | 73% | NA | 60 | 60 | 1–4 | SOF/RBV, SOF/SIM, SOF/DCV, SOF/LDV, SIM/DCV | NA | 12 wks | [41] |
| Mangia, 2018 | Worldwide | Abstract | Prospective | 1545 | 59 (26–86) | 68% | NA | 1318 | 227 | NA | DAA | NA | 53 (<1–144) wks | [42] |
| Mazzarelli, 2018 | UK | Original | Retrospective | 113 | >65 | 53% | 61% | 101 | 12 | 1–4 | SOF/LDV ± RBV, SOF/DCV ± RBV, SOF/RBV, OBV/PTV/r ± DSV ± RBV | NA | 38 wks (12–132) | [43] |
| Papatheodoridis, 2017 | Greece | Abstract | Retrospective | 604 | 57 ± 11 | 58% | 67% | 386 (CHC158) | 60 | 1–5 | SOF/SIM ± RBV, SOF/DCV ± RBV, SOF/LDV ± RBV, 3D ± RBV, SOF/RBV ± pegIFNa, SOF/DCV ± RBV, 2D/RBV | Unknown | NA | [44] |
| Pascasio, 2017 | Spain | Original | Retrospective | 171 | 54 (51–61) | 81% | 49% | 17 | 154 | 1,3,4 | SOF/RBV, SOF/DCV ± RBV, SOF/SIM ± RBV, SOF/LDV ± RBV, 2D 3D ± RBV | No | NA | [45] |
| Poordad, 2016 | USA | Original | Prospective | 60 | 58 (19–75) | 63% | 60% | 12 | 48 | 1–6 | DCV/SOF/RBV | No | 24 wks | [46] |
| Ridruejo, 2019 | Argentina | Original | Prospective | 906 | 60 ± 12 | 52% | 55% | 486 | 91 | 1–4 | SOF/DCV ± RBV | No | 22.3 mo | [47] |
| Sanai, 2018 | Arab | Original | Prospective | 213 | 59.6 ± 12.1 | 41% | 40% | 165 | 48 | 4 | SOF/LDV ± RBV | No | 12 wks | [48] |
| Saxena, 2015 | USA | Original | Retrospective | 156 | 61 (58–64) | 61% | 55% | 101 | 55 | 1 | SOF/SIM ± RBV | Yes | 12 wks | [49] |
| Shiffman, 2015 | USA | Original | Retrospective | 120 | 60 (29–79) | 63% | 51% | 81 | 39 | 1 | SIM/SOF | NA | 24 mo | [50] |
| Steinebrunner, 2018 | Germany | Original | Retrospective | 199 | 59 ± 10, (27–83) | 67% | 56% | 152 | 47 | 1–4 | SOF/LDV ± RBV, PTV/r/OMV/DSV ± RBV | NA | 12 wks | [51] |
| Tahata, 2021 | Japan | Original | Prospective | 190 | 68 (40–87) | 52% | 57% | 108 | 82 | 1–4 | LDV/SOF, EBR/GZR, GLE/PIB, SOF/RBV, SOF/VEL ± RBV | No | 12 wks | [52] |
| Terrault, 2016 | USA | Original | Prospective | 2255 | 60 (18–87) | 60% | 50% | 917 (CHC924) | 414 | 1 | SOF/LDV/RBV | No | 12 | [53] |
| Tmu, 2019 | India | Original | Retrospective | 103 | 50 (29–82) | 64% | 18% | 28 (CHC28) | 47 | 1,2 | SOF/RBV | No | 12 wks | [54] |
| Verna, 2020 | Worldwide | Original | Prospective | 642 | 60 (25–89) | 68% | 65% | 178 | 393 | 4 | SOF/LDV, SOF/DCV, SOF/Vel, EBR/GZR | No | 12 wks | [55] |
| Wei, 2020 | China | Original | Prospective | 222 | 58.9 ± 10.7 | 50% | 9% | 31 (CHC165) | 26 | 1–6 | OBV/PTV/r/DSV, SOF/DCV ± RBV, SOF/VEL ± RBV, SOF/RBV, EBR/GZR, DCV/ASV, GLE/PIB ± RBV | No | Median, 36 wks | [56] |
| Welzel, 2016 | Germany | Original | Retrospective | 485 | 57 (27–87) | 66% | 70% | 223 (CHC97) | 165 | 1–5 | DCV/SOF ± RBV | No | 12 wks | [57] |
| Belli, 2016 | Europe | Original | Retrospective | 103 | 54 (34–71) | 68% | NA | 0 | 103 | 1–3 | SOF/RBV, SOF/DCV ± RBV, SOF/LDV ± RBV, SOF/SIM ± RBV | No | 51.9 (32.9–67.4) wks | [58] |
| Belli, 2018 | Europe | Original | Retrospective | 36,382 | 54 (34–71) | 69% | NA | 0 | 36,382 | NA | Protease inhibitor | NA | NA | [59] |
| Bittermann, 2021 | USA | Original | Retrospective | 8394 | 57 (53–61) | 70% | NA | 0 | 8394 | NA | DAA | NA | [60] | |
| Charlton, 2015 | USA | Original | Prospective | 108 | 59 (55–62) | 67% | 65% | 0 | 108 | 1 | SOF/LDV/RBV | No | NA | [9] |
| Curry, 2015 | USA | Original | Prospective | 267 | 58 (40–73) | 70% | 55% | 0 | 267 | 1–6 | SOF/Vel ± RBV | No | 12 wks | [5] |
| Curry, 2016 | Worldwide | Abstract | Prospective | 667 | NA | NA | NA | 0 | 667 | 1/4 | SOF/LDV | No | 12 wks | [61] |
| Debnath, 2019 | India | Abstract | Retrospective | 62 | Median 48 | 54% | NA | 0 | 62 | NA | SOF/DCV, LDV Vel ± RBV | No | 24 wks | [62] |
| El-Sherif, 2018 | Worldwide | Original | Retrospective | 622 | 59 (54–62) | 72% | NA | 0 | 622 | 1–4 | SOF/LDV/RBV, Vel/SOF ± RBV, SOF + RBV | No | 255 (251–236) days | [63] |
| Flemming, 2017 | USA | Original | Retrospective | 47,591 | 56 (IQR, 51–61) | 71% | NA | 0 | 33,947 | NA | DAA, PI | NA | NA | [64] |
| Foster, 2016 | UK | Original | Prospective | 409 | 54 (28–80) | 73% | 61% | 0 | 409 | 1/3 | SOF/LDV ± RBV, SOF/DCV ± RBV | No | 12 wks | [26] |
| Gentile, 2019 | Italy | Original | Prospective | 89 | 72 (67–76) | 46% | 42% | 0 | 89 | 1–4 | SOF/LDV SOF/RBV SOF/DCV | No | 11 months | [65] |
| Hanafy, 2019 | Egypt | Original | Retrospective | 160 | 51.4 ± 6.3 | 78% | 0 | 0 | 160 | 4 | SOF/DCV/RBV | No | 29.3 ± 1.9 mo | [66] |
| Lin, 2018 | China | Abstract | Retrospective | 56 | 63.6 ± 8.1 | 39% | 24% | 0 | 56 | 1–3 | DAA | NA | 12.5 ± 7.3 months | [63] |
| Lourenco, 2021 | Brazil | Original | Retrospective | 85 | 56.13 ± 11.14 | 51% | 54% | 0 | 85 | 1–3 | SOF/DCV ± RBV, SOF/SIM ± RBV | No | 12–24 wks | [67] |
| Manolakopoulos, 2017 | Greece | Abstract | Retrospective | 126 | 59 ± 12.82 | 62% | 56% | 0 | 126 | 1–3 | SOF, SOF/SIM, SOF/DSV, SOF/LDV, 3D/2D, SOF/VEL, EBR/GZP | No | 12 wks | [68] |
| McCaughan, 2017 | Australia | Original | Prospective | 108 | 56 (51–61) | 73% | 40% | 0 | 108 | 1–4 | SOF/DCV ± RBV | No | 12 wks | [69] |
| Modi, 2016 | USA | Original | Prospective | 42 | 58 (32–69) | 74% | 52% | 0 | 42 | 1 | SOF/SIM ± RBV | Yes | 12 wks | [70] |
| Mohamed Essa, 2019 | Egypt | Original | Retrospective | 75 | >60.20 (26.7) | 69% | NA | 0 | 75 | NA | SOF/DCV, SOF/LDV ± RBV | No | 6 mo | [71] |
| Sandmann, 2018 | Worldwide | Original | Retrospective | 35 | 55.5 ± 8.97 | 80% | 54% | 0 | 35 | 1–4 | SOF/DCV ± RBV, SOF/SIM, SOF/LDV ± RBV, PTV/r/OBV/DSV | No | 18 (IQR 8–29) mo | [72] |
| Outcomes | No. of Studies | Pooled Event Rate | 95% CI | I2 (%) |
|---|---|---|---|---|
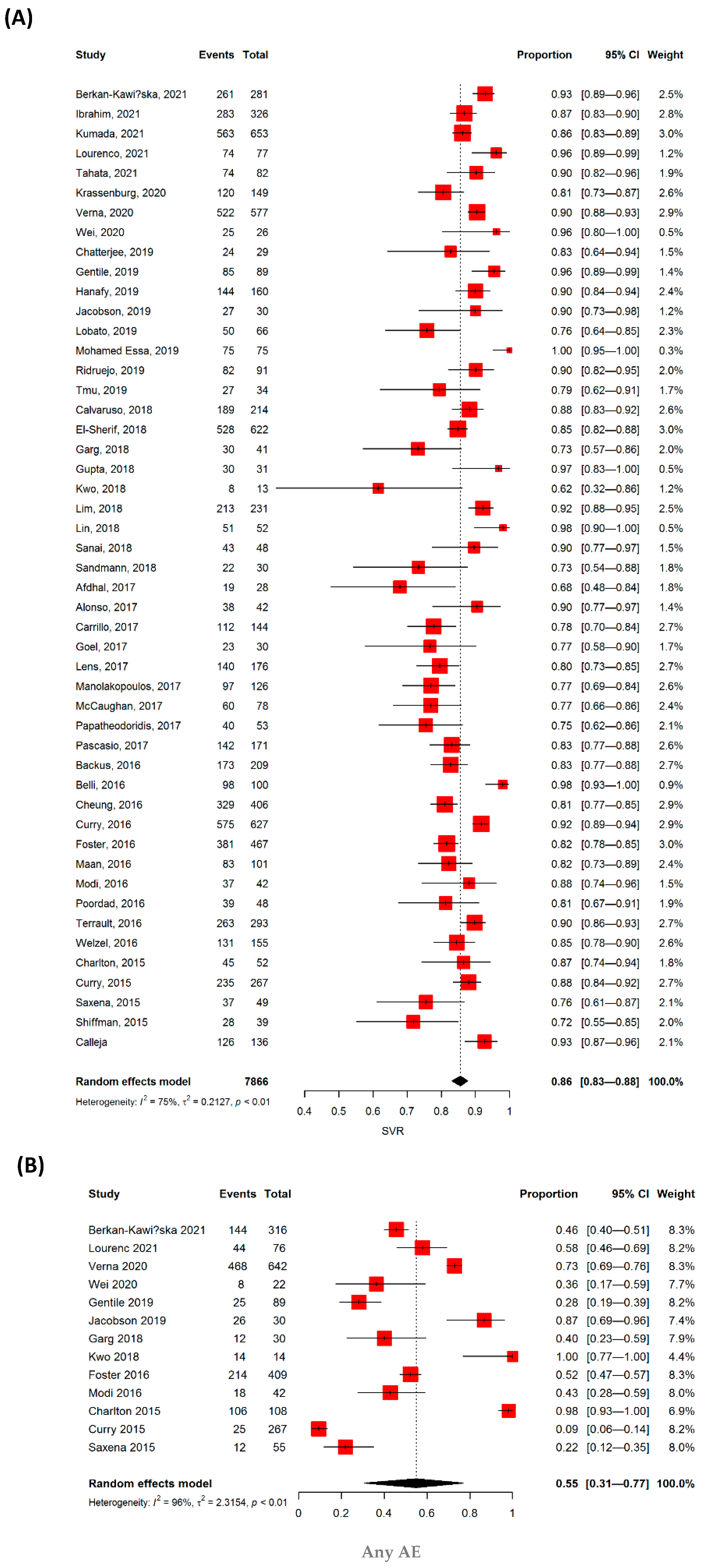
| SVR, overall | 49 | 0.86 | 0.83–0.88 | 68 |
| Age (years) | ||||
| ≥60 | 14 | 0.87 | 0.81–0.92 | 78.3 |
| <60 | 35 | 0.84 | 0.82–0.87 | 66.1 |
| Previous interferon treatment | ||||
| Yes | 3 | 0.85 | 0.83–0.88 | 71.9 |
| No | 11 | 0.88 | 0.79–0.93 | 82.6 |
| Protease inhibitor based | ||||
| Yes | 6 | 0.85 | 0.75–0.91 | 78.7 |
| No | 37 | 0.86 | 0.84–0.89 | 74.4 |
| Genotype | ||||
| GT 1 | 7 | 0.86 | 0.77–0.92 | 75.7 |
| GT 3 | 3 | 0.8 | 0.45–0.95 | 50.5 |
| GT 4 | 3 | 0.88 | 0.82–0.92 | 0 |
| GT Mixed | 35 | 0.85 | 0.82–0.88 | 77.1 |
| Study design | ||||
| Prospective | 25 | 0.86 | 0.83–0.89 | 70.9 |
| Retrospective | 23 | 0.84 | 0.80–0.88 | 73.1 |
| Industrial sponsorship | ||||
| Yes | 27 | 0.86 | 0.83–0.89 | 77.7 |
| No | 22 | 0.85 | 0.8–0.88 | 71 |
| Study region | ||||
| Asia | 9 | 0.87 | 0.77–0.93 | 57.6 |
| USA | 11 | 0.85 | 0.79–0.89 | 67.4 |
| Europe | 14 | 0.86 | 0.81–0.9 | 79.1 |
| Others | 15 | 0.86 | 0.8–0.88 | 71 |
| Outcomes | No. of Studies | Pooled Event Rate | 95% CI | I2 (%) |
|---|---|---|---|---|
| SVR, overall | 49 | 0.86 | 0.83–0.88 | 68 |
| Adverse effect | 13 | 0.55 | 0.31–0.77 | 96 |
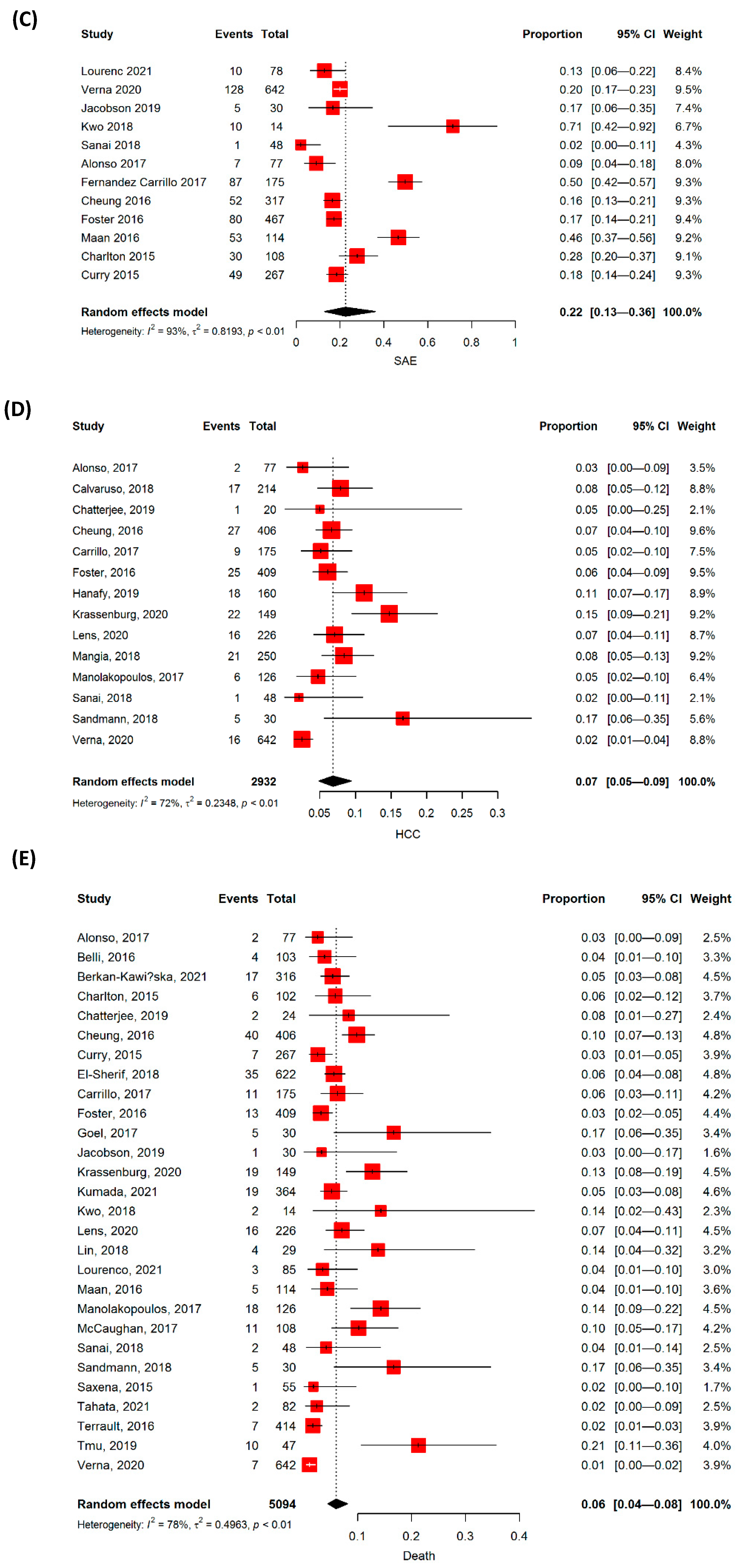
| Serious adverse effect | 12 | 0.22 | 0.13–0.36 | 93 |
| DAA discontinuation | 11 | 0.06 | 0.04–0.08 | 52 |
| Hepatocellular carcinoma | 14 | 0.07 | 0.05–0.09 | 72.2 |
| Mortality | 28 | 0.06 | 0.04–0.08 | 77.6 |
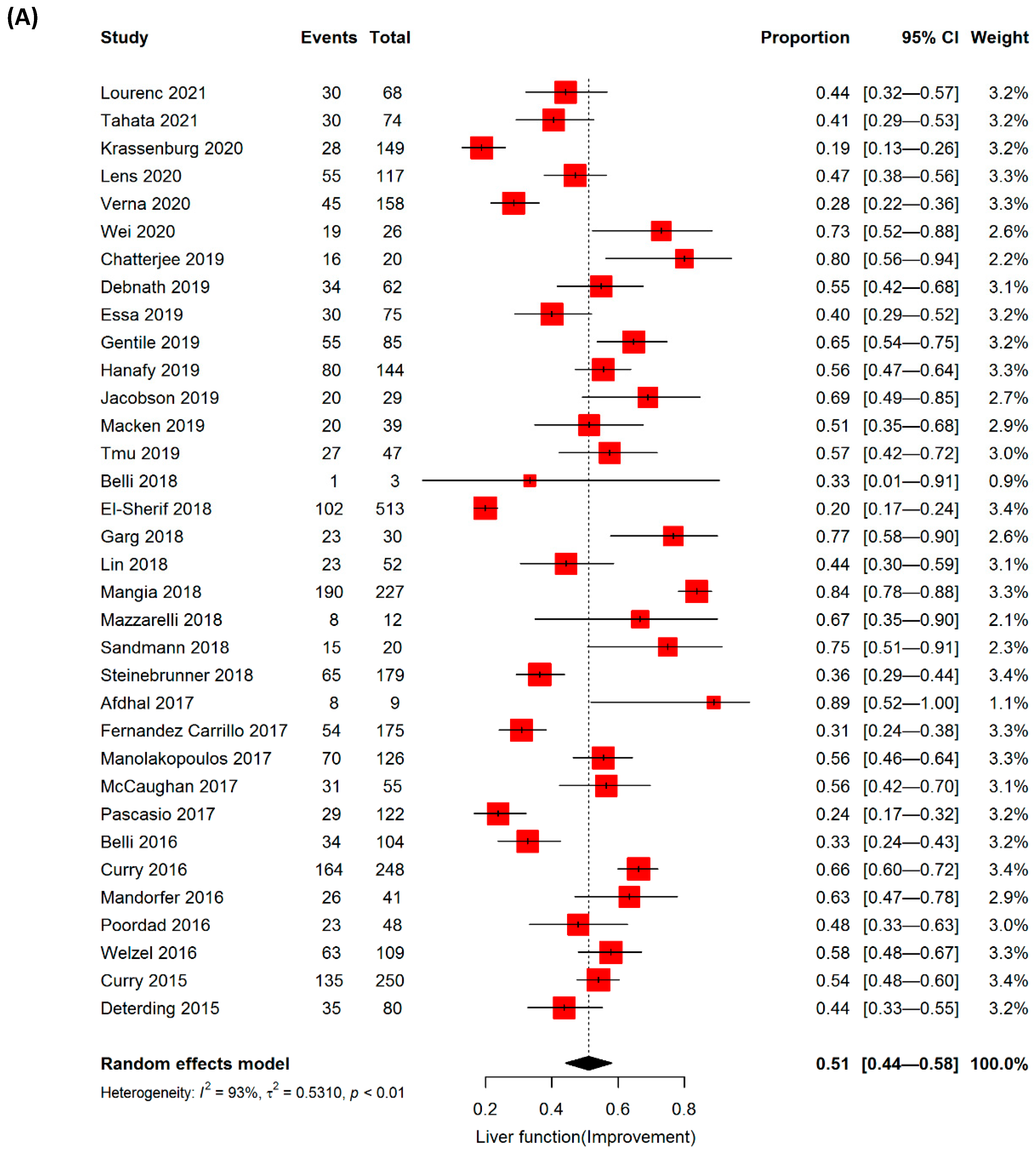
| Improvement in liver function | 34 | 0.51 | 0.44–0.58 | 93 |
| Worsening of liver function | 20 | 0.16 | 0.12–0.21 | 73 |
| Delisting from liver transplantation | 6 | 0.16 | 0.05–0.40 | 98.8 |
| Outcomes | No. of Studies | Pooled Event Rate | 95% CI | I2 (%) |
|---|---|---|---|---|
| Adverse effect | ||||
| Yes | 4 | 0.49 | 0.11–0.88 | 88.4 |
| No | 9 | 0.58 | 0.24–0.86 | 97.1 |
| Serious adverse effect | ||||
| Yes | 3 | 0.23 | 0.07–0.83 | 79.4 |
| No | 9 | 0.18 | 0.09–0.33 | 77.9 |
| Worsening of liver function | ||||
| Yes | 4 | 0.22 | 0.20–0.25 | 0 |
| No | 14 | 0.14 | 0.09–0.20 | 80.6 |
| Improvement in liver function | ||||
| Yes | 2 | 0.49 | 0–1.00 | 92.7 |
| No | 23 | 0.51 | 0.42–0.59 | 93.2 |
| Hepatocellular carcinoma | ||||
| Yes | 1 | 0.05 | 0.03–0.1 | NA |
| No | 11 | 0.07 | 0.04–0.1 | 77.8 |
| Mortality | ||||
| Yes | 5 | 0.05 | 0.04–0.07 | 0 |
| No | 21 | 0.06 | 0.04–0.09 | 82.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
An, J.; Park, D.A.; Ko, M.J.; Ahn, S.B.; Yoo, J.-J.; Jun, D.W.; Yim, S.Y. Direct-Acting Antivirals for HCV Treatment in Decompensated Liver Cirrhosis Patients: A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 1517. https://doi.org/10.3390/jpm12091517
An J, Park DA, Ko MJ, Ahn SB, Yoo J-J, Jun DW, Yim SY. Direct-Acting Antivirals for HCV Treatment in Decompensated Liver Cirrhosis Patients: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(9):1517. https://doi.org/10.3390/jpm12091517
Chicago/Turabian StyleAn, JiHyun, Dong Ah Park, Min Jung Ko, Sang Bong Ahn, Jeong-Ju Yoo, Dae Won Jun, and Sun Young Yim. 2022. "Direct-Acting Antivirals for HCV Treatment in Decompensated Liver Cirrhosis Patients: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 9: 1517. https://doi.org/10.3390/jpm12091517