
Correlations between Peak Nasal Inspiratory Flow, Acoustic Rhinometry, 4-Phase Rhinomanometry and Reported Nasal Symptoms
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
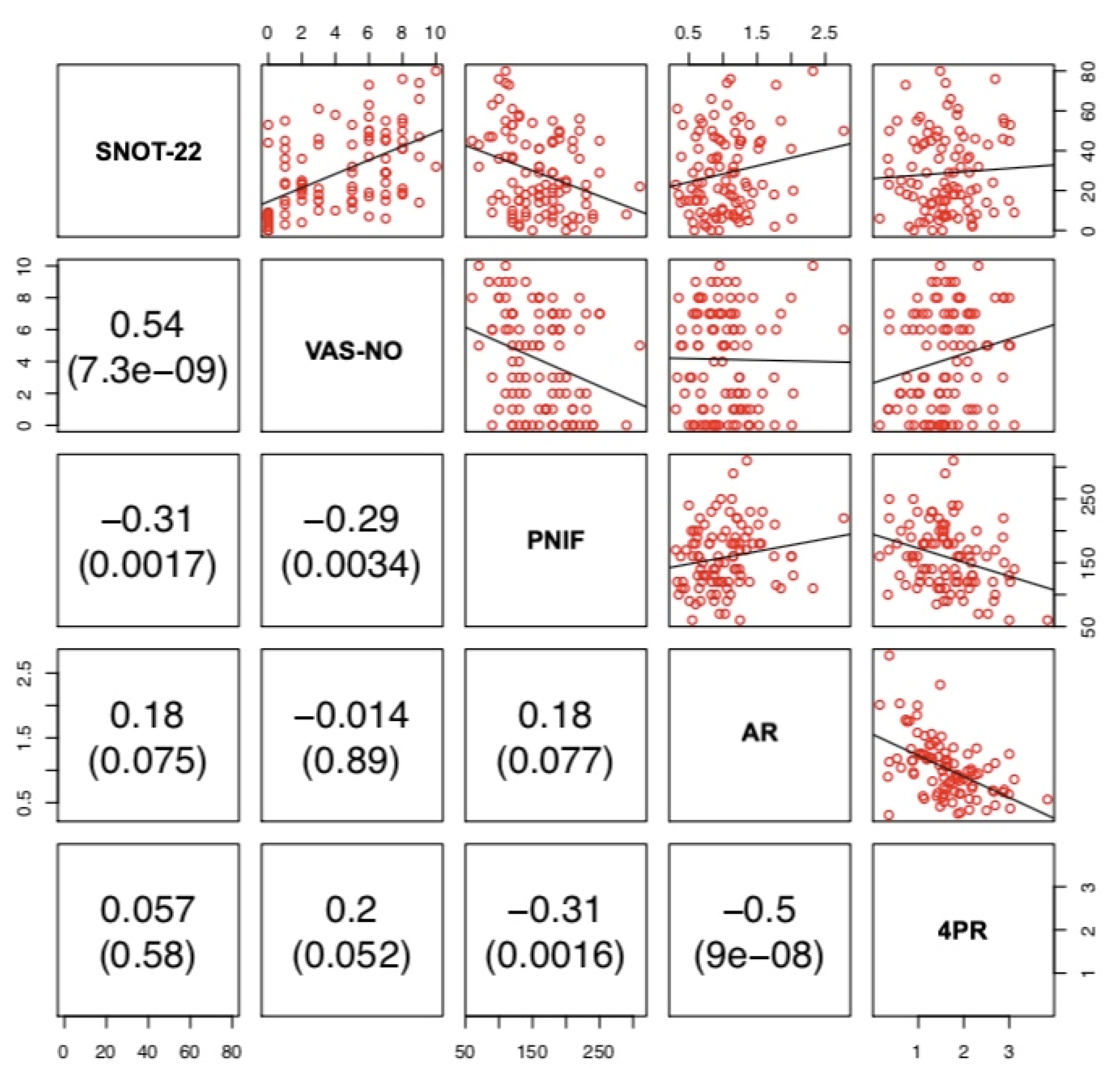
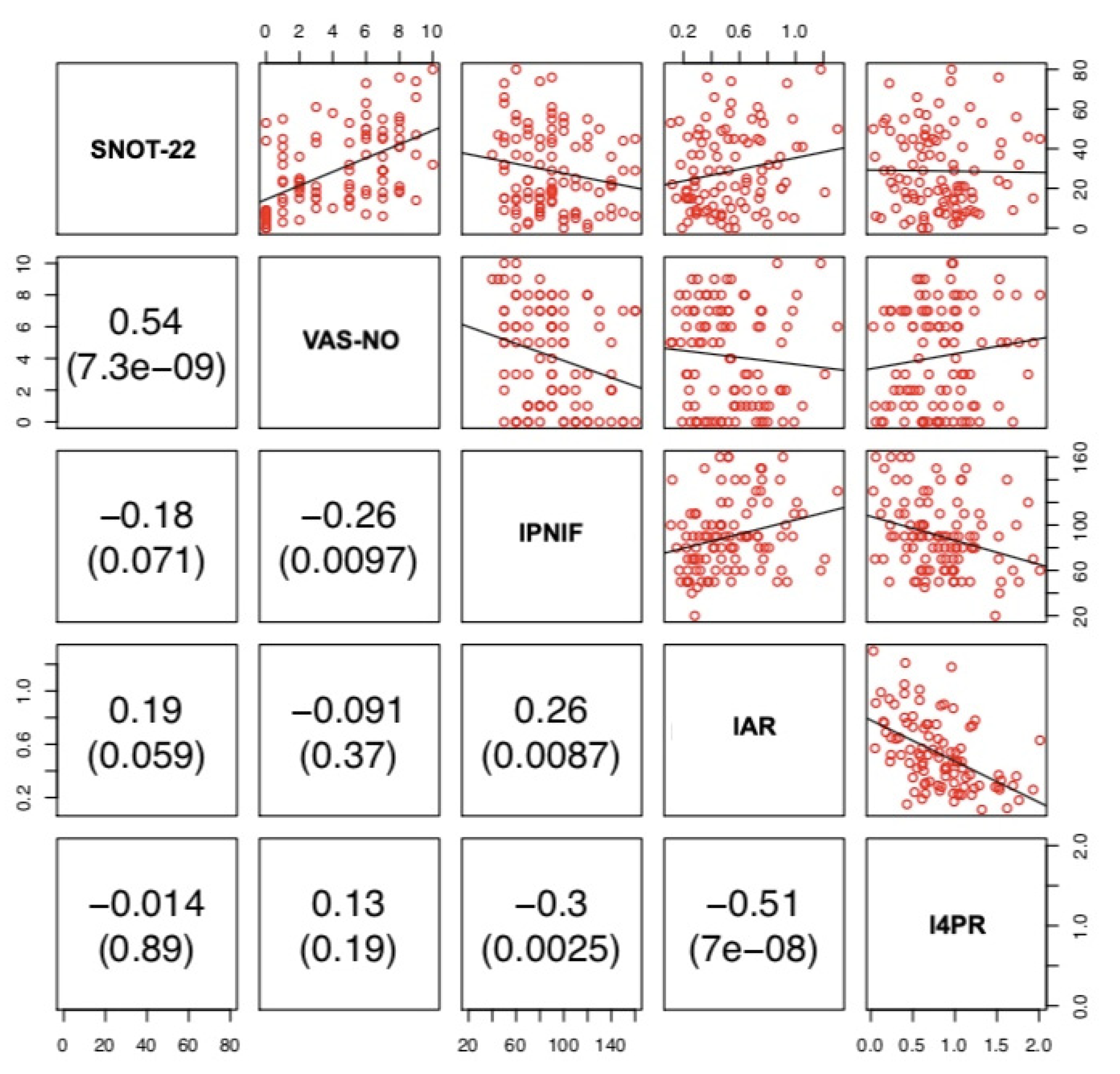
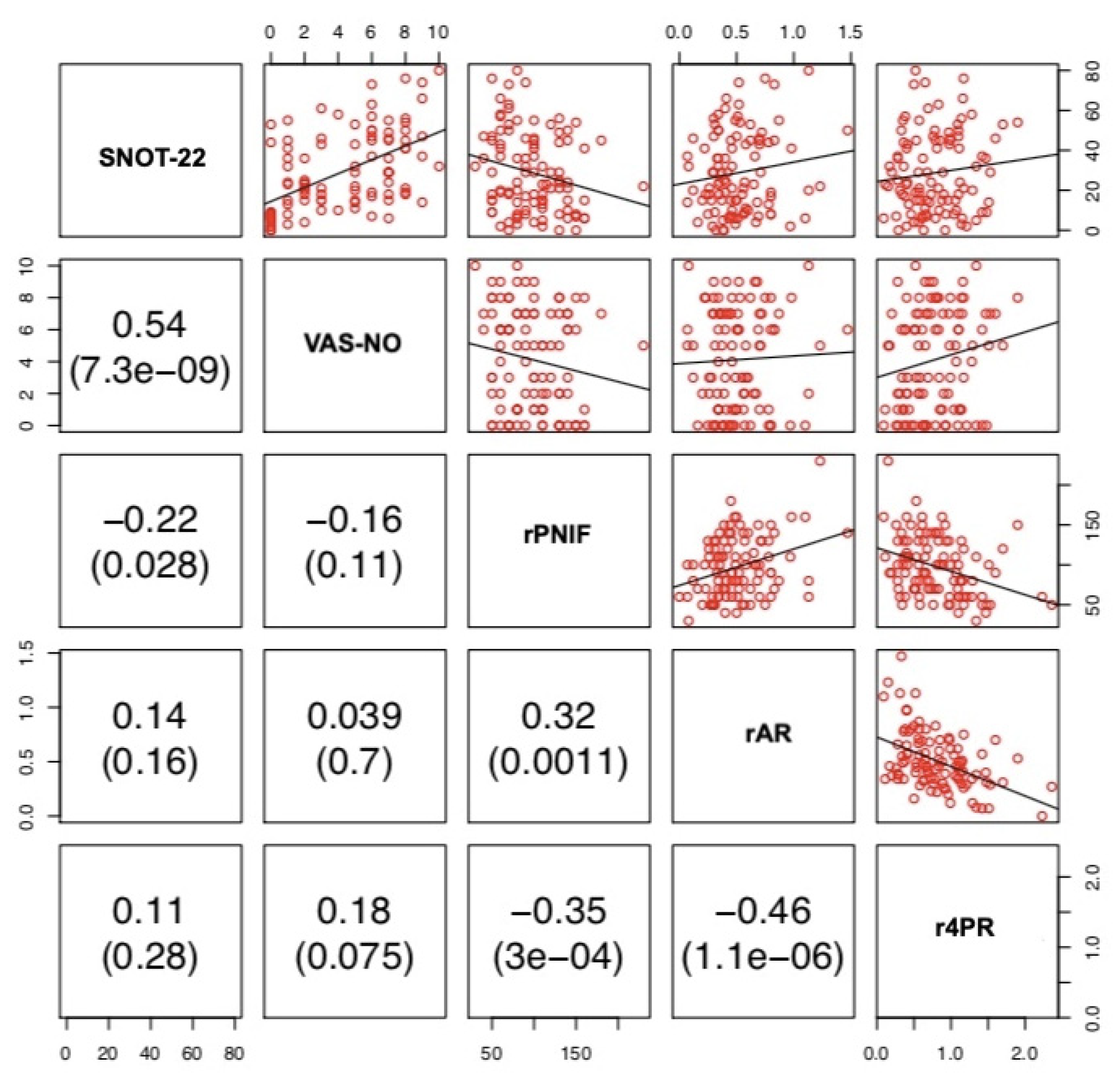
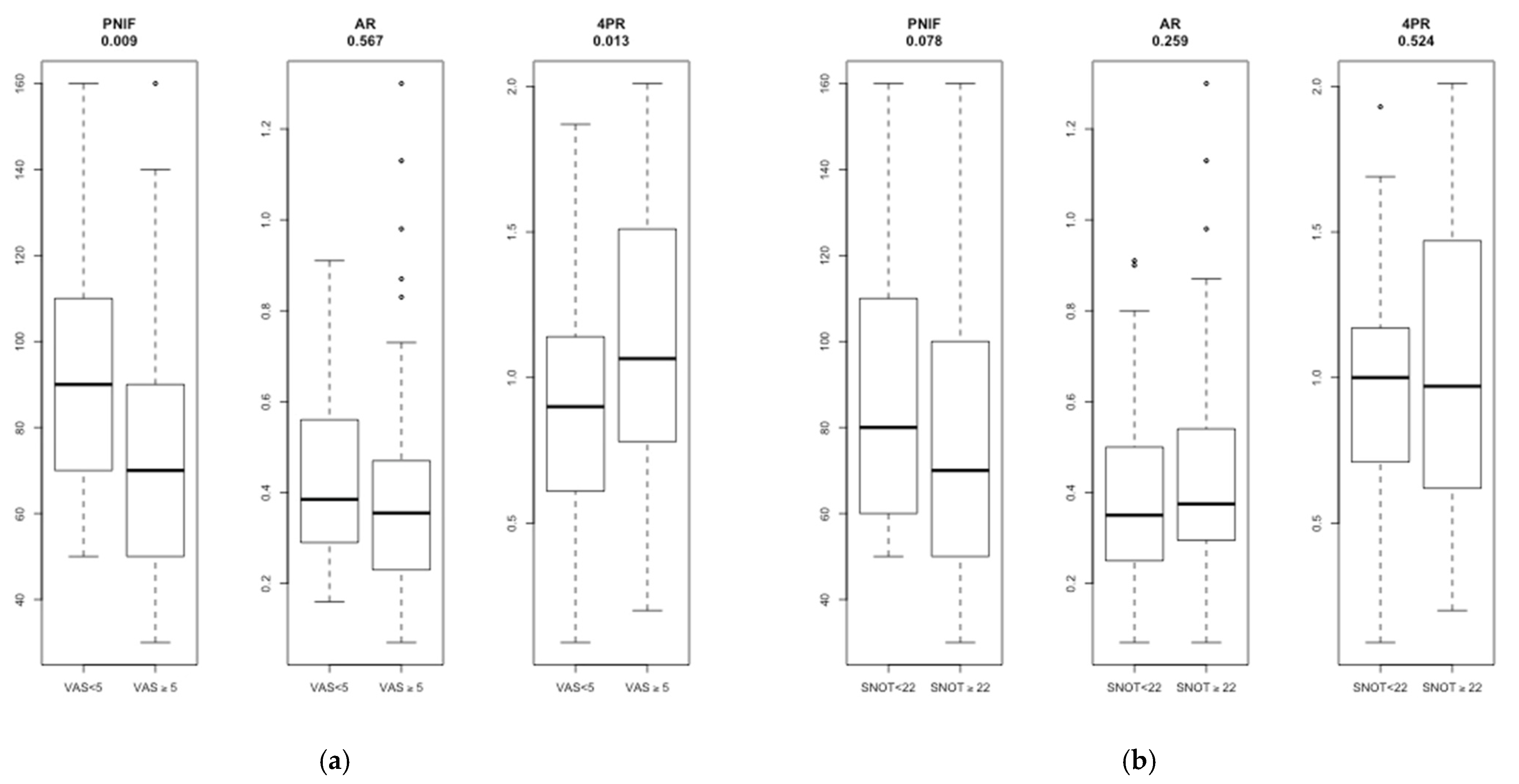
3. Results
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rimmer, J.; Hellings, P.; Lund, V.J.; Alobid, I.; Beale, T.; Dassi, C.; Douglas, R.; Hopkins, C.; Klimek, L.; Landis, B.; et al. European position paper on diagnostic tools in rhinology. Rhinology 2019, 57, 1–41. [Google Scholar] [CrossRef]
- Yepes-Nunez, J.J.; Bartra, J.; Munoz-Cano, R.; Sanchez-Lopez, J.; Serrano, C.; Mullol, J.; Alobid, I.; Sastre, J.; Picado, C.; Valero, A. Assessment of nasal obstruction: Correlation between subjective and objective techniques. Allergol. Et Immunopathol. 2013, 41, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Pendolino, A.L.; Nardello, E.; Lund, V.J.; Maculan, P.; Scarpa, B.; Martini, A.; Ottaviano, G. Comparison between unilateral PNIF and rhinomanometry in the evaluation of nasal cycle. Rhinology 2018, 56, 122–126. [Google Scholar] [CrossRef]
- Clarke, R.W.; Jones, A.S. The limitations of peak nasal flow measurement. Clin. Otolaryngol. Allied Sci. 1994, 19, 502–504. [Google Scholar] [CrossRef]
- Vogt, K.; Bachmann-Harildstad, G.; Lintermann, A.; Nechyporenko, A.; Peters, F.; Wernecke, K.D. The new agreement of the international RIGA consensus conference on nasal airway function tests. Rhinology 2018, 56, 133–143. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Hellings, P.W. Objective measurements of nasal function: Necessary before nasal surgery? Rhinology 2014, 52, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.S.; Willatt, D.J.; Durham, L.M. Nasal airflow: Resistance and sensation. J. Laryngol. Otol. 1989, 103, 909–911. [Google Scholar] [CrossRef]
- Kim, C.S.; Moon, B.K.; Jung, D.H.; Min, Y.G. Correlation between nasal obstruction symptoms and objective parameters of acoustic rhinometry and rhinomanometry. Auris Nasus Larynx 1998, 25, 45–48. [Google Scholar] [CrossRef]
- Szucs, E.; Clement, P.A. Acoustic rhinometry and rhinomanometry in the evaluation of nasal patency of patients with nasal septal deviation. Am. J. Rhinol. 1998, 12, 345–352. [Google Scholar] [CrossRef]
- Mozzanica, F.; Gera, R.; Bulgheroni, C.; Ambrogi, F.; Schindler, A.; Ottaviani, F. Correlation between Objective and Subjective Assessment of Nasal Patency. Iran. J. Otorhinolaryngol. 2016, 28, 313–319. [Google Scholar] [PubMed]
- Simola, M.; Malmberg, H. Sensation of nasal airflow compared with nasal airway resistance in patients with rhinitis. Clin. Otolaryngol. Allied Sci. 1997, 22, 260–262. [Google Scholar] [CrossRef] [PubMed]
- Ottaviano, G.; Pendolino, A.L.; Nardello, E.; Maculan, P.; Martini, A.; Russo, M.; Lund, V.J. Peak nasal inspiratory flow measurement and visual analogue scale in a large adult population. Clin. Otolaryngol. 2019, 44, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Hellings, P.W. Entering a new era of Predictive Medicine in Rhinology. Rhinology 2018, 56, 97–98. [Google Scholar] [CrossRef] [PubMed]
- Lund, V.J. Measuring the breath of life. Rhinology 2014, 52, 97–98. [Google Scholar] [CrossRef]
- Mozzanica, F.; Preti, A.; Gera, R.; Gallo, S.; Bulgheroni, C.; Bandi, F.; Ottaviani, F.; Castelnuovo, P. Cross-cultural adaptation and validation of the SNOT-22 into Italian. Eur. Arch. Otorhinolaryngol. 2017, 274, 887–895. [Google Scholar] [CrossRef]
- Ottaviano, G.; Scadding, G.K.; Coles, S.; Lund, V.J. Peak nasal inspiratory flow; normal range in adult population. Rhinology 2006, 44, 32–35. [Google Scholar]
- Ottaviano, G.; Scadding, G.K.; Scarpa, B.; Accordi, D.; Staffieri, A.; Lund, V.J. Unilateral peak nasal inspiratory flow, normal values in adult population. Rhinology 2012, 50, 386–392. [Google Scholar] [CrossRef]
- Ottaviano, G.; Fokkens, W.J. Measurements of nasal airflow and patency: A critical review with emphasis on the use of peak nasal inspiratory flow in daily practice. Allergy 2016, 71, 162–174. [Google Scholar] [CrossRef]
- Ottaviano, G.; Scadding, G.K.; Iacono, V.; Scarpa, B.; Martini, A.; Lund, V.J. Peak nasal inspiratory flow and peak expiratory flow. Upright and sitting values in an adult population. Rhinology 2016, 54, 160–163. [Google Scholar] [CrossRef]
- Pendolino, A.L.; Scarpa, B.; Ottaviano, G. Relationship Between Nasal Cycle, Nasal Symptoms and Nasal Cytology. Am. J. Rhinol. Allergy 2019, 33, 644–649. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doulaptsi, M.; Prokopakis, E.; Seys, S.; Pugin, B.; Steelant, B.; Hellings, P. Visual analogue scale for sino-nasal symptoms severity correlates with sino-nasal outcome test 22: Paving the way for a simple outcome tool of CRS burden. Clin. Transl. Allergy 2018, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Sami, A.S.; Scadding, G.K.; Howarth, P. A UK community-based survey on the prevalence of rhinosinusitis. Clin. Otolaryngol. 2018, 43, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Crivellaro, M.A.; Ottaviano, G.; Maculan, P.; Pendolino, A.L.; Vianello, L.; Mason, P.; Gioffre, F.; Bizzotto, R.; Scarpa, B.; Simoni, E.; et al. Upper and Lower Respiratory Signs and Symptoms in Workers Occupationally Exposed to Flour Dust. Int. J. Environ. Res. Public Health 2020, 17, 7075. [Google Scholar] [CrossRef]
- Gamerra, M.; Cantone, E.; Sorrentino, G.; De Luca, R.; Russo, M.B.; De Corso, E.; Bossa, F.; De Vivo, A.; Iengo, M. Mathematical model for preoperative identification of obstructed nasal subsites. Acta Otorhinolaryngol. Ital. 2017, 37, 410–415. [Google Scholar] [CrossRef]
- Clarke, J.D.; Eccles, R. Paradoxical sensation of nasal airflow in patients with common cold. Are we measuring the correct modality? Acta Otolaryngol. 2005, 125, 1307–1311. [Google Scholar] [CrossRef]
- Clement, P.A.; Halewyck, S.; Gordts, F.; Michel, O. Critical evaluation of different objective techniques of nasal airway assessment: A clinical review. Eur. Arch. Otorhinolaryngol. 2014, 271, 2617–2625. [Google Scholar] [CrossRef] [PubMed]
- van Egmond, M.; van Heerbeek, N.; Ter Haar, E.L.M.; Rovers, M.M. Clinimetric properties of the Glasgow Health Status Inventory, Glasgow Benefit Inventory, Peak Nasal Inspiratory Flow, and 4-Phase Rhinomanometry in adults with nasal obstruction. Rhinology 2017, 55, 126–134. [Google Scholar] [CrossRef]
- Numminen, J.; Ahtinen, M.; Huhtala, H.; Rautiainen, M. Comparison of rhinometric measurements methods in intranasal pathology. Rhinology 2003, 41, 65–68. [Google Scholar]
- Volstad, I.; Olafsson, T.; Steinsvik, E.A.; Dahl, F.A.; Skrindo, I.; Bachmann-Harildstad, G. Minimal unilateral peak nasal inspiratory flow correlates with patient reported nasal obstruction. Rhinology 2019, 57, 436–443. [Google Scholar] [CrossRef]
- Ottaviano, G.; Lund, V.J.; Nardello, E.; Scarpa, B.; Frasson, G.; Staffieri, A.; Scadding, K. Comparison between unilateral PNIF and rhinomanometry in healthy and obstructed noses. Rhinology 2014, 52, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.H.; Eccles, R. Comparison of classic and 4-phase rhinomanometry methods, is there any difference? Rhinology 2014, 52, 360–365. [Google Scholar] [CrossRef]
- Hirschberg, A.; Rezek, O. Correlation between objective and subjective assessments of nasal patency. ORL J. Otorhinolaryngol. Relat. Spec. 1998, 60, 206–211. [Google Scholar] [CrossRef]
- Whitcroft, K.L.; Andrews, P.J.; Randhawa, P.S. Peak nasal inspiratory flow correlates with quality of life in functional endoscopic sinus surgery. Clin. Otolaryngol. 2017, 42, 1187–1192. [Google Scholar] [CrossRef] [PubMed]
- Marioni, G.; Ottaviano, G.; Staffieri, A.; Zaccaria, M.; Lund, V.J.; Tognazza, E.; Coles, S.; Pavan, P.; Brugin, E.; Ermolao, A. Nasal functional modifications after physical exercise: Olfactory threshold and peak nasal inspiratory flow. Rhinology 2010, 48, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Fuller, J.C.; Gadkaree, S.K.; Levesque, P.A.; Lindsay, R.W. Peak nasal inspiratory flow is a useful measure of nasal airflow in functional septorhinoplasty. Laryngoscope 2019, 129, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Cherobin, G.B.; Voegels, R.L.; Pinna, F.R.; Gebrim, E.; Bailey, R.S.; Garcia, G.J.M. Rhinomanometry versus Computational Fluid Dynamics: Correlated, but Different Techniques. Am. J. Rhinol. Allergy 2021, 35, 245–255. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects (n = 101) | SNOT-22 ≥ 22 (n = 53) | VAS ≥ 5 (n = 50) | SNOT-22 ≥ 22 and VAS ≥ 5 (n = 36) | |
|---|---|---|---|---|
| Age, median [P25–P75], yr | 45 [27–58] | 47 [30–59] | 42 [27–56] | 46 [29–59] |
| Sex, No (%) | ||||
| Female | 43 (42.6%) | 28 (52.8%) | 19 (38%) | 17 (47.2%) |
| Male | 58 (57.4%) | 25 (47.2%) | 31 (62%) | 19 (52.8%) |
| Height, median [P25–P75], m | 1.72 [1.64–180] | 1.70 [1.60–1.80] | 1.73 [1.63–1.80] | 1.70 [1.60–1.80] |
| BMI, median [P25–P75], Kg/m2 | 23.8 [21.54–26.35] | 23.8 [21.6–26.6] | 24.1 [21.6–27] | 24.1 [21.6–26.3] |
| Allergy, No (%) | 50 (49.5%) | 28 (52.8%) | 28 (56%) | 19 (52.8%) |
| Asthma, No (%) | 24 (23.8%) | 13 (24.5%) | 11 (22%) | 7 (19.4%) |
| Smoke, No (%) | 13 (12.9%) | 3 (5.7%) | 5 (1%) | 2 (5.5%) |
| Reason for attendance, No (%) | ||||
| CRSsNP | 16 (15.8%) | 11 (20.7%) | 11 (22.0%) | 6 (16.0%) |
| CRSwNP | 30 (29.7%) | 15 (28.3%) | 8 (1.6%) | 9 (25.0%) |
| Nasal septal deviation | 26 (25.7%) | 15 (28.3%) | 17 (34.0%) | 12 (33.3%) |
| CRS + nasal septal deviation | 8 (7.9%) | 5 (9.4%) | 7 (1.4%) | 4 (11.1%) |
| Other | 21 (20.8%) | 6 (11.3%) | 6 (1.2%) | 4 (11.1%) |
| Nasal medications, No (%) | ||||
| Only steroid spray | 16 (15.8%) | 9 (17.0%) | 10 (20.0%) | 6 (16.7%) |
| Only douches (normal saline) | 13 (12.9%) | 7 (13.2%) | 7 (14.0%) | 6 (16.7%) |
| Steroid and douches (normal saline) | 26 (25.7%) | 13 (24.5%) | 10 (20.0%) | 7 (19.4%) |
| Previous nasal surgery, No (%) | ||||
| ESS | 25 (24.8%) | 13 (24.5%) | 9 (18.0%) | 6 (16.7%) |
| Septoplasty | 10 (9.9%) | 6 (11.3%) | 5 (10.0%) | 5 (13.9%) |
| Turbinoplasty | 2 (1.9%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| PNIF, median [P25–P75], L/min | 160 [120–190] | 150 [110–190] | 150 [110–180] | 125 [110–180] |
| 4PR, median [P25–P75], Pa/cm3·s | 1.59 [1.14–1.64] | 1.59 [1.04–1.99] | 1.74 [1.32–2.12] | 1.74 [1.27–2.12] |
| MCA, median [P25–P75], cm2 | 1 [0.67–1.24] | 1.03 [0.77–1.26] | 1.02 [0.65–1.17] | 0.94 [0.69–1.20] |
| SNOT-22, median [P25–P75] | 24 [12–45] | 45 [32–53] | 37 [20–50] | 45 [35–54] |
| VAS-NO, median [P25–P75] | 5 [1–7] | 6 [3–7] | 7 [6–8] | 7 [6–8] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ottaviano, G.; Pendolino, A.L.; Scarpa, B.; Torsello, M.; Sartori, D.; Savietto, E.; Cantone, E.; Nicolai, P. Correlations between Peak Nasal Inspiratory Flow, Acoustic Rhinometry, 4-Phase Rhinomanometry and Reported Nasal Symptoms. J. Pers. Med. 2022, 12, 1513. https://doi.org/10.3390/jpm12091513
Ottaviano G, Pendolino AL, Scarpa B, Torsello M, Sartori D, Savietto E, Cantone E, Nicolai P. Correlations between Peak Nasal Inspiratory Flow, Acoustic Rhinometry, 4-Phase Rhinomanometry and Reported Nasal Symptoms. Journal of Personalized Medicine. 2022; 12(9):1513. https://doi.org/10.3390/jpm12091513
Chicago/Turabian StyleOttaviano, Giancarlo, Alfonso Luca Pendolino, Bruno Scarpa, Miriam Torsello, Daniele Sartori, Enrico Savietto, Elena Cantone, and Piero Nicolai. 2022. "Correlations between Peak Nasal Inspiratory Flow, Acoustic Rhinometry, 4-Phase Rhinomanometry and Reported Nasal Symptoms" Journal of Personalized Medicine 12, no. 9: 1513. https://doi.org/10.3390/jpm12091513