

Effect of General Anesthesia Maintenance with Propofol or Sevoflurane on Fractional Exhaled Nitric Oxide and Eosinophil Blood Count: A Prospective, Single Blind, Randomized, Clinical Study on Patients Undergoing Thyroidectomy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Μethods
2.1. Study Population
2.2. Study Design and Anesthetic Management
2.3. Study Endpoints
2.4. Statistical Analysis
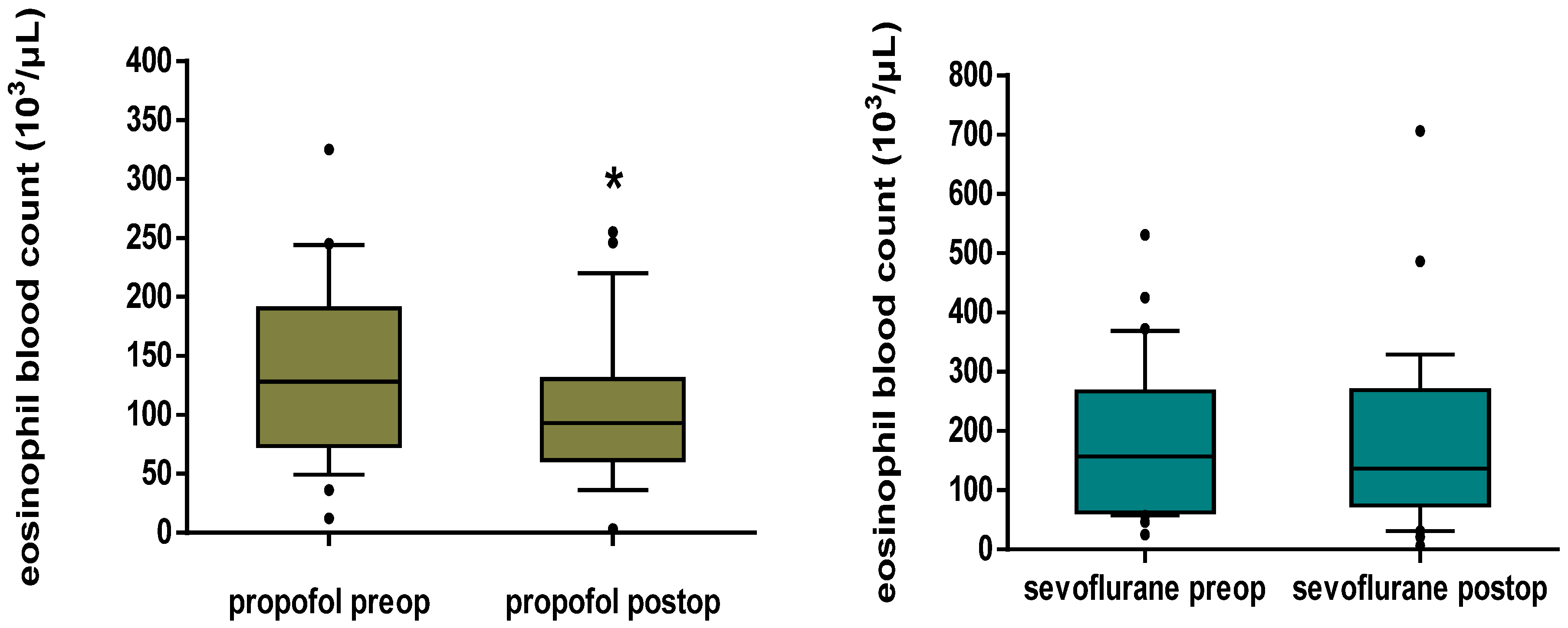
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maniscalco, M.; Sofia, M.; Pelaia, G. Nitric oxide in upper airways inflammatory diseases. Inflamm. Res. 2007, 56, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.B.; Punihaole, D.; Levine, T.B. Characterization of the Role of Nitric Oxide and Its Clinical Applications. Cardiology 2012, 122, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Panduri, V.; Weitzman, S.A.; Chandel, N.S.; Kamp, D.W. Mitochondrial-derived free radicals mediate asbestos-induced alveolar epithelial cell apoptosis. Am. J. Physiol. Cell. Mol. Physiol. 2004, 286, L1220–L1227. [Google Scholar] [CrossRef] [PubMed]
- Tufvesson, E.; Andersson, C.; Weidner, J.; Erjefält, J.S.; Bjermer, L. Inducible nitric oxide synthase expression is increased in the alveolar compartment of asthmatic patients. Allergy 2016, 72, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Radi, R. Immuno-spin trapping: A breakthrough for the sensitive detection of protein-derived radicals, a commentary on “Protein radical formation on thyroid peroxidase during turnover”. Free Radic. Biol. Med. 2006, 41, 416–417. [Google Scholar] [CrossRef] [PubMed]
- Bayable, S.D.; Melesse, D.Y.; Lema, G.F.; Ahmed, S.A. Perioperative management of patients with asthma during elective surgery: A systematic review. Ann. Med. Surg. 2021, 70, 102874. [Google Scholar] [CrossRef] [PubMed]
- Petsky, H.L.; Kew, K.M.; Turner, C.; Chang, A.B. Exhaled nitric oxide levels to guide treatment for adults with asthma. Cochrane Database Syst. Rev. 2016, 2016, CD011440. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Cowan, J.O.; Brassett, K.P.; Herbison, G.P.; Taylor, D.R. Use of Exhaled Nitric Oxide Measurements to Guide Treatment in Chronic Asthma. N. Engl. J. Med. 2005, 352, 2163–2173. [Google Scholar] [CrossRef]
- Saraiva-Romanholo, B.M.; Machado, F.S.; Almeida, F.M.; Nunes, M.D.P.T.; Martins, M.A.; Vieira, J.E. Non-Asthmatic Patients Show Increased Exhaled Nitric Oxide Concentrations. Clinics 2009, 64, 5–10. [Google Scholar] [CrossRef]
- Berry, M.A.; Shaw, D.E.; Green, R.H.; Brightling, C.E.; Wardlaw, A.J.; Pavord, I.D. The use of exhaled nitric oxide concentration to identify eosinophilic airway inflammation: An observational study in adults with asthma. Clin. Exp. Allergy 2005, 35, 1175–1179. [Google Scholar] [CrossRef]
- Warke, T.J.; Fitch, P.S.; Brown, V.; Taylor, R.; Lyons, J.D.M.; Ennis, M.; Shields, M.D. Exhaled nitric oxide correlates with airway eosinophils in childhood asthma. Thorax 2002, 57, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Li, W.; Pauluhn, J.; Trübel, H.; Wang, C. Rat models of acute lung injury: Exhaled nitric oxide as a sensitive, noninvasive real-time biomarker of prognosis and efficacy of intervention. Toxicology 2013, 310, 104–114. [Google Scholar] [CrossRef]
- Lee, R.P.; Wang, D.; Kao, S.J.; Chen, I.H. The Lung Is the Major Site That Produces Nitric Oxide to Induce Acute Pulmonary Oedema in Endotoxin Shock. Clin. Exp. Pharmacol. Physiol. 2001, 28, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J.; Kharitonov, A.S. Exhaled nitric oxide: A new lung function test. Thorax 1996, 51, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.-M.; Wu, G.-J.; Tai, Y.-T.; Sun, W.-Z.; Lin, Y.-L.; Jean, W.-C.; Chen, T.-L. Propofol reduces nitric oxide biosynthesis in lipopolysaccharide-activated macrophages by downregulating the expression of inducible nitric oxide synthase. Arch. Toxicol. 2003, 77, 418–423. [Google Scholar] [CrossRef]
- Liu, M.-C.; Tsai, P.-S.; Yang, C.-H.; Liu, C.-H.; Chen, C.-C.; Huang, C.-J. Propofol significantly attenuates iNOS, CAT-2, and CAT-2B transcription in lipopolysaccharide-stimulated murine macrophages. Acta Anaesthesiol. Taiwanica 2006, 44, 73–81. [Google Scholar]
- Chu, C.-H.; Liu, D.D.; Hsu, Y.-H.; Lee, K.-C.; Chen, I.H. Propofol exerts protective effects on the acute lung injury induced by endotoxin in rats. Pulm. Pharmacol. Ther. 2007, 20, 503–512. [Google Scholar] [CrossRef]
- Gao, J.; Zeng, B.; Zhou, L.; Yuan, S. Protective effects of early treatment with propofol on endotoxin-induced acute lung injury in rats. Br. J. Anaesth. 2004, 92, 277–279. [Google Scholar] [CrossRef]
- Krumholz, W.; Abdulle, O.; Knecht, J.; Hempelmann, G. Effects of i.v. anaesthetic agents on the chemotaxis of eosinophils in vitro. Br. J. Anaesth. 1999, 83, 333–335. [Google Scholar] [CrossRef]
- Bedirli, N.; Demirtas, C.Y.; Akkaya, T.; Salman, B.; Alper, M.; Bedirli, A.; Pasaoglu, H. Volatile anesthetic preconditioning attenuated sepsis induced lung inflammation. J. Surg. Res. 2012, 178, e17–e23. [Google Scholar] [CrossRef]
- Liu, R.; Ishibe, Y.; Ueda, M. Isoflurane–Sevoflurane Administration before Ischemia Attenuates Ischemia–Reperfusion-induced Injury in Isolated Rat Lungs. Anesthesiology 2000, 92, 833–840. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, U.G.; Moher, D.; CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society. Recommendations for standardized procedures for the on-line and off-line measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide in adults and children-1999. Am. J. Respir. Crit. Care Med. 1999, 160, 2104–2211. [Google Scholar] [CrossRef]
- American Thoracic Society; European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef] [PubMed]
- Pisi, R.; Aiello, M.; Tzani, P.; Marangio, E.; Olivieri, D.; Chetta, A. Measurement of Fractional Exhaled Nitric Oxide by a New Portable Device: Comparison with the Standard Technique. J. Asthma 2010, 47, 805–809. [Google Scholar] [CrossRef]
- Matthews, J.N.; Altman, D.G.; Campbell, M.J.; Royston, P. Analysis of serial measurements in medical research. BMJ 1990, 300, 230–235. [Google Scholar] [CrossRef]
- Gustafsson, L.; Leone, A.; Persson, M.; Wiklund, N.; Moncada, S. Endogenous nitric oxide is present in the exhaled air of rabbits, guinea pigs and humans. Biochem. Biophys. Res. Commun. 1991, 181, 852–857. [Google Scholar] [CrossRef]
- Alving, K.; Weitzberg, E.; Lundberg, J.M. Increased amount of nitric oxide in exhaled air of asthmatics. Eur. Respir. J. 1993, 6, 1368–1370. [Google Scholar] [PubMed]
- Silkoff, P.E.; McClean, P.; Spino, M.; Erlich, L.A.; Slutsky, A.S.; Zamel, N. Dose-Response Relationship and Reproducibility of the Fall in Exhaled Nitric Oxide After Inhaled Beclomethasone Dipropionate Therapy in Asthma Patients. Chest 2001, 119, 1322–1328. [Google Scholar] [CrossRef]
- Maniscalco, M.; Bianco, A.; Mazzarella, G.; Motta, A. Recent Advances on Nitric Oxide in the Upper Airways. Curr. Med. Chem. 2016, 23, 2736–2745. [Google Scholar] [CrossRef]
- Harnan, E.S.; Tappenden, P.; Essat, M.; Gomersall, T.; Minton, J.; Wong, R.; Pavord, I.; Everard, M.; Lawson, R. Measurement of exhaled nitric oxide concentration in asthma: A systematic review and economic evaluation of NIOX MINO, NIOX VERO and NObreath. Health Technol. Assess. 2015, 19, 820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahy, J.V. Type 2 inflammation in asthma—Present in most, absent in many. Nat. Rev. Immunol. 2015, 15, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Kharitonov, S.; Barnes, P. Clinical aspects of exhaled nitric oxide. Eur. Respir. J. 2000, 16, 781–792. [Google Scholar] [CrossRef] [PubMed]
- Soma, T.; Iemura, H.; Naito, E.; Miyauchi, S.; Uchida, Y.; Nakagome, K.; Nagata, M. Implication of fraction of exhaled nitric oxide and blood eosinophil count in severe asthma. Allergol. Int. 2018, 67, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Logotheti, H.; Pourzitaki, C.; Tsaousi, G.; Aidoni, Z.; Vekrakou, A.; Ekaterini, A.; Gourgoulianis, K. The role of exhaled nitric oxide in patients with chronic obstructive pulmonary disease undergoing laparotomy surgery—The noxious study. Nitric Oxide 2016, 61, 62–68. [Google Scholar] [CrossRef]
- Murphy, P.G.; Myers, D.S.; Davies, M.; Webster, N.R.; Jones, J.G. The antioxidant potential of propofol (2,6-DIISOPROPYLPHENOL). Br. J. Anaesth. 1992, 68, 613–618. [Google Scholar] [CrossRef]
- Aarts, L.; Van Der Hee, R.; Dekker, I.; De Jong, J.; Langemeijer, H.; Bast, A. The widely used anesthetic agent propofol can replace α-tocopherol as an antioxidant. FEBS Lett. 1995, 357, 83–85. [Google Scholar] [CrossRef]
- Chang, H.; Tsai, S.-Y.; Chang, Y.; Chen, T.-L.; Chen, R.-M. Therapeutic concentrations of propofol protects mouse macrophages from nitric oxide-induced cell death and apoptosis. Can. J. Anaesth. 2002, 49, 477–480. [Google Scholar] [CrossRef]
- González-Correa, J.A.; Cruz-Andreotti, E.; Arrebola, M.M.; López-Villodres, J.A.; Jódar, M.; De La Cruz, J.P. Effects of propofol on the leukocyte nitric oxide pathway: In vitro and ex vivo studies in surgical patients. Naunyn-Schmiedebergs Arch. Exp. Pathol. Pharmakol. 2008, 376, 331–339. [Google Scholar] [CrossRef]
- Chen, H.I.; Hsieh, N.-K.; Kao, S.J.; Su, C.-F. Protective effects of propofol on acute lung injury induced by oleic acid in conscious rats. Crit. Care Med. 2008, 36, 1214–1221. [Google Scholar] [CrossRef]
- Wang, D.; Wei, J.; Hsu, K.; Jau, J.-C.; Lieu, M.-W.; Chao, T.-J.; Chen, H.I. Effects of nitric oxide synthase inhibitors on systemic hypotension, cytokines and inducible nitric oxide synthase expression and lung injury following endotoxin administration in rats. J. Biomed. Sci. 1999, 6, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.-L.; Zhang, H.; Szabo, C.; Preiser, J.-C. Effects of Nitric Oxide in Septic Shock. Am. J. Respir. Crit. Care Med. 2000, 161, 1781–1785. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.F.; Zhu, Y.S.; Jiang, H.; Xu, H.; Sun, Y. Isoflurane Preconditioning Ameliorates Endotoxin-Induced Acute Lung Injury and Mortality in Rats. Anesthesia Analg. 2009, 109, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Helmy, S.A.K.; Wahby, M.A.M.; El-Nawaway, M. The effect of anaesthesia and surgery on plasma cytokine production. Anaesthesia 1999, 54, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-Y.; Meng, J.-X.; Liu, Z.; Liu, X.-W.; Huang, Y.-G.; Zhao, J. Propofol Attenuates Airway Inflammation in a Mast Cell-Dependent Mouse Model of Allergic Asthma by Inhibiting the Toll-like Receptor 4/Reactive Oxygen Species/Nuclear Factor κB Signaling Pathway. Inflammation 2018, 41, 914–923. [Google Scholar] [CrossRef]
- Zhang, J.; Bai, C. Elevated Serum Interleukin-8 Level as a Preferable Biomarker for Identifying Uncontrolled Asthma and Glucocorticosteroid Responsiveness. Tanafos 2017, 16, 260–269. [Google Scholar]
- Ogawa, Y.E.; Duru, A.E.; Ameredes, B.T. Role of IL-10 in the Resolution of Airway Inflammation. Curr. Mol. Med. 2008, 8, 437–445. [Google Scholar] [CrossRef]
- Wilson, E.B.; Brooks, D.G. The Role of IL-10 in Regulating Immunity to Persistent Viral Infections. Negat. Co-Recept. Ligands 2011, 350, 39–65. [Google Scholar] [CrossRef]
- Ke, J.J.; Zhan, J.; Feng, X.B.; Wu, Y.; Rao, Y.; Wang, Y.L. A Comparison of the Effect of Total Intravenous Anaesthesia with Propofol and Remifentanil and Inhalational Anaesthesia with Isoflurane on the Release of Pro- and Anti-Inflammatory Cytokines in Patients Undergoing Open Cholecystectomy. Anaesth. Intensiv. Care 2008, 36, 74–78. [Google Scholar] [CrossRef]
- Wakabayashi, S.; Yamaguchi, K.; Kumakura, S.; Murakami, T.; Someya, A.; Kajiyama, Y.; Nagaoka, I.; Inada, E. Effects of anesthesia with sevoflurane and propofol on the cytokine/chemokine production at the airway epithelium during esophagectomy. Int. J. Mol. Med. 2014, 34, 137–144. [Google Scholar] [CrossRef]
- Jin, Y.; Zhao, X.; Li, H.; Wang, Z.; Wang, D. Effects of sevoflurane and propofol on the inflammatory response and pulmonary function of perioperative patients with one-lung ventilation. Exp. Ther. Med. 2013, 6, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.-T.; Duan, X.-H.; Yang, Y.-F.; Wang, Y.; Bai, Q.-L.; Zhang, X. Effects of propofol or sevoflurane anesthesia on the perioperative inflammatory response, pulmonary function and cognitive function in patients receiving lung cancer resection. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 5515–5522. [Google Scholar] [CrossRef]
- Habre, W.; Matsumoto, I.; Sly, P.D. Propofol or halothane anaesthesia for children with asthma: Effects on respiratory mechanics. Br. J. Anaesth. 1996, 77, 739–774. [Google Scholar] [CrossRef] [PubMed]
- Lauer, R.; Vadi, M.; Mason, L. Anaesthetic management of the child with co-existing pulmonary disease. Br. J. Anaesth. 2012, 109, i47–i59. [Google Scholar] [CrossRef]
- Conti, G.; Dell’Utri, D.; Vilardi, V.; De Blasi, R.A.; Pelaia, P.; Antonelli, M.; Bufi, M.; Rosa, G.; Gasparetto, A. Propofol induces bronchodilation in mechanically ventilated chronic obstructive pulmonary disease (COPD) patients. Acta Anaesthesiol. Scand. 1993, 37, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Molliex, S.; Crestani, B.; Dureuil, B.; Bastin, J.; Rolland, C.; Aubier, M.; Desmonts, J.-M. Effects of Halothane on Surfactant Biosynthesis by Rat Alveolar Type II Cells in Primary Culture. Anesthesiology 1994, 81, 668–676. [Google Scholar] [CrossRef]
- Puglisi, F.; Crovace, A.; Staffieri, F.; Capuano, P.; Carravetta, G.; De Fazio, M.; Lograno, G.; Lacitignola, L.; Troilo, V.L.; Martines, G.; et al. Comparison of hemodynamic and respiratory effects of propofol and sevoflurane during carbon dioxide pneumoperitoneum in a swine model. Chir. Ital. 2007, 59, 105–111. [Google Scholar]
- Ouedraogo, N.; Roux, E.; Forestier, F.; Rossetti, M.; Savineau, J.-P.; Marthan, R. Effects of Intravenous Anesthetics on Normal and Passively Sensitized Human Isolated Airway Smooth Muscle. Anesthesiology 1998, 88, 317–326. [Google Scholar] [CrossRef]
- Peratoner, A.; Nascimento, C.S.; Santana, M.C.E.; Cadete, R.A.; Negri, E.M.; Gullo, A.; Rocco, P.R.M.; Zin, W.A. Effects of propofol on respiratory mechanic and lung histology in normal rats. Br. J. Anaesth. 2004, 92, 737–740. [Google Scholar] [CrossRef]
- Eames, W.O.; Rooke, A.G.; Wu, R.S.-C.; Bishop, M.J. Comparison of the Effects of Etomidate, Propofol, and Thiopental on Respiratory Resistance after Tracheal Intubation. Anesthesiology 1996, 84, 1307–1311. [Google Scholar] [CrossRef]
- Yamakage, M.; Hirshman, C.A.; Croxton, T.L. Inhibitory Effects of Thiopental, Ketamine, and Propofol on Voltage-dependent Calcium sup 2+ Channels in Porcine Tracheal Smooth Muscle Cells. Anesthesiology 1995, 83, 1274–1282. [Google Scholar] [CrossRef] [PubMed]
- Ginz, H.F.; Zorzato, F.; Iaizzo, P.A.; Urwyler, A. Effect of three anaesthetic techniques on isometric skeletal muscle strength. Br. J. Anaesth. 2004, 92, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Fagerlund, M.J.; Krupp, J.; Dabrowski, M.A. Propofol and AZD3043 Inhibit Adult Muscle and Neuronal Nicotinic Acetylcholine Receptors Expressed in Xenopus Oocytes. Pharmaceuticals 2016, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- Haeseler, G.; Störmer, M.; Bufler, J.; Dengler, R.; Hecker, H.; Piepenbrock, S.; Leuwer, M. Propofol Blocks Human Skeletal Muscle Sodium Channels in a Voltage-Dependent Manner. Anesthesia Analg. 2001, 92, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-Y.; Simpson, J.L.; Powell, H.; Yang, I.; Upham, J.; Reynolds, P.N.; Hodge, S.; James, A.L.; Jenkins, C.; Peters, M.; et al. Full blood count parameters for the detection of asthma inflammatory phenotypes. Clin. Exp. Allergy 2014, 44, 1137–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Propofol Group (n = 30) | Sevoflurane Group (n = 30) | p Value, Group Comparison |
|---|---|---|---|
| Sex (M/F) | 5/25 | 4/26 | 1.000 |
| ASA (I/II/III) | 28/2/0 | 25/5/0 | 0.424 |
| Age (years), mean ± SD | 48.8 ± 12.0 | 49.3 ± 12.2 | 0.88 |
| Weight (kg), mean ± SD | 70.2 ± 13.9 | 76.1 ± 13.1 | 0.097 |
| Height (cm), mean ± SD | 164.7 ± 5.4 | 164.8 ± 5.9 | 0.910 |
| Smoking status (non-smoker/ex-smoker/smoker) | 30/0/0 | 26/4/0 | 0.117 |
| Indication for surgery; Thyroid nodule/Hyperthyroidism/Substernal goiter/Thyroid cancer | 8/6/11/5 | 12/1/9/8 | 0.153 |
| Duration of surgery (min), median [IQR] | 95.0 [75.0–105.0] | 90.0 [75.0–105.0] | 0.542 |
| Duration of anesthesia, (min), median [IQR] | 110.0 [90.0–130.0] | 110.0 [100.0–120.0] | 0.591 |
| Baseline SBP (mmHg), mean ± SD | 135.2 ± 21.1 | 137.1 ± 19.5 | 0.714 |
| Baseline DBP (mmHg), mean ± SD | 77.6 ± 8.1 | 74.2 ± 8.1 | 0.111 |
| Baseline MAP (mmHg), mean ± SD | 96.2 ± 11.3 | 93.7 ± 12.1 | 0.413 |
| Baseline HR (bpm), mean ± SD | 76.0 ± 8.7 | 78.6 ± 9.7 | 0.268 |
| Variables | Propofol Group (n = 30) | Sevoflurane Group (n = 30) | p Value, Group Comparison |
|---|---|---|---|
| Standardized SBP over time (mmHg), mean ± SD | 123.4 ± 14.3 | 119.6 ± 11.2 | 0.260 |
| Standardized DBP over time (mmHg), mean ± SD | 76.8 ± 8.9 | 68.4 ± 8.8 * | 0.001 |
| Standardized MAP over time (mmHg), mean ± SD | 93.2 ± 10.1 | 86.2 ± 9.2 * | 0.007 |
| Standardized HR over time (bpm), mean ± SD | 71.6 ± 7.7 | 76.6 ± 8.3 * | 0.019 |
| Standardized BIS over time, mean ± SD | 45.2 ± 3.8 | 47.2 ± 2.6 * | 0.019 |
| Standardized SaO2 over time (%), mean ± SD | 98.7 ± 0.5 | 98.6 ± 0.6 | 0.301 |
| Standardized ETCO2 over time (mmHg), mean ± SD | 36.4 ± 2.9 | 36.5 ± 3.8 | 0.925 |
| Standardized Ppeak over time (cm H2O), mean ± SD | 16.6 ± 4.3 | 18.8 ± 3.4 * | 0.032 |
| Standardized Ppl over time (cm H2O), mean ± SD | 14.6 ± 4.2 | 16.6 ± 3.4 | 0.054 |
| Standardized compliance over time (mL/cm H2O), median [IQR] | 42.4 [35.0–52.9] | 33.0 [30.0–41.5] * | 0.027 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vekrakou, A.; Papacharalampous, P.; Logotheti, H.; Valsami, S.; Argyra, E.; Vassileiou, I.; Theodoraki, K. Effect of General Anesthesia Maintenance with Propofol or Sevoflurane on Fractional Exhaled Nitric Oxide and Eosinophil Blood Count: A Prospective, Single Blind, Randomized, Clinical Study on Patients Undergoing Thyroidectomy. J. Pers. Med. 2022, 12, 1455. https://doi.org/10.3390/jpm12091455
Vekrakou A, Papacharalampous P, Logotheti H, Valsami S, Argyra E, Vassileiou I, Theodoraki K. Effect of General Anesthesia Maintenance with Propofol or Sevoflurane on Fractional Exhaled Nitric Oxide and Eosinophil Blood Count: A Prospective, Single Blind, Randomized, Clinical Study on Patients Undergoing Thyroidectomy. Journal of Personalized Medicine. 2022; 12(9):1455. https://doi.org/10.3390/jpm12091455
Chicago/Turabian StyleVekrakou, Artemis, Panagiota Papacharalampous, Helena Logotheti, Serena Valsami, Eriphyli Argyra, Ioannis Vassileiou, and Kassiani Theodoraki. 2022. "Effect of General Anesthesia Maintenance with Propofol or Sevoflurane on Fractional Exhaled Nitric Oxide and Eosinophil Blood Count: A Prospective, Single Blind, Randomized, Clinical Study on Patients Undergoing Thyroidectomy" Journal of Personalized Medicine 12, no. 9: 1455. https://doi.org/10.3390/jpm12091455