
Assessment of Radiation-Induced Bladder and Bowel Cancer Risks after Conventionally and Hypo-Fractionated Radiotherapy for the Preoperative Management of Rectal Carcinoma
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Treatment Protocols, Techniques and Plan Optimization
2.3. Dosimetric Analysis and Comparison
2.4. Radiobiological Analysis
3. Results
3.1. Dosimetric Analysis and Comparison
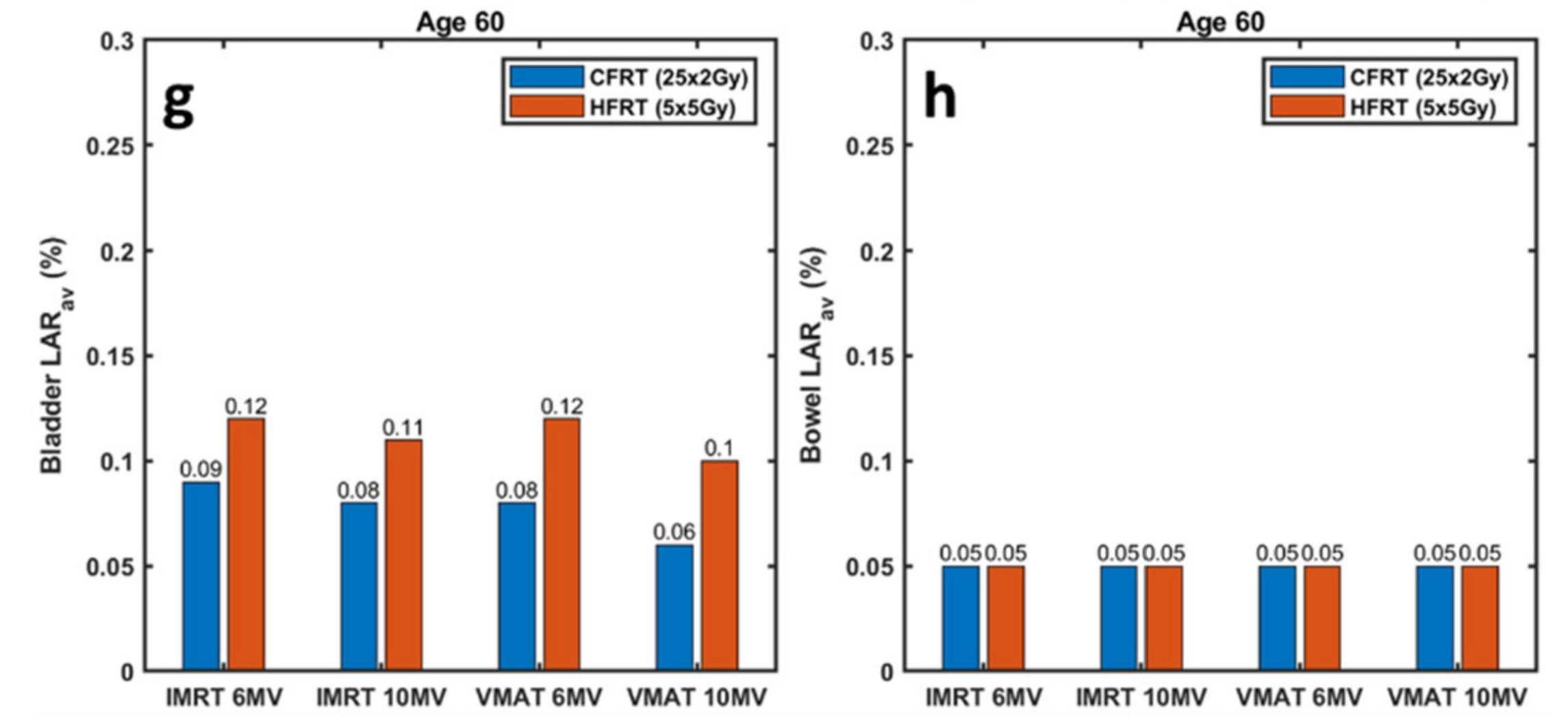
3.2. Radiobiological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, T.; Ruszkowska, M.; Danielewicz, A.; Niedźwiedzka, E.; Arłukowicz, T.; Przybyłowicz, K.E. A Review of Colorectal Cancer in Terms of Epidemiology, Risk Factors, Development, Symptoms and Diagnosis. Cancers 2021, 13, 2025. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal Cancer Statistics, 2020. CA A Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Joseph, D.A.; King, J.B.; Dowling, N.F.; Thomas, C.C.; Richardson, L.C. Vital Signs: Colorectal Cancer Screening Test Use—United States, 2018. Mmwr. Morb. Mortal. Wkly. Rep. 2020, 69, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Jin, F.; Luo, H.; Zhou, J.; Wu, Y.; Sun, H.; Liu, H.; Zheng, X.; Wang, Y. Dose–Time Fractionation Schedules of Preoperative Radiotherapy and Timing to Surgery for Rectal Cancer. Ther. Adv. Med. Oncol. 2020, 12, 1758835920907537. [Google Scholar] [CrossRef]
- Oronsky, B.; Reid, T.; Larson, C.; Knox, S.J. Locally Advanced Rectal Cancer: The Past, Present, and Future. Semin. Oncol. 2020, 47, 85–92. [Google Scholar] [CrossRef]
- Qiaoli, W.; Yongping, H.; Wei, X.; Guoqiang, X.; Yunhe, J.; Qiuyan, L.; Cheng, L.; Mengling, G.; Jiayi, L.; Wei, X.; et al. Preoperative Short-Course Radiotherapy (5 × 5 Gy) with Delayed Surgery versus Preoperative Long-Course Radiotherapy for Locally Resectable Rectal Cancer: A Meta-Analysis. Int. J. Colorectal Dis. 2019, 34, 2171–2183. [Google Scholar] [CrossRef]
- Liu, L.; Wang, H.; Yang, R.; Wang, J. Dosimetric Comparison of Fixed-Field Intensity-Modulated Radiotherapy and Volumetric-Modulated Arc Radiotherapy for Preoperative Rectal Cancer. Precis. Radiat. Oncol. 2018, 2, 39–43. [Google Scholar] [CrossRef]
- Bujko, K.; Nowacki, M.P.; Nasierowska-Guttmejer, A.; Michalski, W.; Bebenek, M.; Kryj, M. Long-Term Results of a Randomized Trial Comparing Preoperative Short-Course Radiotherapy with Preoperative Conventionally Fractionated Chemoradiation for Rectal Cancer. Br. J. Surg. 2006, 93, 1215–1223. [Google Scholar] [CrossRef]
- Palta, M.; Willett, C.G.; Czito, B.G. Short-Course versus Long-Course Chemoradiation in Rectal Cancer--Time to Change Strategies? Curr. Treat Options Oncol. 2014, 15, 421–428. [Google Scholar] [CrossRef]
- Skóra, T.; Nowak-Sadzikowska, J.; Martynów, D.; Wszołek, M.; Sas-Korczyńska, B. Preoperative Short-Course Radiotherapy in Rectal Cancer Patients: Results and Prognostic Factors. J. Radiat. Oncol. 2018, 7, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Li, S.; Yue, H.; Wang, M.; Hu, Q.; Wang, H.; Li, T.; Li, C.; Wu, H.; Zhang, Y. Impact of Nominal Photon Energies on Normal Tissue Sparing in Knowledge-Based Radiotherapy Treatment Planning for Rectal Cancer Patients. PLoS ONE 2019, 14, e0213271. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, H.; Podgorsak, M.B. The Dosimetric Significance of Using 10 MV Photons for Volumetric Modulated Arc Therapy for Post-Prostatectomy Irradiation of the Prostate Bed. Radiol. Oncol. 2016, 50, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Sung, W.; Park, J.M.; Choi, C.H.; Ha, S.W.; Ye, S.J. The Effect of Photon Energy on Intensity-Modulated Radiation Therapy (IMRT) Plans for Prostate Cancer. Radiat. Oncol. J. 2012, 30, 27–35. [Google Scholar] [CrossRef]
- Shi, J.; Yang, F.; Ju, X.; Huang, Y.; Jiang, F. Comparative Study on Dosimetry of VMAT and IMRT in Assisted Radiotherapy after Radical Resection of Rectal Cancer. Oncol. Lett. 2017, 13, 2971–2974. [Google Scholar] [CrossRef]
- Dapper, H.; Rodríguez, I.; Münch, S.; Peeken, J.C.; Borm, K.; Combs, S.E.; Habermehl, D. Impact of VMAT-IMRT Compared to 3D Conformal Radiotherapy on Anal Sphincter Dose Distribution in Neoadjuvant Chemoradiation of Rectal Cancer. Radiat. Oncol. 2018, 13, 1–9. [Google Scholar] [CrossRef]
- Zhao, J.; Hu, W.; Cai, G.; Wang, J.; Xie, J.; Peng, J.; Zhang, Z. Dosimetric Comparisons of VMAT, IMRT and 3DCRT for Locally Advanced Rectal Cancer with Simultaneous Integrated Boost. Oncotarget 2016, 7, 6345–6351. [Google Scholar] [CrossRef]
- Martling, A.; Smedby, K.E.; Birgisson, H.; Olsson, H.; Granath, F.; Ekbom, A.; Glimelius, B. Risk of Second Primary Cancer in Patients Treated with Radiotherapy for Rectal Cancer. Br. J. Surg. 2017, 104, 278–287. [Google Scholar] [CrossRef]
- Marcu, L.G. Photons—Radiobiological Issues Related to the Risk of Second Malignancies. Phys. Med. 2017, 42, 213–220. [Google Scholar] [CrossRef]
- Dracham, C.B.; Shankar, A.; Madan, R. Radiation Induced Secondary Malignancies: A Review Article. Radiat. Oncol. J. 2018, 36, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Nikolakopoulou, A.; Peppa, V.; Alexiou, A.; Pissakas, G.; Terzoudi, G.; Karaiskos, P. Comparison and Evaluation of Different Radiotherapy Techniques Using Biodosimetry Based on Cytogenetics. Cancers 2022, 14, 146. [Google Scholar] [CrossRef] [PubMed]
- Haciislamoglu, E.; Gungor, G.; Aydin, G.; Canyilmaz, E.; Guler, O.C.; Zengin, A.Y.; Yenice, K.M. Estimation of Secondary Cancer Risk after Radiotherapy in High-Risk Prostate Cancer Patients with Pelvic Irradiation. J. Appl. Clin. Med. Phys. 2020, 21, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Mazonakis, M.; Kachris, S.; Damilakis, J. Secondary Bladder and Rectal Cancer Risk Estimates Following Standard Fractionated and Moderately Hypofractionated VMAT for Prostate Carcinoma. Med. Phys. 2020, 47, 2805–2813. [Google Scholar] [CrossRef]
- Mazonakis, M.; Lyraraki, E.; Damilakis, J. Second Cancer Risk Assessments after Involved-Site Radiotherapy for Mediastinal Hodgkin Lymphoma. Med. Phys. 2017, 44, 3866–3874. [Google Scholar] [CrossRef] [PubMed]
- Mazonakis, M.; Lyraraki, E.; Tolia, M.; Damilakis, J. Risk for Second Bladder and Rectal Malignancies from Cervical Cancer Irradiation. J. Appl. Clin. Med. Phys. 2021, 22, 103–109. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, J.; Ao, N.; Yu, H.; Peng, Y.; Ou, L.; Zhang, S. Secondary Cancer Risk after Radiation Therapy for Breast Cancer with Different Radiotherapy Techniques. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Chao, P.J.; Tsai, I.H.; Huang, C.C.; Lin, C.H.; Shieh, C.S.; Hsieh, Y.W.; Yang, P.Y.; Lee, H.F.; Lee, T.F. Radiation-Induced Secondary Cancer Risk Assessment in Patients with Lung Cancer After Stereotactic Body Radiotherapy Using the CyberKnife M6 System With Lung-Optimized Treatment. Front. Bioeng. Biotechnol. 2020, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- König, L.; Hörner-Rieber, J.; Forsthoefel, M.; Haering, P.; Meixner, E.; Eichkorn, T.; Krämer, A.; Mielke, T.; Tonndorf-Martini, E.; Haefner, M.F.; et al. Secondary Malignancy Risk Following Proton vs. X-Ray Radiotherapy of Thymic Epithelial Tumors: A Comparative Modeling Study of Thoracic Organ-Specific Cancer Risk. Cancers 2022, 14, 2409. [Google Scholar] [CrossRef]
- Schneider, U.; Sumila, M.; Robotka, J. Site-Specific Dose-Response Relationships for Cancer Induction from the Combined Japanese A-Bomb and Hodgkin Cohorts for Doses Relevant to Radiotherapy. Theor. Biol. Med. Model. 2011, 8, 27. [Google Scholar] [CrossRef]
- Appelt, A.L.; Kerkhof, E.M.; Nyvang, L.; Harderwijk, E.C.; Abbott, N.L.; Teo, M.; Peters, F.P.; Kronborg, C.J.S.; Spindler, K.L.G.; Sebag-Montefiore, D.; et al. Robust Dose Planning Objectives for Mesorectal Radiotherapy of Early Stage Rectal CancerA Multicentre Dose Planning Study. Tech. Innov. Patient Support Radiat. Oncol. 2019, 11, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Gay, H.A.; Barthold, H.J.; O’Meara, E.; Bosch, W.R.; el Naqa, I.; Al-Lozi, R.; Rosenthal, S.A.; Lawton, C.; Lee, W.R.; Sandler, H.; et al. Pelvic Normal Tissue Contouring Guidelines for Radiation Therapy: A Radiation Therapy Oncology Group Consensus Panel Atlas. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e353–e362. [Google Scholar] [CrossRef] [PubMed]
- Dominello, M.M.; Nalichowski, A.; Paximadis, P.; Kaufman, I.; McSpadden, E.; Joiner, M.; Miller, S.; Konski, A. Limitations of the Bowel Bag Contouring Technique in the Definitive Treatment of Cervical Cancer. Pract. Radiat. Oncol. 2014, 4, e15–e20. [Google Scholar] [CrossRef] [PubMed]
- Kvinnsland, Y.; Muren, L.P. The Impact of Organ Motion on Intestine Doses and Complication Probabilities in Radiotherapy of Bladder Cancer. Radiother. Oncol. 2005, 76, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Hong, T.S.; Moughan, J.; Garofalo, M.C.; Bendell, J.; Berger, A.C.; Oldenburg, N.B.E.; Anne, P.R.; Perera, F.; Lee, R.J.; Jabbour, S.K.; et al. NRG Oncology Radiation Therapy Oncology Group 0822: A Phase 2 Study of Preoperative Chemoradiation Therapy Using Intensity Modulated Radiation Therapy in Combination with Capecitabine and Oxaliplatin for Patients with Locally Advanced Rectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Faria, S.; Kopek, N.; Hijal, T.; Liberman, S.; Charlebois, P.; Stein, B.; Meterissian, S.; Meguerditchian, A.; Fawaz, Z.; Artho, G. Phase II Trial of Short-Course Radiotherapy Followed by Delayed Surgery for Locoregionally Advanced Rectal Cancer. Colorectal Dis. 2014, 16, O66–O70. [Google Scholar] [CrossRef]
- Paddick, I. A Simple Scoring Ratio to Index the Conformity of Radiosurgical Treatment Plans. Technical Note. J. Neurosurg. 2000, 93, 219–222. [Google Scholar] [CrossRef]
- Dasu, A.; Toma-Dasu, I. Models for the Risk of Secondary Cancers from Radiation Therapy. Phys. Med. 2017, 42, 232–238. [Google Scholar] [CrossRef]
- Mazonakis, M.; Damilakis, J. Cancer Risk after Radiotherapy for Benign Diseases. Phys. Med. 2017, 42, 285–291. [Google Scholar] [CrossRef]
- Zwahlen, D.R.; Bischoff, L.I.; Gruber, G.; Sumila, M.; Schneider, U. Estimation of Second Cancer Risk after Radiotherapy for Rectal Cancer: Comparison of 3D Conformal Radiotherapy and Volumetric Modulated Arc Therapy Using Different High Dose Fractionation Schemes. Radiat. Oncol. 2016, 11, 1–9. [Google Scholar] [CrossRef]
- Arias, E.; Heron, M.; Xu, J. United States State Life Tables, 2014 National Vital Statistics Report; National Center for Health Statistics: Hyattsville, MD, USA, 2017; Volume 66. [Google Scholar]
- Lin, J.-C.; Tsai, J.-T.; Chen, L.-J.; Li, M.-H.; Liu, W.-H. Compared Planning Dosimetry of TOMO, VMAT and IMRT in Rectal Cancer with Different Simulated Positions. Oncotarget 2017, 8, 42020. [Google Scholar] [CrossRef] [Green Version]
- Luna, R.B.; de Torres Olombrada, M.V. MARC Preoperative Rectal Cancer Treatments vs. 3D Conformal Radiotherapy. A Dose Distribution Comparative Study. PLoS ONE 2019, 14, e0221262. [Google Scholar] [CrossRef]
- Yeo, S.G.; Oh, J.H.; Kim, D.Y.; Baek, J.Y.; Kim, S.Y.; Park, J.W.; Kim, M.J.; Chang, H.J.; Kim, T.H.; Lee, J.H.; et al. Preoperative Short-Course Concurrent Chemoradiation Therapy Followed by Delayed Surgery for Locally Advanced Rectal Cancer: A Phase 2 Multicenter Study (KROG 10-01). Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Bujko, K.; Wyrwicz, L.; Rutkowski, A.; Malinowska, M.; Pietrzak, L.; Kryński, J.; Michalski, W.; Oledzki, J.; Kuśnierz, J.; Zajac, L.; et al. Long-Course Oxaliplatin-Based Preoperative Chemoradiation versus 5 × 5 Gy and Consolidation Chemotherapy for CT4 or Fixed CT3 Rectal Cancer: Results of a Randomized Phase III Study. Ann. Oncol. 2016, 27, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Ngan, S.Y.; Burmeister, B.; Fisher, R.J.; Solomon, M.; Goldstein, D.; Joseph, D.; Ackland, S.P.; Schache, D.; McClure, B.; McLachlan, S.A.; et al. Randomized Trial of Short-Course Radiotherapy versus Long-Course Chemoradiation Comparing Rates of Local Recurrence in Patients with T3 Rectal Cancer: Trans-Tasman Radiation Oncology Group Trial 01.04. J. Clin. Oncol. 2012, 30, 3827–3833. [Google Scholar] [CrossRef]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.K.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. Short-Course Radiotherapy Followed by Chemotherapy before Total Mesorectal Excision (TME) versus Preoperative Chemoradiotherapy, TME, and Optional Adjuvant Chemotherapy in Locally Advanced Rectal Cancer (RAPIDO): A Randomised, Open-Label, Phase 3 Trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar] [CrossRef]
- Erlandsson, J.; Holm, T.; Pettersson, D.; Berglund, Å.; Cedermark, B.; Radu, C.; Johansson, H.; Machado, M.; Hjern, F.; Hallböök, O.; et al. Optimal Fractionation of Preoperative Radiotherapy and Timing to Surgery for Rectal Cancer (Stockholm III): A Multicentre, Randomised, Non-Blinded, Phase 3, Non-Inferiority Trial. Lancet Oncol. 2017, 18, 336–346. [Google Scholar] [CrossRef]
- Schneider, U.; Besserer, J.; MacK, A. Hypofractionated Radiotherapy Has the Potential for Second Cancer Reduction. Theor. Biol. Med. Model. 2010, 7, 1–8. [Google Scholar] [CrossRef]
- Morton, L.M.; Onel, K.; Curtis, R.E.; Hungate, E.A.; Armstrong, G.T. The Rising Incidence of Second Cancers: Patterns of Occurrence and Identification of Risk Factors for Children and Adults. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, e57–e67. [Google Scholar] [CrossRef]
- Kendal, W.S.; Nicholas, G. A Population-Based Analysis of Second Primary Cancers after Irradiation for Rectal Cancer. American J. Clin. Oncol. Cancer Clin. Trials 2007, 30, 333–339. [Google Scholar] [CrossRef]
- Wiltink, L.M.; Nout, R.A.; Fiocco, M.; Kranenbarg, E.M.K.; Jürgenliemk-Schulz, I.M.; Jobsen, J.J.; Nagtegaal, I.D.; Rutten, H.J.T.; van de Velde, C.J.H.; Creutzberg, C.L.; et al. No Increased Risk of Second Cancer after Radiotherapy in Patients Treated for Rectal or Endometrial Cancer in the Randomized TME, PORTEC-1, and PORTEC-2 Trials. J. Clin. Oncol. 2015, 33, 1640–1646. [Google Scholar] [CrossRef]
- Rombouts, A.J.M.; Hugen, N.; Elferink, M.A.G.; Feuth, T.; Poortmans, P.M.P.; Nagtegaal, I.D.; de Wilt, J.H.W. Incidence of Second Tumors after Treatment with or without Radiation for Rectal Cancer. Ann. Oncol. 2017, 28, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Kry, S.F.; Salehpour, M.; Followill, D.S.; Stovall, M.; Kuban, D.A.; White, R.A.; Rosen, I.I. The Calculated Risk of Fatal Secondary Malignancies from Intensity-Modulated Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Roeder, F.; Meldolesi, E.; Gerum, S.; Valentini, V.; Rödel, C. Recent Advances in (Chemo-)Radiation Therapy for Rectal Cancer: A Comprehensive Review. Radiat. Oncol. 2020, 15, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Tseng, M.; Soon, Y.Y.; Vellayappan, B.; Ho, F.; Tey, J. Radiation Therapy for Rectal Cancer. J. Gastrointest. Oncol. 2019, 10, 1238–1250. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OAR | CFRT (25 × 2 Gy) | HFRT (5 × 5 Gy) |
|---|---|---|
| Bowel | < 180 cc | < 200 cc |
| < 100 cc | ||
| < 65 cc | ||
| Bladder | < 40% | < 35% |
| < 15% | ||
| Femoral Heads | < 40% | < 40% |
| < 25% |
| Radiobiological Parameter | Bladder | Bowel |
|---|---|---|
| R | 0.06 | 0.09 |
| α (Gy−1) | 0.219 | 0.591 |
| α/β (Gy) | 3.0 | 3.0 |
| β(1/Gy2) | 0.073 | 0.197 |
| ) | 3.8 | 10 |
| −0.024 | −0.056 | |
| 2.38 | 6.9 |
| Structure | Dosimetric Index | IMRT | VMAT | ||
|---|---|---|---|---|---|
| 6 MV | 10 MV | 6 MV | 10 MV | ||
| PTV | HI | 1.05 ± 0 | 1.05 ± 0 | 1.06 ± 0.01 | 1.06 ± 0.01 |
| CI | 0.84 ± 0.01 | 0.85 ± 0.01 | 0.84 ± 0.02 | 0.84 ± 0.01 | |
| Bladder | V40Gy (%) | 10.85 ± 8.35 | 10.52 ± 8.18 | 11.90 ± 9.07 | 11.85 ± 8.79 |
| V45Gy (%) | 5.43 ± 4.85 | 5.23 ± 4.68 | 5.70 ± 4.41 | 5.52 ± 4.39 | |
| Bowel | V35Gy (cc) | 118.10 ± 31.90 | 129.47 ± 37.25 | 131.42 ± 38.39 | 137.42 ± 38.12 |
| V40Gy (cc) | 62.61 ± 18.64 | 63.61 ± 20.37 | 68.15 ± 23.56 | 70.23 ± 22.91 | |
| V45Gy (cc) | 33.97 ± 20.26 | 32.60 ± 19.40 | 25.45 ± 19.58 | 35.45 ± 20.41 | |
| Structure | Dosimetric Index | IMRT | VMAT | ||
|---|---|---|---|---|---|
| 6 MV | 10 MV | 6 MV | 10 MV | ||
| PTV | HI | 1.05 ± 0 | 1.05 ± 0 | 1.06 ± 0.01 | 1.06 ± 0.01 |
| CI | 0.84 ± 0.01 | 0.85 ± 0.01 | 0.84 ± 0.02 | 0.84 ± 0.01 | |
| Bladder | V22Gy (%) | 7.07 ± 2.90 | 7.10 ± 2.45 | 7.02 ± 2.87 | 7.10 ± 2.00 |
| Bowel | V20Gy (cc) | 79.50 ± 49.06 | 81.00 ± 48.73 | 81.26 ± 46.43 | 84.27 ± 51.57 |
| CFRT (25 × 2 Gy) | HFRT (5 × 5 Gy) | ||||
|---|---|---|---|---|---|
| Delivery Technique | Photon Beam Energy | Bladder | Bowel | Bladder | Bowel |
| IMRT | 6 MV | 38.2 ± 9.0 | 16.5 ± 4.0 | 50.7 ± 16.1 | 15.8 ± 4.3 |
| 10 MV | 31.7 ± 6.7 | 15.8 ± 4.2 | 46.2 ± 15.9 | 15.8 ± 4.3 | |
| VMAT | 6 MV | 33.7 ± 8.1 | 16.3 ± 4.0 | 46.5 ± 13.8 | 17.1 ± 4.1 |
| 10 MV | 26.0 ± 5.7 | 15.7 ± 3.7 | 40.0 ± 10.6 | 15.8 ± 4.3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsali, E.; Pappas, E.P.; Lyraraki, E.; Lymperopoulou, G.; Mazonakis, M.; Karaiskos, P. Assessment of Radiation-Induced Bladder and Bowel Cancer Risks after Conventionally and Hypo-Fractionated Radiotherapy for the Preoperative Management of Rectal Carcinoma. J. Pers. Med. 2022, 12, 1442. https://doi.org/10.3390/jpm12091442
Matsali E, Pappas EP, Lyraraki E, Lymperopoulou G, Mazonakis M, Karaiskos P. Assessment of Radiation-Induced Bladder and Bowel Cancer Risks after Conventionally and Hypo-Fractionated Radiotherapy for the Preoperative Management of Rectal Carcinoma. Journal of Personalized Medicine. 2022; 12(9):1442. https://doi.org/10.3390/jpm12091442
Chicago/Turabian StyleMatsali, Ekaterini, Eleftherios P. Pappas, Efrossyni Lyraraki, Georgia Lymperopoulou, Michalis Mazonakis, and Pantelis Karaiskos. 2022. "Assessment of Radiation-Induced Bladder and Bowel Cancer Risks after Conventionally and Hypo-Fractionated Radiotherapy for the Preoperative Management of Rectal Carcinoma" Journal of Personalized Medicine 12, no. 9: 1442. https://doi.org/10.3390/jpm12091442