
Clinical Utility of Circulating Tumor Cells for Predicting Major Histopathological Response after Neoadjuvant Chemoradiotherapy in Patients with Esophageal Cancer
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Neoadjuvant Chemoradiotherapy
2.3. Clinical Restaging after Neoadjuvant Chemoradiotherapy
2.4. Surgical Resection
2.5. Pathological Assessment
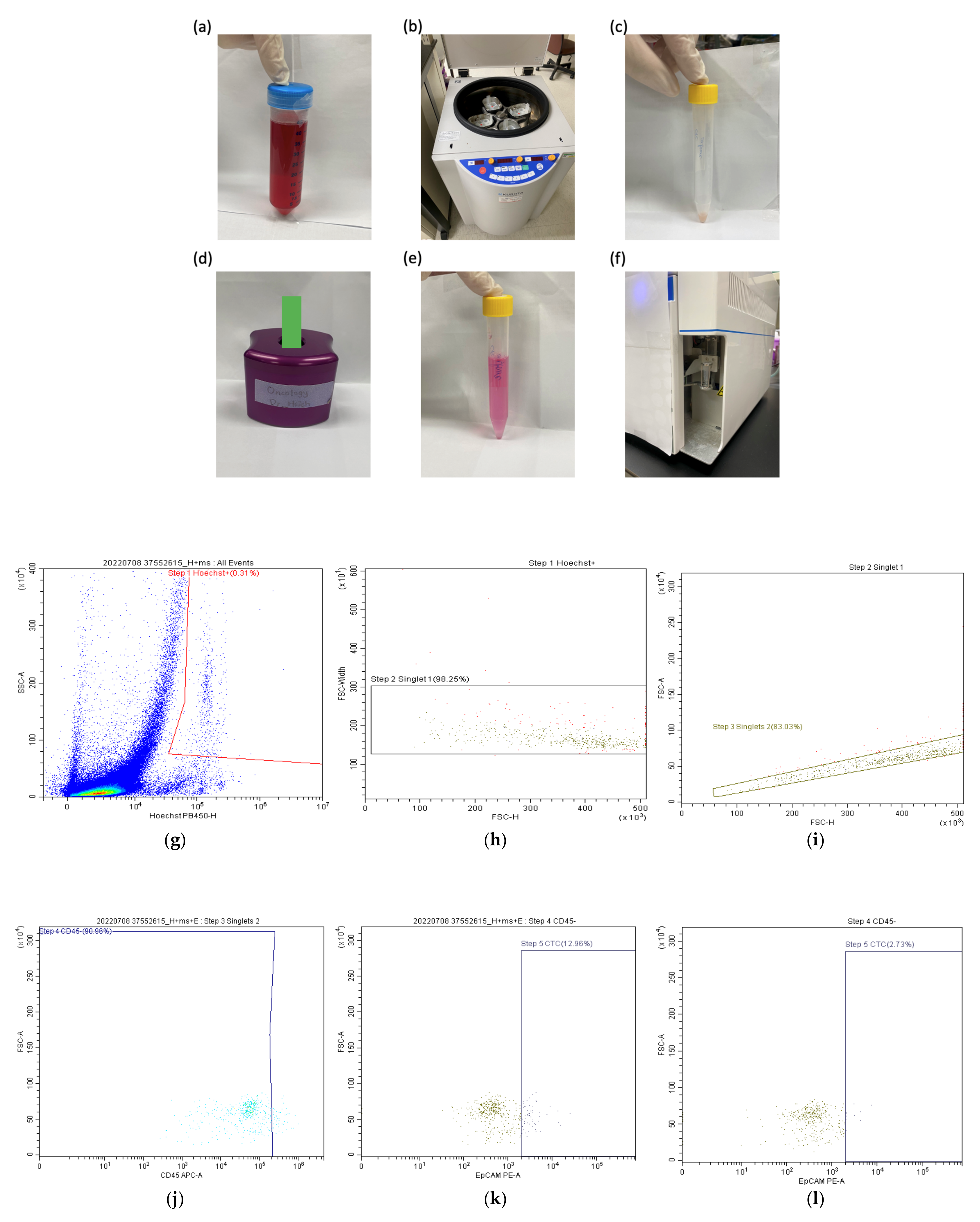
2.6. Quantification of Circulating Tumor Cells by Flow Cytometry
2.7. Statistics
3. Results
3.1. Patient Characteristics
3.2. Quantification of Circulating Tumor Cells and Determination of the Optimal Cutoff Value
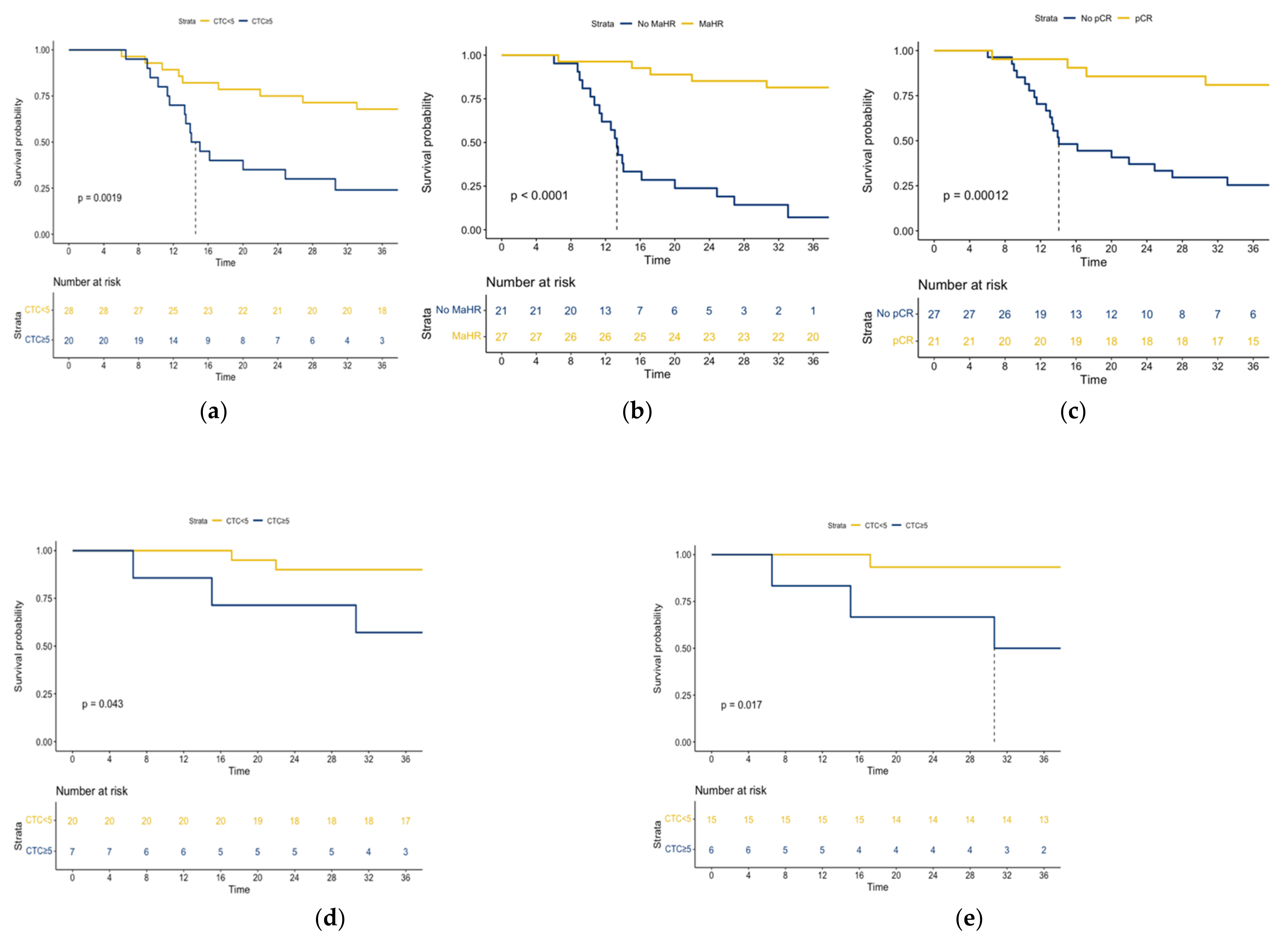
3.3. Survival Analysis
3.4. Accuracy of Clinical Response Assessment and Circulating Tumor Cells in the Detection of MaHR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef]
- Castoro, C.; Scarpa, M.; Cagol, M.; Alfieri, R.; Ruol, A.; Cavallin, F.; Michieletto, S.; Zanchettin, G.; Chiarion-Sileni, V.; Corti, L. Complete clinical response after neoadjuvant chemoradiotherapy for squamous cell cancer of the thoracic oesophagus: Is surgery always necessary? J. Gastrointest. Surg. 2013, 17, 1375–1381. [Google Scholar] [CrossRef]
- Piessen, G.; Messager, M.; Mirabel, X.; Briez, N.; Robb, W.B.; Adenis, A.; Mariette, C. Is there a role for surgery for patients with a complete clinical response after chemoradiation for esophageal cancer? An intention-to-treat case-control study. Ann. Surg. 2013, 258, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Van der Wilk, B.J.; Noordman, B.J.; Neijenhuis, L.K.; Nieboer, D.; Nieuwenhuijzen, G.A.; Sosef, M.N.; Henegouwen, M.I.; Lagarde, S.M.; Spaander, M.C.; Valkema, R. Active surveillance versus immediate surgery in clinically complete responders after neoadjuvant chemoradiotherapy for esophageal cancer: A multicenter propensity matched study. Ann. Surg. 2021, 274, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Qin, J.; Jing, S.; Liu, Q.; Cheng, Y.; Wang, Y.; Cao, F. Clinical complete response after chemoradiotherapy for carcinoma of thoracic esophagus: Is esophagectomy always necessary? A systematic review and meta-analysis. Thorac. Cancer 2018, 9, 1638–1647. [Google Scholar] [CrossRef] [PubMed]
- Chao, Y.-K.; Chuang, W.-Y.; Yeh, C.-J.; Chang, H.-K.; Tseng, C.-K. Anatomical distribution of residual cancer in patients with oesophageal squamous cell carcinoma who achieved clinically complete response after neoadjuvant chemoradiotherapy. Eur. J. Cardio-Thorac. Surg. 2018, 53, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, H.M.; Donohoe, C.; Elliot, J.; Ahmed, Z.; Malik, V.; Ravi, N.; Reynolds, J.V. Can CT-PET and endoscopic assessment post-neoadjuvant chemoradiotherapy predict residual disease in esophageal cancer? Ann. Surg. 2016, 264, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Z.; Wang, X.; Geng, X.; Li, Y.; Mu, J.; Tan, F.; Xue, Q.; Gao, S.; He, J. Liquid biopsy for esophageal cancer: Is detection of circulating cell-free DNA as a biomarker feasible? Cancer Commun. 2021, 41, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Agostini, M.; Pucciarelli, S.; Enzo, M.V.; Del Bianco, P.; Briarava, M.; Bedin, C.; Maretto, I.; Friso, M.L.; Lonardi, S.; Mescoli, C.; et al. Circulating cell-free DNA: A promising marker of pathologic tumor response in rectal cancer patients receiving preoperative chemoradiotherapy. Ann. Surg. Oncol. 2011, 18, 2461–2468. [Google Scholar] [CrossRef] [PubMed]
- Parsons, H.A.; Rhoades, J.; Reed, S.C.; Gydush, G.; Ram, P.; Exman, P.; Xiong, K.; Lo, C.C.; Li, T.; Fleharty, M.; et al. Sensitive Detection of Minimal Residual Disease in Patients Treated for Early-Stage Breast Cancer. Clin. Cancer Res. 2020, 26, 2556–2564. [Google Scholar] [CrossRef] [Green Version]
- Song, B.G.; Kwon, W.; Kim, H.; Lee, E.M.; Han, Y.M.; Kim, H.; Byun, Y.; Lee, K.B.; Lee, K.H.; Lee, K.T.; et al. Detection of Circulating Tumor Cells in Resectable Pancreatic Ductal Adenocarcinoma: A Prospective Evaluation as a Prognostic Marker. Front. Oncol. 2020, 10, 616440. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.T.; Miao, J.; Liu, J.W.; Zhang, L.G.; Zhang, Q.G. Prognostic value of circulating tumor cells in esophageal cancer. World J. Gastroenterol. 2017, 23, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Chirieac, L.R.; Swisher, S.G.; Ajani, J.A.; Komaki, R.R.; Correa, A.M.; Morris, J.S.; Roth, J.A.; Rashid, A.; Hamilton, S.R.; Wu, T.T. Posttherapy pathologic stage predicts survival in patients with esophageal carcinoma receiving preoperative chemoradiation. Cancer 2005, 103, 1347–1355. [Google Scholar] [CrossRef]
- Lawrence, D.; Brown, T.T.C. Anirban DasGupta. Interval Estimation for a Binomial Proportion. Stat. Sci. 2001, 16, 101–117. [Google Scholar]
- Eyck, B.M.; Onstenk, B.D.; Noordman, B.J.; Nieboer, D.; Spaander, M.C.; Valkema, R.; Lagarde, S.M.; Wijnhoven, B.P.; van Lanschot, J.J.B. Accuracy of detecting residual disease after neoadjuvant chemoradiotherapy for esophageal cancer: A systematic review and meta-analysis. Ann. Surg. 2020, 271, 245–256. [Google Scholar] [CrossRef]
- Cheedella, N.K.; Suzuki, A.; Xiao, L.; Hofstetter, W.L.; Maru, D.M.; Taketa, T.; Sudo, K.; Blum, M.A.; Lin, S.H.; Welch, J.; et al. Association between clinical complete response and pathological complete response after preoperative chemoradiation in patients with gastroesophageal cancer: Analysis in a large cohort. Ann. Oncol. 2013, 24, 1262–1266. [Google Scholar] [CrossRef]
- Sun, W.; Li, G.; Wan, J.; Zhu, J.; Shen, W.; Zhang, Z. Circulating tumor cells: A promising marker of predicting tumor response in rectal cancer patients receiving neoadjuvant chemo-radiation therapy. Oncotarget 2016, 7, 69507. [Google Scholar] [CrossRef]
- Hinz, S.; Röder, C.; Tepel, J.; Hendricks, A.; Schafmayer, C.; Becker, T.; Kalthoff, H. Cytokeratin 20 positive circulating tumor cells are a marker for response after neoadjuvant chemoradiation but not for prognosis in patients with rectal cancer. BMC Cancer 2015, 15, 953. [Google Scholar] [CrossRef]
- Huang, X.; Gao, P.; Song, Y.; Sun, J.; Chen, X.; Zhao, J.; Liu, J.; Xu, H.; Wang, Z. Relationship between circulating tumor cells and tumor response in colorectal cancer patients treated with chemotherapy: A meta-analysis. BMC Cancer 2014, 14, 976. [Google Scholar] [CrossRef]
- Hsu, F.M.; Cheng, J.C.; Chang, Y.L.; Lee, J.M.; Koong, A.C.; Chuang, E.Y. Circulating mRNA Profiling in Esophageal Squamous Cell Carcinoma Identifies FAM84B As A Biomarker In Predicting Pathological Response to Neoadjuvant Chemoradiation. Sci. Rep. 2015, 5, 10291. [Google Scholar] [CrossRef]
- Chen, W.; Li, Y.; Yuan, D.; Peng, Y.; Qin, J. Practical value of identifying circulating tumor cells to evaluate esophageal squamous cell carcinoma staging and treatment efficacy. Thorac. Cancer 2018, 9, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Noordman, B.J.; Spaander, M.C.W.; Valkema, R.; Wijnhoven, B.P.L.; van Berge Henegouwen, M.I.; Shapiro, J.; Biermann, K.; van der Gaast, A.; van Hillegersberg, R.; Hulshof, M.; et al. Detection of residual disease after neoadjuvant chemoradiotherapy for oesophageal cancer (preSANO): A prospective multicentre, diagnostic cohort study. Lancet Oncol. 2018, 19, 965–974. [Google Scholar] [CrossRef]
- Valkema, M.J.; Noordman, B.J.; Wijnhoven, B.P.L.; Spaander, M.C.W.; Biermann, K.; Lagarde, S.M.; Bennink, R.J.; Schreurs, W.M.J.; Roef, M.J.; Hobbelink, M.G.G.; et al. Accuracy of (18)F-FDG PET/CT in Predicting Residual Disease After Neoadjuvant Chemoradiotherapy for Esophageal Cancer. J. Nucl. Med. 2019, 60, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Pantel, K.; Deneve, E.; Nocca, D.; Coffy, A.; Vendrell, J.P.; Maudelonde, T.; Riethdorf, S.; Alix-Panabieres, C. Circulating epithelial cells in patients with benign colon diseases. Clin. Chem. 2012, 58, 936–940. [Google Scholar] [CrossRef]
- Liao, C.J.; Hsieh, C.H.; Chiu, T.K.; Zhu, Y.X.; Wang, H.M.; Hung, F.C.; Chou, W.P.; Wu, M.H. An Optically Induced Dielectrophoresis (ODEP)-Based Microfluidic System for the Isolation of High-Purity CD45neg/EpCAMneg Cells from the Blood Samples of Cancer Patients-Demonstration and Initial Exploration of the Clinical Significance of These Cells. Micromachines 2018, 9, 563. [Google Scholar] [CrossRef]
- Chiu, S.Y.; Hsieh, C.H.; You, J.F.; Chu, P.Y.; Hung, H.Y.; Chu, P.H.; Wu, M.H. Enhancing Prediction Performance by Add-On Combining Circulating Tumor Cell Count, CD45neg EpCAMneg Cell Count on Colorectal Cancer, Advance, and Metastasis. Cancers 2021, 13, 2521. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Entire Cohort n = 48 | pCR n = 21 | No pCR n = 27 | P | MaHR n = 27 | No MaHR n = 21 | P | |
|---|---|---|---|---|---|---|---|
| Sex | 1.0 | 0.858 | |||||
| Male | 43 (90) | 19 (90) | 24 (89) | 24 (89) | 19 (90) | ||
| Female | 5 (10) | 2 (10) | 3 (11) | 3 (11) | 2 (10) | ||
| Age, years | 56 ± 12.5 | 57.76 ± 10.11 | 54.81 ± 8.49 | 0.278 | 57.56 ± 10.41 | 54.24 ± 7.33 | 0.221 |
| Clinical stage | 0.383 | 0.683 | |||||
| II | 6 (13) | 4 (19) | 2 (7) | 4 (15) | 2 (10) | 0.221 | |
| III−IVa | 42 (87) | 17 (81) | 25 (93) | 23 (85) | 19 (90) | 0.683 | |
| Tumor length, cm | 5.54 ± 3.9 | 5.02 ± 3.42 | 6.19 ± 2.24 | 0.171 | 4.95 ± 3.14 | 6.57 ± 2.22 | 0.058 |
| Chemotherapy regimen | 0.897 | 0.498 | |||||
| PF | 11 (23) | 5 (24) | 6 (22) | 5 (19) | 6 (26) | ||
| CROSS | 37 (77) | 16 (76) | 21 (78) | 22 (81) | 15 (74) | ||
| cCR | 21(44) | 14 (67) | 7 (26) | 0.005 | 17 (63) | 4 (19) | 0.002 |
| CTCs count per mL of blood | 5.02 ± 1.42 | 3.83 ± 4.98 | 5.94 ± 5.01 | 0.153 | 3.61 ± 4.53 | 6.83 ± 5.22 | 0.027 |
| Pathological T stage | <0.001 | <0.001 | |||||
| ypT0 | 24 (50) | 21 (100) | 3 (11) | 21 (78) | 3 (14) | ||
| ypT1 | 5 (11) | 0 (0) | 5 (19) | 3 (11) | 2 (10) | ||
| ypT2 | 3 (6) | 0 (0) | 3 (11) | 2 (7) | 1 (4) | ||
| ypT3 | 14 (29) | 0 (0) | 14 (52) | 1 (4) | 13 (62) | ||
| ypT4 | 2 (4) | 0 (0) | 2 (7) | 0 (0) | 2 (10) | ||
| Pathological N stage | 0.007 | <0.001 | |||||
| ypN0 | 38 (79) | 21 (100) | 17 (63) | 27 (100) | 11 (52) | ||
| ypN+ | 8 (17) | 0 (0) | 8 (30) | 0 (0) | 8 (38) | ||
| ypNx | 2 (4) | 0 (0) | 2 (7) | 0 (0) | 2 (10) |
| pCR | MaHR | ||||||
|---|---|---|---|---|---|---|---|
| CTCs Count per mL of Blood | n (%) | OR | 95% CI | P | OR | 95% CI | P |
| ≥ 0 = 0 | 37 (77) 11 (23) | 1 2.88 | 0.71–11.62 | 0.138 | 1 2.526 | 0.58–11.05 | 0.218 |
| ≥ 3 < 3 | 29 (60) 19 (40) | 1 2.16 | 0.66–7.10 | 0.205 | 1 2.971 | 0.85–10.44 | 0.089 |
| ≥ 5 < 5 | 20 (42) 28 (58) | 1 2.69 | 0.80–9.04 | 0.109 | 1 4.643 | 1.36–15.91 | 0.023 |
| ≥ 7 < 7 | 11 (23) 37 (77) | 1 2.53 | 0.58–11.05 | 0.218 | 1 4.923 | 1.11–21.82 | 0.036 |
| No MaHR | MaHR | FNR | Specificity | NPV | Accuracy | |
|---|---|---|---|---|---|---|
| No cCR | 17 | 10 | 4/21 (29%) | 17/27 (63%) | 17/21 (81%) | 34/48 (71%) |
| cCR | 4 | 17 | ||||
| CTC count ≥5 per mL of blood | 13 | 7 | 8/21 (38%) | 20/27 (74%) | 20/28 (71%) | 33/48 (69%) |
| CTC count <5 per mL of blood | 8 | 20 | ||||
| Non-cCR or CTC count ≥5 per mL of blood | 20 | 13 | 1/21 (5%) | 14/27 (52%) | 14/15 (93%) | 34/48 (71%) |
| cCR and CTC count <5 per mL of blood | 1 | 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, X.; Leow, O.Q.-Y.; Chiu, C.-H.; Hou, M.-M.; Hsieh, J.C.-H.; Chao, Y.-K. Clinical Utility of Circulating Tumor Cells for Predicting Major Histopathological Response after Neoadjuvant Chemoradiotherapy in Patients with Esophageal Cancer. J. Pers. Med. 2022, 12, 1440. https://doi.org/10.3390/jpm12091440
Gao X, Leow OQ-Y, Chiu C-H, Hou M-M, Hsieh JC-H, Chao Y-K. Clinical Utility of Circulating Tumor Cells for Predicting Major Histopathological Response after Neoadjuvant Chemoradiotherapy in Patients with Esophageal Cancer. Journal of Personalized Medicine. 2022; 12(9):1440. https://doi.org/10.3390/jpm12091440
Chicago/Turabian StyleGao, Xing, Osbert Qi-Yao Leow, Chien-Hung Chiu, Ming-Mo Hou, Jason Chia-Hsun Hsieh, and Yin-Kai Chao. 2022. "Clinical Utility of Circulating Tumor Cells for Predicting Major Histopathological Response after Neoadjuvant Chemoradiotherapy in Patients with Esophageal Cancer" Journal of Personalized Medicine 12, no. 9: 1440. https://doi.org/10.3390/jpm12091440