
A Pilot Study Assessing a Closed-Loop System for Goal-Directed Fluid Therapy in Abdominal Surgery Patients
 ,
,
Abstract
:1. Background
2. Materials and Methods
2.1. Intraoperative Management
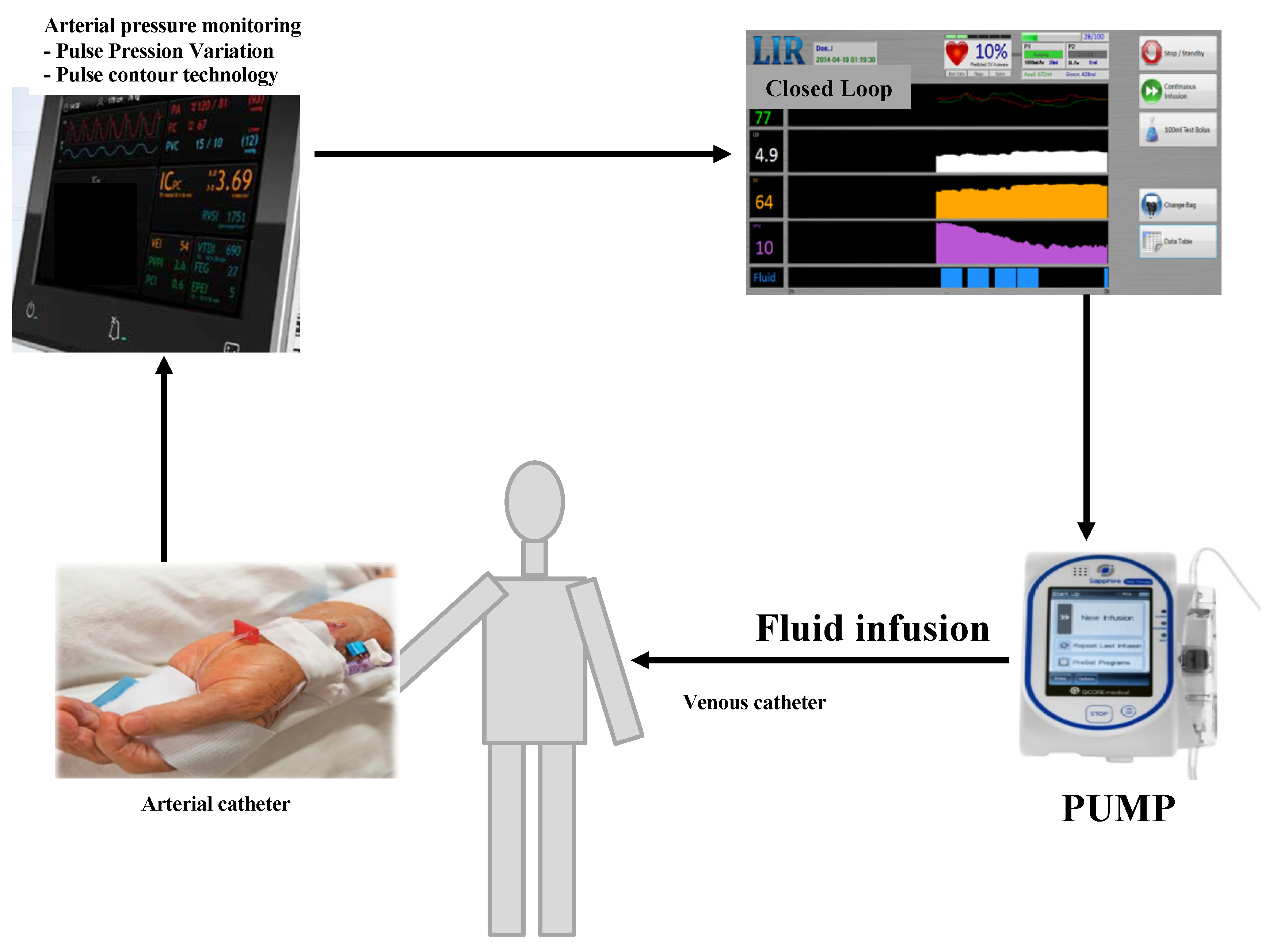
2.2. Closed-Loop System Description and Setup
2.3. CL and Anaesthesiologist Agreement
- Invalid preload parameters,
- Poor quality of the pulse contour signal,
- No hemodynamic signs of hypovolemia,
- Any dysfunction of the device.
2.4. Data Collection
2.5. Study Outcomes
- -
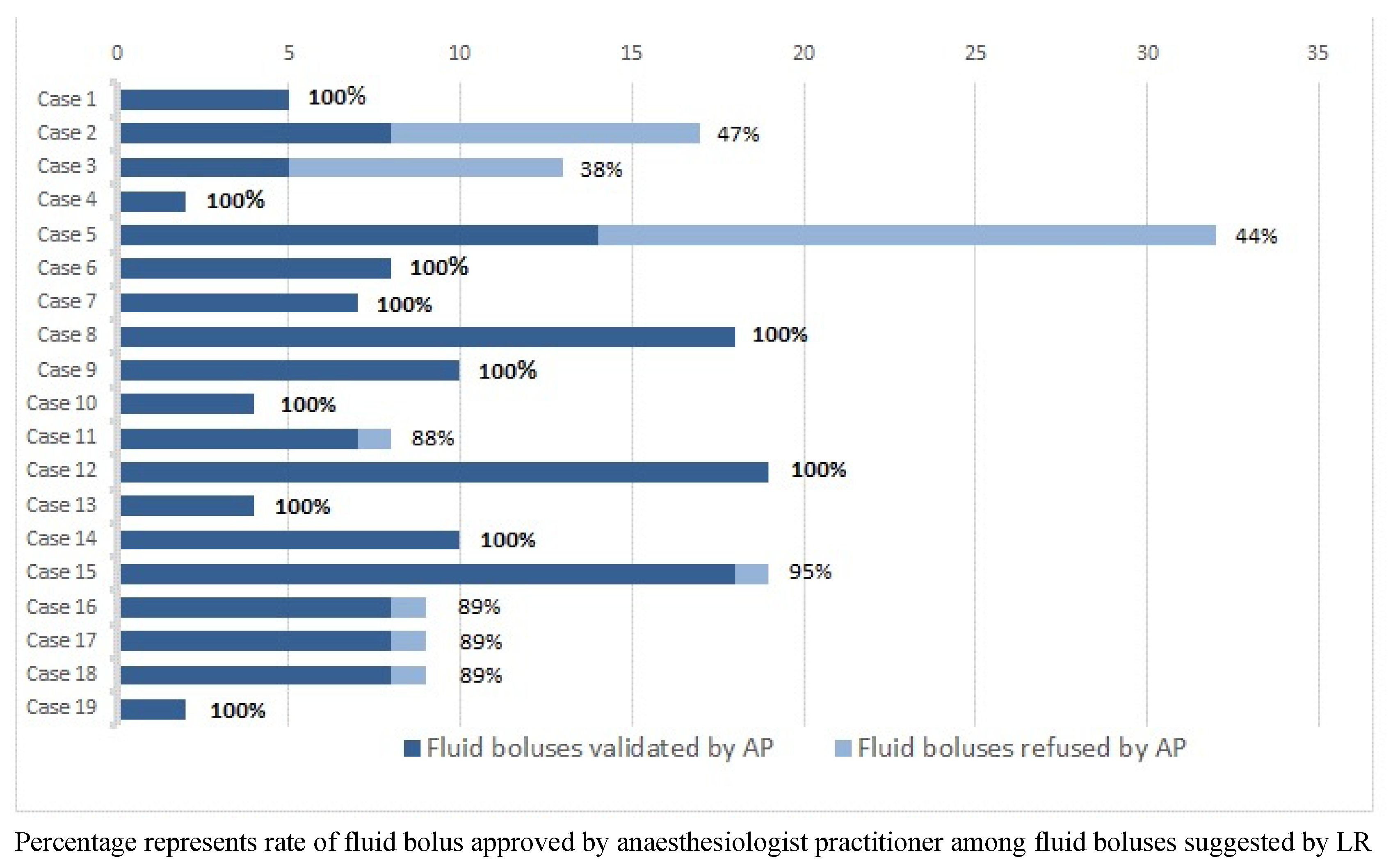
- The proportion of fluid boluses administered by the anaesthesiologist in charge of the patient beyond the boluses recommended by CL,
- -
- The percentage of surgery time spent beyond the optimal CI and above 2.5 L/min/m2 with a PPV value < 13% (preload-independent state),
- -
- CI variability throughout the surgery defined by the CI’s coefficient of variation (CV).
2.6. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Sinclair, S.; James, S.; Singer, M. Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: Randomised controlled trial. BMJ 1997, 315, 909–912. [Google Scholar] [CrossRef]
- Gan, T.J.; Soppitt, A.; Maroof, M.; el-Moalem, H.; Robertson, K.M.; Moretti, E.; Dwane, P.; Glass, P.S.A. Goal-directed intraoperative fluid administration reduces length of hospital stay after major surgery. Anesthesiology 2002, 97, 820–826. [Google Scholar] [CrossRef]
- Hamilton, M.A.; Cecconi, M.; Rhodes, A. A systematic review and meta-analysis on the use of preemptive hemodynamic intervention to improve postoperative outcomes in moderate and high-risk surgical patients. Anesth. Analg. 2011, 112, 1392–1402. [Google Scholar] [CrossRef]
- Cannesson, M.; Ramsingh, D.; Rinehart, J.; Demirjian, A.; Vu, T.; Vakharia, S.; Imagawa, D.; Yu, Z.; Greenfield, S.; Kain, Z. Perioperative goal-directed therapy and postoperative outcomes in patients undergoing high-risk abdominal surgery: A historical-prospective, comparative effectiveness study. Crit. Care 2015, 19, 261. [Google Scholar] [CrossRef]
- Cecconi, M.; Corredor, C.; Arulkumaran, N.; Abuella, G.; Ball, J.; Grounds, R.M.; Hamilton, M.; Rhodes, A. Clinical review: Goal-directed therapy-what is the evidence in surgical patients? The effect on different risk groups. Crit. Care 2012, 17, 209. [Google Scholar] [CrossRef]
- Rhodes, A.; Cecconi, M.; Hamilton, M.; Poloniecki, J.; Woods, J.; Boyd, O.; Bennett, D.; Grounds, R.M. Goal-directed therapy in high-risk surgical patients: A 15-year follow-up study. Intensive Care Med. 2010, 36, 1327–1332. [Google Scholar] [CrossRef]
- Pearse, R.M.; Harrison, D.A.; MacDonald, N.; Gillies, M.A.; Blunt, M.; Ackland, G.; Grocott, M.P.W.; Ahern, A.; Griggs, K.; Scott, R.; et al. Effect of a perioperative, cardiac output-guided hemodynamic therapy algorithm on outcomes following major gastrointestinal surgery: A randomized clinical trial and systematic review. JAMA 2014, 311, 2181–2190. [Google Scholar] [CrossRef]
- Osawa, E.A.; Rhodes, A.; Landoni, G.; Galas, F.R.B.G.; Fukushima, J.T.; Park, C.H.L.; Almeida, J.P.; Nakamura, R.E.; Strabelli, T.M.V.; Pileggi, B.; et al. Effect of Perioperative Goal-Directed Hemodynamic Resuscitation Therapy on Outcomes Following Cardiac Surgery: A Randomized Clinical Trial and Systematic Review. Crit. Care Med. 2016, 44, 724–733. [Google Scholar] [CrossRef]
- Benes, J.; Zatloukal, J.; Simanova, A.; Chytra, I.; Kasal, E. Cost analysis of the stroke volume variation guided perioperative hemodynamic optimization—An economic evaluation of the SVVOPT trial results. BMC Anesthesiol. 2014, 14, 40. [Google Scholar] [CrossRef]
- Vallet, B.; Blanloeil, Y.; Cholley, B.; Orliaguet, G.; Pierre, S.; Tavernier, B. Guidelines for perioperative haemodynamic optimization. Ann. Fr. Anesth. Reanim. 2013, 32, e151–e158. [Google Scholar] [CrossRef]
- Brienza, N.; Biancofiore, G.; Cavaliere, F.; Corcione, A.; De Gasperi, A.; De Rosa, R.C.; Fumagalli, R.; Giglio, M.T.; Locatelli, A.; Lorini, F.L.; et al. Clinical guidelines for perioperative hemodynamic management of non cardiac surgical adult patients. Minerva Anestesiol. 2019, 85, 1315–1333. [Google Scholar] [CrossRef] [PubMed]
- Thiele, R.H.; Raghunathan, K.; Brudney, C.S.; Lobo, D.N.; Martin, D.; Senagore, A.; Cannesson, M.; Gan, T.J.; Mythen, M.M.G.; Shaw, A.D.; et al. American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on perioperative fluid management within an enhanced recovery pathway for colorectal surgery. Perioper. Med. 2016, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Suehiro, K.; Tanaka, K.; Mukai, A.; Joosten, A.; Desebbe, O.; Alexander, B.; Cannesson, M.; Nishikawa, K. Hemodynamic monitoring and management in high-risk surgery: A survey among Japanese anesthesiologists. J. Anesth. 2016, 30, 526–529. [Google Scholar] [CrossRef] [PubMed]
- Cannesson, M.; Pestel, G.; Ricks, C.; Hoeft, A.; Perel, A. Hemodynamic monitoring and management in patients undergoing high risk surgery: A survey among North American and European anesthesiologists. Crit. Care 2011, 15, R197. [Google Scholar] [CrossRef]
- Molliex, S.; Passot, S.; Morel, J.; Futier, E.; Lefrant, J.Y.; Constantin, J.M.; Le Manach, Y.; Pereira, B. Opti-Aged group, Azurea clinical research Network. A multicentre observational study on management of general anaesthesia in elderly patients at high-risk of postoperative adverse outcomes. Anaesth. Crit. Care Pain Med. 2019, 38, 15–23. [Google Scholar] [CrossRef]
- Peden, C.J.; Stephens, T.; Martin, G.; Kahan, B.C.; Thomson, A.; Rivett, K.; Wells, D.; Richardson, G.; Kerry, S.; Bion, J.; et al. Effectiveness of a national quality improvement programme to improve survival after emergency abdominal surgery (EPOCH): A stepped-wedge cluster-randomised trial. Lancet 2019, 393, 2213–2221. [Google Scholar] [CrossRef]
- Habicher, M.; Balzer, F.; Mezger, V.; Niclas, J.; Müller, M.; Perka, C.; Krämer, M.; Sander, M. Implementation of goal-directed fluid therapy during hip revision arthroplasty: A matched cohort study. Perioper. Med. 2016, 5, 31. [Google Scholar] [CrossRef]
- Rinehart, J.; Alexander, B.; Le Manach, Y.; Hofer, C.; Tavernier, B.; Kain, Z.N.; Cannesson, M. Evaluation of a novel closed-loop fluid-administration system based on dynamic predictors of fluid responsiveness: An in silico simulation study. Crit. Care 2011, 15, R278. [Google Scholar] [CrossRef]
- Rinehart, J.; Lee, C.; Canales, C.; Kong, A.; Kain, Z.; Cannesson, M. Closed-loop fluid administration compared to anaesthesiologist management for hemodynamic optimization and resuscitation during surgery: An in vivo study. Anesth. Analg. 2013, 117, 1119–1129. [Google Scholar] [CrossRef]
- Rinehart, J.; Le Manach, Y.; Douiri, H.; Lee, C.; Lilot, M.; Le, K.; Canales, C.; Cannesson, M. First closed-loop goal directed fluid therapy during surgery: A pilot study. Ann. Fr. Anesth. Reanim. 2014, 33, 35–41. [Google Scholar] [CrossRef]
- Joosten, A.; Raj Lawrence, S.; Colesnicenco, A.; Coeckelenbergh, S.; Vincent, J.L.; Van der Linden, P.; Cannesson, M.; Rinehart, J. Personalized Versus Protocolized Fluid Management Using Noninvasive Hemodynamic Monitoring (Clearsight System) in Patients Undergoing Moderate-Risk Abdominal Surgery. Anesth. Analg. 2019, 129, e8–e12. [Google Scholar] [CrossRef]
- Toulouse, E.; Lafont, B.; Granier, S.; Mcgurk, G.; Bazin, J.E. French legal approach to patient consent in clinical research. Anaesth. Crit. Care Pain Med. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Simon, R. Optimal two-stage designs for phase II clinical trials. Control Clin. Trials 1989, 10, 1–10. [Google Scholar] [CrossRef]
- Joosten, A.; Hafiane, R.; Pustetto, M.; Obbergh, L.V.; Quackels, T.; Buggenhout, A.; Vincent, J.-L.; Ickx, B.; Rinehart, J. Practical impact of a decision support for goal-directed fluid therapy on protocol adherence: A clinical implementation study in patients undergoing major abdominal surgery. J. Clin. Monit. Comput. 2019, 33, 15–24. [Google Scholar] [CrossRef]
- Maheshwari, K.; Malhotra, G.; Bao, X.; Lahsaci, P.; Hand, W.R.; Fleming, N.W.; Ramsingh, D.; Treggiari, M.M.; Sessler, D.I.; Miller, T.E.; et al. Assisted fluid management software guidance for intraoperative fluid administration. Anesthesiology 2021, 135, 273–283. [Google Scholar] [CrossRef]
- Joosten, A.; Rinehart, J.; Van der Linden, P.; Brenton, A.; Penna, C.; De Montblanc, J.; Cannesson, M.; Vincent, J.-L.; Vicaut, E. Jacques Duranteau Computer-assisted Individualized Hemodynamic Management Reduces Intraoperative Hypotension in Intermediate- and High-risk Surgery: A Randomized Controlled Trial. Anesthesiology 2021, 135, 258–272. [Google Scholar] [CrossRef]
- Michard, F.; Teboul, J.L. Predicting fluid responsiveness in ICU patients: A critical analysis of the evidence. Chest 2002, 121, 2000–2008. [Google Scholar] [CrossRef]
- Cecconi, M.; Hofer, C.; Teboul, J.L.; Pettila, V.; Wilkman, E.; Molnar, Z.; Della Rocca, G.; Aldecoa, C.; Artigas, A.; Jog, S.; et al. Investigators F, Group ET: Fluid challenges in intensive care: The FENICE study: A global inception cohort study. Intensive Care Med. 2015, 41, 1529–1537. [Google Scholar] [CrossRef]
- Alexander, B.; Rinehart, J.; Cannesson, M.; Duranteau, J.; Joosten, A. Closed-loop hemodynamic management. Best Pract. Res. Clin. Anaesthesiol. 2019, 33, 199–209. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| BASELINE | |
| Age (years) | 61 (49–68) |
| Sex, No (%) | |
| Men | 10 (53%) |
| Height (cm) | 168 (162–176) |
| Weight (kg) | 69 (62–80) |
| BMI (kg/m2) | 26 (22–28) |
| Comorbidities, N (%) | |
| Hypertension | 7 (37%) |
| Complicated diabetes | 1 (5%) |
| Obesity (BMI > 30) | 2 (10.5%) |
| ASA, N (%) | |
| ASA I | 1 (5%) |
| ASA II | 14 (74%) |
| ASA III | 4 (21%) |
| ASA IV | 0 |
| Surgical procedure | |
| Type of procedure, N (%) | |
| Bowel resection | 8 (42%) |
| Pancreaticoduodenectomy | 5 (26%) |
| Adrenalectomy | 2 (11%) |
| Splenopancreatectomy | 2 (11%) |
| Others | 2 (10%) |
| Coloscopy | 10 (53%) |
| Laparoscopy | 9 (47%) |
| Epidural analgesia | 8 (42%) |
| Biology | |
| Baseline creatinine (µmol/L) | 73 (59–81) |
| Secondary Outcomes | |
| Overall median CI L/min/m2 | 2.9 (2.7–3.4) |
| Patients with mean CI was >2.5 L/min/m2 | 15 (79%) |
| Patients who spent ≥85% of their surgery time with a PPV <13% | 7/19 (37%) |
| Median CI coefficient of variation | 13 % (10–17) |
| Median arterial lactate at the end of surgery (mmol/L) | 1.1 (0.9–1.2) |
| Median serum creatinine on Day 1 (µmol/L) | 62 (56–76) |
| Median length of hospital stay (days) | 10 (5–14) |
| Median high dependency bed length of stay (days) | 4 (0–7) |
| Median time to oral liquid (days) | 2 (0.5–6) |
| Median time to solid intake (days) | 3 (1–9.5) |
| HR (bpm) | MAP (mmHg) | CI (L.min−1.m−2) | SVI (mL.m−2) | CV of CI (%) | % Time with CI ≥ 2.5 L.min−1.m−2 | %Time with PPV < 13% | |
|---|---|---|---|---|---|---|---|
| Patient # 1 | 63 ± 4 | 72 ± 9 | 2.74 ± 0.25 | 43 ± 3 | 9 | 89 | 92 |
| Patient # 2 | 84 ± 6 | 98 ± 12 | 3.84 ± 0.53 | 46 ± 5 | 14 | 98 | 40 |
| Patient # 3 | 75 ± 10 | 108 ± 12 | 2.35 ± 0.41 | 31 ± 2 | 17 | 45 | 72 |
| Patient # 4 | 55 ± 4 | 85 ± 17 | 3.64 ± 0.47 | 37 ± 3 | 13 | 100 | 93 |
| Patient # 5 | 99 ± 6 | 68 ± 8 | 5.55 ± 0.79 | 56 ± 9 | 14 | 100 | 42 |
| Patient # 6 | 68 ± 8 | 81 ± 10 | 1.92 ± 0.35 | 28 ± 3 | 18 | 0 | 68 |
| Patient # 7 | 86 ± 9 | 60 ± 9 | 4.38 ± 0.55 | 51 ± 2 | 13 | 100 | 90 |
| Patient # 8 | 63 ± 5 | 76 ± 11 | 2.89 ± 0.37 | 45 ± 4 | 13 | 92 | 10 |
| Patient # 9 | 59 ± 5 | 72 ± 10 | 2.28 ± 0.24 | 38 ± 3 | 11 | 14 | 82 |
| Patient # 10 | 75 ± 4 | 84 ± 7 | 3.07 ± 0.28 | 41 ± 2 | 9 | 100 | 94 |
| Patient # 11 | 70 ± 4 | 80 ± 6 | 3.05 ± 0.25 | 44 ± 3 | 8 | 99 | 39 |
| Patient # 12 | 63 ± 11 | 68 ± 11 | 2.26 ± 0.39 | 36 ± 3 | 17 | 32 | 46 |
| Patient # 13 | 65 ± 5 | 69 ± 9 | 2.93 ± 0.48 | 45 ± 5 | 16 | 84 | 33 |
| Patient # 14 | 60 ± 7 | 76 ± 20 | 2.89 ± 0.53 | 48 ± 9 | 18 | 76 | 89 |
| Patient # 15 | 74 ± 9 | 73 ± 8 | 2.66 ± 0.34 | 36 ± 2 | 13 | 71 | 76 |
| Patient # 16 | 59 ± 8 | 88 ± 11 | 2.73 ± 0.43 | 47 ± 4 | 16 | 75 | 53 |
| Patient # 17 | 78 ± 7 | 78 ± 14 | 3.10 ± 0.32 | 40 ± 2 | 10 | 96 | 79 |
| Patient # 18 | 71 ± 3 | 72 ± 9 | 3.41 ± 0.31 | 48 ± 4 | 9 | 100 | 98 |
| Patient # 19 | 84 ± 15 | 97 ±9 | 2.84 ± 0.48 | 34 ± 2 | 17 | 80 | 98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gricourt, Y.; Prin Derre, C.; Demattei, C.; Bertran, S.; Louart, B.; Muller, L.; Simon, N.; Lefrant, J.-Y.; Cuvillon, P.; Jaber, S.; et al. A Pilot Study Assessing a Closed-Loop System for Goal-Directed Fluid Therapy in Abdominal Surgery Patients. J. Pers. Med. 2022, 12, 1409. https://doi.org/10.3390/jpm12091409
Gricourt Y, Prin Derre C, Demattei C, Bertran S, Louart B, Muller L, Simon N, Lefrant J-Y, Cuvillon P, Jaber S, et al. A Pilot Study Assessing a Closed-Loop System for Goal-Directed Fluid Therapy in Abdominal Surgery Patients. Journal of Personalized Medicine. 2022; 12(9):1409. https://doi.org/10.3390/jpm12091409
Chicago/Turabian StyleGricourt, Yann, Camille Prin Derre, Christophe Demattei, Sébastien Bertran, Benjamin Louart, Laurent Muller, Natacha Simon, Jean-Yves Lefrant, Philippe Cuvillon, Samir Jaber, and et al. 2022. "A Pilot Study Assessing a Closed-Loop System for Goal-Directed Fluid Therapy in Abdominal Surgery Patients" Journal of Personalized Medicine 12, no. 9: 1409. https://doi.org/10.3390/jpm12091409