
Functional Neuroimaging in Dissociative Disorders: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
Quality Assessment Tool and Risk of Bias
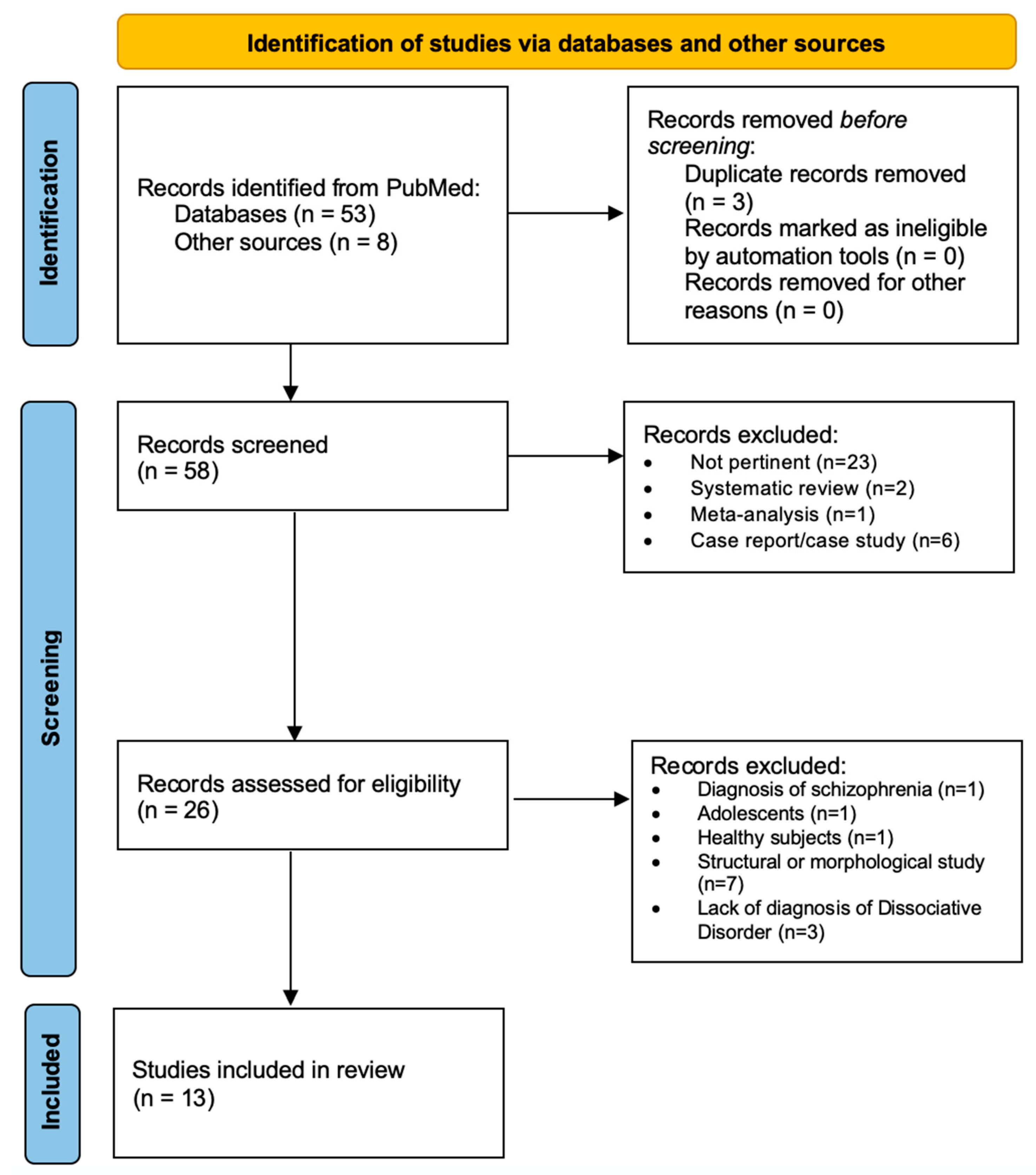
3. Results
4. Discussion
4.1. Functional Changes in the Limbic/Paralimbic System
4.2. Functional Changes in Frontal and Prefrontal Cortices
4.3. Functional Changes in Other Cortical Areas
4.4. Subcortical Functional Changes
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders V; American Psychiatric Association Publishing: Arlington, VA, USA, 2022; ISBN 0-89042-575-2. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders II; American Psychiatric Association Publishing: Arlington, VA, USA, 1968. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders III; American Psychiatric Association: Arlington, VA, USA, 1980. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders-IV-TR; American Psychiatric Association: Arlington, VA, USA, 2000; ISBN 0-89042-024-6. [Google Scholar]
- Spiegel, D.; Lewis-Ferńandez, R.; Lanius, R.; Vermetten, E.; Simeon, D.; Friedman, M. Dissociative disorders in DSM-5. Annu. Rev. Clin. Psychol. 2013, 9, 299–326. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, S.; Campodonico, C.; Varese, F. The relationship between childhood adversities and dissociation in severe mental illness: A meta-analytic review. Acta Psychiatr. Scand. 2018, 138, 509–525. [Google Scholar] [CrossRef] [PubMed]
- Vonderlin, R.; Kleindienst, N.; Alpers, G.W.; Bohus, M.; Lyssenko, L.; Schmahl, C. Dissociation in victims of childhood abuse or neglect: A meta-analytic review. Psychol. Med. 2018, 48, 2467–2476. [Google Scholar] [CrossRef] [PubMed]
- Putnam, F.W.; Guroff, J.J.; Silberman, E.K.; Barban, L.; Post, R.M. The clinical phenomenology of multiple personality disorder: Review of 100 recent cases. J. Clin. Psychiatry 1986, 47, 285–293. [Google Scholar]
- Schultz, R.; Braun, B.G.; Kluft, R.P. Multiple personality disorder: Phenomenology of selected variables in comparison to major depression. Dissociation Prog. Dissociative Disord. 1989, 2, 45–51. [Google Scholar]
- Baker, D.; Hunter, E.; Lawrence, E.; Medford, N.; Patel, M.; Senior, C.; Sierra, M.; Lambert, M.V.; Phillips, M.L.; David, A.S. Depersonalisation disorder: Clinical features of 204 cases. Br. J. Psychiatry 2003, 182, 428–433. [Google Scholar] [CrossRef]
- Michal, M.; Adler, J.; Wiltink, J.; Reiner, I.; Tschan, R.; Wölfling, K.; Weimert, S.; Tuin, I.; Subic-Wrana, C.; Beutel, M.E.; et al. A case series of 223 patients with depersonalization-derealization syndrome. BMC Psychiatry 2016, 16, 203. [Google Scholar] [CrossRef]
- Mathew, R.J.; Jack, R.A.; West, W.S. Regional cerebral blood flow in a patient with multiple personality. Am. J. Psychiatry 1985, 142, 504–505. [Google Scholar] [CrossRef]
- Saxe, G.N.; Vasile, R.G.; Hill, T.C.; Bloomingdale, K.; Van Der Kolk, B.A. SPECT imaging and multiple personality disorder. J. Nerv. Ment. Dis. 1992, 180, 662–663. [Google Scholar] [CrossRef]
- Elzinga, B.M.; Ardon, A.M.; Heijnis, M.K.; De Ruiter, M.B.; Van Dyck, R.; Veltman, D.J. Neural correlates of enhanced working-memory performance in dissociative disorder: A functional MRI study. Psychol. Med. 2007, 37, 235–245. [Google Scholar] [CrossRef]
- Tsai, G.E.; Condie, D.; Wu, M.T.; Chang, I.W. Functional magnetic resonance imaging of personality switches in a woman with dissociative identity disorder. Harv. Rev. Psychiatry 1999, 7, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Lanius, R.A.; Vermetten, E.; Loewenstein, R.J.; Brand, B.; Schmahl, C.; Bremner, J.D.; Spiegel, D. Emotion Modulation in PTSD: Clinical and Neurobiological Evidence for a Dissociative Subtype. Am. J. Psychiatry 2010, 167, 640–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sierra, M.; Berrios, G. Depersonalization: Neurobiological perspectives. Biol. Psychiatry 1998, 4, 898–908. [Google Scholar] [CrossRef]
- Eddy, C.M. The junction between self and other? Temporo-parietal dysfunction in neuropsychiatry. Neuropsychologia 2016, 89, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Blanke, O.; Ortigue, S.; Landis, T.; Seeck, M. Stimulating illusory own-body perceptions. Nature 2002, 419, 269–270. [Google Scholar] [CrossRef]
- Blanke, O.; Mohr, C.; Michel, C.M.; Pascual-Leone, A.; Brugger, P.; Seeck, M.; Landis, T.; Thut, G. Linking out-of-body experience and self processing to mental own-body imagery at the temporoparietal junction. J. Neurosci. 2005, 25, 550–557. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Scottish Intercollegiate Guidelines Network SIGN Assessment Tool. Available online: https://www.sign.ac.uk/what-we-do/methodology/checklists/ (accessed on 21 August 2022).
- Chechko, N.; Stickel, S.; Kellermann, T.; Kirner, A.; Habel, U.; Fernández, G.; Schneider, F.; Kohn, N. Progressively analogous evidence of covert face recognition from functional magnetic resonance imaging and skin conductance responses studies involving a patient with dissociative amnesia. Eur. J. Neurosci. 2018, 48, 1964–1975. [Google Scholar] [CrossRef]
- Savoy, R.L.; Frederick, B.B.; Keuroghlian, A.S.; Wolk, P.C. Voluntary switching between identities in dissociative identity disorder: A functional MRI case study. Cogn. Neurosci. 2012, 3, 112–119. [Google Scholar] [CrossRef]
- Thomas-Antérion, C.; Dubas, F.; Decousus, M.; Jeanguillaume, C.; Guedj, E. Clinical characteristics and brain PET findings in 3 cases of dissociative amnesia: Disproportionate retrograde deficit and posterior middle temporal gyrus hypometabolism. Neurophysiol. Clin. 2014, 44, 355–362. [Google Scholar] [CrossRef]
- Kitamura, S.; Yasuno, F.; Inoue, M.; Kosaka, J.; Kiuchi, K.; Matsuoka, K.; Kishimoto, T.; Suhara, T. Increased binding of 5-HT1A receptors in a dissociative amnesic patient after the recovery process. Psychiatry Res. 2014, 224, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Back, T.; Haag, C.; Buchberger, A.; Mayer, T. [Diffusion-weighted MR imaging in a case of dissociative amnesia]. Nervenarzt 1998, 69, 909–912. [Google Scholar] [CrossRef] [PubMed]
- Comparelli, A.; Kotzalidis, G.D.; Di Pietro, S.; Del Casale, A.; De Carolis, A. A case of rapid conversion to psychosis of delusional misidentification associated with derealisation, verbal memory impairment and FDG-PET imaging abnormalities. Eur. Child Adolesc. Psychiatry 2014, 23, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Mutluer, T.; Şar, V.; Kose-Demiray, Ç.; Arslan, H.; Tamer, S.; Inal, S.; Kaçar, A.Ş. Lateralization of Neurobiological Response in Adolescents with Post-Traumatic Stress Disorder Related to Severe Childhood Sexual Abuse: The Tri-Modal Reaction (T-MR) Model of Protection. J. Trauma Dissociation 2018, 19, 108–125. [Google Scholar] [CrossRef]
- Veltman, D.J.; de Ruiter, M.B.; Rombouts, S.A.R.B.; Lazeron, R.H.C.; Barkhof, F.; Van Dyck, R.; Dolan, R.J.; Phaf, R.H. Neurophysiological correlates of increased verbal working memory in high-dissociative participants: A functional MRI study. Psychol. Med. 2005, 35, 175–185. [Google Scholar] [CrossRef]
- Reinders, A.A.T.S.; Chalavi, S.; Schlumpf, Y.R.; Vissia, E.M.; Nijenhuis, E.R.S.; Jäncke, L.; Veltman, D.J.; Ecker, C. Neurodevelopmental origins of abnormal cortical morphology in dissociative identity disorder. Acta Psychiatr. Scand. 2018, 137, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, L.I.; Dean, S.L.; Schlumpf, Y.R.; Vissia, E.M.; Nijenhuis, E.R.S.; Chatzi, V.; Jäncke, L.; Veltman, D.J.; Chalavi, S.; Reinders, A.A.T.S. A neurostructural biomarker of dissociative amnesia: A hippocampal study in dissociative identity disorder. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Schlumpf, Y.R.; Reinders, A.A.T.S.; Nijenhuis, E.R.S.; Luechinger, R.; van Osch, M.J.P.; Jäncke, L. Dissociative part-dependent resting-state activity in dissociative identity disorder: A controlled FMRI perfusion study. PLoS ONE 2014, 9, e98795. [Google Scholar] [CrossRef]
- Reinders, A.A.T.S.; Willemsen, A.T.M.; den Boer, J.A.; Vos, H.P.J.; Veltman, D.J.; Loewenstein, R.J. Opposite brain emotion-regulation patterns in identity states of dissociative identity disorder: A PET study and neurobiological model. Psychiatry Res. 2014, 223, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Chalavi, S.; Vissia, E.M.; Giesen, M.E.; Nijenhuis, E.R.S.; Draijer, N.; Barker, G.J.; Veltman, D.J.; Reinders, A.A.T.S. Similar cortical but not subcortical gray matter abnormalities in women with posttraumatic stress disorder with versus without dissociative identity disorder. Psychiatry Res. 2015, 231, 308–319. [Google Scholar] [CrossRef]
- Daniels, J.K.; Gaebler, M.; Lamke, J.-P.; Walter, H. Grey matter alterations in patients with depersonalization disorder: A voxel-based morphometry study. J. Psychiatry Neurosci. 2015, 40, 19–27. [Google Scholar] [CrossRef]
- Irle, E.; Lange, C.; Weniger, G.; Sachsse, U. Size abnormalities of the superior parietal cortices are related to dissociation in borderline personality disorder. Psychiatry Res. 2007, 156, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.R.; Farmer, M.; Kämpe, R.; Cremers, H.R.; Hamilton, J.P. Functional Connectivity Between Extrastriate Body Area and Default Mode Network Predicts Depersonalization Symptoms in Major Depression: Findings From an A Priori Specified Multinetwork Comparison. Biol. Psychiatry. Cogn. Neurosci. Neuroimaging 2019, 4, 627–635. [Google Scholar] [CrossRef] [PubMed]
- Oda, K.; Matsushima, E.; Okubo, Y.; Ohta, K.; Murata, Y.; Koike, R.; Miyasaka, N.; Kato, M. Abnormal regional cerebral blood flow in systemic lupus erythematosus patients with psychiatric symptoms. J. Clin. Psychiatry 2005, 66, 907–913. [Google Scholar] [CrossRef]
- Fauvé, P.; Tyvaert, L.; Husson, C.; Hologne, E.; Gao, X.; Maillard, L.; Schwan, R.; Banasiak, C.; El-Hage, W.; Hossu, G.; et al. Functional MRI-based study of emotional experience in patients with psychogenic non-epileptic seizures: Protocol for an observational case-control study-EMOCRISES study. PLoS ONE 2022, 17, e0262216. [Google Scholar] [CrossRef] [PubMed]
- Schlumpf, Y.R.; Nijenhuis, E.R.S.; Chalavi, S.; Weder, E.V.; Zimmermann, E.; Luechinger, R.; La Marca, R.; Reinders, A.A.T.S.; Jäncke, L. Dissociative part-dependent biopsychosocial reactions to backward masked angry and neutral faces: An fMRI study of dissociative identity disorder. NeuroImage. Clin. 2013, 3, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Brand, M.; Eggers, C.; Reinhold, N.; Fujiwara, E.; Kessler, J.; Heiss, W.-D.; Markowitsch, H.J. Functional brain imaging in 14 patients with dissociative amnesia reveals right inferolateral prefrontal hypometabolism. Psychiatry Res. 2009, 174, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Vissia, E.M.; Lawrence, A.J.; Chalavi, S.; Giesen, M.E.; Draijer, N.; Nijenhuis, E.R.S.; Aleman, A.; Veltman, D.J.; Reinders, A.A.T.S. Dissociative identity state-dependent working memory in dissociative identity disorder: A controlled functional magnetic resonance imaging study. BJPsych Open 2022, 8, e82. [Google Scholar] [CrossRef]
- Reinders, A.A.T.S.; Nijenhuis, E.R.S.; Quak, J.; Korf, J.; Haaksma, J.; Paans, A.M.J.; Willemsen, A.T.M.; den Boer, J.A. Psychobiological characteristics of dissociative identity disorder: A symptom provocation study. Biol. Psychiatry 2006, 60, 730–740. [Google Scholar] [CrossRef]
- Ketay, S.; Hamilton, H.K.; Haas, B.W.; Simeon, D. Face processing in depersonalization: An fMRI study of the unfamiliar self. Psychiatry Res. 2014, 222, 107–110. [Google Scholar] [CrossRef]
- Weniger, G.; Siemerkus, J.; Barke, A.; Lange, C.; Ruhleder, M.; Sachsse, U.; Schmidt-Samoa, C.; Dechent, P.; Irle, E. Egocentric virtual maze learning in adult survivors of childhood abuse with dissociative disorders: Evidence from functional magnetic resonance imaging. Psychiatry Res. 2013, 212, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Medford, N.; Brierley, B.; Brammer, M.; Bullmore, E.T.; David, A.S.; Phillips, M.L. Emotional memory in depersonalization disorder: A functional MRI study. Psychiatry Res. 2006, 148, 93–102. [Google Scholar] [CrossRef]
- Lemche, E.; Surguladze, S.A.; Giampietro, V.P.; Anilkumar, A.; Brammer, M.J.; Sierra, M.; Chitnis, X.; Williams, S.C.R.; Gasston, D.; Joraschky, P.; et al. Limbic and prefrontal responses to facial emotion expressions in depersonalization. Neuroreport 2007, 18, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Lemche, E.; Sierra-Siegert, M.; David, A.S.; Phillips, M.L.; Gasston, D.; Williams, S.C.R.; Giampietro, V.P. Cognitive load and autonomic response patterns under negative priming demand in depersonalization-derealization disorder. Eur. J. Neurosci. 2016, 43, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Reinders, A.A.T.S.; Willemsen, A.T.M.; Vissia, E.M.; Vos, H.P.J.; den Boer, J.A.; Nijenhuis, E.R.S. The Psychobiology of Authentic and Simulated Dissociative Personality States: The Full Monty. J. Nerv. Ment. Dis. 2016, 204, 445–457. [Google Scholar] [CrossRef]
- David, S.P.; Ware, J.J.; Chu, I.M.; Loftus, P.D.; Fusar-Poli, P.; Radua, J.; Munafò, M.R.; Ioannidis, J.P.A. Potential reporting bias in fMRI studies of the brain. PLoS ONE 2013, 8, e70104. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Fink, G.R.; Markowitsch, H.J.; Reinkemeier, M.; Bruckbauer, T.; Kessler, J.; Heiss, W.-D. Cerebral Representation of One’s Own Past: Neural Networks Involved in Autobiographical Memory. J. Neurosci. 1996, 16, 4275–4282. [Google Scholar] [CrossRef]
- Tulving, E.; Kapur, S.; Craik, F.I.M.; Moscovitch, M.; Houle, S. Hemispheric encoding/retrieval asymmetry in episodic memory: Positron emission tomography findings. Proc. Natl. Acad. Sci. USA 1994, 91, 2016–2020. [Google Scholar] [CrossRef]
- Del Casale, A.; Kotzalidis, G.D.; Rapinesi, C.; Janiri, D.; Aragona, M.; Puzella, A.; Spinazzola, E.; Maggiora, M.; Giuseppin, G.; Tamorri, S.M.; et al. Neural functional correlates of empathic face processing. Neurosci. Lett. 2017, 655, 68–75. [Google Scholar] [CrossRef]
- Botvinick, M.M.; Cohen, J.D.; Carter, C.S. Conflict monitoring and anterior cingulate cortex: An update. Trends Cogn. Sci. 2004, 8, 539–546. [Google Scholar] [CrossRef]
- Del Casale, A.; Ferracuti, S.; Barbetti, A.S.; Bargagna, P.; Zega, P.; Iannuccelli, A.; Caggese, F.; Zoppi, T.; De Luca, G.P.; Parmigiani, G.; et al. Grey Matter Volume Reductions of the Left Hippocampus and Amygdala in PTSD: A Coordinate-Based Meta-Analysis of Magnetic Resonance Imaging Studies. Neuropsychobiology 2022, 81, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Serova, L.I.; Nwokafor, C.; Van Bockstaele, E.J.; Reyes, B.A.S.; Lin, X.; Sabban, E.L. Single prolonged stress PTSD model triggers progressive severity of anxiety, altered gene expression in locus coeruleus and hypothalamus and effected sensitivity to NPY. Eur. Neuropsychopharmacol. 2019, 29, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Serova, L.; Mulhall, H.; Sabban, E. NPY1 Receptor Agonist Modulates Development of Depressive-Like Behavior and Gene Expression in Hypothalamus in SPS Rodent PTSD Model. Front. Neurosci. 2017, 11, 203. [Google Scholar] [CrossRef]
- Schmitz, T.W.; Johnson, S.C. Self-appraisal decisions evoke dissociated dorsal-ventral aMPFC networks. Neuroimage 2006, 30, 1050–1058. [Google Scholar] [CrossRef]
- Marsh, R.; Zhu, H.; Schultz, R.T.; Quackenbush, G.; Royal, J.; Skudlarski, P.; Peterson, B.S. A developmental fMRI study of self-regulatory control. Hum. Brain Mapp. 2006, 27, 848–863. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.L.; Drevets, W.C.; Rauch, S.L.; Lane, R. Neurobiology of emotion perception I: The neural basis of normal emotion perception. Biol. Psychiatry 2003, 54, 504–514. [Google Scholar] [CrossRef]
- Kostopoulos, P.; Petrides, M. The mid-ventrolateral prefrontal cortex: Insights into its role in memory retrieval. Eur. J. Neurosci. 2003, 17, 1489–1497. [Google Scholar] [CrossRef]
- Hiser, J.; Koenigs, M. The Multifaceted Role of the Ventromedial Prefrontal Cortex in Emotion, Decision Making, Social Cognition, and Psychopathology. Biol. Psychiatry 2018, 83, 638–647. [Google Scholar] [CrossRef]
- Krystal, J.; Bennett, A.; Bremner, J.; Southwitck, S.; Charney, D. Toward a cognitive neuroscience of dissociation and altered memory functions in post-traumatic stress disorder. In Neurobiological and Clinical Consequences of Stress: From Normal Adaptions to PTSD; Raven Press: New York, NY, USA, 1995; pp. 239–268. [Google Scholar]
- Steuber, E.R.; Seligowski, A.V.; Roeckner, A.R.; Reda, M.; Lebois, L.A.M.; van Rooij, S.J.H.; Murty, V.P.; Ely, T.D.; Bruce, S.E.; House, S.L.; et al. Thalamic volume and fear extinction interact to predict acute posttraumatic stress severity. J. Psychiatr. Res. 2021, 141, 325–332. [Google Scholar] [CrossRef]
- Del Casale, A.; Kotzalidis, G.D.; Rapinesi, C.; Serata, D.; Ambrosi, E.; Simonetti, A.; Pompili, M.; Ferracuti, S.; Tatarelli, R.; Girardi, P. Functional neuroimaging in obsessive-compulsive disorder. Neuropsychobiology 2011, 64, 61–85. [Google Scholar] [CrossRef] [PubMed]
- Del Casale, A.; Rapinesi, C.; Kotzalidis, G.D.; De Rossi, P.; Curto, M.; Janiri, D.; Criscuolo, S.; Alessi, M.C.; Ferri, V.R.; De Giorgi, R.; et al. Executive functions in obsessive–compulsive disorder: An activation likelihood estimate meta-analysis of fMRI studies. World J. Biol. Psychiatry 2016, 17, 378–393. [Google Scholar] [CrossRef] [PubMed]
- LeDoux, J.E. Emotion circuits in the brain. Annu. Rev. Neurosci. 2000, 23, 155–184. [Google Scholar] [CrossRef] [PubMed]
- Reiman, E.M. The application of positron emission tomography to the study of normal and pathologic emotions. J. Clin. Psychiatry 1997, 58, 4–12. [Google Scholar] [PubMed]
- Reinders, A.A.T.S.; Willemsen, A.T.M.; Vos, H.P.J.; den Boer, J.A.; Nijenhuis, E.R.S. Fact or factitious? A psychobiological study of authentic and simulated dissociative identity States. PLoS ONE 2012, 7, e39279. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Article | Tech | Participants | Age | Medications | Comorbidity | General Findings |
|---|---|---|---|---|---|---|
| Brand et al., 2009 | PET | -Patients: 14 (11 males and 4 females) with Dissociative Amnesia (DSM-IV) | -Patients’ mean age: 36.57 years | -1 headache, migraine | Compared to controls, dissociative patients showed a significantly decreased glucose utilization in the right inferolateral prefrontal cortex. | |
| Functional brain imaging in 14 patients with dissociative amnesia reveals right inferolateral prefrontal hypometabolism | -Control group: 19 healthy individuals (13 males and 6 females) without neurological or psychiatric history | -Controls’ mean age: 45.32 years | -1 closed head injury with headache, ataxia, right arm hemiparesis, diagnosis of conversion hysteria, diffuse abdominal and chest pain without organic causation | |||
| -1 motor symptoms (potential mild apoplexy) | ||||||
| -1 hypothyroidism | ||||||
| Elzinga et al., 2007 | fMRI | All participants were female | -Patients’ mean age: 40.8 (±10.7) | -1 mirtazapine (30 mg/day) and venlafaxine (75 mg/day) | Patients’ co-morbid diagnoses: | Both patients and controls activated brain regions involved in working memory (anterior, dorsolateral, and ventrolateral prefrontal cortex and parietal cortex). |
| -Patients: 7 diagnosed with DID; 6 diagnosed with Dissociative Disorder NOS (DSM-IV, SCID-D) | ||||||
| Neural correlates of enhanced working-memory performance in dissociative disorder: a functional MRI study. | -Controls: 16 healthy subjects without psychiatric disorder history | -Controls’ mean age: 34.6 (±10.9) | -1 citalopram 70 mg/day | -12 PTSD | Dissociative patients showed more engagement of left anterior prefrontal cortex, dorsolateral prefrontal cortex, and parietal cortex. | |
| RoB: high | All other participants were free of medication | -2 Major depressive Disorder | ||||
| Possible cause of heterogeneity: two different diagnoses in the study sample | -4 Dysthymia | |||||
| Patients’ history: | ||||||
| -10 Major depressive disorder | ||||||
| -6 Alcohol abuse | ||||||
| -3 Substance abuse | ||||||
| Ketay et al., 2014 | fMRI | -9 participants with Depersonalization Disorder diagnosis | Participants’ age: 18–55 years | Participants were medically and neurologically healthy subjects, besides their psychiatric diagnosis | Compared to controls, dissociative patients showed significantly more activation in right anterior cingulate cortex, bilateral medial prefrontal cortex, and left middle frontal gyrus in response to self vs. stranger faces. | |
| Face processing in depersonalization: An fMRI study of the unfamiliar self | (SCID-I/P, SCID-II, SCID-D) | |||||
| -10 control participants (Dissociative Experiences Scale’s score < 10) | ||||||
| Lemche et al., 2007 | fMRI | -9 patients (4 female, 5 male) with Depersonalization diagnosis (DSM-IV criteria) | -Patients: 36.1 ± 2.3 years | -3 paroxetine, fluoxetine, olanzapine (medicated with lowest effective doses) | 6 patients had a secondary comorbidity of anxiety or depression (psychotic symptoms had been excluded) | When exposed to happy and sad facial expressions, patients showed lower subcortical limbic activity and negative correlations between skin conductance measures in bilateral dorsal prefrontal cortices. |
| Limbic and prefrontal responses to facial emotion expressions in depersonalization | -12 healthy subjects (5 female, 7 male) | -Controls: 27.3 ± 1.9 years | - 6 no medication | |||
| Lemche et al., 2016 | fMRI | -9 patients with diagnosis of Depersonalization Derealization Disorder | -Patients: mean age 36.11 (±2.34) years | Patients showed slight neuropsychological deficits in terms of reduced short-term memory, distractibility, and inability to suppress stress-related arousal states under cognitive task, but selective attention, cognitive inhibition and working memory were not impaired overall. | ||
| Cognitive load and autonomic response patterns under negative priming demand in depersonalization derealization disorder | (DSM-V criteria) | |||||
| -12 healthy control subjects | -Controls: mean age 27.25 (±1.95) years | |||||
| Medford et al., 2006 | fMRI | -10 patients (9 male, 1 female with diagnosis of Depersonalization Disorder (DSM-IV criteria) | Patients: 23–50 years (mean age 31.2, SD = 9.3) | -2 fluoxetine (40 mg/day) | Dissociative patients showed stronger recognition for clearly emotive words, but not for neutral words encoded in an emotive context. Furthermore, patients did not show activation of emotional processing areas during encoding process. | |
| Emotional memory in depersonalization disorder: A functional MRI study | -12 healthy male controls | Controls: 22–34 years (mean age 27.8, SD = 3.6) | -3 lamotrigine (250 mg/day) | |||
| -1 lamotrigine (50 mg/day) and paroxetine (40 mg/day) | ||||||
| -4 no medication | ||||||
| Reinders et al., 2006 | PET | 11 female patients with DID (according to DSM-IV criteria and SCID-D) | Patients’ age: 27–48 years | Exclusion criteria: pregnancy, traumatic experiences in a hospital setting, systemic or neurological illness, and no command of the Dutch language | PET data revealed different neural networks to be associated with different | |
| Psychobiological Characteristics of Dissociative Identity Disorder: A Symptom Provocation Study | processing of the neutral and trauma-related memory script by neutral-related state and trauma-related state. | |||||
| Reinders et al., 2014 | PET | -11 patients (all female) with diagnosis of DID (DSM-IV, SCID-D) | -Patients’ mean age = 41.0, SD = 6.1) | Exclusion criteria: pregnancy, traumatic experiences in a hospital setting, systemic or neurological illness, and no command of the Dutch language. | DID patients showed similar pattern of activation to PTSD model. | |
| Opposite brain emotion-regulation patterns in identity states of dissociative identity disorder: A PET study and neurobiological model | -16 healthy control subjects (all female) without psychiatric disease or current or past trauma-related problems, instructed to simulate dissociative identity states | -Controls’ mean age = 41.1, SD = 10.7) | The hypo-aroused identity | |||
| state activates the prefrontal cortex, cingulate, posterior association areas, and parahippocampal gyri (overmodulating emotion regulation), whereas the hyper-aroused identity state activates the amygdala, | ||||||
| the insula, and the dorsal striatum, (undermodulating emotion regulation). | ||||||
| Reinders et al., 2016 | PET | 29 subjects: | -Patients: mean age 41.0 (SD = 6.1) | Prefrontal hyperactivation during neutral personality state in response to trauma-related words vs. neutral words. | ||
| The Psychobiology of Authentic and Simulated Dissociative Personality States: The Full Monty | -11 patients with DID (DSM-IV) | Right hippocampus and left amygdala different activation patterns have been associated with DID. | ||||
| -18 mentally healthy control individuals (all female): 10 high-fantasy-prone DID-simulating, 8 low-fantasy-prone DID-simulating (without history potentially traumatizing events) | -High-fantasy-prone DID-simulating controls: mean age 38.2 (SD = 10.9) | Involvement of the caudate nucleus both in the switch between identity states and in the maintenance of the altered identity state. | ||||
| Controls were instructed to simulate different dissociative personality states and write the autobiographical analog “neutral” and “trauma” memory scripts. | -Low-fantasy-prone DID-simulating controls: mean age 42.5 (SD = 10.1) | |||||
| Schlumpf et al., 2013 | fMRI | -Patients: 15 females with Dissociative Identity Disorder diagnosis (DSM-IV criteria and SCID-D), considering the ANP and EP prototypes of DID. | -DID group mean age: 43.3 years (SD = 9.1) | -13 patients: mainly antidepressant | Exclusion criteria: | Compared to DID-ANP, DID-EP showed longest reaction times when exposed to neutral faces and more involvement of the parahippocampal gyrus. |
| Dissociative part-dependent biopsychosocial reactions to backward masked angry and neutral faces: An fMRI study of dissociative identity disorder. | -DID simulating control group: 15 female actors, who were instructed to simulate DID-ANP and DID-EP. | -Simulating control group mean age: 43.2 years (SD = 10.4) | -2 patients: no medication | -comorbid psychosis, drug abuse or addiction, antisocial or histrionic personality disorder, neurological or organic brain disease | When compared to EP-simulating subjects, DID-EP showed more involvement in the brainstem, face-sensitive regions, and motor-related areas. | |
| DID-ENP, when exposed to neutral and angry faces, showed a decreased activation all over the brain. | ||||||
| Schlumpf et al., 2014 | fMRI | -Patients: 15 females with Dissociative Identity Disorder diagnosis (DSM-IV criteria and SCID-D), considering the ANP and EP prototypes of DID. | -DID group mean age: 43.3 years (SD =9.1) | -13 patients: mainly antidepressant | Exclusion criteria: comorbid psychosis, drug abuse or addiction, antisocial or histrionic personality disorder, neurological or organic brain disease | ANP-EP comparison: ANP perfusion patterns showed elevated involvement of bilateral thalamus, EP showed increased perfusion in the dorsomedial prefrontal cortex, primary somatosensory cortex, and motor-related areas. |
| Dissociative Part-Dependent Resting-State Activity in Dissociative Identity Disorder: A Controlled fMRI Perfusion Study | -DID simulating control group: 15 female actors, who were instructed to simulate DID-ANP and DID-EP. | -Simulating control group mean age: 43.2 years (SD = 10.4) | -2 patients: no medication | ANP and EP- simulating controls fitted their role-play strategies, activating brain structures involved in visual mental images and empathizing feelings. | ||
| (The sample was part of a larger study) | ||||||
| Vissia et al., 2022 | fMRI | 62 female participants: | The sample was part of a larger multicenter study | Results showed the activation of prefrontal parietal network, main working memory in the left frontal pole and ventrolateral prefrontal cortex in all three simulated neutral states and in trauma-related identity states of DID-simulators, but not in trauma-related identity state of DID-patients and PTSD-patients, which did not activate parietal regions. | ||
| Dissociative identity state-dependent working memory in dissociative identity disorder: a controlled functional magnetic resonance imaging study | -14 patients diagnosed with Dissociative Identity Disorder | |||||
| -16 DID-simulating healthy controls | ||||||
| -a paired of control group: 16 subjects with PTSD and 16 healthy controls (control group consisting of NIS and TIS) | ||||||
| Weniger et al., 2013 | fMRI | -Patients: 14 female inpatients with history of childhood abuse and a diagnoses of Dissociative Amnesia or DID (DSM-IV, SCID-D) | -Patients’ age: 24–50 years | -7 patients were medicated with antidepressant: doxepine, mirtazapine, fluoxetine, paroxetine, venlafaxine, duloxetine | -10 Dissociative Amnesia | Compared to controls, dissociative patients showed a similar (although weaker) pattern of activity changes during egocentric learning. Dissociative disorder severity was associated to better performance and to stronger activity in cingulate gyrus and precuneus. Attentional and visuospatial mnemonic functioning were preserved in individuals with dissociative disorder. |
| Egocentric virtual maze learning in adult survivors of childhood abuse with dissociative disorders: Evidence from functional magnetic resonance imaging | -Controls: 14 healthy females (no neurological or psychiatric history, no traumatic exposure history) | -Controls’ age: | -4 patients were medicated with antipsychotics (aripiprazole, quetiapine) | -10 DID | ||
| RoB: high | 21–48 years | -3 patients were free of psychotropic medications | -4 Depersonalization Disorder | |||
| Possible cause of heterogeneity: two different diagnoses in the study sample | -12 Borderline Personality Disorder | |||||
| -6 Major Depression | ||||||
| -9 Anxiety Disorder | ||||||
| Exclusion criteria: history of PTSD, psychotic disorder, neurological disorder, current substance use |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Modesti, M.N.; Rapisarda, L.; Capriotti, G.; Del Casale, A. Functional Neuroimaging in Dissociative Disorders: A Systematic Review. J. Pers. Med. 2022, 12, 1405. https://doi.org/10.3390/jpm12091405
Modesti MN, Rapisarda L, Capriotti G, Del Casale A. Functional Neuroimaging in Dissociative Disorders: A Systematic Review. Journal of Personalized Medicine. 2022; 12(9):1405. https://doi.org/10.3390/jpm12091405
Chicago/Turabian StyleModesti, Martina Nicole, Ludovica Rapisarda, Gabriela Capriotti, and Antonio Del Casale. 2022. "Functional Neuroimaging in Dissociative Disorders: A Systematic Review" Journal of Personalized Medicine 12, no. 9: 1405. https://doi.org/10.3390/jpm12091405