
Thiopurine S-Methyltransferase Polymorphisms Predict Hepatotoxicity in Azathioprine-Treated Patients with Autoimmune Diseases

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Study Population
2.3. Data Collection
2.4. TMPT Genotyping
2.5. Statistical Analysis
3. Results
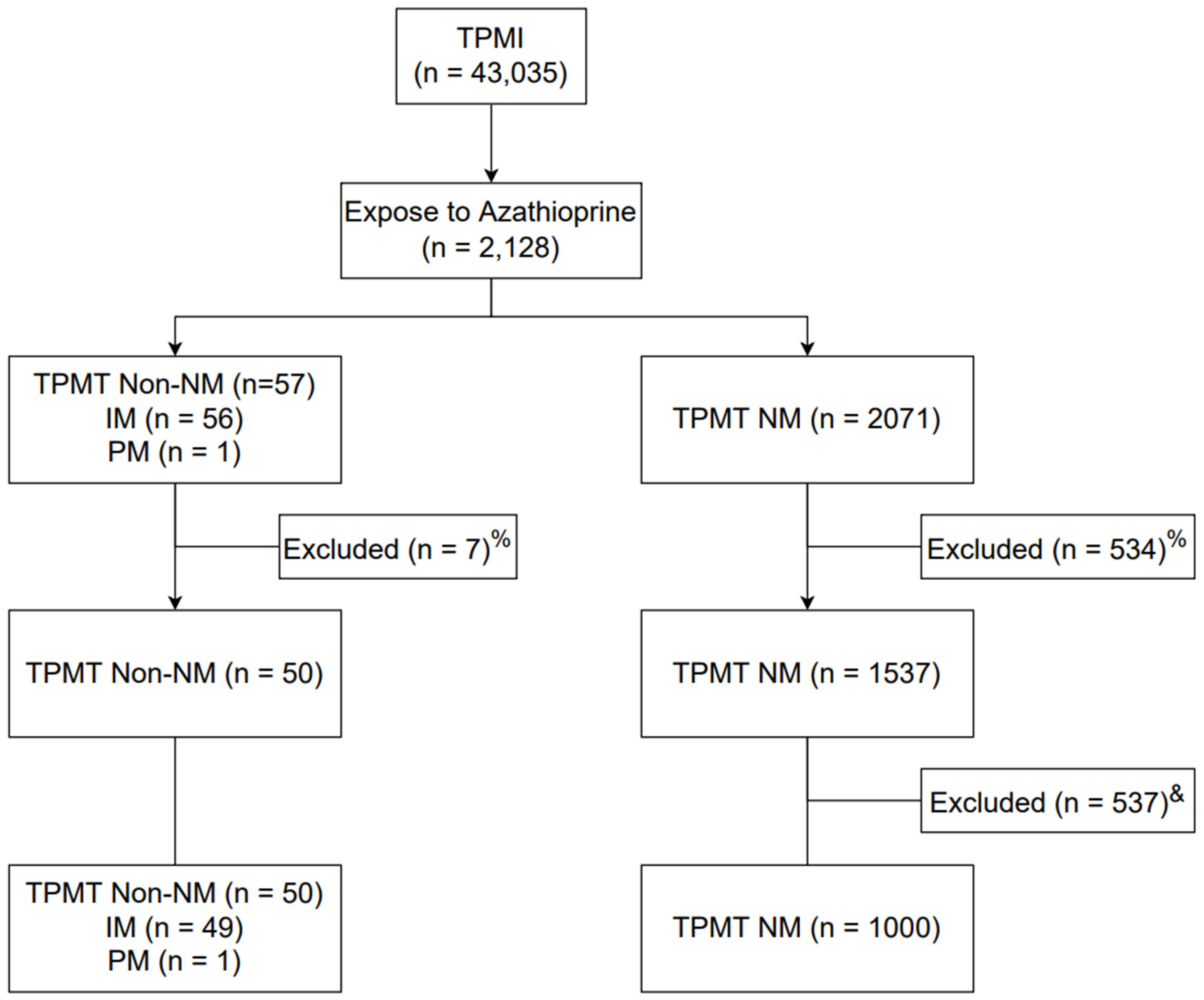
3.1. Study Patient Flow
3.2. Demographics of the Selected Patients
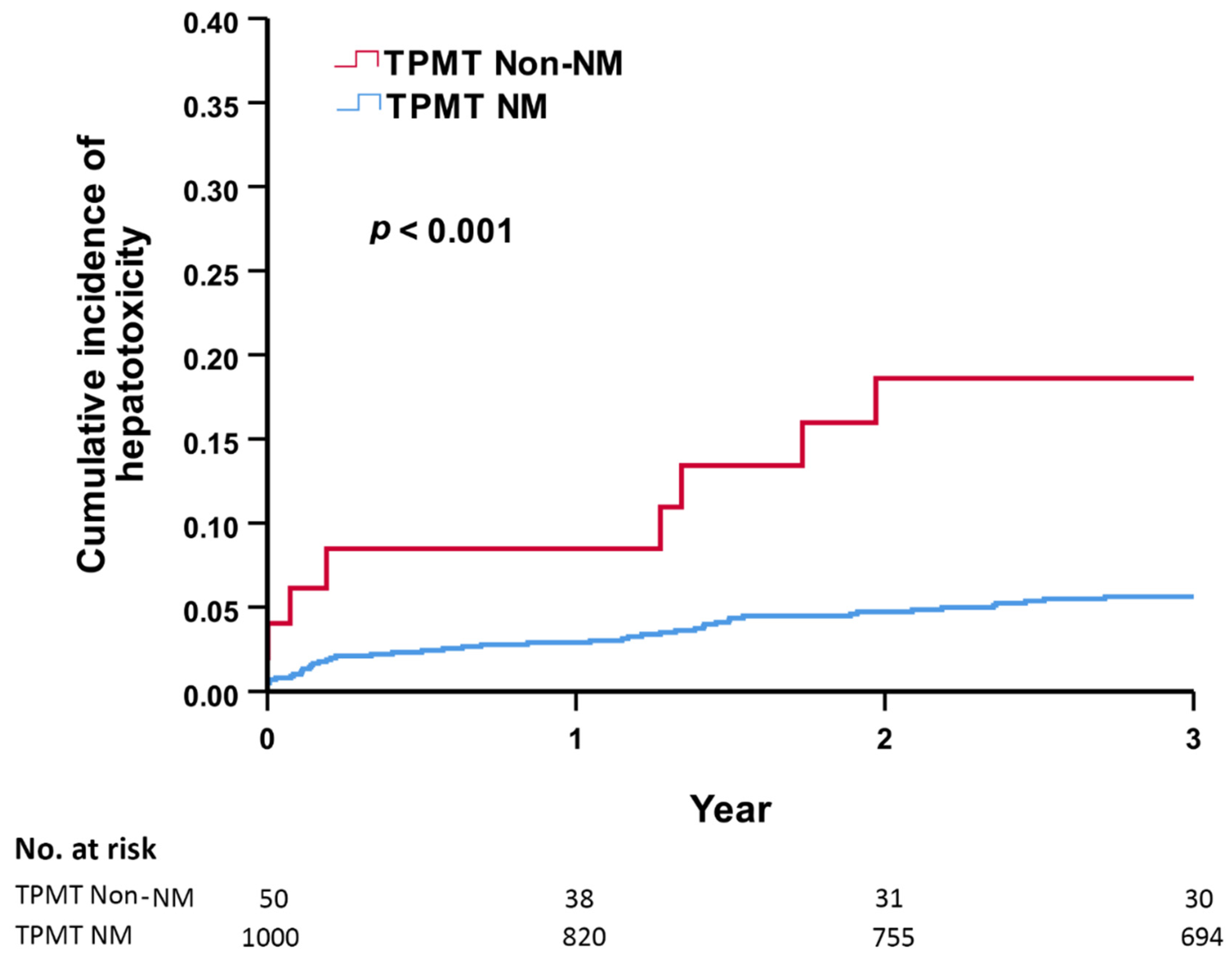
3.3. TPMT Phenotypes and Risks of Hepatotoxicity and Leukopenia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pego-Reigosa, J.M.; Cobo-Ibáñez, T.; Calvo-Alén, J.; Loza-Santamaría, E.; Rahman, A.; Muñoz-Fernández, S.; Rúa-Figueroa, Í. Efficacy and Safety of Nonbiologic Immunosuppressants in the Treatment of Nonrenal Systemic Lupus Erythematosus: A Systematic Review. Arthritis Care Res. 2013, 65, 1775–1785. [Google Scholar] [CrossRef] [PubMed]
- Bertsias, G.; Ioannidis, J.P.A.; Boletis, J.; Bombardieri, S.; Cervera, R.; Dostal, C.; Font, J.; Gilboe, I.M.; Houssiau, F.; Huizinga, T.; et al. EULAR recommendations for the management of systemic lupus erythematosus. Report of a Task Force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics. Ann. Rheum. Dis. 2007, 67, 195–205. [Google Scholar] [CrossRef] [PubMed]
- Østensen, M.; Khamashta, M.; Lockshin, M.; Parke, A.; Brucato, A.; Carp, H.; Doria, A.; Rai, R.; Meroni, P.; Cetin, I.; et al. Anti-inflammatory and immunosuppressive drugs and reproduction. Arthritis Res. Ther. 2006, 8, 209. [Google Scholar] [CrossRef]
- Ran, Z.; Wu, K.; Matsuoka, K.; Jeen, Y.T.; Wei, S.C.; Ahuja, V.; Chen, M.; Hu, P.J.; Andoh, A.; Kim, H.J.; et al. Asian Organization for Crohn’s and Colitis and Asia Pacific Association of Gastroenterology practice recommendations for medical management and monitoring of inflammatory bowel disease in Asia. J. Gastroenterol. Hepatol. 2020, 36, 637–645. [Google Scholar] [CrossRef]
- Lichtenstein, G.R.; Loftus, E.V.; Isaacs, K.L.; Regueiro, M.D.; Gerson, L.B.; Sands, B.E. ACG Clinical Guideline: Management of Crohn’s Disease in Adults. Am. J. Gastroenterol. 2018, 113, 481–517. [Google Scholar] [CrossRef]
- Gomollón, F.; Dignass, A.; Annese, V.; Tilg, H.; Van Assche, G.; Lindsay, J.O.; Peyrin-Biroulet, L.; Cullen, G.J.; Daperno, M.; Kucharzik, T.; et al. 3rd European Evidence-based Consensus on the Diagnosis and Management of Crohn’s Disease 2016: Part 1: Diagnosis and Medical Management. J. Crohn’s Colitis 2017, 11, 3–25. [Google Scholar] [CrossRef]
- Harbord, M.; Eliakim, R.; Bettenworth, D.; Karmiris, K.; Katsanos, K.; Kopylov, U.; Kucharzik, T.; Molnár, T.; Raine, T.; Sebastian, S.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 2: Current Management. J. Crohn’s Colitis 2017, 11, 769–784. [Google Scholar] [CrossRef]
- Mack, C.L.; Adams, D.; Assis, D.N.; Kerkar, N.; Manns, M.P.; Mayo, M.J.; Vierling, J.M.; Alsawas, M.; Murad, M.H.; Czaja, A.J. Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases. Hepatology 2019, 72, 671–722. [Google Scholar] [CrossRef]
- Joly, P.; Horvath, B.; Patsatsi, A.; Uzun, S.; Bech, R.; Beissert, S.; Bergman, R.; Bernard, P.; Borradori, L.; Caproni, M.; et al. Updated S2K guidelines on the management of pemphigus vulgaris and foliaceus initiated by the european academy of dermatology and venereology (EADV). J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1900–1913. [Google Scholar] [CrossRef]
- Chouchana, L.; Narjoz, C.; Beaune, P.; Loriot, M.A.; Roblin, X. Review article: The benefits of pharmacogenetics for improving thiopurine therapy in inflammatory bowel disease. Aliment. Pharmacol. Ther. 2011, 35, 15–36. [Google Scholar] [CrossRef]
- Lennard, L. The clinical pharmacology of 6-mercaptopurine. Eur. J. Clin. Pharm. 1992, 43, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Ngo, S.; Sauvetre, G.; Vittecoq, O.; Lévesque, H.; Marie, I. Azathioprine-associated severe myelosuppression: Indication of routine determination of thiopurine S-methyltransferase variant? Rev. Med. Int. 2011, 32, 373–376. [Google Scholar] [CrossRef] [PubMed]
- Boonsrirat, U.; Angsuthum, S.; Vannaprasaht, S.; Kongpunvijit, J.; Hirankarn, N.; Tassaneeyakul, W.; Avihingsanon, Y. Azathioprine-induced fatal myelosuppression in systemic lupus erythematosus patient carrying TPMT*3C polymorphism. Lupus 2008, 17, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Bastida, G.; Nos, P.; Aguas, M.; Beltrán, B.; Rubín, A.; Dasí, F.; Ponce, J. Incidence, risk factors and clinical course of thiopurine-induced liver injury in patients with inflammatory bowel disease. Aliment. Pharm. 2005, 22, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Appell, M.L.; Berg, J.; Duley, J.; Evans, W.E.; Kennedy, M.A.; Lennard, L.; Marinaki, T.; McLeod, H.L.; Relling, M.V.; Schaeffeler, E.; et al. Nomenclature for alleles of the thiopurine methyltransferase gene. Pharm. Genom. 2013, 23, 242–248. [Google Scholar] [CrossRef]
- Engen, R.M.; Marsh, S.; Van Booven, D.J.; McLeod, H.L. Ethnic differences in pharmacogenetically relevant genes. Curr. Drug Targets 2006, 7, 1641–1648. [Google Scholar] [CrossRef]
- Corominas, H.; Domènech, M.; del Río, E.; Gich, I.; Domingo, P.; Baiget, M. Frequency of thiopurine S-methyltransferase alleles in different ethnic groups living in Spain. Med. Clin. 2006, 126, 410–412. [Google Scholar] [CrossRef]
- Dong, X.W.; Zheng, Q.; Zhu, M.M.; Tong, J.L.; Ran, Z.H. Thiopurine S-methyltransferase polymorphisms and thiopurine toxicity in treatment of inflammatory bowel disease. World J. Gastroenterol. 2010, 16, 3187–3195. [Google Scholar] [CrossRef]
- Liu, Y.-P.; Wu, H.-Y.; Yang, X.; Xu, H.-Q.; Li, Y.-C.; Shi, D.-C.; Huang, J.-F.; Huang, Q.; Fu, W.-L. Association between Thiopurine S-methyltransferase Polymorphisms and Thiopurine-Induced Adverse Drug Reactions in Patients with Inflammatory Bowel Disease: A Meta-Analysis. PLoS ONE 2015, 10, e0121745. [Google Scholar] [CrossRef]
- Liu, Y.-P.; Xu, H.-Q.; Li, M.; Yang, X.; Yu, S.; Fu, W.-L.; Huang, Q. Association between Thiopurine S-Methyltransferase Polymorphisms and Azathioprine-Induced Adverse Drug Reactions in Patients with Autoimmune Diseases: A Meta-Analysis. PLoS ONE 2015, 10, e0144234. [Google Scholar] [CrossRef] [Green Version]
- Wei, C.-Y.; Yang, J.-H.; Yeh, E.-C.; Tsai, M.-F.; Kao, H.-J.; Lo, C.-Z.; Chang, L.-P.; Lin, W.-J.; Hsieh, F.-J.; Belsare, S.; et al. Genetic profiles of 103,106 individuals in the Taiwan Biobank provide insights into the health and history of Han Chinese. NPJ Genom. Med. 2021, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Relling, M.V.; Schwab, M.; Whirl-Carrillo, M.; Suarez-Kurtz, G.; Pui, C.H.; Stein, C.M.; Moyer, A.M.; Evans, W.E.; Klein, T.E.; Antillon-Klussmann, F.G.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clin. Pharm. 2018, 105, 1095–1105. [Google Scholar] [CrossRef]
- Ansari, A.; Arenas, M.; Greenfield, S.M.; Morris, D.; Lindsay, J.; Gilshenan, K.; Smith, M.; Lewis, C.; Marinaki, A.; Duley, J.; et al. Prospective evaluation of the pharmacogenetics of azathioprine in the treatment of inflammatory bowel disease. Aliment. Pharmacol. Ther. 2008, 28, 973–983. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, O.; Latiano, A.; Bossa, F.; Vecchi, M.; D’Incà, R.; Guagnozzi, D.; Tonelli, F.; Cucchiara, S.; Valvano, M.R.; Latiano, T.; et al. Sequential evaluation of thiopurine methyltransferase, inosine triphosphate pyrophosphatase, and HPRT1 genes polymorphisms to explain thiopurines’ toxicity and efficacy. Aliment. Pharmacol. Ther. 2007, 26, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Schwab, M.; Schäffeler, E.; Marx, C.; Fischer, C.; Lang, T.; Behrens, C.; Gregor, M.; Eichelbaum, M.; Zanger, U.M.; Kaskas, B.A. Azathioprine therapy and adverse drug reactions in patients with inflammatory bowel disease: Impact of thiopurine S-methyltransferase polymorphism. Pharmacogenetics 2002, 12, 429–436. [Google Scholar] [CrossRef]
- Winter, J.W.; Gaffney, D.; Shapiro, D.; Spooner, R.J.; Marinaki, A.M.; Sanderson, J.D.; Mills, P.R. Assessment of thiopurine methyltransferase enzyme activity is superior to genotype in predicting myelosuppression following azathioprine therapy in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2007, 25, 1069–1077. [Google Scholar] [CrossRef]
- Wroblova, K.; Kolorz, M.; Batovsky, M.; Zboril, V.; Suchankova, J.; Bartos, M.; Ulicny, B.; Pav, I.; Bartosova, L. Gene Polymorphisms Involved in Manifestation of Leucopenia, Digestive Intolerance, and Pancreatitis in Azathioprine-Treated Patients. Dig. Dis. Sci. 2012, 57, 2394–2401. [Google Scholar] [CrossRef]
- Zabala-Fernández, W.; Barreiro-de Acosta, M.; Echarri, A.; Carpio, D.; Lorenzo, A.; Castro, J.; Martínez-Ares, D.; Pereira, S.; Martin-Granizo, I.; Corton, M.; et al. A pharmacogenetics study of TPMT and ITPA genes detects a relationship with side effects and clinical response in patients with inflammatory bowel disease receiving Azathioprine. J. Gastrointestin Liver Dis. 2011, 20, 247–253. [Google Scholar]
- Ezhilarasan, D. Hepatotoxic potentials of methotrexate: Understanding the possible toxicological molecular mechanisms. Toxicology 2021, 458, 152840. [Google Scholar] [CrossRef]
- Rana, P.; Aleo, M.D.; Wen, X.; Kogut, S. Hepatotoxicity reports in the FDA adverse event reporting system database: A comparison of drugs that cause injury via mitochondrial or other mechanisms. Acta. Pharm. Sin. B 2021, 11, 3857–3868. [Google Scholar] [CrossRef]
- Chen, C.H.; Huang, M.H.; Yang, J.C.; Nien, C.K.; Yang, C.C.; Yeh, Y.H.; Yueh, S.K. Prevalence and etiology of elevated serum alanine aminotransferase level in an adult population in Taiwan. J. Gastroenterol. Hepatol. 2007, 22, 1482–1489. [Google Scholar] [CrossRef] [PubMed]
- Siramolpiwat, S.; Sakonlaya, D. Clinical and histologic features of Azathioprine-induced hepatotoxicity. Scand. J. Gastroenterol. 2017, 52, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.; Jha, D.K.; Kumar, M.P.; Kasudhan, K.S.; Kumar, A.; Sarwal, D.; Mishra, S.; Singh, A.K.; Bhatia, P.; Patil, A.; et al. Prevalence of polymorphisms in thiopurine metabolism and association with adverse outcomes: A South Asian region-specific systematic review and meta-analysis. Expert Rev. Clin. Pharm. 2021, 14, 491–501. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | TPMT Non-NM (n = 50) | TPMT NM (n = 1000) | p-Value |
|---|---|---|---|
| Age | 51.5 ± 11.7 | 51.4 ± 11.6 | 0.95 |
| Gender | |||
| Female | 43 (86.0) | 858 (85.8) | 0.97 |
| Male | 7 (14.0) | 142 (14.2) | |
| AZA dose (mg) | 36.4 ± 17.9 | 39.6 ± 23.47 | 0.35 |
| Biochemistry | |||
| WBC count (U/L) | 3920 (3600–5400) | 3900 (3500–5660) | 0.73 |
| ALT (U/L) | 13.5 (11–27) | 13 (10–21) | 0.16 |
| Medication | |||
| MTX | 6 (12.0) | 125 (12.5) | 0.92 |
| Cyclophosphamide | 5 (10.0) | 137 (13.7) | 0.46 |
| Comorbidity | |||
| Hepatitis B | 6 (12.0) | 36 (3.6) | 0.01 |
| SLE | 30 (60.0) | 647 (64.7) | 0.50 |
| SS | 24 (48.0) | 456 (45.6) | 0.74 |
| DM and polymyositis | 7 (14.0) | 129 (12.9) | 0.82 |
| Pemphigus | 3 (6.0) | 25 (2.5) | 0.14 |
| Other autoimmune diseases ^ | 12 (24.0) | 244 (24.4) | 0.95 |
| Division | |||
| IMRH | 42 (84) | 864 (86.4) | 0.52 |
| NEPH | 5 (10) | 59 (5.9) | |
| NEUR | 2 (4) | 24 (2.4) | |
| DERM | 0 (0) | 27 (2.7) | |
| Others & | 1 (2) | 26 (2.6) | |
| Variable | TPMT non-NM (n = 50) | TPMT NM (n = 1000) | p-Value |
|---|---|---|---|
| AZA dose (mg) | |||
| ≤25 | 27 (54.0) | 563 (56.3) | 0.21 |
| 25–50 | 21 (42.0) | 333 (33.3) | |
| >50 | 2 (4.0) | 104 (10.4) | |
| Outcome postAZA exposure | |||
| Leukopenia ^ cases | 28 (59.5) | 611 (63.3) | 0.60 |
| Hepatitis & cases | 10 (20.0) | 150 (15.0) | 0.33 |
| Lowest WBC (U/L) | 4375 (3210–5420) | 4200 (3150–5390) | 0.52 |
| Highest ALT (U/L) | 38 (22–84) | 39 (26–73) | 0.68 |
| Onset of leukopenia ^ (days) | 1359.3 ± 1709.7 | 1597.3 ± 1606.6 | 0.44 |
| Onset of hepatitis & (days) | 676.3 ± 837.9 | 2395.8 ± 1911.0 | <0.0001 |
| Hepatotoxicity ^ | p-Value | ||
|---|---|---|---|
| HR | 95% CI | ||
| Age | 0.99 | 0.98–1.01 | 0.60 |
| Gender (reference female) | 1.77 | 1.07–2.91 | 0.03 |
| TPMT non-NM genotype | 3.85 | 1.83–8.10 | 0.0004 |
| AZA dose (mg) | 1.00 | 1.00–1.01 | 0.31 |
| MTX | 1.62 | 1.03–2.57 | 0.04 |
| Hepatitis B carrier | 1.18 | 0.40–3.48 | 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheu, H.-S.; Chen, Y.-M.; Liao, Y.-J.; Wei, C.-Y.; Chen, J.-P.; Lin, H.-J.; Hung, W.-T.; Huang, W.-N.; Chen, Y.-H. Thiopurine S-Methyltransferase Polymorphisms Predict Hepatotoxicity in Azathioprine-Treated Patients with Autoimmune Diseases. J. Pers. Med. 2022, 12, 1399. https://doi.org/10.3390/jpm12091399
Sheu H-S, Chen Y-M, Liao Y-J, Wei C-Y, Chen J-P, Lin H-J, Hung W-T, Huang W-N, Chen Y-H. Thiopurine S-Methyltransferase Polymorphisms Predict Hepatotoxicity in Azathioprine-Treated Patients with Autoimmune Diseases. Journal of Personalized Medicine. 2022; 12(9):1399. https://doi.org/10.3390/jpm12091399
Chicago/Turabian StyleSheu, Heh-Shiang, Yi-Ming Chen, Yi-Ju Liao, Chia-Yi Wei, Jun-Peng Chen, Hsueh-Ju Lin, Wei-Ting Hung, Wen-Nan Huang, and Yi-Hsing Chen. 2022. "Thiopurine S-Methyltransferase Polymorphisms Predict Hepatotoxicity in Azathioprine-Treated Patients with Autoimmune Diseases" Journal of Personalized Medicine 12, no. 9: 1399. https://doi.org/10.3390/jpm12091399