
A Randomized Controlled Trial of Three Advanced Wound Dressings in Split-Thickness Skin Grafting Donor Sites—A Personalized Approach?
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
2.3. Wound Dressing Material
2.4. Treatment Allocation and Schedule
2.5. Treatment Regime of Wound Dressings
- (1)
- Primary wound dressing: Biatain® Ibu (Coloplast A/S, Humlebæk, Denmark), Mepilex® Ag (Mölnlycke, Göteborg, Sweden), epicite + hydro (QRSKIN GmbH, Würzburg, Germany)
- (2)
- Secondary wound dressing (only for epicite + hydro): fatty gauze;
- (3)
- Secondary wound dressing: sterile dry gauze;
- (4)
- Secondary wound dressing: adhesive bandage.
2.6. Study Assessments and Endpoints
2.7. Statistical Analysis
3. Results
3.1. Wound Healing
3.2. Pain
3.3. Handling of Dressings
3.3.1. Subjective Dressing Handling Evaluation by Patient
3.3.2. Subjective Dressing Handling Evaluation by Healthcare Personnel
3.4. Scar Evaluation
3.4.1. PSAS by Patient
3.4.2. VSS by Observer
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brown, J.E.; Holloway, S.L. An Evidence-Based Review of Split-Thickness Skin Graft Donor Site Dressings. Int. Wound J. 2018, 15, 1000–1009. [Google Scholar] [CrossRef]
- Broussard, K.C.; Powers, J.G. Wound Dressings: Selecting the Most Appropriate Type. Am. J. Clin. Dermatol. 2013, 14, 449–459. [Google Scholar] [CrossRef] [PubMed]
- McBride, C.A.; Kimble, R.M.; Stockton, K.A. Prospective Randomised Controlled Trial of AlgisiteTM M, CuticerinTM, and Sorbact® as Donor Site Dressings in Paediatric Split-Thickness Skin Grafts. Burn. Trauma 2018, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Langridge, B.; Al-Hadad, A.; Khan, R.A.; Junejo, M.H.; Mosahebi, A. Biological versus Non-Biological Dressings in the Management of Split-Thickness Skin-Graft Donor Sites: A Systematic Review and Meta-Analysis. J. Wound Care 2020, 29, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Carta, T.; Gawaziuk, J.P.; Diaz-Abele, J.; Liu, S.; Jeschke, M.; Logsetty, S. Properties of an Ideal Burn Dressing: A Survey of Burn Survivors and Front-Line Burn Healthcare Providers. Burns 2019, 45, 364–368. [Google Scholar] [CrossRef] [PubMed]
- Kamolz, L.P.; Giretzlehner, M.; Trop, M.; Parvizi, D.; Spendel, S.; Schintler, M.; Justich, I.; Wiedner, M.; Laback, C.; Lumenta, D.B. The Properties of the “Ideal” Donor Site Dressing: Results of a Worldwide Online Survey. Ann. Burns Fire Disasters 2013, 26, 136–141. [Google Scholar]
- Karlsson, M.; Elmasry, M.; Steinvall, I.; Sjöberg, F.; Olofsson, P. Scarring at Donor Sites after Split-Thickness Skin Graft: A Prospective, Longitudinal, Randomized Trial. Adv. Skin Wound Care 2020, 33, 1–5. [Google Scholar] [CrossRef]
- Chiang, S.-H.; Xu, X.; Cheung, D.S.T.; Hsu, Y.-H.; Chen, C.-E.; Lin, C.-H.; Smith, R.; Lin, C.-C. Comparison between Aquacel and Aquacel Foam Dressing on Split-Thickness Skin Graft Donor Site. J. Wound Care 2021, 30, S14–S20. [Google Scholar] [CrossRef]
- Pak, C.S.; Park, D.H.; Oh, T.S.; Lee, W.J.; Jun, Y.J.; Lee, K.A.; Oh, K.S.; Kwak, K.H.; Rhie, J.W. Comparison of the Efficacy and Safety of Povidone-iodine Foam Dressing (Betafoam), Hydrocellular Foam Dressing (Allevyn), and Petrolatum Gauze for Split-thickness Skin Graft Donor Site Dressing. Int. Wound J. 2019, 16, 379–386. [Google Scholar] [CrossRef]
- Haik, J.; Ullman, Y.; Gur, E.; Ad-El, D.; Egozi, D.; Kruchevsky, D.; Zissman, S.; Biros, E.; Nir, R.-R.; Kornhaber, R.; et al. Advances in the Use of Electrospun Nanofibrous Polymeric Matrix for Dermal Healing at the Donor Site After the Split-Thickness Skin Graft Excision: A Prospective, Randomized, Controlled, Open-Label, Multicenter Study. J. Burn Care Res. 2022, 43, 889–898. [Google Scholar] [CrossRef]
- Davies, P.; McCarty, S.; Hamberg, K. Silver-Containing Foam Dressings with Safetac: A Review of the Scientific and Clinical Data. J. Wound Care 2017, 26, S1–S32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markl, P.; Prantl, L.; Schreml, S.; Babilas, P.; Landthaler, M.; Schwarze, H. Management of Split-Thickness Donor Sites with Synthetic Wound Dressings: Results of a Comparative Clinical Study. Ann. Plast. Surg. 2010, 65, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Serebrakian, A.T.; Pickrell, B.B.; Varon, D.E.; Mohamadi, A.; Grinstaff, M.W.; Rodriguez, E.K.; Nazarian, A.; Halvorson, E.G.; Sinha, I. Meta-Analysis and Systematic Review of Skin Graft Donor-Site Dressings with Future Guidelines. Plast. Reconstr. Surg.—Glob. Open 2018, 6, e1928. [Google Scholar] [CrossRef]
- Schiefer, J.L.; Aretz, G.F.; Fuchs, P.C.; Bagheri, M.; Funk, M.; Schulz, A.; Daniels, M. Comparison of Wound Healing and Patient Comfort in Partial-thickness Burn Wounds Treated with SUPRATHEL and Epicte Hydro Wound Dressings. Int. Wound J. 2021, 19, 782–790. [Google Scholar] [CrossRef] [PubMed]
- Bacakova, L.; Pajorova, J.; Bacakova, M.; Skogberg, A.; Kallio, P.; Kolarova, K.; Svorcik, V. Versatile Application of Nanocellulose: From Industry to Skin Tissue Engineering and Wound Healing. Nanomaterials 2019, 9, 164. [Google Scholar] [CrossRef] [PubMed]
- de Mattos, I.B.; Holzer, J.C.J.; Tuca, A.-C.; Groeber-Becker, F.; Funk, M.; Popp, D.; Mautner, S.; Birngruber, T.; Kamolz, L.-P. Uptake of PHMB in a Bacterial Nanocellulose-Based Wound Dressing: A Feasible Clinical Procedure. Burns 2019, 45, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Bernardelli de Mattos, I.; Nischwitz, S.P.; Tuca, A.-C.; Groeber-Becker, F.; Funk, M.; Birngruber, T.; Mautner, S.I.; Kamolz, L.-P.; Holzer, J.C.J. Delivery of Antiseptic Solutions by a Bacterial Cellulose Wound Dressing: Uptake, Release and Antibacterial Efficacy of Octenidine and Povidone-Iodine. Burns 2020, 46, 918–927. [Google Scholar] [CrossRef]
- Nischwitz, S.P.; Bernardelli de Mattos, I.; Hofmann, E.; Groeber-Becker, F.; Funk, M.; Mohr, G.J.; Branski, L.K.; Mautner, S.I.; Kamolz, L.P. Continuous PH Monitoring in Wounds Using a Composite Indicator Dressing—A Feasibility Study. Burns 2019, 45, 1336–1341. [Google Scholar] [CrossRef]
- Wiegand, C.; Moritz, S.; Hessler, N.; Kralisch, D.; Wesarg, F.; Müller, F.A.; Fischer, D.; Hipler, U.-C. Antimicrobial Functionalization of Bacterial Nanocellulose by Loading with Polihexanide and Povidone-Iodine. J. Mater. Sci. Mater. Med. 2015, 26, 245. [Google Scholar] [CrossRef]
- Aljghami, M.E.; Saboor, S.; Amini-Nik, S. Emerging Innovative Wound Dressings. Ann. Biomed. Eng. 2019, 47, 659–675. [Google Scholar] [CrossRef]
- Gottrup, F.; Jørgensen, B.; Karlsmark, T.; Sibbald, R.G.; Rimdeika, R.; Harding, K.; Price, P.; Venning, V.; Vowden, P.; Jünger, M.; et al. Reducing Wound Pain in Venous Leg Ulcers with Biatain Ibu: A Randomized, Controlled Double-Blind Clinical Investigation on the Performance and Safety. Wound Repair Regen. 2008, 16, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Romanelli, M.; Dini, V.; Polignano, R.; Bonadeo, P.; Maggio, G. Ibuprofen Slow-Release Foam Dressing Reduces Wound Pain in Painful Exuding Wounds: Preliminary Findings from an International Real-Life Study. J. Dermatolog. Treat. 2009, 20, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Baryza, M.J.; Baryza, G.A. The Vancouver Scar Scale: An Administration Tool and Its Interrater Reliability. J. Burn Care Rehabil. 1995, 16, 535–538. [Google Scholar] [CrossRef]
- Draaijers, L.J.; Tempelman, F.R.H.; Botman, Y.A.M.; Tuinebreijer, W.E.; Middelkoop, E.; Kreis, R.W.; van Zuijlen, P.P.M. The Patient and Observer Scar Assessment Scale: A Reliable and Feasible Tool for Scar Evaluation. Plast. Reconstr. Surg. 2004, 113, 1960–1965. [Google Scholar] [CrossRef]
- Hollander, J.E.; Singer, A.J.; Valentine, S.; Henry, M.C. Wound Registry: Development and Validation. Ann. Emerg. Med. 1995, 25, 675–684. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Venables, W.N.; Ripley, B.D. Modern Applied Statistics with S; Statistics and Computing; Springer: New York, NY, USA, 2002; ISBN 978-1-4419-3008-8. [Google Scholar]
- Rennekampff, H.-O.; Rabbels, J.; Reinhard, V.; Becker, S.T.; Schaller, H.-E. Comparing the Vancouver Scar Scale With the Cutometer in the Assessment of Donor Site Wounds Treated With Various Dressings in a Randomized Trial. J. Burn Care Res. 2006, 27, 345–351. [Google Scholar] [CrossRef]
- Vaheb, M.; Karrabi, M.; Khajeh, M.; Asadi, A.; Shahrestanaki, E.; Sahebkar, M. Evaluation of the Effect of Platelet-Rich Fibrin on Wound Healing at Split-Thickness Skin Graft Donor Sites: A Randomized, Placebo-Controlled, Triple-Blind Study. Int. J. Low. Extrem. Wounds 2021, 20, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Mantha, S.; Thisted, R.; Foss, J.; Ellis, J.E.; Roizen, M.F. A Proposal to Use Confidence Intervals for Visual Analog Scale Data for Pain Measurement to Determine Clinical Significance. Anesth. Analg. 1993, 77, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Brown, N.J.; Kimble, R.M.; Rodger, S.; Ware, R.S.; Cuttle, L. Play and Heal: Randomized Controlled Trial of DittoTM Intervention Efficacy on Improving Re-Epithelialization in Pediatric Burns. Burns 2014, 40, 204–213. [Google Scholar] [CrossRef]
- Walburn, J.; Vedhara, K.; Hankins, M.; Rixon, L.; Weinman, J. Psychological Stress and Wound Healing in Humans: A Systematic Review and Meta-Analysis. J. Psychosom. Res. 2009, 67, 253–271. [Google Scholar] [CrossRef]
- Gee Kee, E.L.; Kimble, R.M.; Cuttle, L.; Khan, A.; Stockton, K.A. Randomized Controlled Trial of Three Burns Dressings for Partial Thickness Burns in Children. Burns 2015, 41, 946–955. [Google Scholar] [CrossRef] [PubMed]
- Sterling, J.P. Silver-Resistance, Allergy, and Blue Skin: Truth or Urban Legend? Burns 2014, 40, S19–S23. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-Q.; Chang, H.-E.; Francis, R.; Olszowy, H.; Liu, P.-Y.; Kempf, M.; Cuttle, L.; Kravchuk, O.; Phillips, G.E.; Kimble, R.M. Silver Deposits in Cutaneous Burn Scar Tissue Is a Common Phenomenon Following Application of a Silver Dressing. J. Cutan. Pathol. 2009, 36, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; Dalziel, S.R.; Herd, E.; Johnson, K.; Wong She, R.; Shepherd, M. A Randomized Controlled Study of Silver-Based Burns Dressing in a Pediatric Emergency Department. J. Burn Care Res. 2016, 37, e340–e347. [Google Scholar] [CrossRef]
- Tang, H.; Lv, G.; Fu, J.; Niu, X.; Li, Y.; Zhang, M.; Zhang, G.; Hu, D.; Chen, X.; Lei, J.; et al. An Open, Parallel, Randomized, Comparative, Multicenter Investigation Evaluating the Efficacy and Tolerability of Mepilex Ag versus Silver Sulfadiazine in the Treatment of Deep Partial-Thickness Burn Injuries. J. Trauma Acute Care Surg. 2015, 78, 1000–1007. [Google Scholar] [CrossRef]
- Khansa, I.; Schoenbrunner, A.R.; Kraft, C.T.; Janis, J.E. Silver in Wound Care—Friend or Foe? Plast. Reconstr. Surg.—Glob. Open 2019, 7, e2390. [Google Scholar] [CrossRef]
- Dumville, J.C.; Gray, T.A.; Walter, C.J.; Sharp, C.A.; Page, T. Dressings for the Prevention of Surgical Site Infection. In Cochrane Database of Systematic Reviews; Dumville, J.C., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2014. [Google Scholar]
- Ono, S.; Imai, R.; Ida, Y.; Shibata, D.; Komiya, T.; Matsumura, H. Increased Wound PH as an Indicator of Local Wound Infection in Second Degree Burns. Burns 2015, 41, 820–824. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total N = 69 | Biatain® Ibu (N = 23) | Mepilex® Ag (N = 22) | Epicite + Hydro (N = 24) |
|---|---|---|---|
| Age (years), mean (SD) | 48 ( ± 18) | 54 (±20) | 47 (±17) |
| Gender, n (%) | |||
| Male | 17 (73.9) | 10 (45.5) | 18 (75.0) |
| Female | 6 (26.1) | 12 (54.5) | 6 (25.0) |
| BMI (kg/m2), median (IR) | 26.0 (7.6) | 25.4 (5.7) | 27.1 (6.0) |
| Length of stay (days intervention—discharge), median (range) | 8 (0–22) | 8 (2–28) | 9 (4–23) |
| Smoking, n | 9 | 11 | 8 |
| ASA risk classification | |||
| ASA 1, n | 5 | 8 | 11 |
| ASA 2, n | 14 | 4 | 9 |
| ASA 3, n | 4 | 10 | 4 |
| ASA 4, n | 0 | 0 | 0 |
| Wound size (mm2), median (IR) | 6800 (8400) | 6800 (12,675) | 10,650 (22,525) |
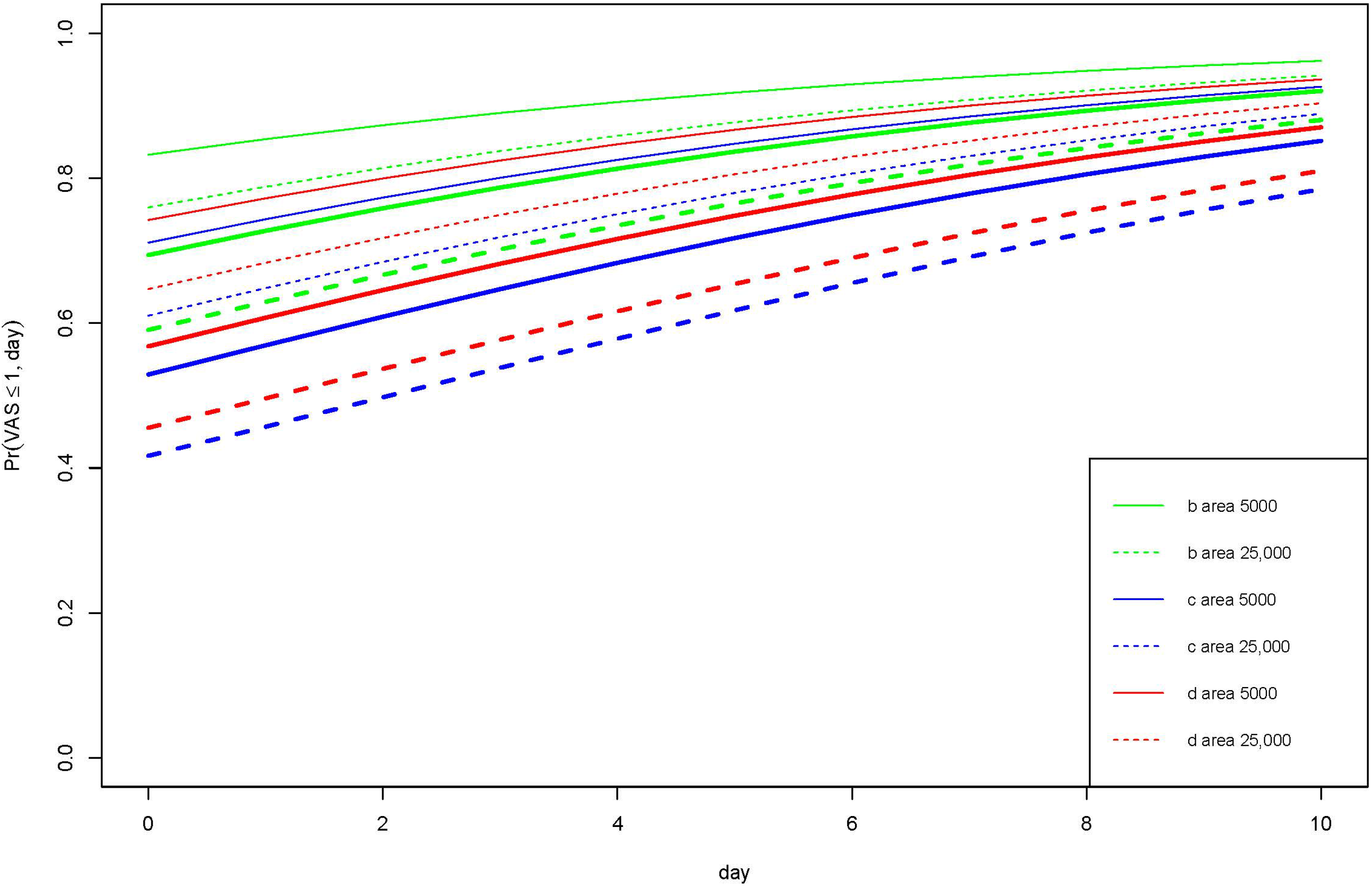
| Probability for ExperiencingVAS Score ≤ 1 | Ibuprofen-Containing Foam | Silver-Impregnated Foam | Nanocellulose | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Day 0 | Day 2 | Day 4 | Day 0 | Day 2 | Day 4 | Day 0 | Day 2 | Day 4 | |
| Wound area 5000 mm2 | |||||||||
| In rest, (%) | 83 | 87 | 91 | 71 | 77 | 83 | 74 | 80 | 85 |
| In motion, (%) | 69 | 76 | 81 | 53 | 61 | 68 | 57 | 65 | 72 |
| Wound area 25,000 mm2 | |||||||||
| In rest, (%) | 76 | 81 | 86 | 61 | 68 | 75 | 65 | 72 | 78 |
| In motion, (%) | 59 | 67 | 73 | 42 | 50 | 58 | 46 | 54 | 62 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hecker, A.; Lumenta, D.B.; Brinskelle, P.; Sawetz, I.; Steiner, A.; Michelitsch, B.; Friedl, H.; Gmainer, D.; Kamolz, L.-P.; Winter, R. A Randomized Controlled Trial of Three Advanced Wound Dressings in Split-Thickness Skin Grafting Donor Sites—A Personalized Approach? J. Pers. Med. 2022, 12, 1395. https://doi.org/10.3390/jpm12091395
Hecker A, Lumenta DB, Brinskelle P, Sawetz I, Steiner A, Michelitsch B, Friedl H, Gmainer D, Kamolz L-P, Winter R. A Randomized Controlled Trial of Three Advanced Wound Dressings in Split-Thickness Skin Grafting Donor Sites—A Personalized Approach? Journal of Personalized Medicine. 2022; 12(9):1395. https://doi.org/10.3390/jpm12091395
Chicago/Turabian StyleHecker, Andrzej, David Benjamin Lumenta, Petra Brinskelle, Isabelle Sawetz, Andreas Steiner, Birgit Michelitsch, Herwig Friedl, Daniel Gmainer, Lars-Peter Kamolz, and Raimund Winter. 2022. "A Randomized Controlled Trial of Three Advanced Wound Dressings in Split-Thickness Skin Grafting Donor Sites—A Personalized Approach?" Journal of Personalized Medicine 12, no. 9: 1395. https://doi.org/10.3390/jpm12091395