
Reinforcing Health Data Sharing through Data Democratization


Abstract
:1. Introduction
- All stakeholders are treated identically without discrimination. The platform and any constructed protocol would not take into account any player’s distinguishing attributes (e.g., size, market volume, profitability, proprietary technology and knowledge, dominance in administrative power or market influence, information sources, etc.) and therefore each player can be treated equally in our platform;
- The promotion of fairness as a complementary. Based on the first fundamental, this is also essential when facing the inequivalence reality among each party, especially quite often seen between the individual data subject (DS) and the so-called “digital oligarchs”.
2. Related Works
3. Classification of Stakeholders and Matching with Roles Defined in GDPR
3.1. Stakeholders Classification
- Computing resource manager (CRM)
- Data consumer (DC)
- Data generator (DG)
- Data manager (DM)
- Dataset provider (DSP)
- Data rights manager (DRM)
- Data analysis service provider (DASP)
3.2. Relation with Roles Defined in GDPRSubsection
- Example: A general practitioner (GP) can provide a value-added service for his/her patients who have their own Personal Health Record (PHR) system which is technically provided and maintained by a PHR service provider who builds their service on infrastructure provided by the public cloud from Amazon. The GP can specify what data are needed for a health monitoring process for purpose of a specific longitudinal study to personalize the care plan for a specific patient. The GP sets up the longitudinal study plan, collects data from a PHR which has the data sourced from different independent wearable sensor data vault used by the patient, outsources part of the collected data to a data analytics service provider for data analysis purpose, accumulate the data, and finally design a new care plan for the patient. To provide legitimate, auditable, and efficient service information and contract management, the GP uses a contract management App to communicate with the patient for negotiating the rights, obligations, prices, and other issues concerning the offering of the service.
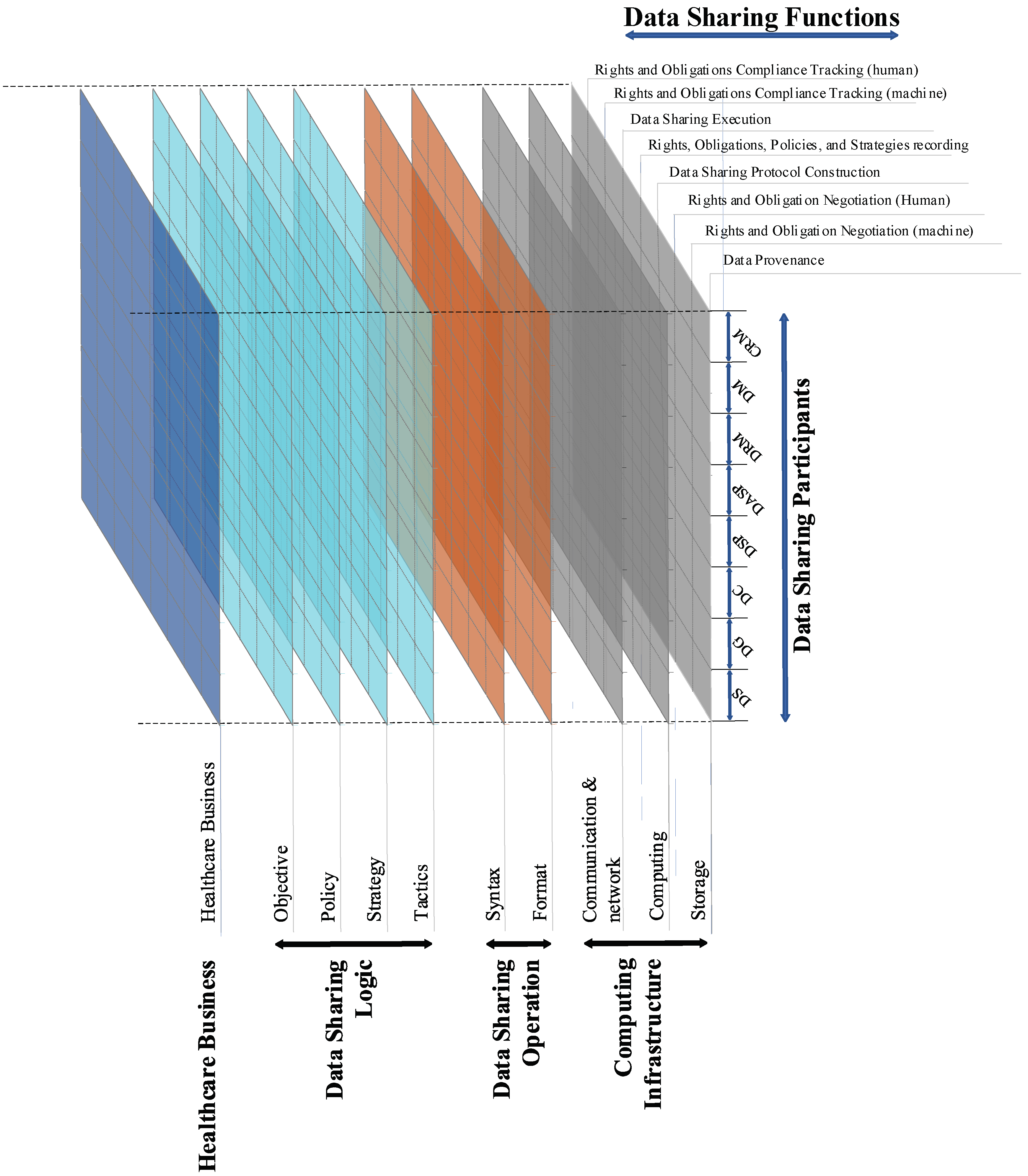
4. Conceptual Layered Architecture of HD Platform
- Data provenance: providing backward traceability of medical devices, the personal device in the homecare environment, etc., and the health data sourced from these devices to be audited in a trusted way regarding rights and operation status;
- Risk Assessment: enabling each data subject to have different risk acceptance tolerance and incentive degrees when they are entitled to rights and benefits from data;
- Computational negotiation: negotiating agents can operate and negotiate decisions. The requirements will be developed in compliance with the GDPR, healthcare regulations, and other relevant policies. When processing and exchanging personal data between the agents, the design of the infrastructure will address such key requirements of the GDPR as data protection by design and by default, accountability, pseudonymization, right of access, and right to be informed, to rectify, to erasure, and to be forgotten;
- Multi-lateral security policing: enabling individuals to be able to share and control access to health data without having to place extensive trust in entities, and institutions must also be able to share data responsibly for research, innovation, and quality assurance across institutional boundaries.
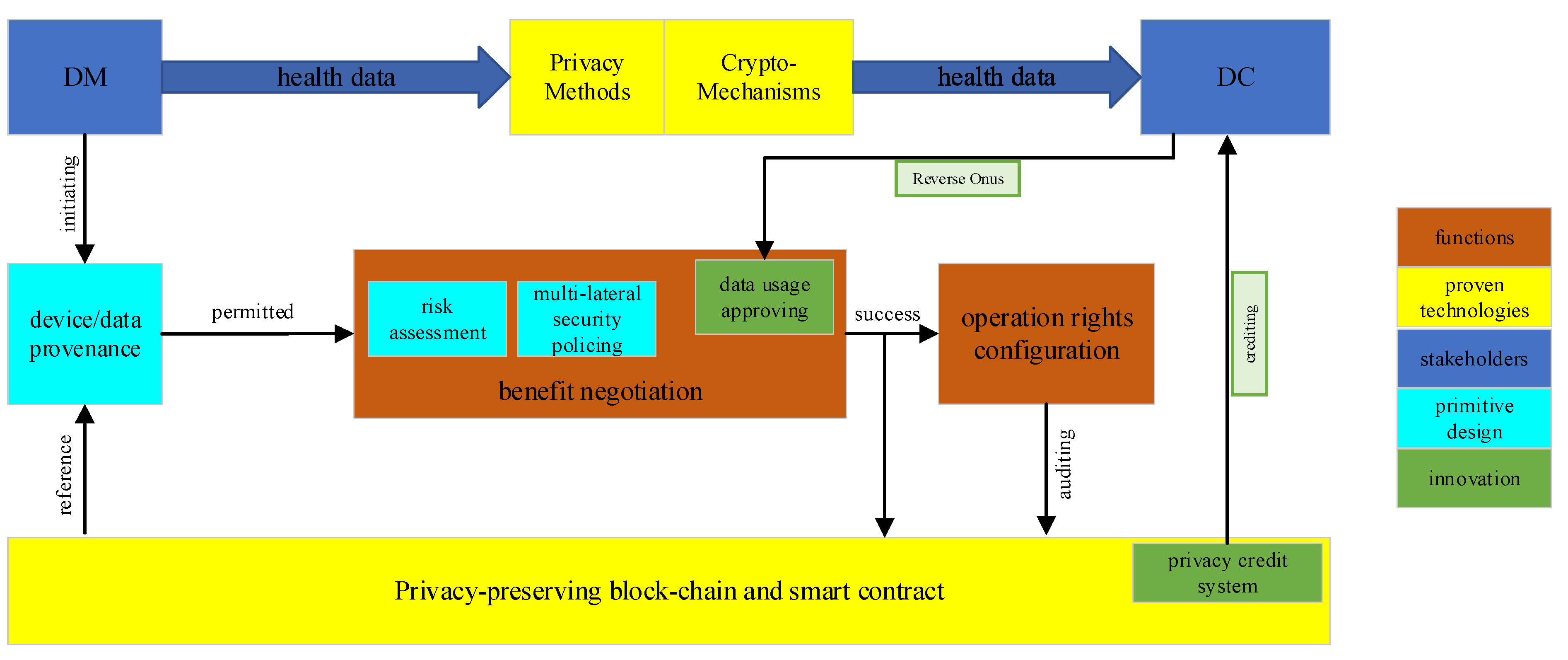
- A data provenance process that clarifies among the concerned players the history of the parties with their rights regarding the data to be shared;
- If a default (pre-defined) right and obligation setting is not unanimously agreed upon by the involved players, a knowledge-driven negotiation process must be performed where each player takes into account different factors such as ethical and legal contexts, risk assessment of data breach/privacy breach, benefit from data sharing, etc., based on risk models, and AI-based inference. As business systems are frequently highly dynamic regarding their objectives, context, processes, etc., a dynamic policy management and mapping in consistency with legal and ethical requirements and principles is inevitable;
- The computational negotiation mechanism takes as inputs the risk assessment result from individual players as well as the multi-party security policy logical representation and reconciliation solution, and generates a new recommendation to all the involved parties for achieving an agreement. This process could iterate in several rounds;
- The outcome of the computational negotiation determines the data sharing protocol and the security and privacy-enhancing technical methods for data sharing (e.g., homomorphic encryption, secure multi-party computation, differential privacy methods, federated machine learning, etc.);
- The new configuration of rights of the involved players is recorded using blockchain technology, and the execution of data sharing is encoded into a smart contract which could trigger the automated data sharing now or in the future.
5. Democratization-Promoting Primitive Design
5.1. Token-Economy-Powered Incentive Mechanism for Promoting Reverse Onus
5.2. Data Usage Approval
- Usage purpose;
- Data precision upper limit in percentage;
- Data requesting schedule instant/time period/data manager triggered/etc;
- Requiring a pattern in the frequency distribution;
- Purposes to precision. The required data precision should be in accordance with the purposes of the data usage;
- Purposes to schedule. To assess whether the data accesses conform to the purposes.
- Purposes to the pattern. To assess whether the data requesting is coherent with the purposes;
- History comparison across entities.
5.3. Token Economy Rules
5.4. Behavior Analysis
- Excessive data transmission, the balance cannot be enough for him to afford the rest of the data, and hence go against his plan of appFm;
- Hoarding the healthcoin (e.g., by utilizing Rule 5 to save healthcoin on purpose) to perform potential privacy data transmission. However, when the balance becomes high, the gain from the new appFm will decrease, and the balance will be exhausted soon since the payments it gets barely cover his expenses.
5.5. Incentive Mechanism
- The credit parameter
- 2.
- Gain/loss ratio θ
- 3.
- Discount ratio δ
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sharing Clinical Research Data: Workshop Summary; The National Academies Press: Washington, DC, USA, 2013.
- Walport, M.; Brest, P. Sharing research data to improve public health. Lancet 2011, 377, 537–539. [Google Scholar] [CrossRef]
- Blobel, B.; Lopez, D.M.; Gonzalez, C. Patient privacy and 12 security concerns on big data for personalized medicine. Health Technol. 2016, 6, 75–81. [Google Scholar] [CrossRef]
- Blobel, B.; Oemig, F.; Ruotsalainen, P.; Lopez, D.M. Transformation of Health and Social Care Systems—An Interdisciplinary Approach Toward a Foundational Architecture. Front. Med. 2022, 9, 802487. [Google Scholar] [CrossRef] [PubMed]
- Scientific American. Available online: https://www.scientificamerican.com/article/how-data-brokers-make-money-off-your-medical-records/ (accessed on 5 August 2022).
- Czeschik, C. Black Market Value of Patient Data. In Digital Marketplaces Unleashed; Springer: Berlin/Heidelberg, Germany, 2018; pp. 883–893. [Google Scholar]
- Ruotsalainen, P.S.; Blobel, B.; Seppälä, A.; Nykänen, P. Trust Information-Based Privacy Architecture for Ubiquitous Health. JMIR mHealth uHealth 2013, 1, e23. [Google Scholar] [CrossRef] [PubMed]
- Blobel, B.; Nordberg, R.; Davis, J.M.; Pharow, P. Modelling privilege management and access control. Int. J. Med. Inform. 2006, 75, 597–623. [Google Scholar] [CrossRef] [PubMed]
- Mallik, P. Data Democratization. Towards Data Science. 18 July 2019. Available online: https://towardsdatascience.com (accessed on 5 August 2022).
- Marr, B. What Is Data Democratization? A Super Simple Explanation and The Key Pros and Cons. 24 July 2017. Available online: https://www.forbes.com (accessed on 5 August 2022).
- Ruotsalainen, P.; Blobel, B. How a service user knows the level of privacy and to whom trust in pHealth systems? Stud. Health Technol. Inform. 2021, 285, 39–48. [Google Scholar] [PubMed]
- ISO 23903:2021; Health Informatics—Interoperability and Integration Reference Architecture—Model and Framework. International Organisation for Standardisation (ISO): Geneva, Switzerland, 2021.
- ISO 22600:2014; Health Informatics—Privilege Management and Access Control. International Organisation for Standardisation (ISO): Geneva, Switzerland, 2014.
- ISO 21298:2017; Health Informatics—Funtional and Structural Roles. International Organisation for Standardisation (ISO): Geneva, Switzerland, 2017.
- HL7 International. HL7 Privacy and Security Logical Data Model, Release 1, June 2021; HL7 International: Ann Arbor, MI, USA, 2021. [Google Scholar]
- Hartvigsen, G.; Pedersen, S. Lessons Learned from 25 Years with Telemedicine in Northern Norway; NST-Rapportserie: Tromso, Norway, 2015; pp. 6–16. [Google Scholar]
- Helseanalyseplattformen. Available online: https://ehelse.no/helsedataprogrammet/helseanalyseplattformen (accessed on 5 August 2022).
- Blobel, B.; Davis, M.; Ruotsalainen, P. Policy Management Standards Enabling Trustworthy pHealth. Stud. Health Technol. Inform. 2014, 200, 8–21. [Google Scholar] [PubMed]
- Ruotsalainen, P.; Blobel, B. Trust Information and Privacy Policies—Enablers for pHealth and Ubiquitous Health. Stud. Health Technol. Inform. 2014, 200, 133–139. [Google Scholar] [PubMed]
- Ruotsalainen, P.; Blobel, B. Trust Model for Protection of Personal Health Data in a Global Environment. Stud. Health Technol. Inform. 2017, 245, 202–206. [Google Scholar] [PubMed]
- Directive 2011/24/EU on Patients’ Rights in Cross-Border Healthcare. Available online: https://ec.europa.eu/health/cross_border_care/policy_en (accessed on 5 August 2022).
- European eHealth. Available online: https://ec.europa.eu/health/sites/health/files/ehealth/docs/ev_20161121_co01_en.pdf (accessed on 5 August 2022).
- Facebook Life Trajectory. Available online: https://www.technologyreview.com/s/514186/lifes-trajectory-seen-through-facebook-data/ (accessed on 5 August 2022).
- Google Clinical Care. Available online: https://theconversation.com/google-is-now-involved-with-healthcare-data-is-that-a-good-thing-58901 (accessed on 5 August 2022).
- Blobel, B.; Ruotsalainen, P. How Does GDPR Support Healthcare Transformation to 5P Medicine? Stud. Health Technol. Inform. 2019, 264, 1135–1339. [Google Scholar] [PubMed]
- Blobel, B.; Ruotsalainen, P. Healthcare Transformation Towards Personalized Medicine—Chances and Challenges. Stud. Health Technol. Inform. 2019, 261, 3–21. [Google Scholar] [PubMed]
- Ruotsalainen, P.; Blobel, B. Digital pHealth—Problems and Solutions for Ethics, Trust and Privacy. Stud. Health Technol. Inform. 2019, 261, 31–46. [Google Scholar] [PubMed]
- The Patient Information Sharing Platform. Available online: https://www.patientslikeme.com/ (accessed on 5 August 2022).
- Helse Sør-Øst Outsourcing Health IT. Available online: https://www.nrk.no/norge/helse-sor-ost_-outsourcing-stoppes-1.13578806 (accessed on 5 August 2022).
- NRK Nordland. Available online: https://www.nrk.no/nordland/irenes-private-helseopplysninger-la-apent-ute-pa-nett_-_-sjokkerende-og-ekkelt-1.13693173 (accessed on 5 August 2022).
- Madge, R. Five Loopholes in the GDPR. Available online: https://medium.com/mydata/five-loopholes-in-the-gdpr-367443c4248b (accessed on 5 August 2022).
- Dette Kan Ramme Viljen Til å Delta i Forskning. Available online: https://forskning.no/2018/04/dette-kan-ramme-viljen-til-delta-i-forskning/produsert-og-finansiert-av/de-nasjonale-forskningsetiske-komiteene (accessed on 5 August 2022).
- Millions of NHS Records Sold to Insurance Firms. Available online: http://www.telegraph.co.uk/news/health/news/10906390/Millions-of-NHS-records-sold-to-insurance-firms.html (accessed on 5 August 2022).
- Patients Will Resist Medical Record Sharing if NHS Bosses Ignore Their Privacy Fears. Available online: https://theconversation.com/patients-will-resist-medical-record-sharing-if-nhs-bosses-ignore-their-privacy-fears-46147 (accessed on 5 August 2022).
- Informasjonssikkerhet er Mer enn Bare Personvern. Hurlen og Gulbrandsen. Available online: https://www.aftenposten.no/meninger/kronikk/i/WV2Vg/Hvor-trygg-kan-pasientjournalen-egentlig-vare-Informasjonssikkerhet-er-mer-enn-bare-personvern--Hurlen-og-Gulbrandsen (accessed on 5 August 2022).
- Ruotsalainen, P.; Blobel, B. Transformed Health Ecosystems—Challenges for Security, Privacy, and Trust. Front. Med. 2022, 9, 827253. [Google Scholar] [CrossRef] [PubMed]
- Nasjonal e-Helsestrategi og Mål 2017–2022. Available online: https://ehelse.no/publikasjoner/nasjonal-e-helsestrategi-og-mal-2017-2022-oppdatert-2019 (accessed on 5 August 2022).
- ANTILOPE Refinement Definition Document. Available online: https://www.antilope-project.eu/wp-content/uploads/2013/05/D1.1-Refinement_of_Antilope_Use_Cases_v1.2.pdf (accessed on 5 August 2022).
- Europe eHealth ev. Available online: https://ec.europa.eu/health/sites/default/files/ehealth/docs/ev_20151123_co03_en.pdf (accessed on 5 August 2022).
- Cole, A.M.; Stephens, K.A.; Keppel, G.A.; Lin, C.-P.; Baldwin, L.-M. Implementation of a health data-sharing infrastructure across diverse primary care organizations. J. Ambul. Care Manag. 2014, 37, 164–170. [Google Scholar] [CrossRef]
- Explaining the Technical Architecture of Health Information Exchange. Available online: https://www.colleaga.org/sites/default/files/attachments/ExplainingTheTechnicalArchitectureOfHIE.pdf (accessed on 5 August 2022).
- Meng, S.; Zhu, L.; Xu, K. Layered Data Sharing Architecture with Blockchain. In Blockchain: Empowering Secure Data Sharing; Springer: Singapore, 2020; pp. 29–37. [Google Scholar]
- Ruotsalainen, P.; Blobel, B. A Model for Calculated Privacy and Trust in pHealth Ecosystems. Stud. Health Technol. Inform. 2018, 249, 29–37. [Google Scholar]
- Ruotsalainen, P.; Blobel, B. Privacy Is Dead—Solutions for Privacy-Enabled Collections and Use of Personal Health Information in Digital Era. Stud. Health Technol. Inform. 2020, 273, 63–74. [Google Scholar] [PubMed]
- Wang, Y.; Tian, Z.; Sun, Y.; Du, X.; Guizani, N. LocJury: An IBN-based location privacy preserving scheme for IoCV. IEEE Trans. Intell. Transp. Syst. 2020, 22, 5028–5037. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Party | Participant Defined in HD | Role Defined in GDPR |
|---|---|---|
| Patient | data subject | data subject |
| GP | data consumer | joint data controller |
| PHR portal managed by the patient | data manager | data processor |
| PHR service provider | dataset provider | joint data controller, data processor |
| Amazon cloud | computing resource manager | data processor |
| Sensor service provider | data generator | data processor |
| Data analytics service provider | data analytics service provider | data processor |
| Contract management App | data rights manager | data processor |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.; Blobel, B.; Yang, B. Reinforcing Health Data Sharing through Data Democratization. J. Pers. Med. 2022, 12, 1380. https://doi.org/10.3390/jpm12091380
Wang Y, Blobel B, Yang B. Reinforcing Health Data Sharing through Data Democratization. Journal of Personalized Medicine. 2022; 12(9):1380. https://doi.org/10.3390/jpm12091380
Chicago/Turabian StyleWang, Yuhang, Bernd Blobel, and Bian Yang. 2022. "Reinforcing Health Data Sharing through Data Democratization" Journal of Personalized Medicine 12, no. 9: 1380. https://doi.org/10.3390/jpm12091380