
MiR-146a Contributes to Thromboinflammation and Recurrence in Young Patients with Acute Myocardial Infarction

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population and Patients’ Characteristics
2.2. Genomic DNA Extraction
2.3. Cell Free DNA Quantification
2.4. CitH3-DNA Complexes Quantification
2.5. miR-146a Genotyping
2.6. Follow-Up and Endpoints
2.7. Statistical Analysis
3. Results
3.1. NETosis Markers in ACS Patients and Healthy Donors
3.2. Relationship between rs2431697 and ACS
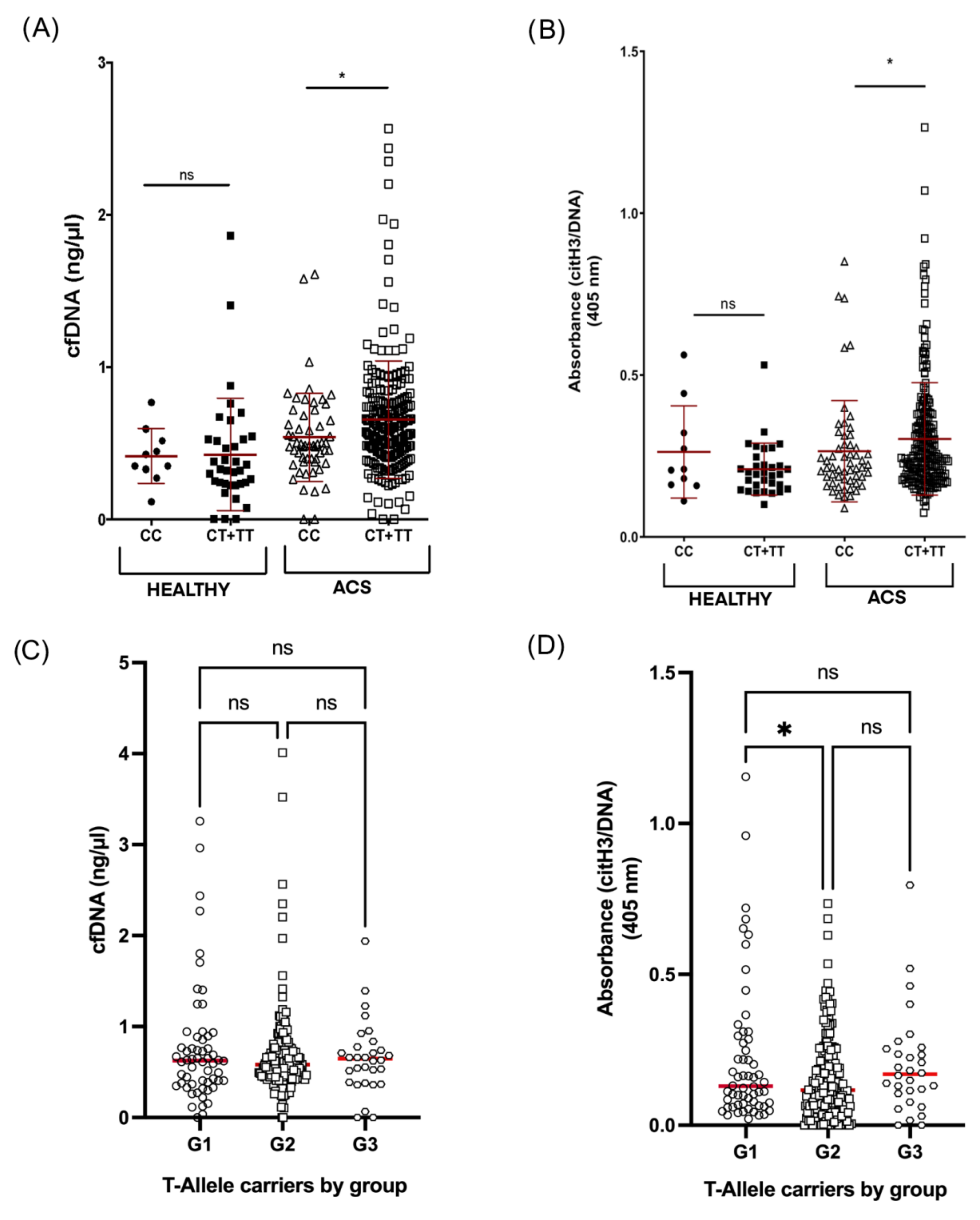
3.3. rs2431697 and NETosis Markers in ACS Patients
3.4. Associations between NETosis Markers and the Outcome of ACS
3.5. Predictive Ability of NETosis Markers Combined with rs2431697 for Cardiovascular Outcomes
4. Discussion
4.1. NETs Markers in Plasma from Young ACS
4.2. Validity of NET Levels beyond the Acute Event
4.3. Association between ACS, NETosis and rs2431697 Genotype
4.4. Clinical Outcomes, NET Markers and rs2431697 Genotype
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, A.; Wang, Y.; Spertus, J.A.; Geda, M.; Lorenze, N.; Nkonde-Price, C.; D’Onofrio, G.; Lichtman, J.H.; Krumholz, H.M. Trends in acute myocardial infarction in young patients and differences by sex and race, 2001 to 2010. J. Am. Coll. Cardiol. 2014, 64, 337–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, J.B.; Borden, W.B. Coronary heart disease in young adults. Curr. Atheroscler. Rep. 2012, 14, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Kolte, D.; Yonetsu, T.; Ye, J.C.; Libby, P.; Fuster, V.; Jang, I.K. Optical Coherence Tomography of Plaque Erosion: JACC Focus Seminar Part 2/3. J. Am. Coll. Cardiol. 2021, 78, 1266–1274. [Google Scholar] [CrossRef]
- Gulati, R.; Behfar, A.; Narula, J.; Kanwar, A.; Lerman, A.; Cooper, L.; Singh, M. Acute Myocardial Infarction in Young Individuals. Mayo Clin. Proc. 2020, 95, 136–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alkarithi, G.; Duval, C.; Shi, Y.; Macrae, F.L.; Ariëns, R.A.S. Thrombus Structural Composition in Cardiovascular Disease. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 2370–2383. [Google Scholar] [CrossRef]
- Stark, K.; Massberg, S. Interplay between inflammation and thrombosis in cardiovascular pathology. Nat. Rev. Cardiol. 2021, 18, 666–682. [Google Scholar] [CrossRef]
- Engelmann, B.; Massberg, S. Thrombosis as an intravascular effector of innate immunity. Nat. Rev. Immunol. 2013, 13, 34–45. [Google Scholar] [CrossRef]
- Pircher, J.; Engelmann, B.; Massberg, S.; Schulz, C. Platelet-Neutrophil Crosstalk in Atherothrombosis. Thromb. Haemost. 2019, 119, 1274–1282. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Brill, A.; Duerschmied, D.; Schatzberg, D.; Monestier, M.; Myers, D.D.; Wrobleski, S.K.; Wakefield, T.W.; Hartwig, J.H.; Wagner, D.D. Extracellular DNA traps promote thrombosis. Proc. Natl. Acad. Sci. USA 2010, 107, 15880–15885. [Google Scholar] [CrossRef] [Green Version]
- Pasterkamp, G.; den Ruijter, H.M.; Giannarelli, C. False Utopia of One Unifying Description of the Vulnerable Atherosclerotic Plaque: A Call for Recalibration That Appreciates the Diversity of Mechanisms Leading to Atherosclerotic Disease. Arterioscler. Thromb. Vasc. Biol. 2022, 42, e86–e95. [Google Scholar] [CrossRef]
- Roldán, V.; Arroyo, A.B.; Salloum-Asfar, S.; Manzano-Fernández, S.; García-Barberá, N.; Marín, F.; Vicente, V.; González-Conejero, R.; Martínez, C. Prognostic role of MIR146A polymorphisms for cardiovascular events in atrial fibrillation. Thromb. Haemost. 2014, 112, 781–788. [Google Scholar] [CrossRef]
- Arroyo, A.B.; de los Reyes-García, A.M.; Rivera-Caravaca, J.M.; Valledor, P.; García-Barberá, N.; Roldán, V.; Vicente, V.; Martínez, C.; González-Conejero, R. MiR-146a Regulates Neutrophil Extracellular Trap Formation That Predicts Adverse Cardiovascular Events in Patients With Atrial Fibrillation. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 892–902. [Google Scholar] [CrossRef] [Green Version]
- Arroyo, A.B.; Fernández-Pérez, M.P.; del Monte, A.; Águila, S.; Méndez, R.; Hernández-Antolín, R.; García-Barberá, N.; de los Reyes-García, A.M.; González-Jiménez, P.; Arcas, M.I.; et al. miR-146a is a pivotal regulator of neutrophil extracellular trap formation promoting thrombosis. Haematologica 2021, 106, 1636–1646. [Google Scholar] [CrossRef] [PubMed]
- Lefrançais, E.; Mallavia, B.; Zhuo, H.; Calfee, C.S.; Looney, M.R. Maladaptive role of neutrophil extracellular traps in pathogen-induced lung injury. JCI Insight 2018, 3, 98178. [Google Scholar] [CrossRef] [Green Version]
- Mangold, A.; Alias, S.; Scherz, T.; Hofbauer, T.; Jakowitsch, J.; Panzenböck, A.; Simon, D.; Laimer, D.; Bangert, C.; Kammerlander, A.; et al. Coronary Neutrophil Extracellular Trap Burden and Deoxyribonuclease Activity in ST-Elevation Acute Coronary Syndrome Are Predictors of ST-Segment Resolution and Infarct SizeNovelty and Significance. Circ. Res. 2015, 116, 1182–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Döring, Y.; Libby, P.; Soehnlein, O. Neutrophil Extracellular Traps Participate in Cardiovascular Diseases: Recent Experimental and Clinical Insights. Circ. Res. 2020, 126, 1228–1241. [Google Scholar] [CrossRef] [PubMed]
- Stakos, D.A.; Kambas, K.; Konstantinidis, T.; Mitroulis, I.; Apostolidou, E.; Arelaki, S.; Tsironidou, V.; Giatromanolaki, A.; Skendros, P.; Konstantinides, S.; et al. Expression of functional tissue factor by neutrophil extracellular traps in culprit artery of acute myocardial infarction. Eur. Heart J. 2015, 36, 1405–1414. [Google Scholar] [CrossRef]
- Liu, J.; Yang, D.; Wang, X.; Zhu, Z.; Wang, T.; Ma, A.; Liu, P. Neutrophil extracellular traps and dsDNA predict outcomes among patients with ST-elevation myocardial infarction. Sci. Rep. 2019, 9, 11599. [Google Scholar] [CrossRef] [Green Version]
- Hofbauer, T.M.; Ondracek, A.S.; Mangold, A.; Scherz, T.; Nechvile, J.; Seidl, V.; Brostjan, C.; Lang, I.M. Neutrophil Extracellular Traps Induce MCP-1 at the Culprit Site in ST-Segment Elevation Myocardial Infarction. Front. Cell Dev. Biol. 2020, 8, 1231. [Google Scholar] [CrossRef]
- Langseth, M.S.; Helseth, R.; Ritschel, V.; Hansen, C.H.; Andersen, G.Ø.; Eritsland, J.; Halvorsen, S.; Fagerland, M.W.; Solheim, S.; Arnesen, H.; et al. Double-Stranded DNA and NETs Components in Relation to Clinical Outcome After ST-Elevation Myocardial Infarction. Sci. Rep. 2020, 10, 5007. [Google Scholar] [CrossRef]
- Wang, X.; Yang, D.; Liu, J.; Fan, X.; Ma, A.; Liu, P. Prognostic value of culprit artery double-stranded DNA in ST-segment elevated myocardial infarction. Sci. Rep. 2018, 8, 9294. [Google Scholar] [CrossRef] [PubMed]
- Morrow, D.A.; Sabatine, M.S.; Brennan, M.L.; De Lemos, J.A.; Murphy, S.A.; Ruff, C.T.; Rifai, N.; Cannon, C.P.; Hazen, S.L. Concurrent evaluation of novel cardiac biomarkers in acute coronary syndrome: Myeloperoxidase and soluble CD40 ligand and the risk of recurrent ischaemic events in TACTICS-TIMI 18. Eur. Heart J. 2008, 29, 1096–1102. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, X.; Li, Z.; Chen, L.; Zhou, L.; Li, C.; Ouyang, D.S. Two Single Nucleotide Polymorphisms (rs2431697 and rs2910164) of miR-146a Are Associated with Risk of Coronary Artery Disease. Int. J. Environ. Res. Public Health 2017, 14, 514. [Google Scholar] [CrossRef]
- Mendell, J.T.; Olson, E.N. MicroRNAs in stress signaling and human disease. Cell 2012, 148, 1172–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helseth, R.; Solheim, S.; Arnesen, H.; Seljeflot, I.; Opstad, T.B. The Time Course of Markers of Neutrophil Extracellular Traps in Patients Undergoing Revascularisation for Acute Myocardial Infarction or Stable Angina Pectoris. Mediat. Inflamm. 2016, 2016, 2182358. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Healthy Donors (n = 300) | ACS Patients (n = 359) | p-Value | |
|---|---|---|---|
| Age, mean (range) | 42 (22–45) | 44 (40–47) | 0.152 |
| Male sex, N (%) | 251 (83.7) | 316 (88.0) | 0.115 |
| STEMI, N (%) | - | 212 (59.1) | - |
| NSTEACS, N (%) | - | 147 (40.9) | |
| NSTEMI, N (%) | - | 134 (37.3) | - |
| Unstable angina, N (%) | - | 13 (3.6) | - |
| Obesity, N (%) | 25 (8.3) | 124 (34.5) | <0.0001 |
| Hypertension, N (%) | 26 (8.7) | 218 (60.7) | <0.0001 |
| Diabetes, N (%) | 6 (2.0) | 74 (20.6) | <0.0001 |
| Dyslipidemia, N (%) | 61 (20.3) | 288 (80.2) | <0.0001 |
| Current smoking, N (%) | 41 (13.7) | 126 (35.1) | <0.0001 |
| rs2431697 genotype | |||
| CC, N (%) | 53 (17.7) | 60 (18.7) | 0.689 |
| CT, N (%) | 141 (47.0) | 154 (42.9) | 0.329 |
| TT, N (%) | 71 (23.7) | 105 (29.2) | 0.106 |
| C-allele, N (%) | 194 (64.7) | 214 (59.6) | 0.183 |
| T-allele, N (%) | 212 (70.7) | 261 (81.3) | 0.563 |
| G1 (n = 79) | G2 (n = 244) | G3 (n = 36) | p-Value | |
|---|---|---|---|---|
| Age, mean ± SD | 42 (39–44) | 45 (42–49) | 41.5 (39–43) | 0.305 |
| Male sex, N (%) | 63 (79.7) | 218 (89.3) | 35 (97.2) | 0.052 |
| STEMI, N (%) | 44 (55.7) | 140 (57.5) | 28 (77.8) | 0.053 |
| NSTEACS, N (%) | 35 (44.3) | 104 (42.5) | 8 (22.2) | |
| Obesity, N (%) | 21 (26.6) | 79 (32.4) | 13 (36.1) | 0.603 |
| Hypertension, N (%) | 21 (26.6) | 64 (26.2) | 6 (16.7) | 0.412 |
| Diabetes, N (%) | 10 (12.6) | 33 (13.5) | 5 (13.9) | 0.922 |
| Dyslipidemia, N (%) | 25 (31.6) | 82 (33.6) | 14 (38.9) | 0.814 |
| Current smoking, N (%) | 50 (63.3) | 177 (72.5) | 28 (77.8) | 0.316 |
| rs2431697 genotype | ||||
| CC, N (%) | 12 (15.2) | 43 (19.8) | 5 (15.6) | 0.745 |
| CT, N (%) | 34 (43.0) | 102 (42.1) | 19 (52.8) | 0.749 |
| TT, N (%) | 26 (32.9) | 72 (29.8) | 8 (22.2) | 0.683 |
| C-allele, N (%) | 46 (58.2) | 145 (59.9) | 24 (66.7) | 0.907 |
| T-allele, N (%) | 60 (83.3) | 174 (80.2) | 27 (84.4) | 0.642 |
| Patient Group | Criteria | OR; 95% CI * | p-Value |
|---|---|---|---|
| Overall cohort | citH3–DNA > Q2 + cfDNA> Q2 + rs2431697 T allele | 1.23; 0.72–2.12 | 0.452 |
| G1 | citH3–DNA > Q2 + cfDNA> Q2 + rs2431697 T allele | 0.38; 0.04–3.48 | 0.391 |
| G2 | citH3–DNA > Q2 + cfDNA> Q2 + rs2431697 T allele | 2.09; 1.10–3.97 | 0.024 |
| G3 | citH3–DNA > Q2 + cfDNA> Q2 + rs2431697 T allele |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de los Reyes-García, A.M.; Rivera-Caravaca, J.M.; Zapata-Martínez, L.; Águila, S.; Véliz-Martínez, A.; García-Barberá, N.; Gil-Perez, P.; Guijarro-Carrillo, P.J.; Orenes-Piñero, E.; López-García, C.; et al. MiR-146a Contributes to Thromboinflammation and Recurrence in Young Patients with Acute Myocardial Infarction. J. Pers. Med. 2022, 12, 1185. https://doi.org/10.3390/jpm12071185
de los Reyes-García AM, Rivera-Caravaca JM, Zapata-Martínez L, Águila S, Véliz-Martínez A, García-Barberá N, Gil-Perez P, Guijarro-Carrillo PJ, Orenes-Piñero E, López-García C, et al. MiR-146a Contributes to Thromboinflammation and Recurrence in Young Patients with Acute Myocardial Infarction. Journal of Personalized Medicine. 2022; 12(7):1185. https://doi.org/10.3390/jpm12071185
Chicago/Turabian Stylede los Reyes-García, Ascensión M., José Miguel Rivera-Caravaca, Laura Zapata-Martínez, Sonia Águila, Andrea Véliz-Martínez, Nuria García-Barberá, Pablo Gil-Perez, Pedro J. Guijarro-Carrillo, Esteban Orenes-Piñero, Cecilia López-García, and et al. 2022. "MiR-146a Contributes to Thromboinflammation and Recurrence in Young Patients with Acute Myocardial Infarction" Journal of Personalized Medicine 12, no. 7: 1185. https://doi.org/10.3390/jpm12071185