
Do Patients with Autoimmune Conditions Have Less Access to Liver Transplantation despite Superior Outcomes?

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design/Setting/Population/Procedure
2.2. Sampling
2.3. Eras
2.4. Etiology of Liver Disease
2.5. Data Collection
2.6. Data Analysis
3. Results
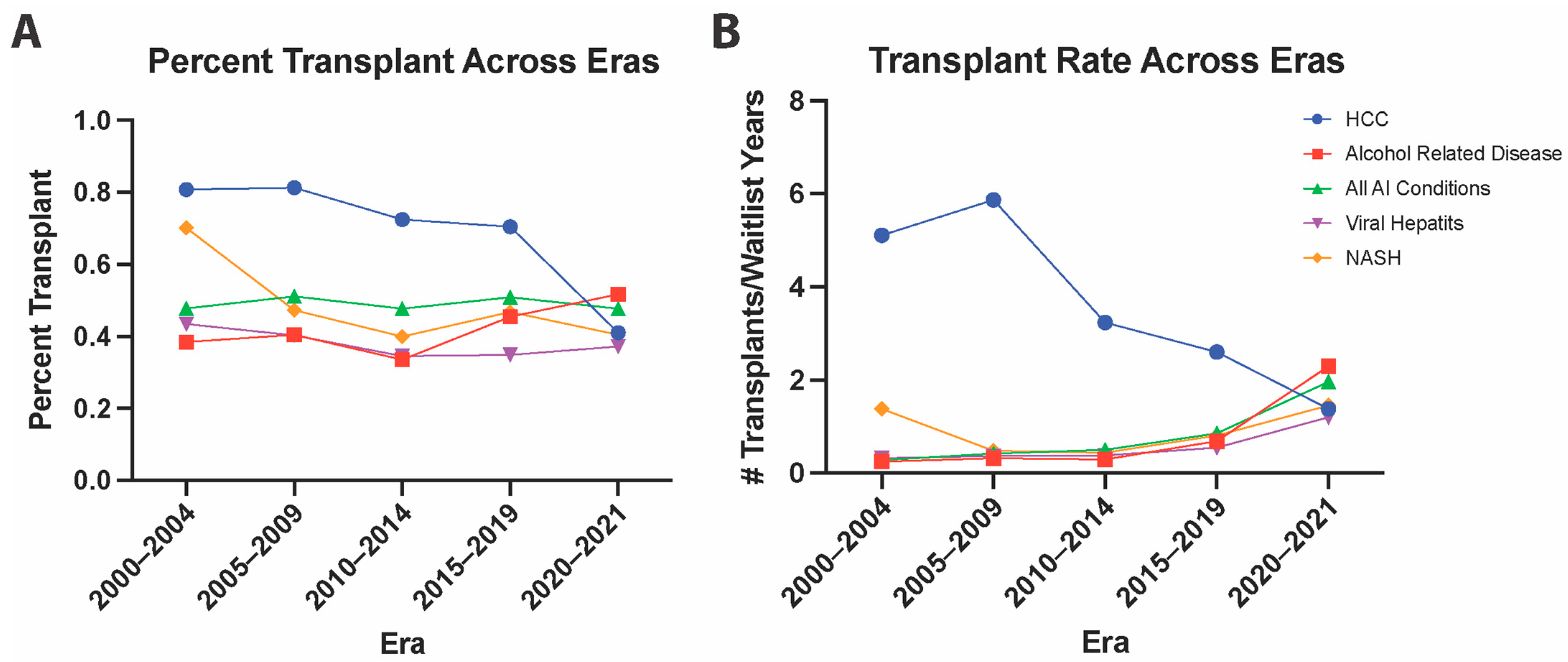
3.1. Trends in Transplant Rates and Percentage of Transplantation
3.2. Multivariate Probability of Transplant
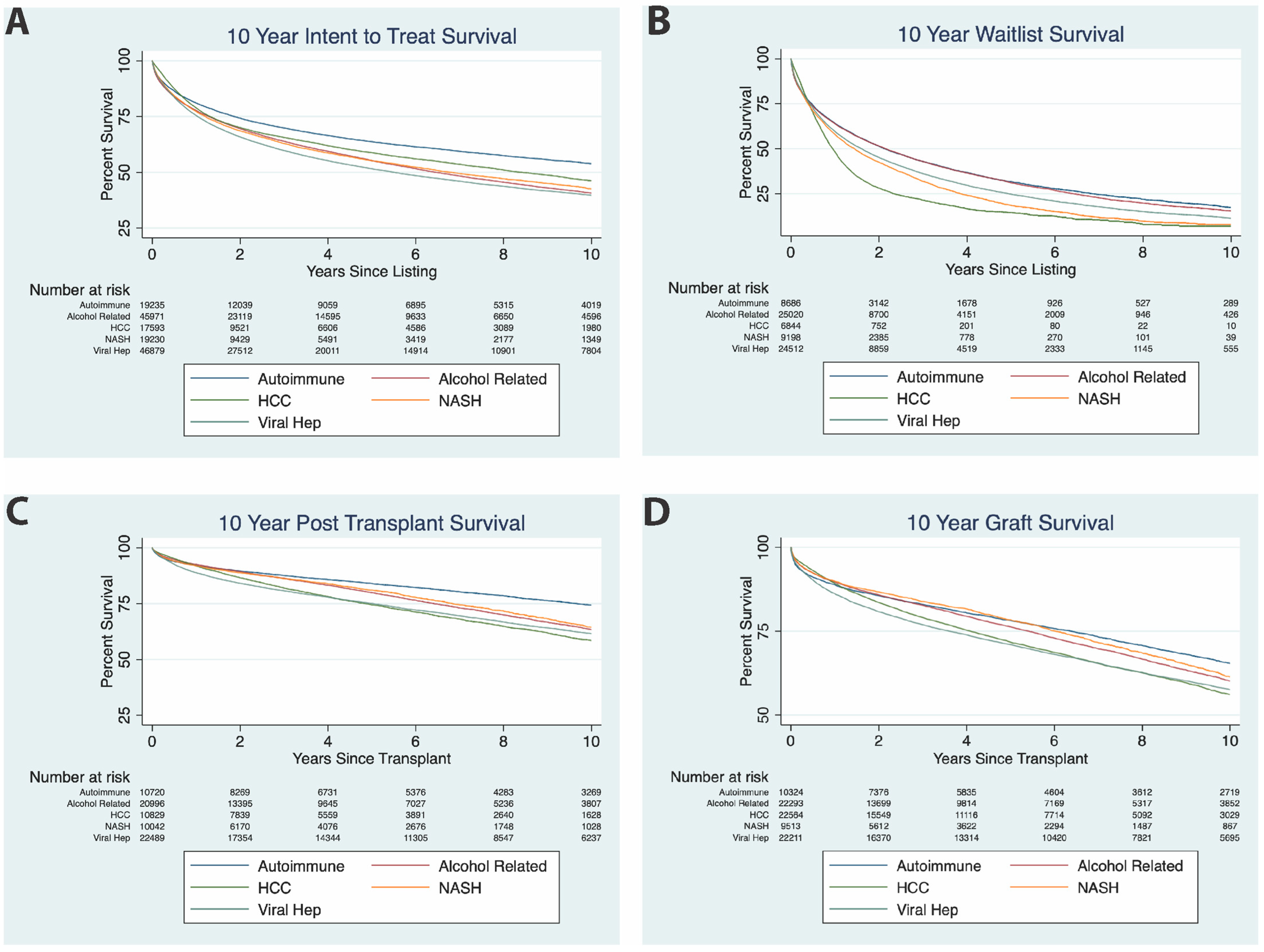
3.3. Intention-to-Treat Survival Analysis
3.4. Waitlist Survival
3.5. Post-Transplant Survival
3.6. Graft Survival Comparison between Conditions
3.7. Analysis of Autoimmune Liver Disease
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ilyas, J.A.; O’Mahony, C.A.; Vierling, J.M. Liver transplantation in autoimmune liver diseases. Best Pract. Res. Clin. Gastroenterol. 2011, 25, 765–782. [Google Scholar] [CrossRef] [PubMed]
- Mellinger, J.L.; Volk, M.L. Transplantation for alcohol-related liver disease: Is it fair? Alcohol Alcohol. 2018, 53, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Silveira, M.G.; Talwalkar, J.A.; Lindor, K.D.; Wiesner, R.H. Recurrent Primary Biliary Cirrhosis After Liver Transplantation. Am. J. Transplant. 2010, 10, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Jacob, D.A.; Neumann, U.P.; Bahra, M.; Klupp, J.; Puhl, G.; Neuhaus, R.; Langrehr, J.M. Long-term follow-up after recurrence of primary biliary cirrhosis after liver transplantation in 100 patients. Clin. Transplant. 2006, 20, 211–220. [Google Scholar] [CrossRef]
- Rowe, I.; Webb, K.; Gunson, B.K.; Mehta, N.; Haque, S.; Neuberger, J. The impact of disease recurrence on graft survival following liver transplantation: A single centre experience. Transpl. Int. 2008, 21, 459–465. [Google Scholar] [CrossRef]
- Futagawa, Y.; Terasaki, P. An analysis of the OPTN/UNOS Liver Transplant Registry. Clin. Transpl. 2004, 315–329. [Google Scholar] [PubMed]
- Jain, A.; DiMartini, A.; Kashyap, R.; Youk, A.; Rohal, S.; Fung, J. Long-term follow-up after liver transplantation for alcoholic liver disease under tacrolimus1. Transplantation 2000, 70, 1335–1342. [Google Scholar] [CrossRef]
- Doyle, M.M.; Vachharajani, N.; Maynard, E.; Shenoy, S.; Anderson, C.; Wellen, J.R.; Lowell, J.A.; Chapman, W.C. Liver Transplantation for Hepatocellular Carcinoma: Long-Term Results Suggest Excellent Outcomes. J. Am. Coll. Surg. 2012, 215, 19–28. [Google Scholar] [CrossRef]
- Afzali, A.; Berry, K.; Ioannou, G.N. Excellent posttransplant survival for patients with nonalcoholic steatohepatitis in the United States. Liver Transplant. 2011, 18, 29–37. [Google Scholar] [CrossRef]
- Onofrio, F.D.Q.; Neong, E.; Adebayo, D.; Kollmann, D.; Adeyi, O.A.; Fischer, S.; Hirschfield, G.M.; Hansen, B.E.; Bhat, M.; Galvin, Z.; et al. Single-Center North American Experience of Liver Transplantation in Autoimmune Hepatitis: Infrequent Indication but Good Outcomes for Patients. J. Can. Assoc. Gastroenterol. 2020, 4, 137–144. [Google Scholar] [CrossRef]
- Neuberger, J. Liver transplantation for primary biliary cirrhosis: Indications and risk of recurrence. J. Hepatol. 2003, 39, 142–148. [Google Scholar] [CrossRef]
- Graziadei, I.W.; Wiesner, R.H.; Marotta, P.J.; Porayko, M.K.; Hay, J.E.; Charlton, M.R.; Poterucha, J.J.; Rosen, C.B.; Gores, G.J.; LaRusso, N.F.; et al. Long-term results of patients undergoing liver transplantation for primary sclerosing cholangitis. Hepatology 1999, 30, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Goss, J.A.; Shackleton, C.R.; Farmer, D.G.; Arnaout, W.S.; Seu, P.; Markowitz, J.S.; Martin, P.; Stribling, R.J.; Goldstein, L.I.; Busuttil, R.W. Orthotopic Liver Transplantation for Primary Scierosing Cholangitis A 12-Year Single Center Experience. Ann. Surg. 1997, 225, 472. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Reyes, J.; Kashyap, R.; Dodson, S.F.; Demetris, A.J.; Ruppert, K.; Abu-Elmagd, K.; Marsh, W.; Madariaga, J.; Mazariegos, G.; et al. Long-Term Survival after Liver Transplantation in 4000 Consecutive Patients at a Single Center. Ann. Surg. 2000, 232, 490–500. [Google Scholar] [CrossRef] [Green Version]
- Roberts, M.S.; Angus, D.C.; Bryce, C.L.; Valenta, Z.; Weissfeld, L. Survival after liver transplantation in the United States: A disease-specific analysis of the UNOS database. Liver Transplant. 2004, 10, 886–897. [Google Scholar] [CrossRef]
- Axelrod, D.A.; Pomfret, E.A. Race and Sex Disparities in Liver Transplantation. JAMA 2008, 300, 2425–2426. [Google Scholar] [CrossRef]
- Cholongitas, E.; Marelli, L.; Kerry, A.; Goodier, D.W.; Nair, D.; Thomas, M.; Patch, D.; Burroughs, A.K. Female Liver Transplant Recipients with the Same GFR as Male Recipients Have Lower MELD Scores? A Systematic Bias. Am. J. Transplant. 2007, 7, 685–692. [Google Scholar] [CrossRef]
- Hurtova, M.; Duclos-Vallée, J.; Johanet, C.; Emile, J.; Roque-Afonso, A.; Bismuth, H.; Feray, C.; Samuel, D. Successful tacrolimus therapy for a severe recurrence of type 1 autoimmune hepatitis in a liver graft recipient. Liver Transplant. 2001, 7, 556–558. [Google Scholar] [CrossRef]
- Liberal, R.; Zen, Y.; Mieli-Vergani, G.; Vergani, D. Liver transplantation and autoimmune liver diseases. Liver Transplant. 2013, 19, 1065–1077. [Google Scholar] [CrossRef]
- Khalaf, H.; Mourad, W.; El-Sheikh, Y.; Abdo, A.; Helmy, A.; Medhat, Y.; Al-Sofayan, M.; Al-Sagheir, M.; Al-Sebayel, M. Liver Transplantation for Autoimmune Hepatitis: A Single-Center Experience. Transplant. Proc. 2007, 39, 1166–1170. [Google Scholar] [CrossRef]
- Astarcioglu, I.; Egeli, T.; Unek, T.; Akarsu, M.; Sagol, O.; Obuz, F.; Ozbilgin, M.; Agalar, A.A.; Ağalar, C. Liver Transplant in Patients with Primary Sclerosing Cholangitis: Long-Term Experience of a Single Center. Exp. Clin. Transplant. 2018, 16, 434–438. [Google Scholar] [PubMed]
- Hay, J.E. Liver Transplantation for primary biliary cirrhosis and primary sclerosing cholangitis: Does medical treatment alter timing and selection? Liver Transplant. Surg. 1998, 4 (Suppl. S1), S9–S17. [Google Scholar]
- Goulis, J.; Leandro, G.; Burroughs, A.K. Randomised controlled trials of ursodeoxycholic-acid therapy for primary biliary cirrhosis: A meta-analysis. Lancet 1999, 354, 1053–1060. [Google Scholar] [CrossRef]
- Lammers, W.J.; van Buuren, H.R.; Hirschfield, G.M.; Janssen, H.L.; Invernizzi, P.; Mason, A.L.; Ponsioen, C.Y.; Floreani, A.; Corpechot, C.; Mayo, M.J.; et al. Levels of Alkaline Phosphatase and Bilirubin Are Surrogate End Points of Outcomes of Patients with Primary Biliary Cirrhosis: An International Follow-up Study. Gastroenterology 2014, 147, 1338–1349.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindor, K.; Therneau, T.; Jorgensen, R.; Malinchoc, M.; Dickson, E. Effects of ursodeoxycholic acid on survival in patients with primary biliary cirrhosis. Gastroenterology 1996, 110, 1515–1518. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Sugawara, Y.; Kokudo, N. Liver transplantation and autoimmune hepatitis. Intractable Rare Dis. Res. 2015, 4, 33–38. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, E.Q.; Levy, M.F.; Goldstein, R.M.; Fasola, C.G.; Tillery, G.W.; Netto, G.J.; Watkins, D.L.; Weinstein, J.S.; Murray, N.G.; Byers, D.; et al. The changing clinical presentation of recurrent primary biliary cirrhosis after liver transplantation. Transplantation 2003, 76, 1583–1588. [Google Scholar] [CrossRef]
- Gautam, M.; Cheruvattath, R.; Balan, V. Recurrence of autoimmune liver disease after liver transplantation: A systematic review. Liver Transplant. 2006, 12, 1813–1824. [Google Scholar] [CrossRef]
- Nevens, F. PBC-transplantation and disease recurrence. Best Pract. Res. Clin. Gastroenterol. 2018, 34, 107–111. [Google Scholar] [CrossRef]
- Levitsky, J.; Hart, J.; Cohen, S.M.; Te, H.S. The effect of immunosuppressive regimens on the recurrence of primary biliary cirrhosis after liver transplantation. Liver Transplant. 2003, 9, 733–736. [Google Scholar] [CrossRef]
- Krishnamoorthy, T.L.; Miezynska-Kurtycz, J.; Hodson, J.; Gunson, B.K.; Neuberger, J.; Milkiewicz, P.; Oo, Y.H. Longterm corticosteroid use after liver transplantation for autoimmune hepatitis is safe and associated with a lower incidence of recurrent disease. Liver Transplant. 2015, 22, 34–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathurin, P.; Moreno, C.; Samuel, D.; Dumortier, J.; Salleron, J.; Durand, F.; Castel, H.; Duhamel, A.; Pageaux, G.-P.; Leroy, V.; et al. Early Liver Transplantation for Severe Alcoholic Hepatitis. N. Engl. J. Med. 2011, 365, 1790–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shipley, L.C.; Singal, A.K. Liver transplantation for alcoholic hepatitis. Transl. Gastroenterol. Hepatol. 2020, 5, 26. [Google Scholar] [CrossRef] [PubMed]
- Cholankeril, G.; Goli, K.; Rana, A.; Hernaez, R.; Podboy, A.; Jalal, P.; Da, B.L.; Satapathy, S.K.; Kim, D.; Ahmed, A.; et al. Impact of COVID-19 Pandemic on Liver Transplantation and Alcohol-Associated Liver Disease in the USA. Hepatology 2021, 74, 3316–3329. [Google Scholar] [CrossRef] [PubMed]
- Herrick-Reynolds, K.M.; Punchhi, G.; Greenberg, R.S.; Strauss, A.T.; Boyarsky, B.J.; Weeks-Groh, S.R.; Krach, M.R.; Anders, R.A.; Gurakar, A.; Chen, P.-H.; et al. Evaluation of Early vs Standard Liver Transplant for Alcohol-Associated Liver Disease. JAMA Surg. 2021, 156, 1026. [Google Scholar] [CrossRef]
- Iruzubieta, P.; Crespo, J.; Fábrega, E. Long-term survival after liver transplantation for alcoholic liver disease. World J. Gastroenterol. 2013, 19, 9198–9208. [Google Scholar] [CrossRef] [PubMed]
- Joo, D.J.; Lee, J.G.; Lee, J.; Yang, S.J.; Han, D.H.; Kim, E.J.; Choi, G.H.; Choi, J.S.; Kim, M.S.; Kim, S.I. Oncologic outcomes of alcohol induced HCC after liver transplantation. Transplantation 2020, 104, S524. [Google Scholar] [CrossRef]
- Wang, X.; Li, J.; Riaz, D.; Shi, G.; Liu, C.; Dai, Y. Outcomes of Liver Transplantation for Nonalcoholic Steatohepatitis: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 12, 394–402.e1. [Google Scholar] [CrossRef]
- Wright, T.L.; Donegan, E.; Hsu, H.H.; Ferrell, L.; Lake, J.R.; Kim, M.; Combs, C.; Fennessy, S.; Roberts, J.P.; Ascher, N.L.; et al. Recurrent and acquired hepatitis C viral infection in liver transplant recipients. Gastroenterology 1992, 103, 317–322. [Google Scholar] [CrossRef]
- Gane, E.J.; Portmann, B.C.; Naoumov, N.V.; Smith, H.M.; Underhill, J.A.; Donaldson, P.T.; Maertens, G.; Williams, R. Long-term outcome of hepatitis C infection after liver transplantation. N. Engl. J. Med. 1996, 334, 815–835. [Google Scholar] [CrossRef]
- Böker, K.H.; Dalley, G.; Bahr, M.J.; Maschek, H.; Tillmann, H.L.; Trautwein, C.; Oldhaver, K.; Bode, U.; Pichlmayr, R.; Manns, M.P. Viral Hepatitis Long-Term Outcome of Hepatitis C Virus Infection after Liver Transplantation. Viral Hepat. 1997, 25, 203–210. [Google Scholar]
- Ghobrial, R.M.; Steadman, R.; Gornbein, J.; Lassman, C.; Holt, C.D.; Chen, P.; Farmer, D.G.; Yersiz, H.; Danino, N.; Collisson, E.; et al. A 10-Year Experience of Liver Transplantation for Hepatitis C: Analysis of Factors Determining Outcome in over 500 Patients. Ann. Surg. 2001, 234, 384–394. [Google Scholar] [CrossRef]
- Sheiner, P.A.; Schwartz, M.E.; Mor, E.; Schluger, L.K.; Theise, N.; Kishikawa, K.; Kolesnikov, V.; Bodenheimer, H.; Emre, S.; Miller, C.M. Severe or multiple rejection episodes are associated with early recurrence of hepatitis C after orthotopic liver transplantation. Hepatology 1995, 21, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Rosen, H.R.; Gretch, D.R.; Oehlke, M.; Flora, K.D.; Benner, K.G.; Rabkin, J.M.; Corless, C.L. Timing and severity of initial hepatitis C recurrence as predictors of long-term liver allograft injury1. Transplantation 1998, 65, 1178–1182. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, E.M.; Erb, S.R.; Partovi, N.; Scudamore, C.H.; Chung, S.W.; Frighetto, L.; Eggen, H.J.; Steinbrecher, U.P. Liver transplantation for chronic hepatitis B infection with the use of combination lamivudine and low-dose hepatitis B immune globulin. Liver Transplant. Surg. 1999, 5, 520–525. [Google Scholar] [CrossRef] [Green Version]
- Lenci, I.; Milana, M.; Grassi, G.; Manzia, T.M.; Gazia, C.; Tisone, G.; Angelico, R.; Baiocchi, L. Hepatitis B virus recurrence after liver transplantation: An old tale or a clear and present danger? World J. Gastroenterol. 2020, 26, 2166. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Table 1: Patient Demographics | ||||||
|---|---|---|---|---|---|---|
| 2000–2004 | 2005–2009 | 2010–2014 | 2015–2019 | 2020 July 2021 | Total | |
| Number of patients | 44,390 | 48,037 | 51,940 | 55,060 | 18,549 | 217,976 |
| Listing age, mean (SD) | 51.1 (10.1) | 52.9 (10.2) | 55.0 (10.2) | 55.7 (11.0) | 54.9 (11.8) | 53.9 (10.6) |
| Gender (%F) | 36.72 | 35 | 35.12 | 36.41 | 37.79 | 35.97 |
| Race (%) | ||||||
| White | 73.44 | 71.28 | 70.33 | 69.8 | 70.15 | 71 |
| Black | 7.87 | 8.62 | 9.05 | 7.8 | 7.08 | 8.23 |
| Hispanic | 13.4 | 14.33 | 14.77 | 16.2 | 16.93 | 14.94 |
| Asian | 4.18 | 4.67 | 4.47 | 4.44 | 4.02 | 4.41 |
| % Transplanted | 48.7 | 45.8 | 49.5 | 44.6 | 48.87 | 52.2 |
| Years waitlist, mean (SD) | 1.45 (2.79) | 1.09 (2.25) | 0.913 (1.78) | 0.587 (1.08) | 0.251 (0.384) | 0.927 (1.99) |
| Diagnosis (% All Patients) | ||||||
| PBC | 3.75 | 2.88 | 2.54 | 2.49 | 2.51 | 3.05 |
| PSC | 4.67 | 4.13 | 3.92 | 3.83 | 4.03 | 4.28 |
| Autoimmune Cirrhosis | 3.32 | 2.91 | 2.96 | 2.97 | 2.75 | 3.12 |
| HCC | 4.62 | 12.19 | 17.67 | 17.06 | 12.77 | 14.7 |
| Alcoholic Cirrhosis | 21.95 | 20.87 | 21.15 | 28.29 | 36.05 | 25.63 |
| Viral Hepatitis | 37.38 | 34.06 | 31.68 | 16.97 | 8 | 27.64 |
| NASH | 1 | 6.16 | 10.78 | 17.92 | 18.03 | 10.17 |
| Donor Characteristics | ||||||
| Mean cold ischemia time hours (SD) | 7.76 (3.59) | 7.18 (3.31) | 6.35 (2.58) | 5.94 (2.13) | 6.35 (2.97) | 6.67 (2.95) |
| DRI (SD) | 1.67 (0.38) | 1.69 (0.40) | 1.66 (0.37) | 1.68 (0.40) | 1.78 (0.43) | 1.68 (0.39) |
| DCD (% Donors) | 1.21 | 2.78 | 2.82 | 4.49 | 4.13 | 3.02 |
| Table 2: Listing Variables Used for Multivariate Analysis | ||
|---|---|---|
| African American | Encephalopathy | Payment Method |
| Age | Highest Level of Education | Private |
| 18–30 | High School Dropout | Medicaid |
| 60–65 | High School | Region |
| >65 | Technical | Serum Na |
| Albumin | Bachelors | <125 |
| 2.0–2.5 | Doctor | 125–130 |
| 1.5–2.0 | ICU | 130–135 |
| <1.5 | INR | 145–150 |
| Ascites at Listing | <2.5 | 150–155 |
| Bilirubin | 2.5–3 | >155 |
| <2 | 3–3.5 | TIPSS |
| 8–16 | 3.5–4 | Transplant Location |
| 16–32 | >4 | Regional |
| >32 | Life Support | National |
| BMI | MELD | Foreign |
| 30–35 | 30–35 | Ventilator Status |
| 35–40 | 35–40 | Working |
| >40 | >40 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keeling, S.S.; McDonald, M.F.; Anand, A.; Goff, C.R.; Christmann, C.R.; Barrett, S.C.; Kueht, M.; Goss, J.A.; Cholankeril, G.; Rana, A. Do Patients with Autoimmune Conditions Have Less Access to Liver Transplantation despite Superior Outcomes? J. Pers. Med. 2022, 12, 1159. https://doi.org/10.3390/jpm12071159
Keeling SS, McDonald MF, Anand A, Goff CR, Christmann CR, Barrett SC, Kueht M, Goss JA, Cholankeril G, Rana A. Do Patients with Autoimmune Conditions Have Less Access to Liver Transplantation despite Superior Outcomes? Journal of Personalized Medicine. 2022; 12(7):1159. https://doi.org/10.3390/jpm12071159
Chicago/Turabian StyleKeeling, Stephanie S., Malcolm F. McDonald, Adrish Anand, Cameron R. Goff, Caroline R. Christmann, Spencer C. Barrett, Michael Kueht, John A. Goss, George Cholankeril, and Abbas Rana. 2022. "Do Patients with Autoimmune Conditions Have Less Access to Liver Transplantation despite Superior Outcomes?" Journal of Personalized Medicine 12, no. 7: 1159. https://doi.org/10.3390/jpm12071159