
Current Approaches in the Allocation of Liver Transplantation

 ,
,  , and
, and
Abstract
:1. Introduction
2. World Liver Transplant History
3. Liver Transplant Allocation
3.1. Indications for Liver Transplant
3.2. Models of Prognosis and Organ Allocation
- University of California in San Francisco (UCSF) criteria (1 nodule ≤ 6.5 cm, or n ≤ 3 nodules ≤ 4.5 cm, or total ≤ 8 cm) [35];
- Additions to the Milan criteria: number of nodules + maximum tumor size without vascular invasion should reach a maximum of seven [33];
- The AFP score, which takes into account the size, number of nodules, and level of AFP (applied in France) [34].
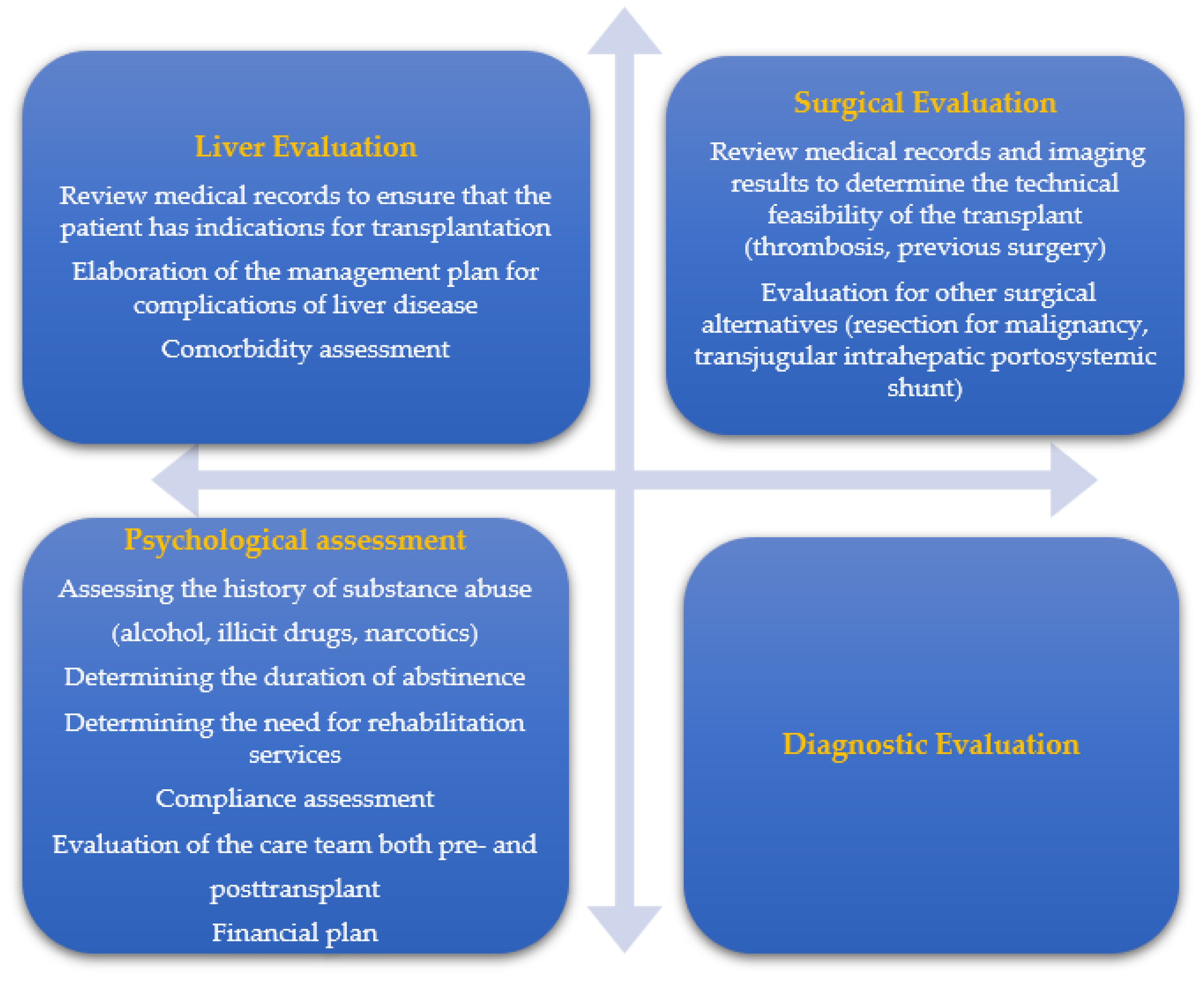
3.3. Pre-Transplant Evaluation
3.4. Absolute Contraindications for Liver Transplantation
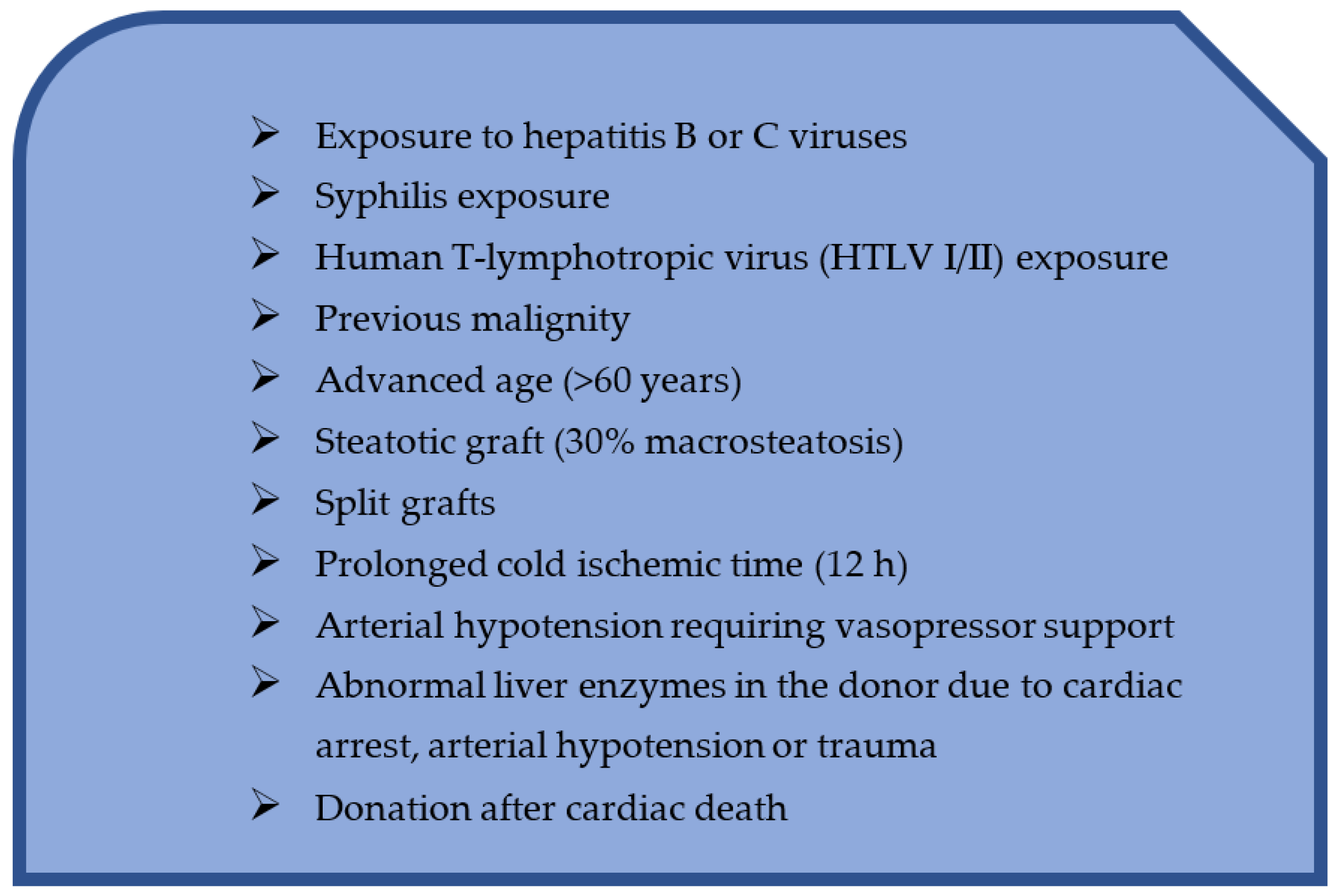
3.5. Relative Contraindications for Liver Transplantation
3.6. Waiting List Management and Exclusion from the List
- Patients with acute hepatic impairment, included in most countries on a “super-emergency” waiting list, giving them absolute priority over all other potential recipients. In this category of patients, the transplant should be performed within hours or days.
- Patients with decompensated liver cirrhosis. The priority of liver transplantation is dictated in this situation by the value of the MELD score. Thus, patients with a very high MELD score will be able to receive a liver transplant within days or weeks, while patients with an intermediate or low MELD score will wait for months or years.
- the usual evaluation of the MELD score;
- standard screening by upper gastrointestinal endoscopy for the presence of esophageal or gastric varices and their prophylaxis;
- evaluation by abdominal ultrasound with vascular Doppler examination, every 6 months, to identify any tumors (hepatocellular carcinoma) or vascular complications;
- adequate prophylaxis of spontaneous bacterial peritonitis. Patients with refractory ascites may benefit from TIPS or repeated evacuation paracentesis.
3.7. Allocation of Organs
3.8. Extension of the Donor Base
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Organ Procurement and Tranplantation Network. Available online: https://optn.transplant.hrsa.gov (accessed on 10 March 2022).
- Bodzin, A.S.; Baker, T.B. Liver Transplantation Today: Where We Are Now and Where We Are Going. Liver Transplant. 2018, 24, 1470–1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adam, R.; Karam, V.; Cailliez, V.; Grady, J.G.O.; Mirza, D.; Cherqui, D.; Klempnauer, J.; Salizzoni, M.; Pratschke, J.; Jamieson, N.; et al. 2018 Annual Report of the European Liver Transplant Registry (ELTR)-50-year evolution of liver transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsien, C.; Tan, H.; Sharma, S.; Palaniyappan, N.; Wijayasiri, P.; Leung, K.; Hayre, J.; Mowlem, E.; Kang, R.; Eddowes, P.J.; et al. Long-term outcomes of liver transplant recipients followed up in non-transplant centers: Care closer to home. Clin. Med. 2021, 21, e32–e38. [Google Scholar] [CrossRef] [PubMed]
- Durand, F.; Antoine, C.; Soubrane, O. Liver Transplantation in France. Liver Transplant. 2019, 25, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Busuttil, R.W.; De Carlis, L.G.; Mihaylov, P.V.; Gridelli, B.; Fassati, L.R.; Starzl, T.E. The First Report of Orthotopic Liver Transplantation in the Western World. Am. J. Transplant. 2012, 12, 1385–1387. [Google Scholar] [CrossRef] [PubMed]
- Welch, C.S. A note on transplantation of the whole liver in dogs. Transpl. Bullet. 1955, 2, 54–55. [Google Scholar]
- Starzl, T.E.; Groth, C.G.; Brettschneider, L.; Penn, I.; Fulginiti, V.A.; Moon, J.B.; Blanchard, H.; Martin, A.J.; Porter, K.A. Orthotopic homotransplantation of the human liver. Ann. Surg. 1968, 168, 392–415. [Google Scholar] [CrossRef]
- Song, A.T.W.; Avelino-Silva, V.I.; Pecora, R.A.A.; Pugliese, V.; D’Albuquerque, L.A.C.; Abdala, E. Liver transplantation: Fifty years of experience. World J. Gastroenterol. 2014, 20, 5363–5374. [Google Scholar] [CrossRef]
- Merion, R.M.; Sharma, P.; Mathur, A.K.; Schaubel, D.E. Evidence-based development of liver allocation: A review. Transpl. Int. 2011, 24, 965–972. [Google Scholar] [CrossRef] [Green Version]
- Calne, R.; Rolles, K.; Thiru, S.; Mcmaster, P.; Craddock, G.; Aziz, S.; White, D.; Evans, D.; Dunn, D.; Henderson, R.; et al. Cyclosporin a initially as the only immunosuppressant in 34 recipients of cadaveric organs: 32 kidneys, 2 pancreases, and 2 livers. Lancet 1979, 314, 1033–1036. [Google Scholar] [CrossRef]
- Meirelles, R.F.; Salvaalaggio, P.; de Rezende, M.B.; Evangelista, A.S.; Guardia, B.D.; Matielo, C.E.L.; Neves, D.B.; Pandullo, F.L.; Felga, G.E.G.; Alves, J.A.S.; et al. Liver transplantation: History, outcames and perspectives. Einstein 2015, 13, 149–152. [Google Scholar] [CrossRef] [PubMed]
- E Starzl, T. The long reach of liver transplantation. Nat. Med. 2012, 18, 1489–1492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sass, D.A.; Reich, D.J. Liver Transplantation in the 21st Century: Expanding the Donor Options. Gastroenterol. Clin. N. Am. 2011, 40, 641–658. [Google Scholar] [CrossRef] [PubMed]
- Eunmi, G.; Man, K.J.; Kyeongman, J.; Hyejeon, P.; Danbee, K.; Junhee, C.; Young, G.; Jinkyeong, P. Recipient age and mortality after liver transplantation: A population-based cohort study. Transplantation 2018, 102, 2025–2032. [Google Scholar]
- O’Leary, J.G.; Lepe, R.; Davis, G.L. Indications for liver transplatation. Gastroenterology 2008, 134, 1764–1776. [Google Scholar] [CrossRef] [Green Version]
- Chu, K.K.-W.; Wong, K.H.-C.; Chok, K.S.-H. Expanding indications for liver transplant: Tumor and patient factors. Gut Liver 2021, 15, 19–30. [Google Scholar] [CrossRef] [Green Version]
- Brancaccio, G.; Vitale, A.; Signoriello, G.; Gaeta, G.B.; Cillo, U. Changing indications for liver transplant: Slow decline of hepatitis viruses in Italy. Infect. Dis. 2020, 52, 557–562. [Google Scholar] [CrossRef]
- Aguire-Valadez, J.; Torre, A.; Vilatoba, M.; Contreras, A.; Sanchez-Cedillo, A.; Antolinez-Motta, J.; Garcia-Juarez, I. Indications for liver transplant. Rev. Invest. Clin. 2014, 66, 534–546. [Google Scholar]
- Marot, A.; Moreno, C.; Deltenre, P. Liver transplant for alcoholic hepatitis: A current clinical overview. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 591–600. [Google Scholar] [CrossRef]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef]
- Kim, S.Y.; Yim, H.J.; Lee, J.; Lee, B.J.; Kim, D.I.; Jung, S.W.; Han, W.S.; Lee, J.S.; Koo, J.S.; Seo, Y.S.; et al. Comparison of CTP, MELD, and MELD-Na scores for predicting short term mortality in patients with liver cirrhosis. Korean J. Gastroenterol. 2007, 50, 92–100. [Google Scholar] [PubMed]
- Tonko, S.; Dufour, J.-F. Hepatology scores. Ther. Umsch. 2013, 70, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Child-Pugh Score for Chronic Liver Disease and Cirrhosis. Available online: https://www.healthline.com (accessed on 5 February 2022).
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.K.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Hanto, D.W.; Fishbein, T.M.; Pinson, C.W.; Olthoff, K.M.; Shiffman, M.L.; Punch, J.D.; Goodrich, N.P. Liver and intestine transplantation: Summary analysis, 1994–2003. Am. J. Transplant. 2005, 5, 916–933. [Google Scholar] [CrossRef] [Green Version]
- De Moraes, A.C.O.; de Oliveira, P.C.; da Fonseca-Neto, O.C. The impact of MELD Score on liver transplant allocation and results: An integrative review. Arq. Bras. Cir. Dig. 2017, 30, 65–68. [Google Scholar] [CrossRef] [Green Version]
- Cholongitas, E.; Burroughs, A. The evaluation in the prioritization for liver transplantation. Ann. Gastroenterol. 2012, 25, 6–13. [Google Scholar]
- Ritschl, P.V.; Wiering, L.; Dziodzio, T.; Jara, M.; Kruppa, J.; Schoeneberg, U.; Raschzok, N.; Butz, F.; Globke, B.; Seika, P.; et al. The Effects of MELD-Based Liver Allocation on Patient Survival and Waiting List Mortality in a Country with a Low Donation Rate. J. Clin. Med. 2020, 9, 1929. [Google Scholar] [CrossRef]
- Luo, X.; Massie, A.B.; Gentry, S.E.; Segev, D.L. MELD allocation system: There is always space to improve. Am. J. Transplant. 2018, 18, 2834–2835. [Google Scholar] [CrossRef] [Green Version]
- Therese, B.; George, M.; David, G. Exception point applications for 15 points: An unintended consequence of the Sgare policy. Liver Transpl. 2012, 18, 1302–1309. [Google Scholar]
- Nobel, Y.R.; Goldberg, D.S. Variable use of MELD exception points in patients with neuroendocrine tumors metastatic to the liver and its impact on patient outcomes. Transplantation 2015, 99, 2341–2346. [Google Scholar] [CrossRef] [Green Version]
- Mazzaferro, V.M.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Duvoux, C.; Roudot–Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver Transplantation for Hepatocellular Carcinoma: A Model Including α-Fetoprotein Improves the Performance of Milan Criteria. Gastroenterology 2012, 143, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.Y.; Ferrell, L.; Bass, N.M.; Watson, J.J.; Bacchetti, P.; Venook, A.; Ascher, N.L.; Roberts, J.P. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology 2001, 33, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Crespo, G.; Trota, N.; Londoño, M.-C.; Mauro, E.; Baliellas, C.; Castells, L.; Castellote, J.; Tort, J.; Forns, X.; Navasa, M. The efficacy of direct anti-HCV drugs improves early post-liver transplant survival and induces significant changes in waiting list composition. J. Hepatol. 2018, 69, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.J.; Aguilar, M.; Cheung, R.; Perumpail, R.B.; Harrison, S.A.; Younossi, Z.M.; Ahmed, A. Non-alcoholic steatohepatitis is the second leading etiology of liver diseases among adults awaiting liver transplantation in the United States. Gastroenterology 2015, 148, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Merion, R.M.; Schaubel, D.E.; Dykstra, D.M.; Freeman, R.B.; Port, F.K.; Wolfe, R.A. The Survival Benefit of Liver Transplantation. Am. J. Transplant. 2005, 5, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Northup, P.G.; Intagliata, N.M.; Shah, N.L.; Pelletier, S.J.; Berg, C.L.; Argo, C.K. Excess mortality on the liver transplant waiting list: Unintended policy consequences and model for End-Stage Liver Disease (MELD) inflation. Hepatology 2014, 61, 285–291. [Google Scholar] [CrossRef]
- Sharma, P.; Schaubel, D.E.; Gong, Q.; Guidinger, M.; Merion, R.M. End-stage liver disease candidates at the highest model for end-stage liver disease scores have higher wait-list mortality than status-1A candidates. Hepatology 2012, 55, 192–198. [Google Scholar] [CrossRef] [Green Version]
- Wiesner, R.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease score and allocation of donor livers. Gastroenterology 2003, 124, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Gustot, T.; Fernandez, J.; Garcia, E.; Morando, F.; Caraceni, P.; Alessandria, C.; Laleman, W.; Trebicka, J.; Elkrief, L.; Hopf, C.; et al. Clinical Course of acute-on-chronic liver failure syndrome and effects on prognosis. Hepatology 2015, 62, 243–252. [Google Scholar] [CrossRef]
- Samji, N.S.; Heda, R.; Satapathy, S.K. Peri-transplant management of nonalcoholic fatty liver disease in liver transplant candidates. Transl. Gastroenterol. Hepatol. 2020, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- White, S.L.; Rawlinson, W.; Boan, P.; Sheppeard, V.; Wong, G.; Waller, K.; Opdam, H.; Kaldor, J.; Fink, M.; Verran, D.; et al. Infectious Disease Transmission in Solid Organ Transplantation: Donor Evaluation, Recipient Risk, and Outcomes of Transmission. Transpl. Direct 2019, 5, e416. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Domínguez-Gil, B.; Busic, M.; Cortez-Pinto, H.; Craig, J.C.; Jager, K.J.; Mahillo, B.; Stel, V.S.; Valentin, M.O.; Zoccali, C.; et al. Organ donation and transplantation: A multi-stakeholder call to action. Nat. Rev. Nephrol. 2021, 17, 554–568. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, N. Selection for Liver Transplantation: Indications and Evaluation. Curr. Hepatol. Rep. 2020, 19, 203–212. [Google Scholar] [CrossRef]
- Legaz, I.; Boix, F.; Lopez, M.; Alfaro, R.; Galian, J.A.; Llorente, S.; Campillo, J.A.; Botella, C.; Ramirez, P.; Sanchez-Bueno, F.; et al. Influence of performed Antibodies in Liver Transplantation. J. Clin. Med. 2020, 9, 708. [Google Scholar] [CrossRef]
- Muro, M. The endless history or search for the true role of alloantibodies in liver transplantation. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101544. [Google Scholar] [CrossRef]
- Farkas, S.; Hackl, C.; Schlitt, H.J. Overview of the Indications and Contraindications for Liver Transplantation. Cold Spring Harb. Perspect. Med. 2014, 4, a015602. [Google Scholar] [CrossRef] [Green Version]
- Varma, V.; Mehta, N.; Kumaran, V.; Nundy, S. Indications and Contraindications for Liver Transplantation. Int. J. Hepatol. 2011, 2011, 121862. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.-C.; Ho, C.-M.; Hu, R.-H.; Ho, M.-C.; Wu, Y.-M.; Lee, P.-H. Prophylactic liver transplantation for high-risk recurrent hepatocellular carcinoma. World J. Hepatol. 2016, 8, 1309–1317. [Google Scholar] [CrossRef]
- Shimamura, T.; Goto, R.; Watanabe, M.; Kawamura, N.; Takada, Y. Liver Transplantation for Hepatocellular Carcinoma: How Should We Improve the Thresholds? Cancers 2022, 14, 419. [Google Scholar] [CrossRef]
- Shoham, S.; Marr, K.A. Invasive fungal infections in solid organ transplant recipients. Futur. Microbiol. 2012, 7, 639–655. [Google Scholar] [CrossRef] [Green Version]
- Cahn-Fuller, K.L.; Parent, B. Transplant eligibility for patients with affective and psychotic disorders: A review of practices and a call for justice. BMC Med. Ethic 2017, 18, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dew, M.A.; DiMartini, A.F.; Steel, J.; Dabbs, A.D.V.; Myaskovsky, L.; Unruh, M.; Greenhouse, J. Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs. Liver Transplant. 2008, 14, 159–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammond, C.; Hussaini, T.; Yoshida, E.M. Medical adherence and liver transplantation: A brief review. Can. Liver J. 2021, 4, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Dolnikov, S.; Adam, R.; Cherqui, D.; Allard, M.A. Liver transplantation in elderly patients: What do we know at the beginning of 2020? Surg. Today 2020, 50, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Nair, S.; Verma, S.; Thuluvath, P.J. Obesity and its effect on survival in patients undergoing orthotopic liver transplantation in the United States. Hepatology 2002, 35, 105–109. [Google Scholar] [CrossRef]
- Cosarderelioglu, C.; Cosar, A.M.; Gurakar, M.; Pustavoitau, A.; Russell, S.D.; Dagher, N.N.; Gurakar, A. Portopulmonary Hypertension and Liver Transplant: Recent Review of the Literature. Exp. Clin. Transplant. 2016, 14, 113–120. [Google Scholar]
- Salgia, R.J.; Goodrich, N.P.; Simpson, H.; Merion, R.M.; Sharma, P. Outcomes of liver transplantation for porto-pulmonary hypertension in model for end-stage liver disease era. Am. J. Dig. Dis. 2014, 59, 1976–1982. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Palli, G.; Taurà, P.; Balust, J.; Beltrán, J.; Zavala, E.; Garcia-Valdecasas, J. Liver Transplantation in High-Risk Patients: Hepatopulmonary Syndrome and Portopulmonary Hypertension. Transplant. Proc. 2005, 37, 3861–3864. [Google Scholar] [CrossRef]
- Price, A.; Whitwell, S.; Henderson, M. Impact of pdychotic disorder on transplant eligibility and outcomes. Curr. Opin. Organ Transplant. 2014, 19, 196–200. [Google Scholar] [CrossRef]
- Botha, J.; Fabian, J.; Etheredge, H.; Conradie, F.; Tiemessen, C.T. HIV and solid organ transplantation: Where are we now? Curr. HIV/AIDS Rep. 2019, 16, 404–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ELTR Report. Available online: http://www.eltr.org (accessed on 10 March 2022).
- Samuel, D.; Coilly, A. Management of patients with liver diseases on the waiting list for transplantation: A major impact to the success of liver transplantation. BMC Med. 2018, 16, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patrizia, B.; Andrew, B.; Ivo, G.; Jacques, P. EASL Clinical practice guidelines: Liver transplantation. J. Hepatol. 2016, 64, 433–485. [Google Scholar]
- Wendon, J.; Cordoba, J.; Dhawan, A.; Larsen, F.S.; Manns, M.; Samuel, D.; Simpson, K.J.; Yaron, I.; Bernardi, M. Clinical Practice EASL Guidelines on the management of acute (fulminant) liver failure. J. Hepatol. 2017, 66, 1047–1048. [Google Scholar] [CrossRef] [PubMed]
- Gheorghe, G.; Bungău, S.; Ceobanu, G.; Ilie, M.; Bacalbaşa, N.; Bratu, O.G.; Vesa, C.M.; Găman, M.-A.; Diaconu, C.C. The non-invasive assessment of hepatic fibrosis. J. Formos. Med. Assoc. 2020, 120, 794–803. [Google Scholar] [CrossRef]
- Felmlee, D.J.; Coilly, A.; Chung, R.T.; Samuel, D.; Baumert, T.F. New perspectives for preventing hepatitis C virus liver graft infection. Lancet Infect. Dis. 2016, 16, 735–745. [Google Scholar] [CrossRef] [Green Version]
- Manns, M.; Samuel, D.; Gane, E.J.; Mutimer, D.; McCaughan, G.; Buti, M.; Prieto, M.; Calleja, J.L.; Peck-Radosavljevic, M.; Müllhaupt, B.; et al. Ledipasvir and sofosbuvir plus ribavirin in patients with genotype 1 or 4 hepatitis C virus infection and advanced liver disease: A multicentre, open-label, randomised, phase 2 trial. Lancet Infect. Dis. 2016, 16, 685–697. [Google Scholar] [CrossRef]
- Debette-Gratien, M.; Tabouret, T.; Antonini, M.T.; Dalmay, F.; Carrier, P.; Legros, R.; Jacques, J.; Vincent, F.; Sautereau, D.; Samuel, D.; et al. Personalized adapted physical activity before liver transplantation: Acceptability and results. Transplantation 2015, 99, 145–150. [Google Scholar] [CrossRef]
- Charpentier, K.P.; Mavanur, A. Removing patients from the liver transplant wait list: A survey of US liver transplant programs. Liver Transplant. 2008, 14, 303–307. [Google Scholar] [CrossRef]
- Elalouf, A.; Pliskin, J.S.; Kogut, T. Attitudes, knowledge, and preferences of the Israeli public regarding the allocation of donor organs for transplantation. ISR J. Health Policy Res. 2020, 9, 25. [Google Scholar] [CrossRef]
- Bartling, T.; Oedingen, C.; Kohlmann, T.; Schrem, H.; Krauth, C. Comparing preferences of physicians and patients regarding the allocation of donor organs: A systematic review. Transplant. Rev. 2019, 34, 100515. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K. Evolution of Liver Transplant Selection Criteria and U.S. Allocation Policy for Patients with Hepatocellular Carcinoma. Semin. Liver Dis. 2020, 40, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, J. Liver allocation. Minerva Gastroenterol. Dietol. 2018, 64, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Moghe, A.; Ganesh, S.; Humar, A.; Molinari, M.; Jonassaint, N. Expanding Donor Selection and Recipient Indications for Living Donor Liver Transplantation. Clin. Liver Dis. 2021, 25, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Trotter, P.B.; Summers, D.M.; Robb, M.; Hulme, W.; Ushiro-Lumb, I.; Watson, C.J.E.; Neuberger, J.; Bradley, J.A. Deceased Organ Donors With a History of Increased Risk Behavior for the Transmission of Blood-Borne Viral Infection: The UK Experience. Transplantation 2017, 101, 1679–1689. [Google Scholar] [CrossRef]
- Bălăceanu, A.; Diaconu, C.; Mateescu, D.; Stănică, A. Hepatocellular carcinoma with hepatic and pulmonary metastasis, inferior vena cava and left pulmonary artery thrombosis in a patient with asymptomatic hepatitis C. Case report. Med. Ultrason. 2010, 12, 345–348. [Google Scholar]
- Nguyen, D. Brain Death and True Patient Care. Linacre Q. 2016, 83, 258–282. [Google Scholar] [CrossRef] [Green Version]
- Abt, P.L.; Desai, N.M.; Crawford, M.D.; Forman, L.M.; Markmann, J.W.; Olthoff, K.M.; Markmann, J.F. Survival Following Liver Transplantation From Non-Heart-Beating Donors. Ann. Surg. 2004, 239, 87–92. [Google Scholar] [CrossRef]
- De l’Hortet, A.C.; Takeishi, K.; Guzman-Lepe, J.; Handa, K.; Matsubara, K.; Fukumitsu, K.; Dorko, K.; Presnell, S.C.; Yagi, H.; Soto-Gutierrez, A. Liver-regenerative transplantation: Regrow and reset. Am. J. Transplant. 2016, 16, 1688–1696. [Google Scholar]
- Hackl, C.; Schmidt, K.M.; Süsal, C.; Döhler, B.; Zidek, M.; Schlitt, H.J. Split liver transplantation: Current developments. World J. Gastroenterol. 2018, 24, 5312–5321. [Google Scholar] [CrossRef]
- Park, G.-C.; Hwang, S.; Song, G.-W.; Jung, D.-H.; Ha, T.-Y.; Ahn, C.-S.; Moon, D.-B.; Kim, K.-H.; Yoon, Y.-I.; Kang, W.-H.; et al. Prognosis of Split Liver Transplantation Compared with Whole Liver Transplantation in Adult Patients: Single-center Results Under the Korean MELD Score-based Allocation Policy. J. Korean Med. Sci. 2020, 35, e304. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.S. Liver Donors in Liver Transplantation. Gastroenterology 2009, 134, 1802–1813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, C.L.; Gillespie, B.W.; Merion, R.M.; Brown, R.S.; Abecassis, M.M.; Trotter, J.F.; Fisher, R.A.; Freise, C.E.; Ghobrial, R.M.; Shaked, A.; et al. Improvement in Survival Associated With Adult-to-Adult Living Donor Liver Transplantation. Gastroenterology 2007, 133, 1806–1813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freise, C.E.; Gillespie, B.W.; Koffron, A.J.; Lok, A.S.F.; Pruett, T.L.; Emond, J.C.; Fair, J.H.; Fisher, R.A.; Olthoff, K.M.; Trotter, J.F.; et al. Recipient Morbidity After Living and Deceased Donor Liver Transplantation: Findings from the A2ALL Retrospective Cohort Study. Am. J. Transplant. 2008, 8, 2569–2579. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Indications for Liver Transplantation. |
|---|
|
| Points | 1 | 2 | 3 |
|---|---|---|---|
| Hepatic encephalopathy | None | Minimal | Advanced |
| Ascites | None | Slight | Moderate |
| Serum bilirubin (mg/dL) | <2.0 | 2–3 | >3.0 |
| Serum albumin (g/dL) | >3.5 | 2.8–3.5 | <2.8 |
| Prothrombin time (seconds) | 1–4 | 5–6 | >6 |
| CTP classes | Score | ||
| A | 5-6 | ||
| B | 7-9 | ||
| C | 10-15 | ||
| Survival | 1 year | 2 years | |
| A | 100% | 85% | |
| B | 80% | 60% | |
| C | 45% | 35% | |
| Exceptional MELD Score Points Appraisal Conditions |
|---|
|
| Absolute Contraindications |
|---|
|
| Relative Contraindications |
|---|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ionescu, V.A.; Diaconu, C.C.; Bungau, S.; Jinga, V.; Gheorghe, G. Current Approaches in the Allocation of Liver Transplantation. J. Pers. Med. 2022, 12, 1661. https://doi.org/10.3390/jpm12101661
Ionescu VA, Diaconu CC, Bungau S, Jinga V, Gheorghe G. Current Approaches in the Allocation of Liver Transplantation. Journal of Personalized Medicine. 2022; 12(10):1661. https://doi.org/10.3390/jpm12101661
Chicago/Turabian StyleIonescu, Vlad Alexandru, Camelia Cristina Diaconu, Simona Bungau, Viorel Jinga, and Gina Gheorghe. 2022. "Current Approaches in the Allocation of Liver Transplantation" Journal of Personalized Medicine 12, no. 10: 1661. https://doi.org/10.3390/jpm12101661