
Multimodality Imaging Assessment of Desmoid Tumors: The Great Mime in the Era of Multidisciplinary Teams

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Epidemiology and Histopathology
3. Clinical Presentation and Treatment
4. Imaging
5. Ultrasound Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Desmoid Tumor | US | CT | MRI |
|---|---|---|---|
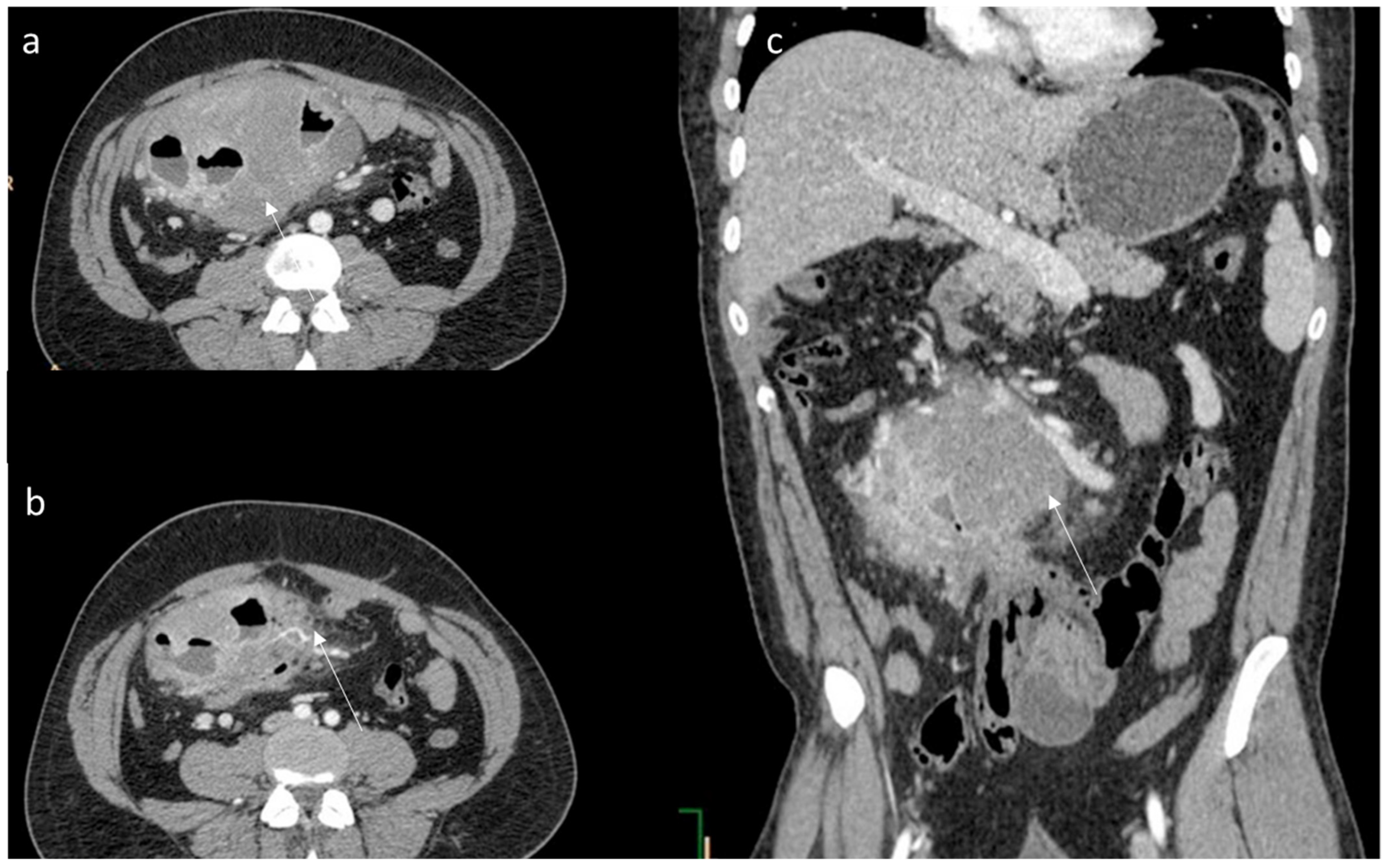
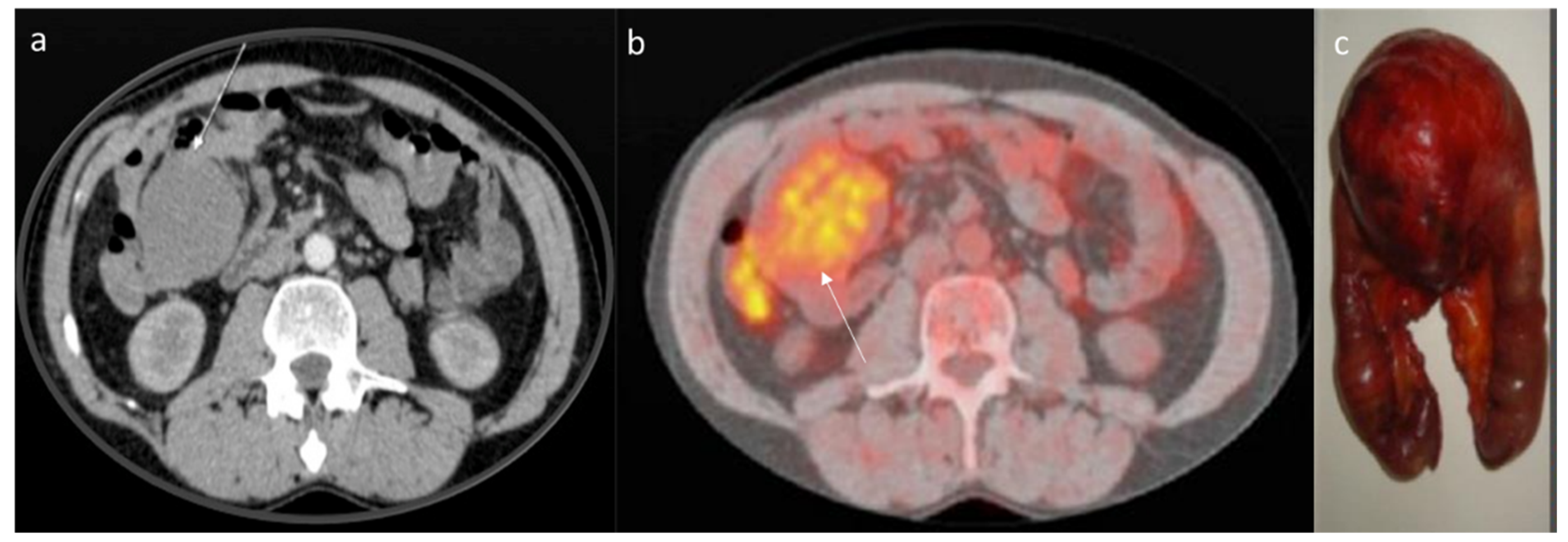
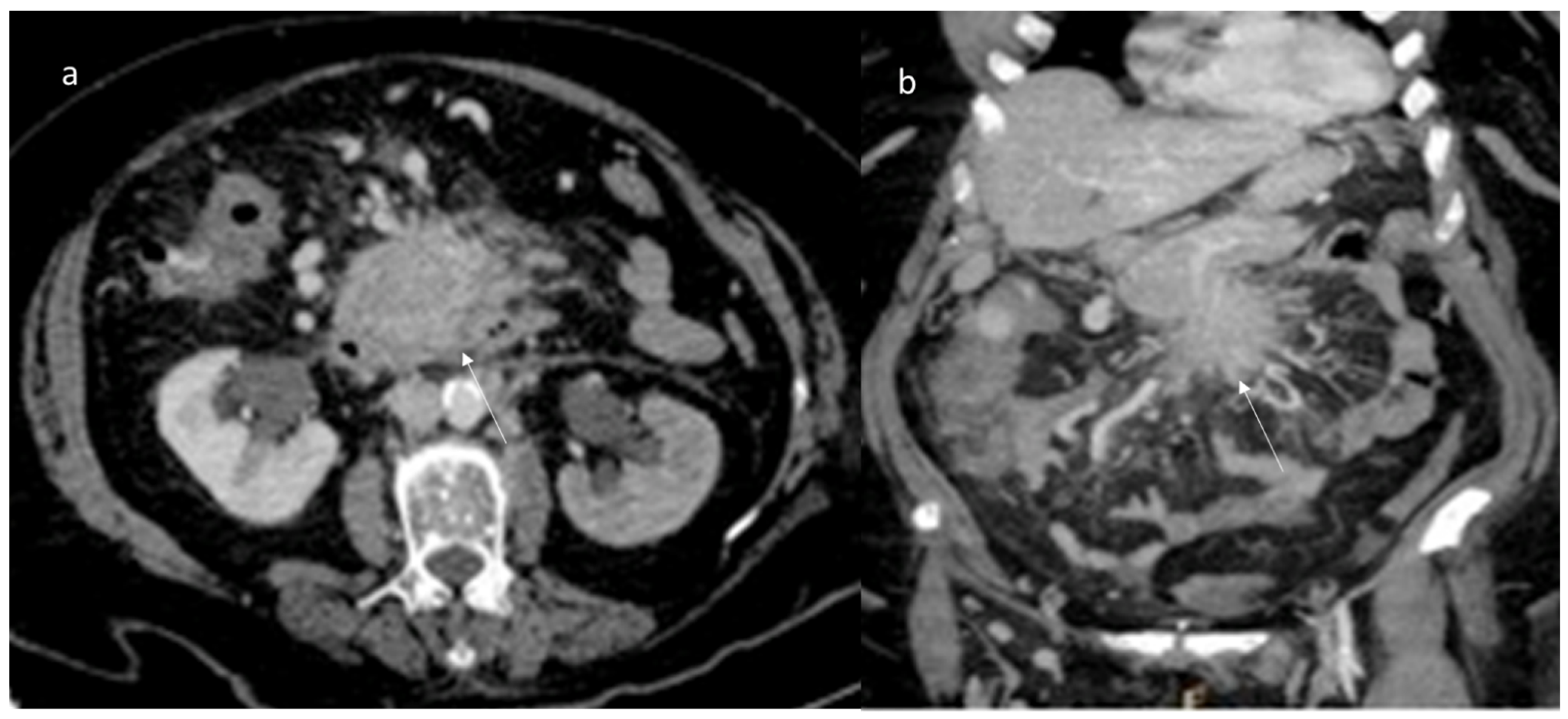
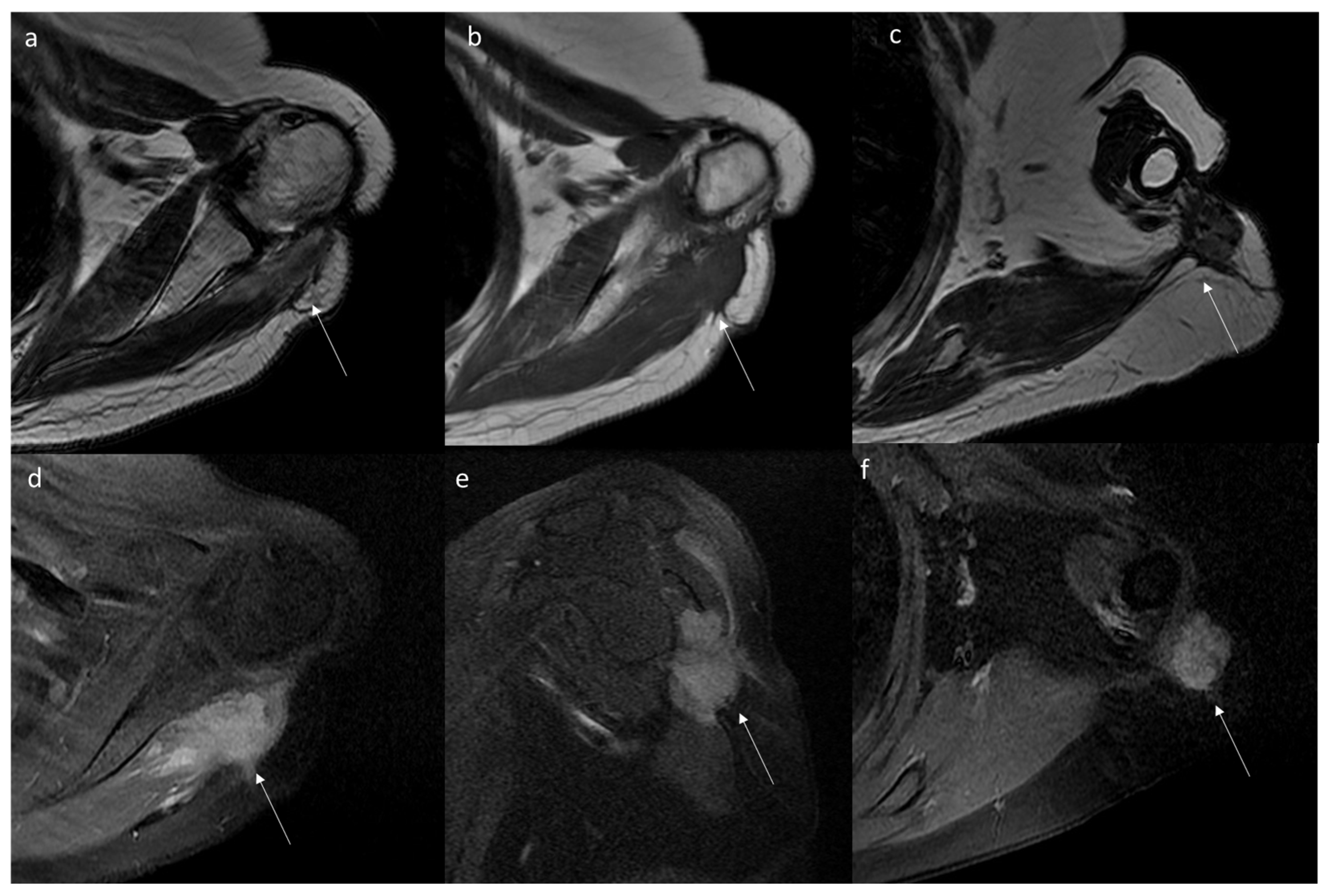
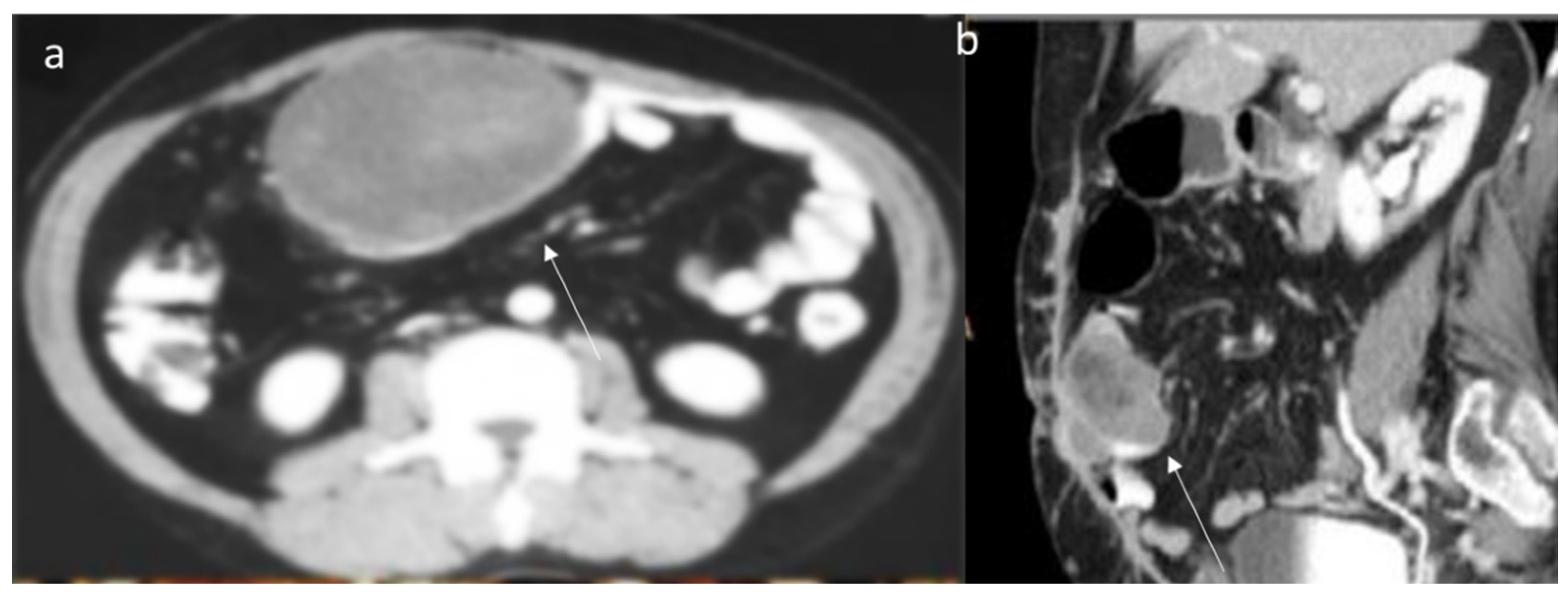
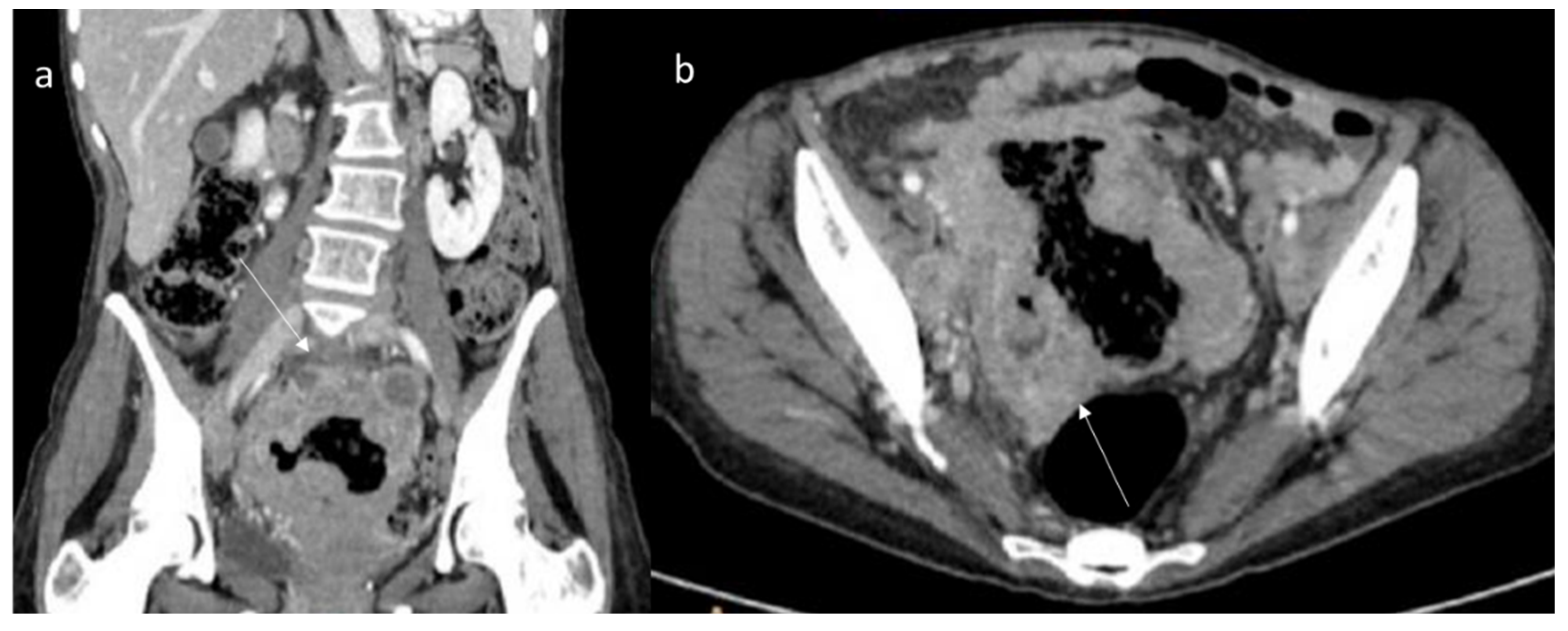
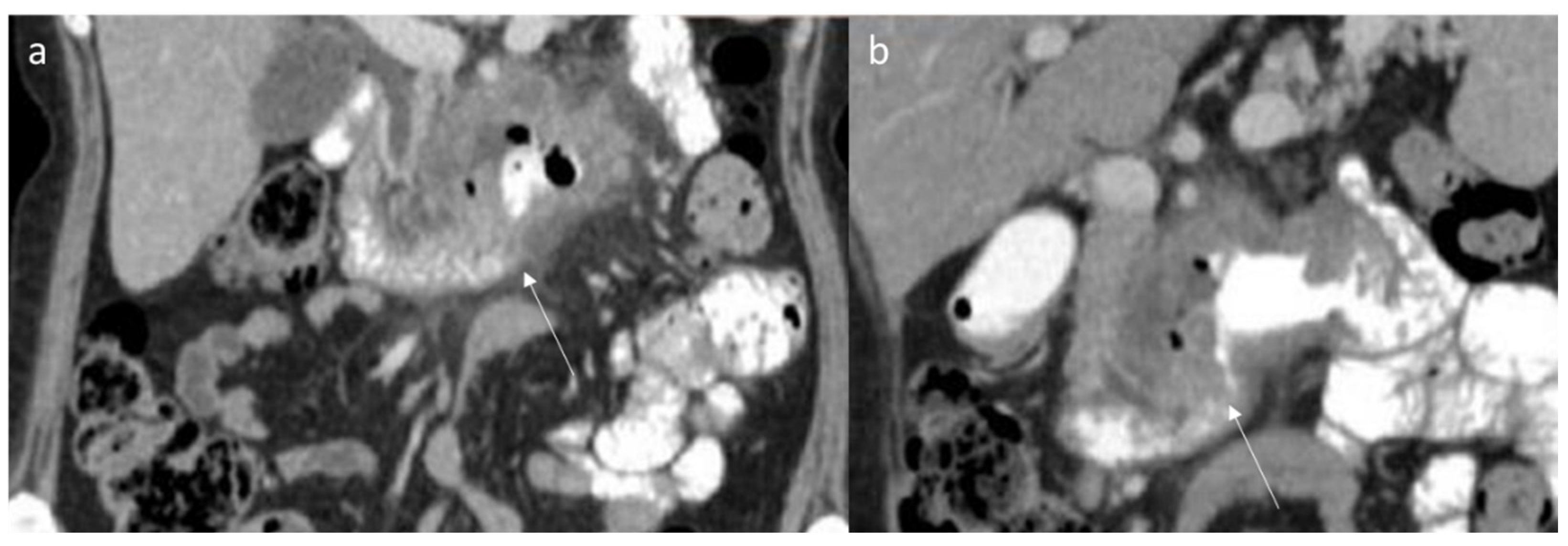
| Abdominal features [80] | Variable appearance ranging from well-circumscribed to poorly defined infiltrative heterogeneous solid mass with variable echogenicity. Vascularity is variable. At CEUS, early enhancement of the contrast agent and a very long washout | CT findings of intra-abdominal lesions are determined by the amount of collagen and myxoid tissue; therefore, the myxoid component of the tumor tends to be hypodense compared to skeletal muscle, while the collagen and fibrotic component may be isodense or hyperdense. After intravenous contrast administration, the enhancement is mild to moderate | Heterogeneous pattern, with signal iso- to hyperintense to skeletal muscle on T2-weighted images and isointense to muscle on T1-weighted images. Decreased signal intensity on T2-weighted images most likely results from dense collagen and hypocellularity; conversely, increased T2 signal intensity reflects a high content of spindle cells. DTs commonly (90%) show moderate to intense contrast enhancement, especially in the more cellular and less fibrotic regions. |
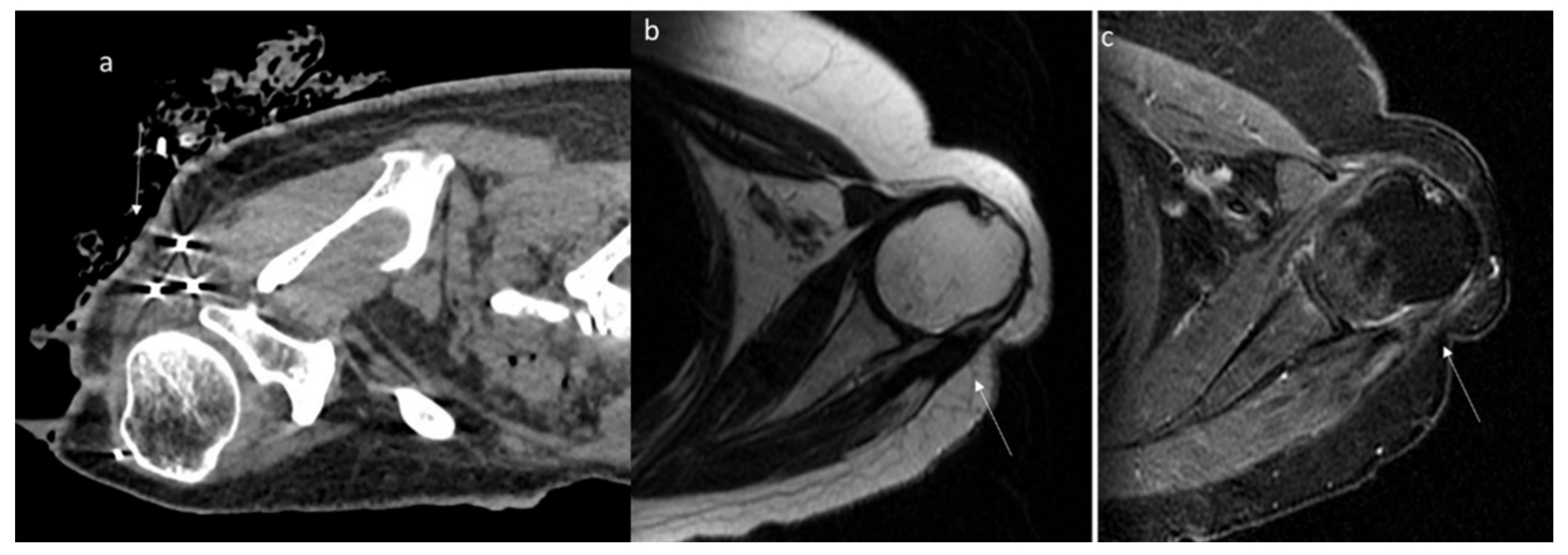
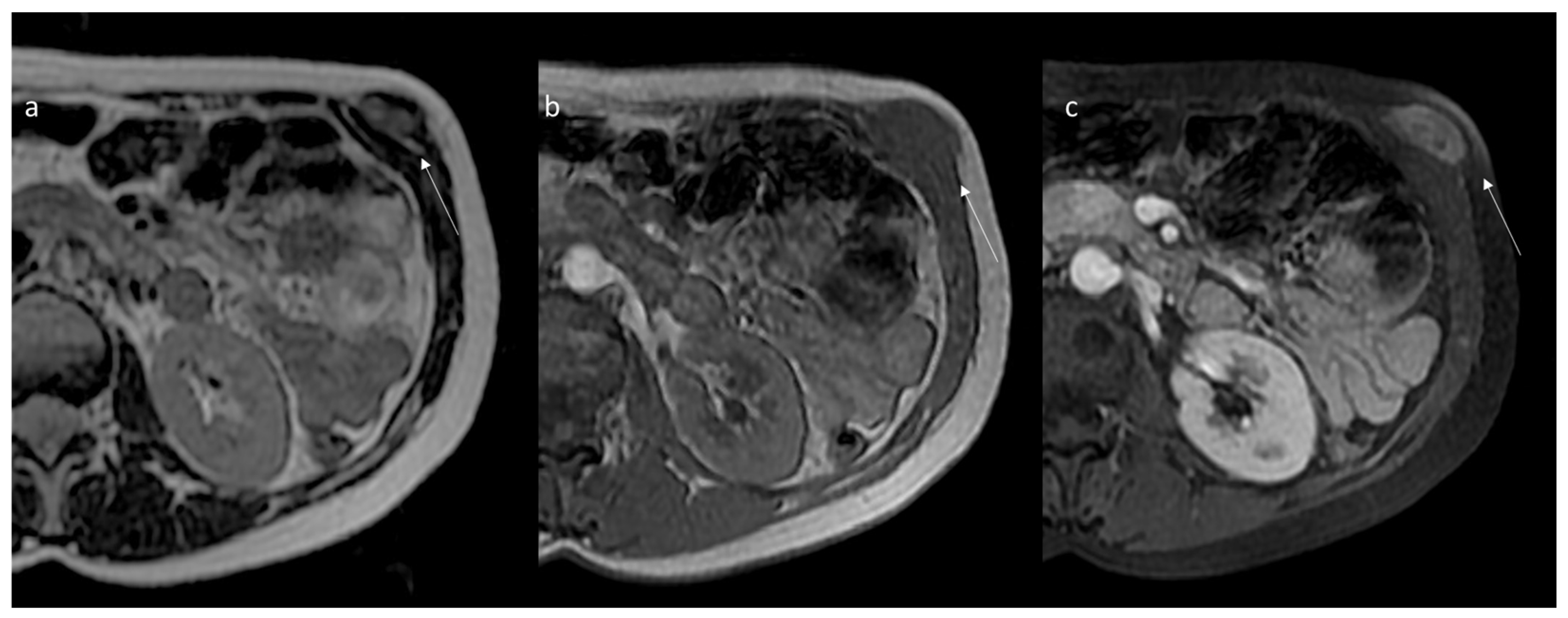
| Extra-abdominal Features [137] | Variable appearance from well-circumscribed to poorly defined infiltrative heterogeneous solid mass with variable echogenicity. Vascularity is variable. At CEUS, early enhancement of the contrast agent and a very long washout | Slightly lower density, a higher degree of enhancement and unclear boundaries | Extra-abdominal DTs typically occur in the intermuscular location along deep fascia and may show a thin rim of surrounding fat (split fat sign), linear enhancing extension along the fascial planes, and feathery margins resembling a flame (flame sign). |
| Advantages | Inexpensive; widely available; safe [111,112,113,114,115,116] | Requires high spatial resolution to obtain sufficient anatomical detail for the detection of deep lesions and for targeting interventional procedures [80] | Multiparametric approach; the exceptional contrast resolution; functional assessment [138,139,140,141,142,143] |
| Weakness | Operator dependence; poor performance for small intra-abdominal lesions; patient’s collaboration [111,112,113,114,115,116] | Radiation exposure [97] | Long examination and interpretation time; high costs [97] |
6. Computed Tomography Assessment
7. Magnetic Resonance Imaging Assessment
8. Differential Diagnoses
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Desmoid Tumor Working Group. The management of desmoid tumours: A joint global consensus-based guideline approach for adult and paediatric patients. Eur. J. Cancer 2020, 127, 96–107. [Google Scholar] [CrossRef] [Green Version]
- Ganeshan, D.; Amini, B.; Nikolaidis, P.; Assing, M.; Vikram, R. Current Update on Desmoid Fibromatosis. J. Comput. Assist. Tomogr. 2019, 43, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Chibon, F.; Salas, S. Adult desmoid tumors: Biology, management and ongoing trials. Curr. Opin. Oncol. 2017, 29, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.V.; Belli, A.; Ottaiano, A.; Nasti, G.; La Porta, M.; Danti, G.; Cappabianca, S.; et al. Intrahepatic cholangiocarcinoma and its differential diagnosis at MRI: How radiologist should assess MR features. Radiol. Med. 2021, 126, 1584–1600. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.A.M.; Cafarelli, F.P.; Paparella, M.T.; Rennie, W.J.; Guglielmi, G. Phosphaturic mesenchymal tumors: Radiological aspects and suggested imaging pathway. Radiol. Med. 2021, 126, 1609–1618. [Google Scholar] [CrossRef] [PubMed]
- Danti, G.; Flammia, F.; Matteuzzi, B.; Cozzi, D.; Berti, V.; Grazzini, G.; Pradella, S.; Recchia, L.; Brunese, L.; Miele, V. Gastrointestinal neuroendocrine neoplasms (GI-NENs): Hot topics in morphological, functional, and prognostic imaging. Radiol. Med. 2021, 126, 1497–1507. [Google Scholar] [CrossRef]
- Karmazanovsky, G.; Gruzdev, I.; Tikhonova, V.; Kondratyev, E.; Revishvili, A. Computed tomography-based radiomics approach in pancreatic tumors characterization. Radiol. Med. 2021, 126, 1388–1395. [Google Scholar] [CrossRef]
- Fusco, R.; Petrillo, M.; Granata, V.; Filice, S.; Sansone, M.; Catalano, O.; Petrillo, A. Magnetic resonance imaging evaluation in neoadjuvant therapy of locally advanced rectal cancer: A systematic review. Radiol. Oncol. 2017, 51, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Fusco, R.; Sansone, M.; Granata, V.; Setola, S.V.; Petrillo, A.; Fusco, R.; Sansone, M.; Granata, V.; Setola, S.V.; Petrillo, A. A systematic review on multiparametric MR imaging in prostate cancer detection. Infect. Agents Cancer 2017, 12, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granata, V.; Fusco, R.; Avallone, A.; Filice, F.; Tatangelo, F.; Piccirillo, M.; Grassi, R.; Izzo, F.; Petrillo, A. Critical analysis of the major and ancillary imaging features of LI-RADS on 127 proven HCCs evaluated with functional and morphological MRI: Lights and shadows. Oncotarget 2017, 8, 51224–51237. [Google Scholar] [CrossRef] [Green Version]
- Linee Guida 2020 Per Sarcomi Dei Tessuti Molli e GIST. Available online: https://www.aiom.it/wp-content/uploads/2020/10/2020_LG_AIOM_Sarcomi.pdf (accessed on 12 June 2022).
- Barabino, M.; Gurgitano, M.; Fochesato, C.; Angileri, S.A.; Franceschelli, G.; Santambrogio, R.; Mariani, N.M.; Opocher, E.; Carrafiello, G. LI-RADS to categorize liver nodules in patients at risk of HCC: Tool or a gadget in daily practice? Radiol. Med. 2021, 126, 5–13. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Filice, S.; Catalano, O.; Piccirillo, M.; Palaia, R.; Izzo, F.; Petrillo, A. The current role and future prospectives of functional parameters by diffusion weighted imaging in the assessment of histologic grade of HCC. Infect. Agents Cancer 2018, 13, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlacchio, A.; Chegai, F.; Roma, S.; Merolla, S.; Bosa, A.; Francioso, S. Degradable starch microspheres transarterial chemoembolization (DSMs-TACE) in patients with unresectable hepatocellular carcinoma (HCC): Long-term results from a single-center 137-patient cohort prospective study. Radiol. Med. 2020, 125, 98–106. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Avallone, A.; Catalano, O.; Filice, F.; Leongito, M.; Palaia, R.; Izzo, F.; Petrillo, A. Major and ancillary magnetic resonance features of LI-RADS to assess HCC: An overview and update. Infect. Agents Cancer 2017, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- De Filippo, M.; Ziglioli, F.; Russo, U.; Pagano, P.; Brunese, L.; Bertelli, E.; Pagnini, F.; Maestroni, U. Radiofrequency ablation (RFA) of T1a renal cancer with externally cooled multitined expandable electrodes. Radiol. Med. 2020, 125, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Arrigoni, F.; Bruno, F.; Gianneramo, C.; Palumbo, P.; Zugaro, L.; Zoccali, C.; Barile, A.; Masciocchi, C. Evolution of the imaging features of osteoid osteoma treated with RFA or MRgFUS during a long-term follow-up: A pictorial review with clinical correlations. Radiol. Med. 2020, 125, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.V.; Palaia, R.; Belli, A.; Miele, V.; Brunese, L.; Petrillo, A.; Izzo, F. Assessment of Ablation Therapy in Pancreatic Cancer: The Radiologist’s Challenge. Front. Oncol. 2020, 10, 560952. [Google Scholar] [CrossRef]
- Granata, V.; Grassi, R.; Fusco, R.; Belli, A.; Palaia, R.; Carrafiello, G.; Miele, V.; Petrillo, A.; Izzo, F. Local ablation of pancreatic tumors: State of the art and future perspectives. World J. Gastroenterol. 2021, 27, 3413–3428. [Google Scholar] [CrossRef]
- Trombadori, C.M.L.; D’Angelo, A.; Ferrara, F.; Santoro, A.; Belli, P.; Manfredi, R. Radial Scar: A management dilemma. Radiol. Med. 2021, 126, 774–785. [Google Scholar] [CrossRef]
- Argalia, G.; Tarantino, G.; Ventura, C.; Campioni, D.; Tagliati, C.; Guardati, P.; Kostandini, A.; Marzioni, M.; Giuseppetti, G.M.; Giovagnoni, A. Shear wave elastography and transient elastography in HCV patients after direct-acting antivirals. Radiol. Med. 2021, 126, 894–899. [Google Scholar] [CrossRef]
- Granata, V.; Petrillo, M.; Fusco, R.; Setola, S.V.; De Lutio Di Castelguidone, E.; Catalano, O.; Piccirillo, M.; Albino, V.; Izzo, F.; Petrillo, A. Surveillance of HCC Patients after Liver RFA: Role of MRI with Hepatospecific Contrast versus Three-Phase CT Scan—Experience of High Volume Oncologic Institute. Gastroenterol. Res. Pract. 2013, 2013, 469097. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Gaibazzi, N.; Tuttolomondo, D.; Fusco, S.; La Mura, V.; Peyvandi, F.; Aliberti, S.; Blasi, F.; Cozzi, D.; Carrafiello, G.; et al. Deep vein thrombosis in COVID-19 patients in general wards: Prevalence and association with clinical and laboratory variables. Radiol. Med. 2021, 126, 722–728. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Chen, D.; Zhou, C.; Luo, M.; Huang, W.; Huang, J.; Huang, J.; Chen, Y. Percutaneous endovenous intervention without vena cava filter for acute proximal deep vein thrombosis secondary to iliac vein compression syndrome: Preliminary outcomes. Radiol. Med. 2021, 126, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Castellana, M.; Virili, C.; Havre, R.F.; Bini, F.; Marinozzi, F.; D’Ambrosio, F.; Giorgino, F.; Giovanella, L.; Prosch, H.; et al. Performance of contrast-enhanced ultrasound (CEUS) in assessing thyroid nodules: A systematic review and meta-analysis using histological standard of reference. Radiol. Med. 2020, 125, 406–415. [Google Scholar] [CrossRef]
- Zhou, M.Y.; Bui, N.Q.; Charville, G.W.; Ghanouni, P.; Ganjoo, K.N. Current management and recent progress in desmoid tumors. Cancer Treat. Res. Commun. 2022, 31, 100562. [Google Scholar] [CrossRef]
- Bilreiro, C.; Soler, J.C.; Ayuso, J.R.; Caseiro-Alves, F.; Ayuso, C. Diagnostic value of morphological enhancement patterns in the hepatobiliary phase of gadoxetic acid-enhanced MRI to distinguish focal nodular hyperplasia from hepatocellular adenoma. Radiol. Med. 2021, 126, 1379–1387. [Google Scholar] [CrossRef]
- Zheng, Q.; Liu, B.; Zhou, Y.; Liu, D. Prognostic factors of abdominal desmoid tumor fibromatosis after surgery: A retrospective study of 52 patients. Asian J. Surg. 2022; ahead of print. [Google Scholar] [CrossRef]
- Minami, Y.; Matsumoto, S.; Ae, K.; Tanizawa, T.; Hayakawa, K.; Saito, M.; Kurosawa, N. The Clinical Features of Multicentric Extra-abdominal Desmoid Tumors. Cancer Diagn. Progn. 2021, 1, 339–343. [Google Scholar] [CrossRef]
- Qin, H.; Que, Q.; Lin, P.; Li, X.; Wang, X.-R.; He, Y.; Chen, J.-Q.; Yang, H. Magnetic resonance imaging (MRI) radiomics of papillary thyroid cancer (PTC): A comparison of predictive performance of multiple classifiers modeling to identify cervical lymph node metastases before surgery. Radiol. Med. 2021, 126, 1312–1327. [Google Scholar] [CrossRef]
- Tsuchihashi, K.; Yamaguchi, K.; Taguchi, R.; Kohashi, K.; Ijichi, K.; Okumura, Y.; Nakano, M.; Ohno, A.; Hioki, T.; Shimokawa, H.; et al. Spontaneous Regression of Metachronous Intra-Abdominal Desmoid Tumor in a Patient with Familial Adenomatous Polyposis. Case Rep. Oncol. 2022, 15, 71–77. [Google Scholar] [CrossRef]
- Negroni, D.; Cassarà, A.; Trisoglio, A.; Soligo, E.; Berardo, S.; Carriero, A.; Stecco, A. Learning curves in radiological reporting of whole-body MRI in plasma cell disease: A retrospective study. Radiol. Med. 2021, 126, 1451–1459. [Google Scholar] [CrossRef]
- Schoelles, K.; Federmann, Y.; Kurz, P.; Selt, F.; Schupp, W.; Lagrèze, W.; Lang, S.; Auw-Haedrich, C. Aggressive fibromatosis in a child: A diagnostic challenge. Pathology, 2022; ahead of print. [Google Scholar] [CrossRef]
- Penel, N.; Bonvalot, S.; Bimbai, A.-M.; Meurgey, A.; Le Loarer, F.; Salas, S.; Piperno-Neumann, S.; Chevreau, C.; Boudou-Rouquette, P.; Dubray-Longeras, P.; et al. Lack of prognostic value of CTNNB1 mutation profile in desmoid-type fibromatosis. Clin. Cancer Res. 2022; ahead of print. [Google Scholar] [CrossRef]
- Damiani, G.; Mikhael, R.; Tzanis, D.; El Zein, S.; Bonvalot, S. Desmoid Tumors Arising on the Mesenteric Surgical Scar of Abdominal Sarcomas. Cureus 2022, 14, e21727. [Google Scholar] [CrossRef]
- Colombo, C.; Fiore, M.; Grignani, G.; Tolomeo, F.; Merlini, A.; Palassini, E.; Collini, P.; Stacchiotti, S.; Casali, P.G.; Perrone, F.; et al. A prospective observational study of Active surveillance in primary desmoid fibromatosis. Clin. Cancer Res. 2022; ahead of print. [Google Scholar] [CrossRef]
- Mastoraki, A.; Schizas, D.; Vassiliu, S.; Saliaris, K.; Giagkos, G.-C.; Theochari, M.; Vergadis, C.; Tolia, M.; Vassiliu, P.; Felekouras, E. Evaluation of diagnostic algorithm and therapeutic interventions for intra-abdominal desmoid tumors. Surg. Oncol. 2022, 41, 101724. [Google Scholar] [CrossRef] [PubMed]
- Coskun, H.S.; Erdogan, F.; Cinka, H.; Dabak, N. Extra-abdominal desmoid fibromatosis: An evaluation of clinical factors affecting local recurrence rates. Acta Orthop. Traumatol. Turc. 2021, 55, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Schlag, H.; Neuhoff, J.; Castein, J.; Hoffmann, C.; Kandziora, F. Sporadic desmoid fibromatosis of the neck after dorsal spondylodesis of the cervical spine. Surg. Neurol. Int. 2022, 13, 64. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, N.; Kopel, J.; Awasthi, S.; Cordero, J. Case report of recurrent fibromatosis with laryngeal involvement: Treatment based on network analyses of NGS data. Mol. Clin. Oncol. 2022, 16, 73. [Google Scholar] [CrossRef]
- Nosé, V.; Lazar, A.J. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Familial Tumor Syndromes. Head Neck Pathol. 2022, 16, 143–157. [Google Scholar] [CrossRef]
- Bruno, F.; Arrigoni, F.; Mariani, S.; Splendiani, A.; Di Cesare, E.; Masciocchi, C.; Barile, A. Advanced magnetic resonance imaging (MRI) of soft tissue tumors: Techniques and applications. Radiol. Med. 2019, 124, 243–252. [Google Scholar] [CrossRef]
- Liu, D.; Perera, W.; Schlicht, S.; Choong, P.; Slavin, J.; Pianta, M. Musculoskeletal desmoid tumours: Diagnostic imaging appearances. J. Med. Imaging Radiat. Oncol. 2015, 59, 461–467. [Google Scholar] [CrossRef]
- Liu, D.; Perera, W.; Schlicht, S.; Choong, P.; Slavin, J.; Pianta, M. Musculoskeletal desmoid tumours: Pre- and post-treatment radiological appearances. J. Med Imaging Radiat. Oncol. 2015, 59, 480–485. [Google Scholar] [CrossRef] [Green Version]
- McDonald, E.S.; Yi, E.S.; Wenger, D.E. Best cases from the AFIP: Extraabdominal desmoid-type fibromatosis. Radiographics 2008, 28, 901–906. [Google Scholar] [CrossRef] [Green Version]
- Eastley, N.; McCulloch, T.; Esler, C.; Hennig, I.; Fairbairn, J.; Gronchi, A.; Ashford, R. Extra-abdominal desmoid fibromatosis: A review of management, current guidance and unanswered questions. Eur. J. Surg. Oncol. (EJSO) 2016, 42, 1071–1083. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, G.; Cifaratti, A.; Scalzo, G.; Magarelli, N. Imaging of superficial and deep fibromatosis. Radiol. Med. 2009, 114, 1292–1307. [Google Scholar] [CrossRef] [PubMed]
- Chianca, V.; Albano, D.; Messina, C.; Vincenzo, G.; Rizzo, S.; Del Grande, F.; Sconfienza, L.M. An update in musculoskeletal tumors: From quantitative imaging to radiomics. Radiol. Med. 2021, 126, 1095–1105. [Google Scholar] [CrossRef]
- Cellina, M.; Gibelli, D.; Martinenghi, C.; Giardini, D.; Soresina, M.; Menozzi, A.; Oliva, G.; Carrafiello, G. Non-contrast magnetic resonance lymphography (NCMRL) in cancer-related secondary lymphedema: Acquisition technique and imaging findings. Radiol. Med. 2021, 126, 1477–1486. [Google Scholar] [CrossRef] [PubMed]
- Brillantino, A.; Iacobellis, F.; Reginelli, A.; Renzi, A.; Grassi, R. Three-dimensional endoanal ultrasound should be considered as first-line diagnostic tool in the preoperative work-up for perianal fistulas. Radiol. Med. 2020, 125, 155–156. [Google Scholar] [CrossRef] [PubMed]
- Nathenson, M.J.; Hu, J.; Ratan, R.; Somaiah, N.; Hsu, R.; DeMaria, P.J.; Catoe, H.W.; Pang, A.; Subhawong, T.K.; Amini, B.; et al. Systemic chemotherapies retain anti-tumor activity in desmoid tumors independent of specific mutations in CTNNB1 or APC: A multi-institutional retrospective study. Clin. Cancer Res. 2022; ahead of print. [Google Scholar]
- Cildag, M.B.; Gok, M.; Abdullayev, O. Pre-procedural shear wave elastography on prediction of hemorrhage after percutaneous real-time ultrasound-guided renal biopsy. Radiol. Med. 2020, 125, 784–789. [Google Scholar] [CrossRef] [PubMed]
- Di Serafino, M.; Notaro, M.; Rea, G.; Iacobellis, F.; Delli Paoli, V.; Acampora, C.; Vallone, G. The lung ultrasound: Facts or artifacts? In the era of COVID-19 outbreak. Radiol. Med. 2020, 125, 738–753. [Google Scholar] [CrossRef] [PubMed]
- Tsukamoto, S.; Takahama, T.; Mavrogenis, A.F.; Tanaka, Y.; Errani, C. Clinical outcomes of medical treatments for progressive desmoid tumors following active surveillance: A systematic review. Musculoskelet. Surg. 2022; ahead of print. [Google Scholar] [CrossRef]
- Laurelli, G.; Falcone, F.; Gallo, M.S.; Scala, F.; Losito, S.; Granata, V.; Cascella, M.; Greggi, S. Long-Term Oncologic and Reproductive Outcomes in Young Women with Early Endometrial Cancer Conservatively Treated: A Prospective Study and Literature Update. Int. J. Gynecol. Cancer 2016, 26, 1650–1657. [Google Scholar] [CrossRef]
- Johns, M.S.; Merritt, W.T.; Rhodes, L.; Ford, C.N.; Thompson, M.; Lee, W.M.; Sheldon, Y.; Petrelli, N.J.; Tiesi, G.J. A cost analysis of sorafenib for desmoid tumors. J. Oncol. Pharm. Pr. 2022; ahead of print. [Google Scholar] [CrossRef]
- Wang, J.; Li, H.; Wang, H.; Li, Q.; Bai, X.; Lv, H.; Nie, C.; Chen, B.; Xu, W.; Tu, S.; et al. Combination of Anlotinib and Celecoxib for the Treatment of Abdominal Desmoid Tumor: A Case Report and Literature Review. Front. Oncol. 2022, 11, 830672. [Google Scholar] [CrossRef]
- Frongillo, E.; Gaudioso, G.; Feragalli, B. Ultrasound and interstitial lung disease: Use and limitations. Radiol. Med. 2020, 125, 66–67. [Google Scholar] [CrossRef]
- Hu, S.; Zhang, H.; Sun, Z.; Ge, Y.; Li, J.; Yu, C.; Deng, Z.; Dou, W.; Wang, X. Preoperative assessment of extrathyroidal extension of papillary thyroid carcinomas by ultrasound and magnetic resonance imaging: A comparative study. Radiol. Med. 2020, 125, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Bonvalot, S.; Minard, V.; Orbach, D.; Gouin, F.; Corradini, N.; Brahmi, M.; Marec-Bérard, P.; Briand, S.; Gaspar, N.; et al. French Sarcoma Group proposals for management of sarcoma patients during the COVID-19 outbreak. Ann. Oncol. 2020, 31, 965–966. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bonifacini, C.; Zannoni, S.; Bernareggi, S.; Messina, C.; Galia, M.; Sconfienza, L.M. Plantar forefoot pain: Ultrasound findings before and after treatment with custom-made foot orthoses. Radiol. Med. 2021, 126, 963–970. [Google Scholar] [CrossRef] [PubMed]
- Mo, S.; Chen, J.; Zhang, R.; Yang, C.; Wang, T.; Chen, L.; Chen, W. High-Intensity Focused Ultrasound Ablation for Postoperative Recurrent Desmoid Tumors: Preliminary Results. Ultrasound Med. Biol. 2022, 48, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.; Lee, J.H.; Lee, Y.H.; Lee, J.; Ahn, J.-H.; Kim, S.H.; Kim, S.H.; Kim, T.I.; Yun, K.-H.; Park, Y.S.; et al. Whole-genome and Transcriptome Sequencing Identified NOTCH2 and HES1 as Potential Markers of Response to Imatinib in Desmoid Tumor (Aggressive Fibromatosis): A Phase II Trial Study. Cancer Res. Treat. 2022; ahead of print. [Google Scholar] [CrossRef]
- Li, X.; Zhang, H.; Chen, L.-Q. Robot-assisted thoracoscopic transdiaphragmatic resection of an infradiaphragmatic desmoid-type fibromatosis. Asian J. Surg. 2022, 45, 976–977. [Google Scholar] [CrossRef]
- Vora, B.M.K.; Munk, P.L.; Somasundaram, N.; Ouellette, H.A.; Mallinson, P.I.; Sheikh, A.; Kadir, H.A.; Tan, T.J.; Yan, Y.Y. Cryotherapy in extra-abdominal desmoid tumors: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0261657. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Setola, S.V.; Piccirillo, M.; Leongito, M.; Palaia, R.; Granata, F.; Lastoria, S.; Izzo, F.; Petrillo, A. Early radiological assessment of locally advanced pancreatic cancer treated with electrochemotherapy. World J. Gastroenterol. 2017, 23, 4767–4778. [Google Scholar] [CrossRef]
- Ossola, C.; Curti, M.; Calvi, M.; Tack, S.; Mazzoni, S.; Genesio, L.; Venturini, M.; Genovese, E.A. Role of ultrasound and magnetic resonance imaging in the prognosis and classification of muscle injuries in professional football players: Correlation between imaging and return to sport time. Radiol. Med. 2021, 126, 1460–1467. [Google Scholar] [CrossRef]
- Emori, M.; Matsumoto, Y.; Murahashi, Y.; Yoshida, M.; Nishida, Y. Efficacy and safety of cyclooxygenase 2 inhibitors for desmoid tumor management: A systematic review. Nagoya J. Med. Sci. 2021, 83, 673–681. [Google Scholar] [CrossRef]
- Ceravolo, I.; Barchetti, G.; Biraschi, F.; Gerace, C.; Pampana, E.; Pingi, A.; Stasolla, A. Early stage glioblastoma: Retrospective multicentric analysis of clinical and radiological features. Radiol. Med. 2021, 126, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- Refai, M.; Andolfi, M.; Barbisan, F.; Roncon, A.; Guiducci, G.M.; Xiumè, F.; Paci, E. Computed tomography-guided microcoil placement for localizing small pulmonary nodules before uniportal video-assisted thoracoscopic resection. Radiol. Med. 2020, 125, 24–30. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, M.; Puglisi, S.; D’Amuri, F.; Gentili, F.; Paladini, I.; Carrafiello, G.; Maestroni, U.; Del Rio, P.; Ziglioli, F.; Pagnini, F. CT-guided percutaneous drainage of abdominopelvic collections: A pictorial essay. Radiol. Med. 2021, 126, 1561–1570. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Liu, H.; Ding, X.; Wu, J.; Tian, Z.; Mao, T. Familial adenomatous polyposis associated with desmoid tumors presenting with abdominal abscess: A case report and literature review. Medicine 2021, 100, e27897. [Google Scholar] [CrossRef]
- Yang, T.; Liu, H.; Liao, Z.; Zhang, C.; Xiang, L.; Yang, J. Postoperative Adjuvant Radiotherapy Can Delay the Recurrence of Desmoid Tumors After R0 Resection in Certain Subgroups. Front. Surg. 2021, 8, 697793. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Li, H.; Gao, J.; Li, J.; Li, M.; Zhou, Z.; Peng, Y. Performance evaluation of a deep learning image reconstruction (DLIR) algorithm in “double low” chest CTA in children: A feasibility study. Radiol. Med. 2021, 126, 1181–1188. [Google Scholar] [CrossRef] [PubMed]
- Schicchi, N.; Fogante, M.; Palumbo, P.; Agliata, G.; Esposto Pirani, P.; Di Cesare, E.; Giovagnoni, A. The sub-millisievert era in CTCA: The technical basis of the new radiation dose approach. Radiol. Med. 2020, 125, 1024–1039. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, P.; Cannizzaro, E.; Bruno, F.; Schicchi, N.; Fogante, M.; Agostini, A.; De Donato, M.C.; De Cataldo, C.; Giovagnoni, A.; Barile, A.; et al. Coronary artery disease (CAD) extension-derived risk strati-fication for asymptomatic diabetic patients: Usefulness of low-dose coronary computed tomography angiography (CCTA) in detecting high-risk profile patients. Radiol. Med. 2020, 125, 1249–1259. [Google Scholar] [CrossRef]
- Cellini, F.; Di Franco, R.; Manfrida, S.; Borzillo, V.; Maranzano, E.; Pergolizzi, S.; Morganti, A.G.; Fusco, V.; Deodato, F.; Santarelli, M.; et al. Palliative radiotherapy indications during the COVID-19 pandemic and in future complex logistic settings: The NORMALITY model. Radiol. Med. 2021, 126, 1619–1656. [Google Scholar] [CrossRef]
- De Felice, F.; Boldrini, L.; Greco, C.; Nardone, V.; Salvestrini, V.; Desideri, I. ESTRO vision 2030: The young Italian Association of Radiotherapy and Clinical Oncology (yAIRO) commitment statement. Radiol. Med. 2021, 126, 1374–1376. [Google Scholar] [CrossRef]
- Bellardita, L.; Colciago, R.R.; Frasca, S.; De Santis, M.C.; Gay, S.; Palorini, F.; La Rocca, E.; Valdagni, R.; Rancati, T.; Lozza, L. Breast cancer patient perspective on opportunities and challenges of a genetic test aimed to predict radio-induced side effects before treatment: Analysis of the Italian branch of the REQUITE project. Radiol. Med. 2021, 126, 1366–1373. [Google Scholar] [CrossRef]
- Braschi-Amirfarzan, M.; Keraliya, A.R.; Krajewski, K.M.; Tirumani, S.H.; Shinagare, A.B.; Hornick, J.; Baldini, E.H.; George, S.; Ramaiya, N.H.; Jagannathan, J.P. Role of Imaging in Management of Desmoid-type Fibromatosis: A Primer for Radiologists. RadioGraphics 2016, 36, 767–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiarilli, M.G.; Pizzi, A.D.; Mastrodicasa, D.; Febo, M.P.; Cardinali, B.; Consorte, B.; Cifaratti, A.; Panara, V.; Caulo, M.; Cannataro, G. Bone marrow magnetic resonance imaging: Physiologic and pathologic findings that radiologist should know. Radiol. Med. 2021, 126, 264–276. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Cortese, M.C.; Duarte, A.; Messina, C.; Gitto, S.; Vicentin, I.; Coppola, A.; Galia, M.; Sconfienza, L.M. Predictive role of ankle MRI for tendon graft choice and surgical reconstruction. Radiol. Med. 2020, 125, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Cobianchi Bellisari, F.; De Marino, L.; Arrigoni, F.; Mariani, S.; Bruno, F.; Palumbo, P.; De Cataldo, C.; Sgalambro, F.; Catallo, N.; Zugaro, L.; et al. T2-mapping MRI evaluation of patellofemoral cartilage in patients submitted to intra-articular platelet-rich plasma (PRP) injections. Radiol. Med. 2021, 126, 1085–1094. [Google Scholar] [CrossRef] [PubMed]
- Ricatti, G.; Veronese, N.; Gangai, I.; Paparella, M.; Testini, V.; Guglielmi, G. Hoffa’s fat pad thickness: A measurement method with sagittal MRI sequences. Radiol. Med. 2021, 126, 886–893. [Google Scholar] [CrossRef]
- Zappia, M.; Sconfienza, L.M.; Guarino, S.; Tumminello, M.; Iannella, G.; Mariani, P.P. Meniscal ramp lesions: Diagnostic performance of MRI with arthroscopy as reference standard. Radiol. Med. 2021, 126, 1106–1116. [Google Scholar] [CrossRef]
- Berardo, S.; Sukhovei, L.; Andorno, S.; Carriero, A.; Stecco, A. Quantitative bone marrow magnetic resonance imaging through apparent diffusion coefficient and fat fraction in multiple myeloma patients. Radiol. Med. 2021, 126, 445–452. [Google Scholar] [CrossRef]
- Orsatti, G.; Zucchetta, P.; Varotto, A.; Crimì, F.; Weber, M.; Cecchin, D.; Bisogno, G.; Spimpolo, A.; Giraudo, C.; Stramare, R. Volumetric histograms-based analysis of apparent diffusion coefficients and standard uptake values for the assessment of pediatric sarcoma at staging: Preliminary results of a PET/MRI study. Radiol. Med. 2021, 126, 878–885. [Google Scholar] [CrossRef]
- Lian, S.; Zhang, C.; Chi, J.; Huang, Y.; Shi, F.; Xie, C. Differentiation between nasopharyngeal carcinoma and lymphoma at the primary site using whole-tumor histogram analysis of apparent diffusion coefficient maps. Radiol. Med. 2020, 125, 647–653. [Google Scholar] [CrossRef]
- Pietragalla, M.; Nardi, C.; Bonasera, L.; Mungai, F.; Taverna, C.; Novelli, L.; De Renzis, A.G.D.; Calistri, L.; Tomei, M.; Occhipinti, M.; et al. The role of diffusion-weighted and dynamic contrast enhancement perfusion-weighted imaging in the evaluation of salivary glands neoplasms. Radiol. Med. 2020, 125, 851–863. [Google Scholar] [CrossRef]
- Momeni, M.; Asadzadeh, M.; Mowla, K.; Hanafi, M.G.; Gharibvand, M.M.; Sahraeizadeh, A. Sensitivity and specificity assessment of DWI and ADC for the diagnosis of osteoporosis in postmenopausal patients. Radiol. Med. 2020, 125, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Fornell-Perez, R.; Vivas-Escalona, V.; Aranda-Sanchez, J.; Gonzalez-Dominguez, M.C.; Rubio-Garcia, J.; Aleman-Flores, P.; Loro-Ferrer, J.F. Primary and post-chemoradiotherapy MRI detection of extramural venous invasion in rectal cancer: The role of diffusion-weighted imaging. Radiol. Med. 2020, 125, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Song, J.; Ma, Z.; Chen, T. Combined dynamic contrast-enhanced magnetic resonance imaging and diffusion-weighted imaging to predict neoadjuvant chemotherapy effect in FIGO stage IB2-IIA2 cervical cancers. Radiol. Med. 2020, 125, 1233–1242. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, C.; Dell’Aversana, F.; Fusco, R.; Grazzini, G.; Chiti, G.; Simonetti, I.; Bruno, F.; Palumbo, P.; Pierpaoli, L.; Valeri, T.; et al. Combined Hepatocellular-Cholangiocarcinoma: What the Multidisciplinary Team Should Know. Diagnostics 2022, 12, 890. [Google Scholar] [CrossRef] [PubMed]
- Bruno, F.; Granata, V.; Bellisari, F.C.; Sgalambro, F.; Tommasino, E.; Palumbo, P.; Arrigoni, F.; Cozzi, D.; Grassi, F.; Brunese, M.C.; et al. Advanced Magnetic Resonance Imaging (MRI) Techniques: Technical Principles and Applications in Nanomedicine. Cancers 2022, 14, 1626. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Setola, S.V.; De Muzio, F.; Aversana, F.D.; Cutolo, C.; Faggioni, L.; Miele, V.; Izzo, F.; Petrillo, A. CT-Based Radiomics Analysis to Predict Histopathological Outcomes Following Liver Resection in Colorectal Liver Metastases. Cancers 2022, 14, 1648. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Belli, A.; Borzillo, V.; Palumbo, P.; Bruno, F.; Grassi, R.; Ottaiano, A.; Nasti, G.; Pilone, V.; et al. Conventional, functional and radiomics assessment for intrahepatic cholangiocarcinoma. Infect. Agents Cancer 2022, 17, 13. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Bicchierai, G.; Cozzi, D.; Grazzini, G.; Danti, G.; De Muzio, F.; Maggialetti, N.; Smorchkova, O.; D’Elia, M.; et al. Diagnostic protocols in oncology: Workup and treatment planning. Part 1: The optimitation of CT protocol. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 6972–6994. [Google Scholar] [CrossRef]
- Minutoli, F.; Pergolizzi, S.; Blandino, A.; Mormina, E.; Amato, E.; Gaeta, M. Effect of granulocyte colony-stimulating factor on bone marrow: Evaluation by intravoxel incoherent motion and dynamic contrast-enhanced magnetic resonance imaging. Radiol. Med. 2020, 125, 280–287. [Google Scholar] [CrossRef]
- Sun, N.N.; Ge, X.L.; Liu, X.S.; Xu, L.L. Histogram analysis of DCE-MRI for chemoradiotherapy response evaluation in locally advanced esophageal squamous cell carcinoma. Radiol. Med. 2020, 125, 165–176. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Setola, S.V.; Castelguidone, E.D.L.D.; Camera, L.; Tafuto, S.; Avallone, A.; Belli, A.; Incollingo, P.; Palaia, R.; et al. The multidisciplinary team for gastroenteropancreatic neuroendocrine tumours: The radiologist’s challenge. Radiol. Oncol. 2019, 53, 373–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halefoglu, A.M.; Ozagari, A.A. Tumor grade estımatıon of clear cell and papıllary renal cell carcınomas usıng contrast-enhanced MDCT and FSE T2 weıghted MR ımagıng: Radıology-pathology correlatıon. Radiol. Med. 2021, 126, 1139–1148. [Google Scholar] [CrossRef] [PubMed]
- Treitl, K.M.; Ricke, J.; Baur-Melnyk, A. Whole-body magnetic resonance imaging (WBMRI) versus whole-body computed tomography (WBCT) for myeloma imaging and staging. Skelet. Radiol. 2022, 51, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Tsili, A.C.; Andriotis, E.; Gkeli, M.G.; Krokidis, M.; Stasinopoulou, M.; Varkarakis, I.M.; Moulopoulos, L.-A. The role of imaging in the management of renal masses. Eur. J. Radiol. 2021, 141, 109777. [Google Scholar] [CrossRef]
- Assadsangabi, R.; Babaei, R.; Songco, C.; Ivanovic, V.; Bobinski, M.; Chen, Y.J.; Nabavizadeh, S.A. Multimodality oncologic evaluation of superficial neck and facial lymph nodes. Radiol. Med. 2021, 126, 1074–1084. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; Maio, F.; Avallone, A.; Nasti, G.; Palaia, R.; Albino, V.; Grassi, R.; Izzo, F.; Petrillo, A. Qualitative assessment of EOB-GD-DTPA and Gd-BT-DO3A MR contrast studies in HCC patients and colorectal liver metastases. Infect. Agents Cancer 2019, 14, 40. [Google Scholar] [CrossRef]
- Agarwal, M.; van der Pol, C.B.; Patlas, M.N.; Udare, A.; Chung, A.D.; Rubino, J. Optimizing the radiologist work environment: Actionable tips to improve workplace satisfaction, efficiency, and minimize burnout. Radiol. Med. 2021, 126, 1255–1257. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Castelguidone, E.D.L.D.; Avallone, A.; Palaia, R.; Delrio, P.; Tatangelo, F.; Botti, G.; Grassi, R.; Izzo, F.; et al. Diagnostic performance of gadoxetic acid–enhanced liver MRI versus multidetector CT in the assessment of colorectal liver metastases compared to hepatic resection. BMC Gastroenterol. 2019, 19, 129. [Google Scholar] [CrossRef] [Green Version]
- Celletti, I.; Fresilli, D.; De Vito, C.; Bononi, M.; Cardaccio, S.; Cozzolino, A.; Durante, C.; Grani, G.; Grimaldi, G.; Isidori, A.M.; et al. TIRADS, SRE and SWE in INDETERMINATE thyroid nodule characterization: Which has better diagnostic performance? Radiol. Med. 2021, 126, 1189–1200. [Google Scholar] [CrossRef]
- Granata, V.; Fusco, R.; Avallone, A.; Catalano, O.; Piccirillo, M.; Palaia, R.; Nasti, G.; Petrillo, A.; Izzo, F. A radiologist’s point of view in the presurgical and intraoperative setting of colorectal liver metastases. Future Oncol. 2018, 14, 2189–2206. [Google Scholar] [CrossRef]
- Spoerl, S.; Spoerl, S.; Reil, S.; Gerken, M.; Ludwig, N.; Taxis, J.; Fischer, R.; Ettl, T.; Reichert, T.E.; Spanier, G. Prognostic Value of Perineural Invasion on Survival and Recurrence in Oral Squamous Cell Carcinoma. Diagnostics 2022, 12, 1062. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Liu, S.; Zhao, Q.; Cui, Y.; Chen, J.; Wang, S. Using the Indocyanine Green (ICG) Lymphography to Screen Breast Cancer Patients at High Risk for Lymphedema. Diagnostics 2022, 12, 983. [Google Scholar] [CrossRef] [PubMed]
- Fukui, K.; Masumoto, N.; Yokoyama, E.; Kanou, A.; Yokozaki, M.; Sasada, S.; Emi, A.; Kadoya, T.; Arihiro, K.; Okada, M. Ultrasonography Combined with Contrast-enhanced Ultrasonography Can Predict Lymphocyte-predominant Breast Cancer. Cancer Diagn. Progn. 2021, 1, 309–316. [Google Scholar] [CrossRef]
- Wei, T.; Lu, M.; Li, J.; Hu, Z.; Li, T.; Cheng, X.; Wang, L.; Pu, W. Comparative study on efficacy and safety of ultrasound guided transoral and transcutaneous core needle biopsy in patients with oral masses. BMC Med. Imaging 2022, 22, 65. [Google Scholar] [CrossRef]
- Spagnuolo, G.M.; Tierney, H.T.; Laver, N.M.; Eldeiry, L.S. A Retrospective Study of Clinicopathologic Outcomes of Nodules with Hürthle Cell Cytology and the Thyroid Nodule App (TNAPP) Ultrasound Recommendations. Endocr. Pract. 2022, 28, 593–598. [Google Scholar] [CrossRef]
- Mital, T.; Kamal, M.; Kumar, M.; Kumar, R.; Bhatia, P.; Singariya, G. Comparison of landmark and real-time ultrasound-guided epidural catheter placement in the pediatric population: A prospective randomized comparative trial. Anesth. Pain Med. 2021, 16, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Sparchez, Z.; Mocan, T.; Craciun, R.; Sparchez, M.; Nolsøe, C. Contrast enhancement for ultrasound-guided interventions: When to use it and what to expect? Ultrasonography 2022, 41, 263–278. [Google Scholar] [CrossRef] [PubMed]
- Povoski, S.P.; Jimenez, R.E. Fibromatosis (desmoid tumor) of the breast mimicking a case of ipsilateral metachronous breast cancer. World J. Surg. Oncol. 2006, 4, 57. [Google Scholar] [CrossRef] [Green Version]
- Escobar, C.; Munker, R.; Thomas, J.O.; Li, B.D.; Burton, G.V. Update on desmoid tumors. Ann. Oncol. 2012, 23, 562–569. [Google Scholar] [CrossRef]
- Mekhail, F.G.; Montgomery, J.R.; Spicer, P.J. Imaging findings of a biopsy-proven desmoid tumor of the axilla in a young female. Radiol. Case Rep. 2022, 17, 1050–1053. [Google Scholar] [CrossRef]
- Wang, L.; Xu, D.; Chen, L.; Huang, P. Percutaneous ultrasound-guided radiofrequency ablation for giant desmoid tumors of the intra-abdominal cavity in a patient with Gardner syndrome. J. Cancer Res. Ther. 2021, 17, 1286–1288. [Google Scholar] [CrossRef]
- Izzo, F.; Palaia, R.; Albino, V.; Amore, A.; Di Giacomo, R.; Piccirillo, M.; Leongito, M.; Nasto, A.; Granata, V.; Petrillo, A.; et al. Hepatocellular carcinoma and liver metastases: Clinical data on a new dual-lumen catheter kit for surgical sealant infusion to prevent perihepatic bleeding and dissemination of cancer cells following biopsy and loco-regional treatments. Infect. Agents Cancer 2015, 10, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granata, V.; Fusco, R.; Piccirillo, M.; Palaia, R.; Petrillo, A.; Lastoria, S.; Izzo, F. Electrochemotherapy in locally advanced pancreatic cancer: Preliminary results. Int. J. Surg. 2015, 18, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Barile, A. Some thoughts and greetings from the new Editor-in-Chief. Radiol. Med. 2021, 126, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, F.; Cannavale, A.; Chisci, E.; Citone, M.; Falcone, G.M.; Michelagnoli, S.; Miele, V. Direct percutaneous embolization of aneurysm sac: A safe and effective procedure to treat post-EVAR type II endoleaks. Radiol. Med. 2021, 126, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Aberle, S.; Kenkel, D.; Becker, A.S.; Puippe, G.; Burger, I.; Schaefer, N.; Pfammatter, T. Outpatient Yttrium-90 microsphere radioembolization: Assessment of radiation safety and quantification of post-treatment adverse events causing hospitalization. Radiol. Med. 2020, 125, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Kasper, B.; Baumgarten, C.; Garcia, J.; Bonvalot, S.; Haas, R.; Haller, F.; Hohenberger, P.; Penel, N.; Messiou, C.; van der Graaf, W.T.; et al. An update on the management of sporadic desmoid-type fibromatosis: A European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG). Ann. Oncol. 2017, 28, 2399–2408. [Google Scholar] [CrossRef] [PubMed]
- Barrow, E.; Newton, K.; Rajashanker, B.; Lee, S.; Evans, G.; Hill, J. Successful radiofrequency ablation of an anterior abdominal wall desmoid in familial adenomatous polyposis. Color. Dis. 2013, 15, e160–e163. [Google Scholar] [CrossRef] [PubMed]
- Cobianchi, L.; Ravetta, V.; Viera, F.T.; Filisetti, C.; Siri, B.; Segalini, E.; Dionigi, P. The challenge of extraabdominal desmoid tumour management in patients with Gardner’s syndrome: Radiofrequency ablation, a promising option. World J. Surg. Oncol. 2014, 12, 361. [Google Scholar] [CrossRef] [Green Version]
- Ilaslan, H.; Schils, J.; Joyce, M.; Marks, K.; Sundaram, M. Radiofrequency ablation: Another treatment option for local control of desmoid tumors. Skelet. Radiol. 2010, 39, 169–173. [Google Scholar] [CrossRef]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.; Belli, A.; Piccirillo, M.; Pradella, S.; Giordano, M.; Cappabianca, S.; Brunese, L.; et al. Abbreviated MRI Protocol for the Assessment of Ablated Area in HCC Patients. Int. J. Environ. Res. Public Health 2021, 18, 3598. [Google Scholar] [CrossRef]
- Masjedi, H.; Zare, M.H.; Siahpoush, N.K.; Razavi-Ratki, S.K.; Alavi, F.; Shabani, M. European trends in radiology: Investigating factors affecting the number of examinations and the effective dose. Radiol. Med. 2020, 125, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Shinzawa, H.; Wakabayashi, H.; Aoki, M.; Sugahara, K.; Iwaba, A.; Haga, H.; Miyano, S.; Terui, Y.; Mitsuhashi, H.; et al. Value of Laparoscopic Microwave Coagulation Therapy for Hepatocellular Carcinoma in Relation to Tumor Size and Location. Endoscopy 2000, 32, 598–603. [Google Scholar] [CrossRef] [PubMed]
- Simo, K.A.; Sereika, S.E.; Newton, K.N.; Gerber, D.A. Laparoscopic-assisted microwave ablation for hepatocellular carcinoma: Safety and efficacy in comparison with radiofrequency ablation. J. Surg. Oncol. 2011, 104, 822–829. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Cortis, K.; Yusuf, G.T.; Gregory, S.; Lewis, D.; Kane, P.; Peddu, P. Complications from percutaneous microwave ablation of liver tumours: A pictorial review. Br. J. Radiol. 2019, 92, 20180864. [Google Scholar] [CrossRef]
- Valentino, M.; Liberatore, M.; Maghella, F.; De Soccio, V.; De Felice, C.; Messineo, D.; Drudi, F.M. Diagnostic imaging and CEUS findings in a rare case of Desmoid-type fibromatosis. A case report. J. Ultrasound 2018, 21, 253–257. [Google Scholar] [CrossRef] [Green Version]
- Xu, W.; Lv, K.; Huang, Y.; Wen, Q.; Pan, M.; Huang, P. Features of ultrasound and contrast enhanced ultrasound in superficial desmoid-type fibromatosis: A series of 19 cases. Clin. Hemorheol. Microcirc. 2022, 80, 211–218. [Google Scholar] [CrossRef]
- Shi, Z.; Zhao, X.-M.; Jiang, J.-M.; Li, M.; Xie, L.-Z. Clinical and imaging features of desmoid tumors of the extremities. World J. Clin. Cases 2021, 9, 8710–8717. [Google Scholar] [CrossRef]
- Figueiredo, G.; O’Shea, A.; Neville, G.M.; Lee, S.I. Rare Mesenchymal Tumors of the Pelvis: Imaging and Pathologic Correlation. RadioGraphics 2022, 42, 143–158. [Google Scholar] [CrossRef]
- Lee, J.H.; Paeng, S.H.; Cho, H.J.; Kim, S.T.; Lee, W.H. Desmoid Fibromatosis in the Multifidus Muscle Misdiagnosed as Intramuscular Schwannoma by Incisional Biopsy: A Case Report. Korean J. Neurotrauma 2021, 17, 212. [Google Scholar] [CrossRef]
- Garcia-Ortega, D.; Martín-Tellez, K.; Cuellar-Hubbe, M.; Martínez-Said, H.; Álvarez-Cano, A.; Brener-Chaoul, M.; Alegría-Baños, J.; Martínez-Tlahuel, J. Desmoid-Type Fibromatosis. Cancers 2020, 12, 1851. [Google Scholar] [CrossRef] [PubMed]
- Young, J.R.; Sternbach, S.; Willinger, M.; Hutchinson, I.D.; Rosenbaum, A.J. The etiology, evaluation, and management of plantar fibromatosis. Orthop. Res. Rev. 2018, 11, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Sabharwal, S.; Ahlawat, S.; Levin, A.S.; Meyer, C.F.; Brooks, E.; Ligon, J.; Morris, C.D. Desmoid tumor mimics local recurrence of extremity sarcoma on MRI. J. Surg. Oncol. 2020, 121, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-S.; Zhu, H.C.; Xu, S.X.; Li, X.T.; Guan, Z.; Li, S. MRI T1 Contrast-Enhanced Signal Intensity Is a Prognostic Indicator of Imatinib Therapy in Desmoid-Type Fibromatosis. Front. Oncol. 2021, 11, 615986. [Google Scholar] [CrossRef]
- Rampado, O.; Depaoli, A.; Marchisio, F.; Gatti, M.; Racine, D.; Ruggeri, V.; Ruggirello, I.; Darvizeh, F.; Fonio, P.; Ropolo, R. Effects of different levels of CT iterative reconstruction on low-contrast detectability and radiation dose in patients of different sizes: An anthropomorphic phantom study. Radiol. Med. 2021, 126, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Shin, N.; Choi, J.A.; Choi, J.M.; Cho, E.S.; Kim, J.H.; Chung, J.J.; Yu, J.S. Sclerotic changes of cavernous hemangioma in the cirrhotic liver: Long-term follow-up using dynamic contrast-enhanced computed tomography. Radiol. Med. 2020, 125, 1225–1232. [Google Scholar] [CrossRef]
- Bottari, A.; Silipigni, S.; Carerj, M.L.; Cattafi, A.; Maimone, S.; Marino, M.A.; Mazziotti, S.; Pitrone, A.; Squadrito, G.; Ascenti, G. Dual-source dual-energy CT in the evaluation of hepatic fractional extracellular space in cirrhosis. Radiol. Med. 2020, 125, 7–14. [Google Scholar] [CrossRef]
- Agostini, A.; Borgheresi, A.; Mari, A.; Floridi, C.; Bruno, F.; Carotti, M.; Schicchi, N.; Barile, A.; Maggi, S.; Giovagnoni, A. Dual-energy CT: Theoretical principles and clinical applications. Radiol. Med. 2019, 124, 1281–1295. [Google Scholar] [CrossRef]
- Okamura, T.; Yamada, Y.; Yamada, M.; Yamazaki, A.; Shiraga, N.; Jinzaki, M. Image quality of virtual monochromatic images obtained using 320-detector row CT: A phantom study evaluating the effects of iterative reconstruction and body size. Eur. J. Radiol. 2017, 95, 212–221. [Google Scholar] [CrossRef]
- Megibow, A.J. Clinical abdominal dual-energy CT: 15 years later. Abdom. Radiol. 2020, 45, 1198–1201. [Google Scholar] [CrossRef]
- Mandel, J.E.; Kim, D.; Yarmohammadi, H.; Ziv, E.; Keohan, M.L.; D’Angelo, S.P.; Gounder, M.M.; Whiting, K.; Qin, L.-X.; Singer, S.; et al. Percutaneous Cryoablation Provides Disease Control for Extra-Abdominal Desmoid-Type Fibromatosis Comparable with Surgical Resection. Ann. Surg. Oncol. 2022, 29, 640–648. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, K.R.; Lea, W.B.; Neilson, J.C.; King, D.M.; Tutton, S.M. Percutaneous cryoablation for the treatment of extra-abdominal desmoid tumors. J. Surg. Oncol. 2019, 120, 366–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitz, J.J.; Schmit, G.D.; Atwell, T.D.; Callstrom, M.R.; Kurup, A.N.; Weisbrod, A.J.; Morris, J.M. Percutaneous Cryoablation of Extraabdominal Desmoid Tumors: A 10-Year Experience. Am. J. Roentgenol. 2016, 207, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Fusco, R.; Catalano, O.; Guarino, B.; Granata, F.; Tatangelo, F.; Avallone, A.; Piccirillo, M.; Palaia, R.; Izzo, F.; et al. Intravoxel incoherent motion (IVIM) in diffusion-weighted imaging (DWI) for Hepatocellular carcinoma: Correlation with histologic grade. Oncotarget 2016, 7, 79357–79364. [Google Scholar] [CrossRef] [Green Version]
- Granata, V.; Fusco, R.; Catalano, O.; Filice, S.; Amato, D.M.; Nasti, G.; Avallone, A.; Izzo, F.; Petrillo, A. Early Assessment of Colorectal Cancer Patients with Liver Metastases Treated with Antiangiogenic Drugs: The Role of Intravoxel Incoherent Motion in Diffusion-Weighted Imaging. PLoS ONE 2015, 10, e0142876. [Google Scholar] [CrossRef]
- Jensen, J.H.; Helpern, J.A. MRI quantification of non-Gaussian water diffusion by kurtosis analysis. NMR Biomed. 2010, 23, 698–710. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Padhani, A.R.; Chenevert, T.L.; Koh, D.-M.; Msc, F.D.K.; Taouli, B.; Le Bihan, D. Body diffusion kurtosis imaging: Basic principles, applications, and considerations for clinical practice. J. Magn. Reson. Imaging 2015, 42, 1190–1202. [Google Scholar] [CrossRef] [Green Version]
- Crimì, F.; Capelli, G.; Spolverato, G.; Bao, Q.R.; Florio, A.; Rossi, S.M.; Cecchin, D.; Albertoni, L.; Campi, C.; Pucciarelli, S.; et al. MRI T2-weighted sequences-based texture analysis (TA) as a predictor of response to neoadjuvant chemo-radiotherapy (nCRT) in patients with locally advanced rectal cancer (LARC). Radiol. Med. 2020, 125, 1216–1224. [Google Scholar] [CrossRef]
- Santone, A.; Brunese, M.C.; Donnarumma, F.; Guerriero, P.; Mercaldo, F.; Reginelli, A.; Miele, V.; Giovagnoni, A.; Brunese, L. Radiomic features for prostate cancer grade detection through formal verification. Radiol. Med. 2021, 126, 688–697. [Google Scholar] [CrossRef]
- Cusumano, D.; Meijer, G.; Lenkowicz, J.; Chiloiro, G.; Boldrini, L.; Masciocchi, C.; Dinapoli, N.; Gatta, R.; Casà, C.; Damiani, A.; et al. A field strength independent MR radiomics model to predict pathological complete response in locally advanced rectal cancer. Radiol. Med. 2021, 126, 421–429. [Google Scholar] [CrossRef]
- Nazari, M.; Shiri, I.; Hajianfar, G.; Oveisi, N.; Abdollahi, H.; Deevband, M.R.; Oveisi, M.; Zaidi, H. Noninvasive Fuhrman grading of clear cell renal cell carcinoma using computed tomography radiomic features and machine learning. Radiol. Med. 2020, 125, 754–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moustafa, A.F.; Eldaly, M.M.; Zeitoun, R.; Shokry, A. Is MRI diffusion-weighted imaging a reliable tool for the diagnosis and post-therapeutic follow-up of extremity soft tissue neoplasms? Indian J. Radiol. Imaging 2019, 29, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, S.; Sinha, A.; Tam, E.; Stirling, J.J.; Simcock, I.; Clark, S.; Goh, V. Diffusion tensor imaging (DTI) of desmoid tumours in familial adenomatous polyposis: Initial experience. Eur. J. Radiol. 2012, 81, 3646–3651. [Google Scholar] [CrossRef]
- Oka, K.; Yakushiji, T.; Sato, H.; Fujimoto, T.; Hirai, T.; Yamashita, Y.; Mizuta, H. Usefulness of diffusion-weighted imaging for differentiating between desmoid tumors and malignant soft tissue tumors. J. Magn. Reson. Imaging 2011, 33, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Petralia, G.; Summers, P.E.; Agostini, A.; Ambrosini, R.; Cianci, R.; Cristel, G.; Calistri, L.; Colagrande, S. Dynamic contrast-enhanced MRI in oncology: How we do it. Radiol. Med. 2020, 125, 1288–1300. [Google Scholar] [CrossRef] [PubMed]
- Fusco, R.; Granata, V.; Sansone, M.; Rega, D.; Delrio, P.; Tatangelo, F.; Romano, C.; Avallone, A.; Pupo, D.; Giordano, M.; et al. Validation of the standardized index of shape tool to analyze DCE-MRI data in the assessment of neo-adjuvant therapy in locally advanced rectal cancer. Radiol. Med. 2021, 126, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, A.; Fusco, R.; Petrillo, M.; Granata, V.; Delrio, P.; Bianco, F.; Pecori, B.; Botti, G.; Tatangelo, F.; Caracò, C.; et al. Standardized Index of Shape (DCE-MRI) and Standardized Uptake Value (PET/CT): Two quantitative approaches to discriminate chemo-radiotherapy locally advanced rectal cancer responders under a functional profile. Oncotarget 2017, 8, 8143–8153. [Google Scholar] [CrossRef] [Green Version]
- Rega, D.; Pace, U.; Scala, D.; Chiodini, P.; Granata, V.; Bucci, A.F.; Pecori, B.; DelRio, P. Treatment of splenic flexure colon cancer: A comparison of three different surgical procedures: Experience of a high volume cancer center. Sci. Rep. 2019, 9, 10953. [Google Scholar] [CrossRef] [Green Version]
- Fusco, R.; Sansone, M.; Granata, V.; Grimm, R.; Pace, U.; Delrio, P.; Tatangelo, F.; Botti, G.; Avallone, A.; Pecori, B.; et al. Diffusion and perfusion MR parameters to assess preoperative short-course radiotherapy response in locally advanced rectal cancer: A comparative explorative study among Standardized Index of Shape by DCE-MRI, intravoxel incoherent motion- and diffusion kurtosis imaging-derived parameters. Abdom. Radiol. 2019, 44, 3683–3700. [Google Scholar] [CrossRef]
- Banerji, A.; Naish, J.H.; Watson, Y.; Jayson, G.C.; Buonaccorsi, G.A.; Parker, G.J. DCE- MRI model selection for investigating dis ruption of microvascular function in livers with metastatic disease. J. Magn. Reson. Imaging 2012, 35, 196–203. [Google Scholar] [CrossRef]
- Khalifa, F.; Soliman, A.; El-Baz, A.; El-Ghar, M.A.; El-Diasty, T.; Gimel’Farb, G.; Ouseph, R.; Dwyer, A.C. Models and methods for analyzing DCE-MRI: A review. Med. Phys. 2014, 41, 124301. [Google Scholar] [CrossRef] [PubMed]
- Mungai, F.; Verrone, G.B.; Bonasera, L.; Bicci, E.; Pietragalla, M.; Nardi, C.; Berti, V.; Mazzoni, L.N.; Miele, V. Imaging biomarkers in the diagnosis of salivary gland tumors: The value of lesion/parenchyma ratio of perfusion-MR pharmacokinetic parameters. Radiol. Med. 2021, 126, 1345–1355. [Google Scholar] [CrossRef]
- Russo, L.; Gui, B.; Miccò, M.; Panico, C.; De Vincenzo, R.; Fanfani, F.; Scambia, G.; Manfredi, R. The role of MRI in cervical cancer > 2 cm (FIGO stage IB2-IIA1) conservatively treated with neoadjuvant chemotherapy followed by conization: A pilot study. Radiol. Med. 2021, 126, 1055–1063. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, W.; Tang, J. Ultrasound-guided high intensity focused ultrasound treatment for extra-abdominal desmoid tumours: Preliminary results. Int. J. Hyperth. 2011, 27, 648–653. [Google Scholar] [CrossRef]
- Ghanouni, P.; Dobrotwir, A.; Bazzocchi, A.; Bucknor, M.; Bitton, R.; Rosenberg, J.; Avedian, R. Magnetic resonance-guided focused ultrasound treatment of extra-abdominal desmoid tumors: A retrospective multicenter study. Eur. Radiol. 2017, 27, 732–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, W.-P.; Han, Z.-Y.; Zhang, J.; Yu, X.-L.; Cheng, Z.-G.; Zhou, X.; Liang, P. Early experience: High-intensity focused ultrasound treatment for intra-abdominal aggressive fibromatosis of failure in surgery. Br. J. Radiol. 2016, 89, 20151026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Huang, Y.; Zhou, M.; Ying, X.; Hu, X. High-intensity focused ultrasound treatment for intra-abdominal desmoid tumors: A report of four cases. J. Med. Ultrason. 2016, 43, 279–284. [Google Scholar] [CrossRef]
- Najafi, A.; Fuchs, B.; Binkert, C.A. Mid-term results of MR-guided high-intensity focused ultrasound treatment for relapsing superficial desmoids. Int. J. Hyperth. 2019, 36, 537–541. [Google Scholar] [CrossRef] [Green Version]
- Griffin, M.O.; Kulkarni, N.M.; O’Connor, S.D.; Sudakoff, G.S.; Lea, W.B.; Tutton, S.M. Magnetic resonance-guided focused ultrasound: A brief review with emphasis on the treatment of extra-abdominal desmoid tumors. Ultrasound Q. 2019, 35, 346–354. [Google Scholar] [CrossRef]
- Avedian, R.S.; Bitton, R.; Gold, G.; Butts-Pauly, K.; Ghanouni, P. Is MR-guided high-intensity focused ultrasound a feasible treatment modality for desmoid tumors? Clin. Orthop. Relat. Res. 2016, 474, 697–704. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Chen, J.-Y.; Zhang, L.; Li, K.-Q.; Xiao, Z.-B.; Mo, S.-J.; Chen, L.; Chen, W.-Z. The safety and ablation efficacy of ultrasound-guided high-intensity focused ultrasound ablation for desmoid tumors. Int. J. Hyperth. 2021, 38, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Bashir, U.; Moskovic, E.; Strauss, D.; Hayes, A.; Thway, K.; Pope, R.; Messiou, C. Soft-tissue masses in the abdominal wall. Clin. Radiol. 2014, 69, e422–e431. [Google Scholar] [CrossRef] [PubMed]
- Masciocchi, C.; Lanni, G.; Conti, L.; Conchiglia, A.; Fascetti, E.; Flamini, S.; Coletti, G.; Barile, A. Soft-tissue inflammatory myofibroblastic tumors (IMTs) of the limbs: Potential and limits of diagnostic imaging. Skelet. Radiol. 2012, 41, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Masciocchi, C.; Sparvoli, L.; Barile, A. Diagnostic imaging of malignant cartilage tumors. Eur. J. Radiol. 1998, 27, S86–S90. [Google Scholar] [CrossRef]
- Barile, A.; Sabatini, M.; Iannessi, F.; Di Cesare, E.; Splendiani, A.; Calvisi, V.; Masciocchi, C. Pigmented villonodular synovitis (PVNS) of the knee joint: Magnetic resonance imaging (MRI) using standard and dynamic paramagnetic contrast media. Report of 52 cases surgically and histologically controlled. Radiol. Med. 2004, 107, 356–366. [Google Scholar]









| Tumor | Desmoid Abdominal Tumor | Other Abdominal Malignancy | Desmoid Extra-Abdominal Tumor | Malignant Soft Tissue Tumors |
|---|---|---|---|---|
| Imaging Assessment [80,137] | The density of the lesions on CT imaging is uniform, and an enhanced scan can show uniform enhancement. Homogeneous signal is isointense in T1-W and hyperintense in T2-W | Inhomogeneous density on CT and signal intensity on MRI, due to necrosis and calcifications, with inhomogeneous contrast enhancement during contrast studies | CT features of desmoid tumors of the extremities exhibited a slightly low density, mild enhancement, unclear boundary and uneven enhancement after contrast administration. Their imaging features on MRI were a round or fusiform shape, unclear boundaries, uniform signal, uneven enhancement, “tree root” or “claw” infiltration and invasion of the neurovascular bundles | Inhomogeneous density on CT and long T1 and long T2 signals, T2 signal intensity higher than that of fat on MRI. Calcification or cystic necrosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simonetti, I.; Bruno, F.; Fusco, R.; Cutolo, C.; Setola, S.V.; Patrone, R.; Masciocchi, C.; Palumbo, P.; Arrigoni, F.; Picone, C.; et al. Multimodality Imaging Assessment of Desmoid Tumors: The Great Mime in the Era of Multidisciplinary Teams. J. Pers. Med. 2022, 12, 1153. https://doi.org/10.3390/jpm12071153
Simonetti I, Bruno F, Fusco R, Cutolo C, Setola SV, Patrone R, Masciocchi C, Palumbo P, Arrigoni F, Picone C, et al. Multimodality Imaging Assessment of Desmoid Tumors: The Great Mime in the Era of Multidisciplinary Teams. Journal of Personalized Medicine. 2022; 12(7):1153. https://doi.org/10.3390/jpm12071153
Chicago/Turabian StyleSimonetti, Igino, Federico Bruno, Roberta Fusco, Carmen Cutolo, Sergio Venanzio Setola, Renato Patrone, Carlo Masciocchi, Pierpaolo Palumbo, Francesco Arrigoni, Carmine Picone, and et al. 2022. "Multimodality Imaging Assessment of Desmoid Tumors: The Great Mime in the Era of Multidisciplinary Teams" Journal of Personalized Medicine 12, no. 7: 1153. https://doi.org/10.3390/jpm12071153