
Construction of a miRNA-Based Nomogram Model to Predict the Prognosis of Endometrial Cancer

 , , and
, , and 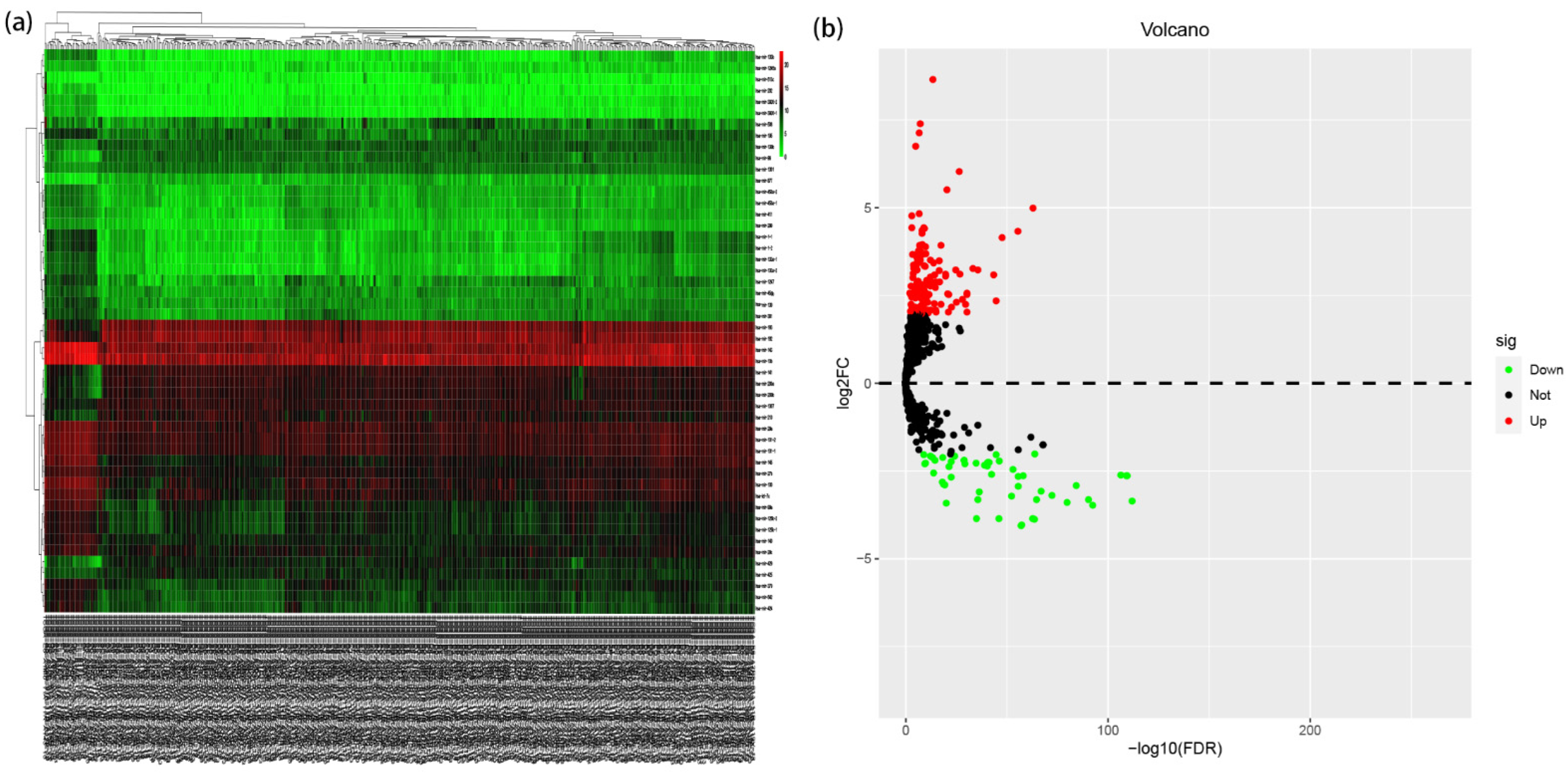{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Resources and Preprocessing
2.2. Identification of Potential Prognostic miRNAs
2.3. Establishment of EC Prognostic Risk Model
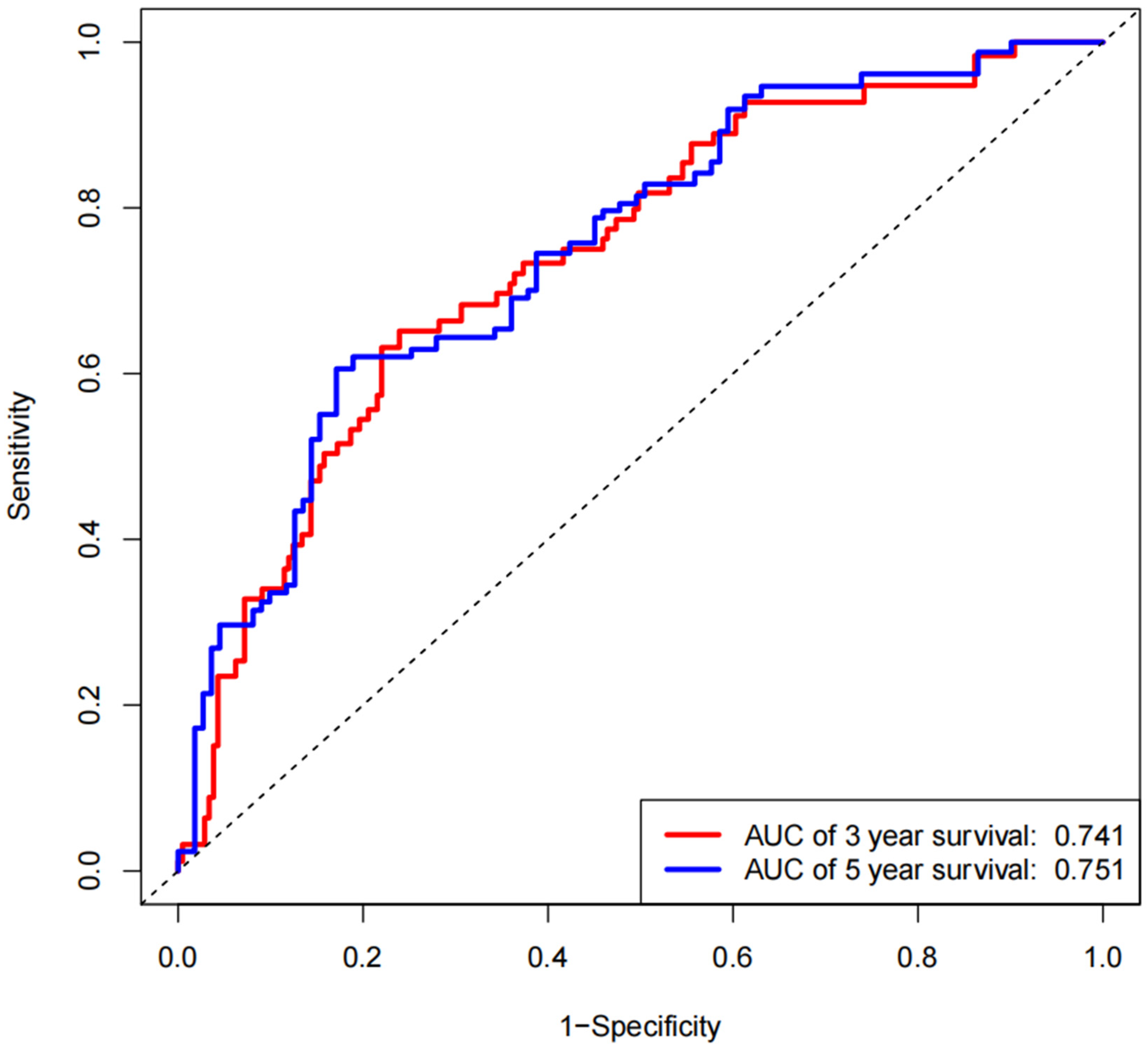
2.4. Calibration and Validation of the EC Survival Nomogram Model (Predictions)
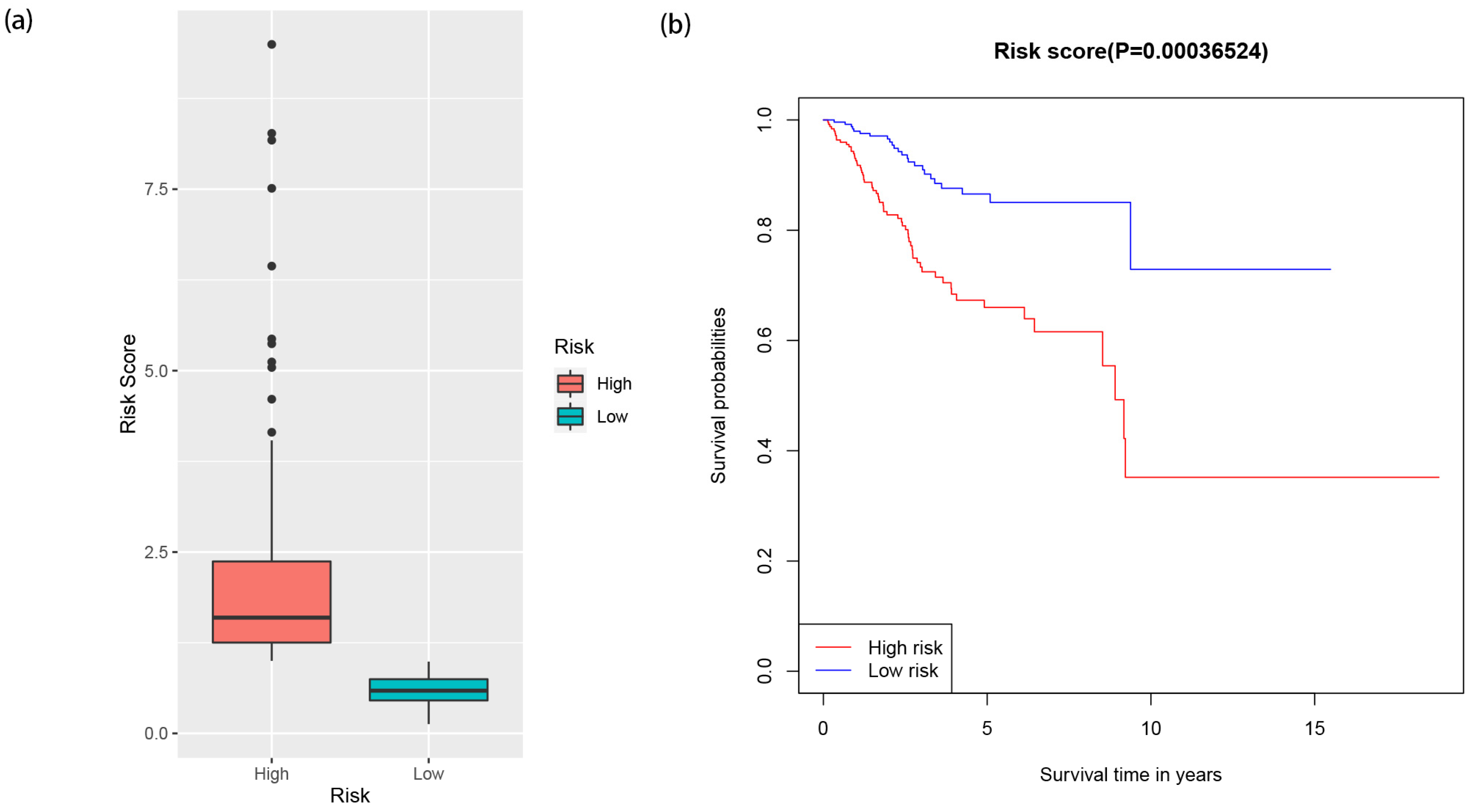
2.5. Visualization of Risk Score of EC Patients in High- and Low-Risk Groups
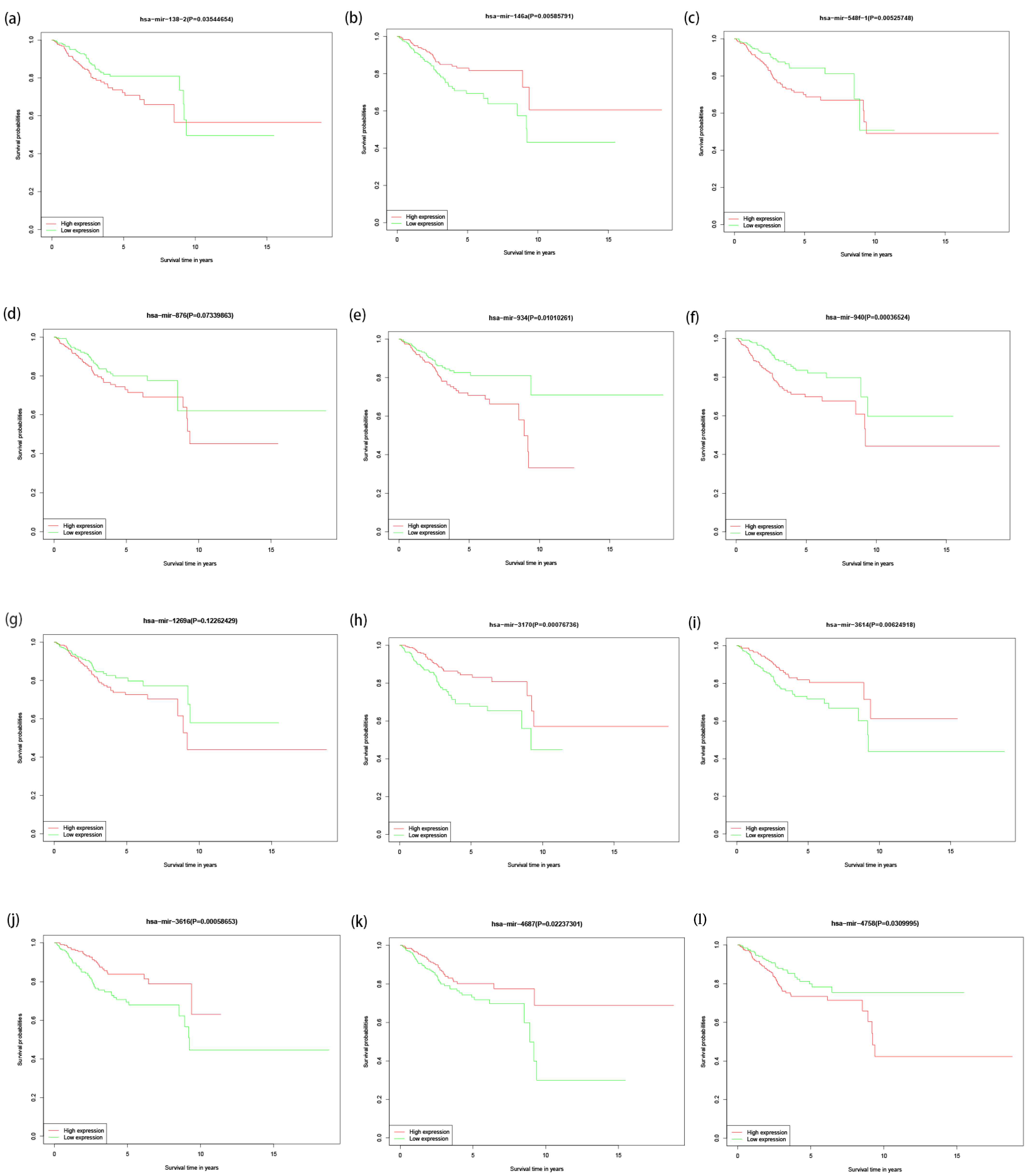
2.6. Survival Analysis of Differentially Expressed miRNAs
2.7. Statistical Analyses
3. Results
3.1. Determining the Significance of Differential Expression of miRNAs
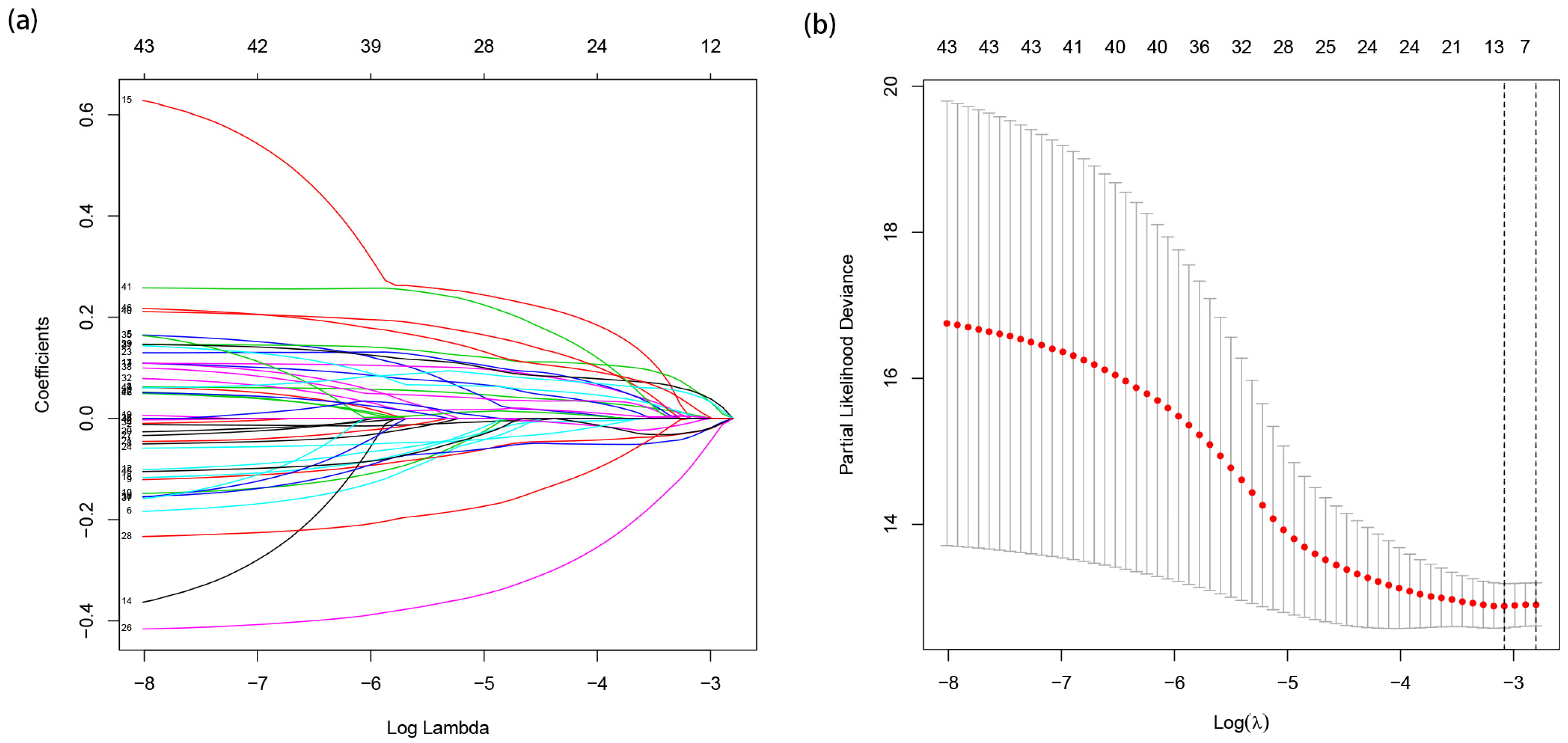
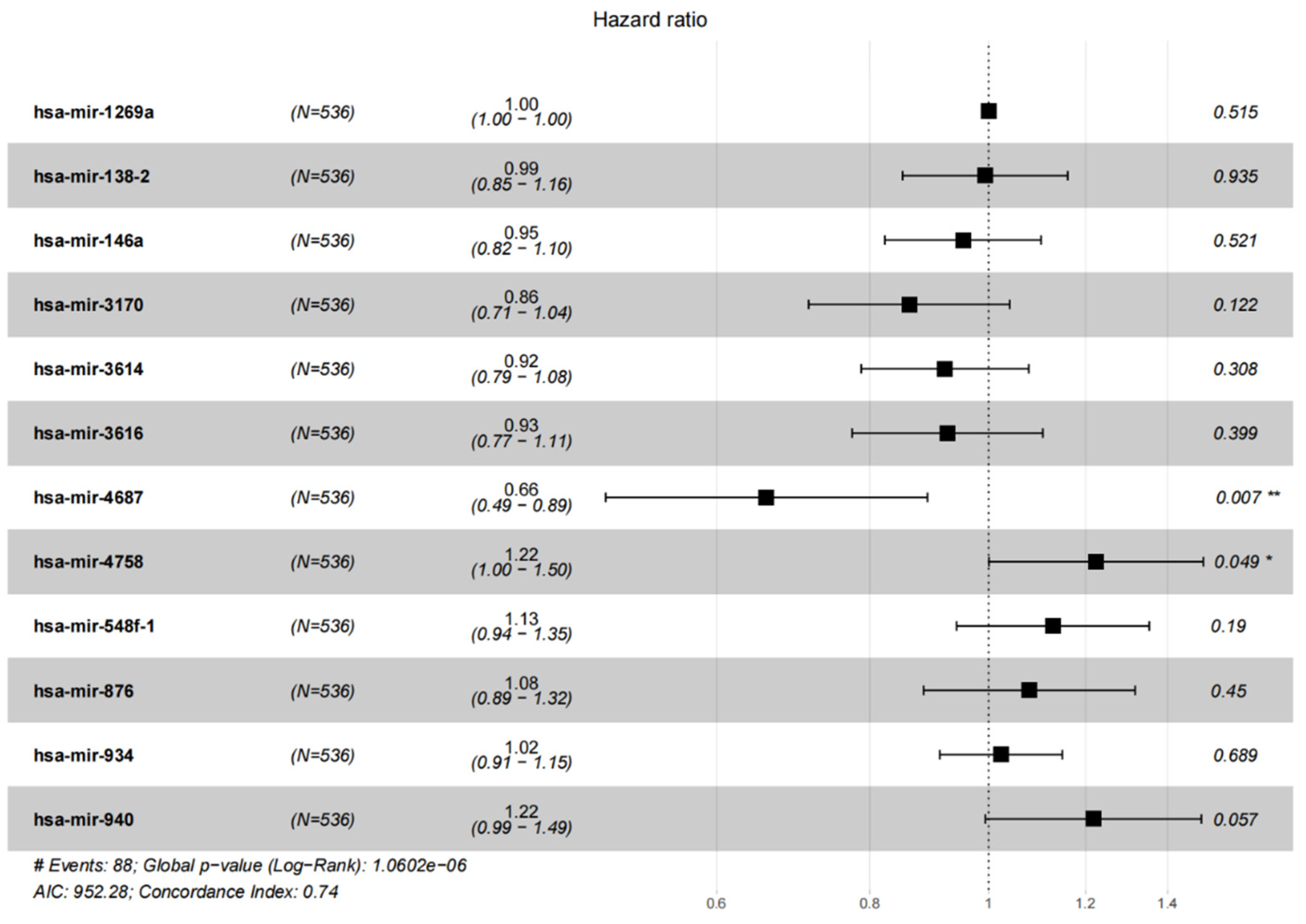
3.2. Construction of EC Prognosis Survival Nomogram Model
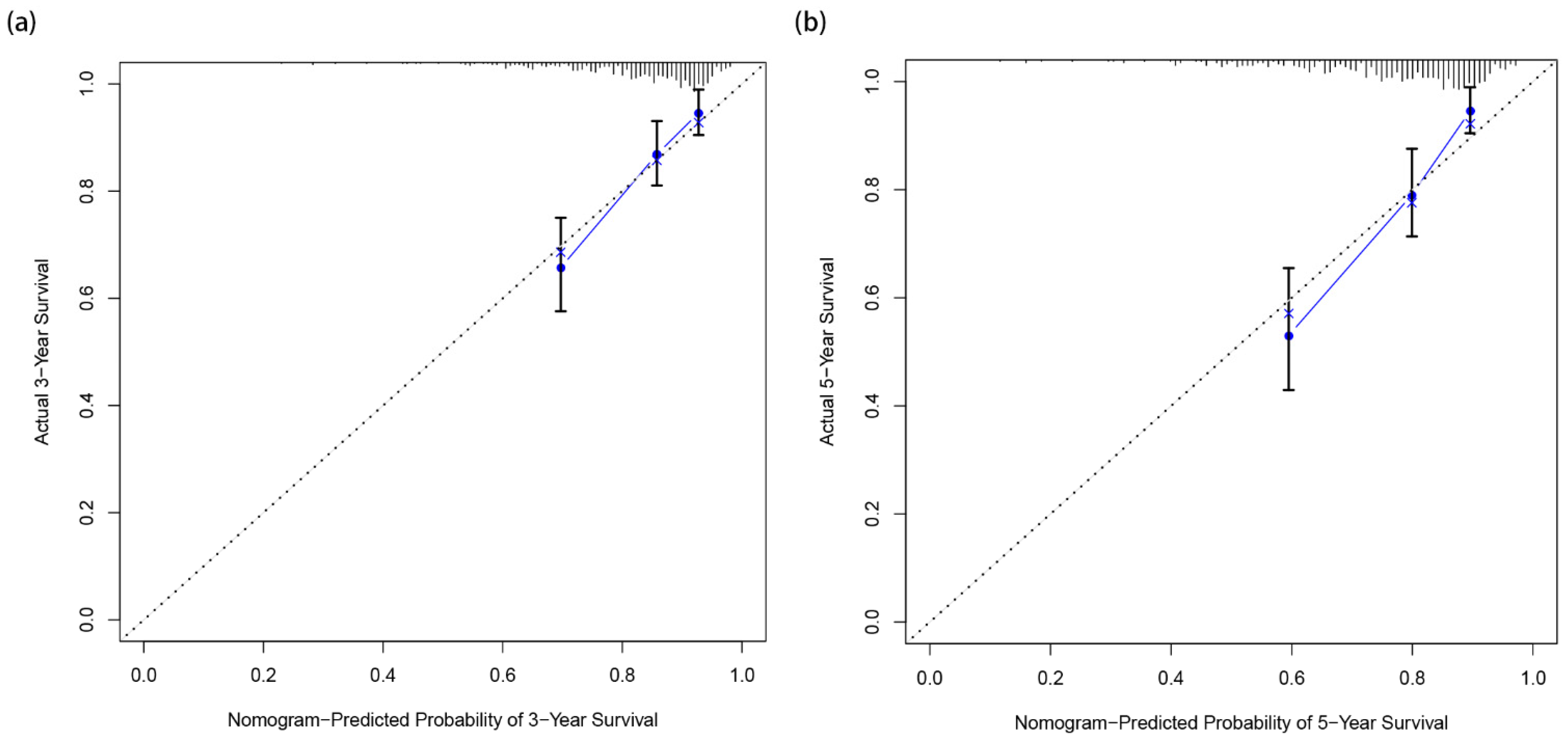
3.3. Calibration and Verification of the Nomogram
3.4. Visualization of Risk Score of EC Patients in High- and Low-Risk Groups and Survival Analysis of 12 miRNAs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lortet-Tieulent, J.; Ferlay, J.; Bray, F.; Jemal, A. International Patterns and Trends in Endometrial Cancer Incidence, 1978–2013. JNCI J. Natl. Cancer Inst. 2018, 110, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Shaw, E.; Farris, M.; McNeil, J.; Friedenreich, C. Obesity and Endometrial Cancer. In Recent Results in Cancer Research Obesity and Cancer; Pischon, T., Nimptsch, K., Eds.; Springer International Publishing: Cham, Switzerland, 2016; Volume 208, pp. 107–136. ISBN 978-3-319-42540-5. [Google Scholar]
- Siegel, R.; DeSantis, C.; Virgo, K.; Stein, K.; Mariotto, A.; Smith, T.; Cooper, D.; Gansler, T.; Lerro, C.; Fedewa, S.; et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J. Clin. 2012, 62, 220–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeckstaens, S.; Dewalheyns, S.; Heremans, R.; Vikram, R.; Timmerman, D.; Bosch, T.V.D.; Verbakel, J.Y. Signs and symptoms associated with uterine cancer in pre- and postmenopausal women. Heliyon 2020, 6, e05372. [Google Scholar] [CrossRef] [PubMed]
- Pastrello, C.; Polesel, J.; Della Puppa, L.; Viel, A.; Maestro, R. Association between hsa-mir-146a genotype and tumor age-of-onset in BRCA1/BRCA2-negative familial breast and ovarian cancer patients. Carcinogenesis 2010, 31, 2124–2126. [Google Scholar] [CrossRef] [Green Version]
- Matteson, K.A.; Robison, K.; Jacoby, V.L. Opportunities for Early Detection of Endometrial Cancer in Women With Postmenopausal Bleeding. JAMA Intern. Med. 2018, 178, 1222–1223. [Google Scholar] [CrossRef]
- Buchanan, E.M.; Weinstein, L.C.; Hillson, C. Endometrial Cancer. Am. Fam. Physician 2009, 80, 1075–1080. [Google Scholar]
- Amant, F.; Moerman, P.; Neven, P.; Timmerman, D.; Van Limbergen, E.; Vergote, I. Endometrial cancer. Lancet 2005, 366, 491–505. [Google Scholar] [CrossRef]
- Albertini, A.-F.; Devouassoux-Shisheboran, M.; Genestie, C. Pathology of endometrioid carcinoma. Bull. Cancer 2012, 99, 7–12. [Google Scholar] [CrossRef]
- Leskela, S.; Pérez-Mies, B.; Rosa-Rosa, J.M.; Cristobal, E.; Biscuola, M.; Palacios-Berraquero, M.L.; Ong, S.; Guia, X.M.-G.; Palacios, J. Molecular Basis of Tumor Heterogeneity in Endometrial Carcinosarcoma. Cancers 2019, 11, 964. [Google Scholar] [CrossRef] [Green Version]
- Bansal, N.; Yendluri, V.; Wenham, R.M. The Molecular Biology of Endometrial Cancers and the Implications for Pathogenesis, Classification, and Targeted Therapies. Cancer Control 2009, 16, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Denschlag, D.; Ulrich, U.; Emons, G. The Diagnosis and Treatment of Endometrial Cancer. Dtsch. Ärztebl. Int. 2011, 108, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Binder, P.S.; Mutch, D.G. Update on Prognostic Markers for Endometrial Cancer. Women’s Health 2014, 10, 277–288. [Google Scholar] [CrossRef] [Green Version]
- Dou, Y.; Kawaler, E.A.; Zhou, D.C.; Gritsenko, M.A.; Huang, C.; Blumenberg, L.; Karpova, A.; Petyuk, V.A.; Savage, S.R.; Satpathy, S.; et al. Proteogenomic Characterization of Endometrial Carcinoma. Cell 2020, 180, 729–748.e26. [Google Scholar] [CrossRef] [PubMed]
- Si, W.; Shen, J.; Zheng, H.; Fan, W. The role and mechanisms of action of microRNAs in cancer drug resistance. Clin. Epigenetics 2019, 11, 25. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Wang, H.; Yao, X.; Zhang, D.; Xie, Y.; Cui, R.; Zhang, X. Circulating MicroRNAs in Cancer: Potential and Challenge. Front. Genet. 2019, 10, 626. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, T.P.; Miskiewicz, J.; Szostak, N.; Szachniuk, M.; Grodecka-Gazdecka, S.; Jagodziński, P.P. In Vitro and In Silico Analysis of miR-125a with rs12976445 Polymorphism in Breast Cancer Patients. Appl. Sci. 2020, 10, 7275. [Google Scholar] [CrossRef]
- Garzon, R.; Calin, G.A.; Croce, C.M. MicroRNAs in Cancer. Annu. Rev. Med. 2009, 60, 167–179. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Jensen, M.A.; Zenklusen, J.C. A Practical Guide to The Cancer Genome Atlas (TCGA). Methods Mol. Biol. Clifton NJ 2016, 1418, 111–141. [Google Scholar] [CrossRef]
- Wu, Y.-S.; Lin, H.; Chen, D.; Yi, Z.; Zeng, B.; Jiang, Y.; Ren, G. A four-miRNA signature as a novel biomarker for predicting survival in endometrial cancer. Gene 2019, 697, 86–93. [Google Scholar] [CrossRef]
- Colaprico, A.; Silva, T.C.; Olsen, C.; Garofano, L.; Cava, C.; Garolini, D.; Sabedot, T.S.; Malta, T.M.; Pagnotta, S.M.; Castiglioni, I.; et al. TCGAbiolinks: An R/Bioconductor package for integrative analysis of TCGA data. Nucleic Acids Res. 2016, 44, e71. [Google Scholar] [CrossRef]
- Anders, S.; Huber, W. Differential expression analysis for sequence count data. Genome Biol. 2010, 11, R106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Brooks, R.A.; Fleming, G.F.; Lastra, R.R.; Lee, N.K.; Moroney, J.W.; Son, C.H.; Tatebe, K.; Veneris, J.L. Current recommendations and recent progress in endometrial cancer. CA Cancer J. Clin. 2019, 69, 258–279. [Google Scholar] [CrossRef] [PubMed]
- Temkin, S.M.; Fleming, G. Current Treatment of Metastatic Endometrial Cancer. Cancer Control 2009, 16, 38–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njoku, K.; Abiola, J.; Russell, J.; Crosbie, E.J. Endometrial cancer prevention in high-risk women. Best Pract. Res. Clin. Obstet. Gynaecol. 2019, 65, 66–78. [Google Scholar] [CrossRef] [PubMed]
- Yi, D.; Wang, R.; Shi, X.; Xu, L.; Yilihamu, Y.; Sang, J. METTL14 promotes the migration and invasion of breast cancer cells by modulating N6-methyladenosine and hsa-miR-146a-5p expression. Oncol. Rep. 2020, 43, 1375–1386. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, M.; Yang, Q. A six-microRNA signature predicts survival of patients with uterine corpus endometrial carcinoma. Curr. Probl. Cancer 2019, 43, 167–176. [Google Scholar] [CrossRef]
- Hill, M.; Tran, N. miRNA interplay: Mechanisms and consequences in cancer. Dis. Model. Mech. 2021, 14, dmm047662. [Google Scholar] [CrossRef]
- Huang, X.; Zhu, X.; Yu, Y.; Zhu, W.; Jin, L.; Zhang, X.; Li, S.; Zou, P.; Xie, C.; Cui, R. Dissecting miRNA signature in colorectal cancer progression and metastasis. Cancer Lett. 2021, 501, 66–82. [Google Scholar] [CrossRef]
- Sengupta, D.; Deb, M.; Kar, S.; Pradhan, N.; Parbin, S.; Kirtana, R.; Singh, S.P.; Suma, S.; Niharika; Roy, A.; et al. Dissecting miRNA facilitated physiology and function in human breast cancer for therapeutic intervention. Semin. Cancer Biol. 2020, 72, 46–64. [Google Scholar] [CrossRef]
- Mazumder, S.; Datta, S.; Ray, J.G.; Chaudhuri, K.; Chatterjee, R. Liquid biopsy: miRNA as a potential biomarker in oral cancer. Cancer Epidemiol. 2019, 58, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Tepe, N.B.; Bozgeyik, E.; Bozdag, Z.; Balat, O.; Ozcan, H.C.; Ugur, M.G. Identification of autophagy-associated miRNA signature for the cervical squamous cell cancer and high-grade cervical intraepithelial lesions. Reprod. Biol. 2021, 21, 100536. [Google Scholar] [CrossRef] [PubMed]
- Sohrabi, E.; Rezaie, E.; Heiat, M.; Sefidi-Heris, Y. An Integrated Data Analysis of mRNA, miRNA and Signaling Pathways in Pancreatic Cancer. Biochem. Genet. 2021, 59, 1326–1358. [Google Scholar] [CrossRef] [PubMed]
- Giambò, F.; Leone, G.M.; Gattuso, G.; Rizzo, R.; Cosentino, A.; Cinà, D.; Teodoro, M.; Costa, C.; Tsatsakis, A.; Fenga, C.; et al. Genetic and Epigenetic Alterations Induced by Pesticide Exposure: Integrated Analysis of Gene Expression, microRNA Expression, and DNA Methylation Datasets. Int. J. Environ. Res. Public Health. 2021, 18, 8697. [Google Scholar] [CrossRef] [PubMed]
- Falzone, L.; Grimaldi, M.; Celentano, E.; Augustin, L.S.A.; Libra, M. Identification of Modulated MicroRNAs Associated with Breast Cancer, Diet, and Physical Activity. Cancers 2020, 12, 2555. [Google Scholar] [CrossRef]
- Chen, W.; Gao, C.; Liu, Y.; Wen, Y.; Hong, X.; Huang, Z. Bioinformatics Analysis of Prognostic miRNA Signature and Potential Critical Genes in Colon Cancer. Front. Genet. 2020, 11, 478. [Google Scholar] [CrossRef]
- Liu, X.; Pu, K.; Wang, Y.; Chen, Y.; Zhou, Y. Gastric cancer-associated microRNA expression signatures: Integrated bioinformatics analysis, validation, and clinical significance. Ann. Transl. Med. 2021, 9, 797. [Google Scholar] [CrossRef]
- Huang, D.-P.; Zeng, Y.-H.; Yuan, W.-Q.; Huang, X.-F.; Chen, S.-Q.; Wang, M.-Y.; Qiu, Y.-J.; Tong, G.-D. Bioinformatics Analyses of Potential miRNA-mRNA Regulatory Axis in HBV-related Hepatocellular Carcinoma. Int. J. Med. Sci. 2021, 18, 335–346. [Google Scholar] [CrossRef]
- Wang, Q.; Xu, K.; Tong, Y.; Dai, X.; Xu, T.; He, D.; Ying, J. Novel miRNA markers for the diagnosis and prognosis of endometrial cancer. J. Cell. Mol. Med. 2020, 24, 4533–4546. [Google Scholar] [CrossRef] [Green Version]
- Lu, N.; Liu, J.; Ji, C.; Wang, Y.; Wu, Z.; Yuan, S.; Xing, Y.; Diao, F. MiRNA based tumor mutation burden diagnostic and prognostic prediction models for endometrial cancer. Bioengineered 2021, 12, 3603–3620. [Google Scholar] [CrossRef]
- Qin, S.; Gao, Y.; Yang, Y.; Zhang, L.; Zhang, T.; Yu, J.; Shi, C. Identifying Molecular Markers of Cervical Cancer Based on Competing Endogenous RNA Network Analysis. Gynecol. Obstet. Investig. 2019, 84, 350–359. [Google Scholar] [CrossRef] [PubMed]
- Serum microRNAs in Clear Cell Carcinoma of the Ovary. Available online: https://www.sciencedirect.com/science/article/pii/S1028455914001855 (accessed on 23 May 2022).
- Sánchez-Chaparro, M.M.; Garza-Veloz, I.; Zayas-Villanueva, O.A.; Martinez-Fierro, M.L.; Delgado-Enciso, I.; Gomez-Govea, M.A.; Martínez-De-Villarreal, L.E.; Reséndez-Pérez, D.; Rodríguez-Sánchez, I.P. Genetic Variants in the 3’UTR of BRCA1 and BRCA2 Genes and Their Putative Effects on the microRNA Mechanism in Hereditary Breast and Ovarian Cancer. Diagnostics 2020, 10, 298. [Google Scholar] [CrossRef] [PubMed]
- Castilla, M.; López-García, M..; Atienza, M.R.; Rosa-Rosa, J.M.; Díaz-Martín, J.; Pecero, M.L.; Vieites, B.; Romero-Pérez, L.; Benítez, J.; Calcabrini, A.; et al. VGLL1 expression is associated with a triple-negative basal-like phenotype in breast cancer. Endocr.-Relat. Cancer 2014, 21, 587–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varkalaite, G.; Vaitkeviciute, E.; Inciuraite, R.; Salteniene, V.; Juzenas, S.; Petkevicius, V.; Gudaityte, R.; Mickevicius, A.; Link, A.; Kupcinskas, L.; et al. Atrophic gastritis and gastric cancer tissue miRNome analysis reveals hsa-miR-129-1 and hsa-miR-196a as potential early diagnostic biomarkers. World J. Gastroenterol. 2022, 28, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Peng, J.; Lai, J.; Liu, H.; Zhang, Z.; Li, X.; Liang, B.; Chen, X.; Zou, B.; Lin, S.; et al. MiR-940 promotes malignant progression of breast cancer by regulating FOXO3. Biosci. Rep. 2020, 40, BSR20201337. [Google Scholar] [CrossRef]
- Song, B.; Zhang, C.; Li, G.; Jin, G.; Liu, C. MiR-940 Inhibited Pancreatic Ductal Adenocarcinoma Growth by Targeting MyD88. Cell. Physiol. Biochem. 2015, 35, 1167–1177. [Google Scholar] [CrossRef]
- Rajendiran, S.; Parwani, A.V.; Hare, R.J.; Dasgupta, S.; Roby, R.K.; Vishwanatha, J.K. MicroRNA-940 suppresses prostate cancer migration and invasion by regulating MIEN1. Mol. Cancer 2014, 13, 250. [Google Scholar] [CrossRef] [Green Version]
- Shen, J.; Ambrosone, C.B.; DiCioccio, R.A.; Odunsi, K.; Lele, S.B.; Zhao, H. A functional polymorphism in the miR-146a gene and age of familial breast/ovarian cancer diagnosis. Carcinogenesis 2008, 29, 1963–1966. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Zhang, F.; Zhang, J.; Sun, Z.; Hao, C.; Cao, H.; Wang, W. A Novel miRNA-Based Model Can Predict the Prognosis of Clear Cell Renal Cell Carcinoma. Technol. Cancer Res. Treat. 2021, 20, 15330338211027923. [Google Scholar] [CrossRef]
- Li, F.; Yang, H.; Kong, T.; Chen, S.; Li, P.; Chen, L.; Cheng, J.; Cui, G.; Zhang, G. PGAM1, regulated by miR-3614-5p, functions as an oncogene by activating transforming growth factor-β (TGF-β) signaling in the progression of non-small cell lung carcinoma. Cell Death Dis. 2020, 11, 710. [Google Scholar] [CrossRef]
- Lu, J.; Liang, J.; Xu, M.; Wu, Z.; Cheng, W.; Wu, J. Identification of an eleven-miRNA signature to predict the prognosis of endometrial cancer. Bioengineered 2021, 12, 4201–4216. [Google Scholar] [CrossRef]
- Wu, K.; Peng, R.; Zhang, Z.; Liu, H.; Sun, Y. Downregulation of Hsa-MiR-3616-3p in Triple-Negative Breast Cancer Is Associated with Cell Migration and Invasion. Res. Sq. [CrossRef]
- Xu, Z.; Wang, Z.; Sun, H.; Xin, H. Evaluation of Exosomal miRNA in Blood as a Potential Diagnostic Biomarker for Human Non-Small Cell Lung Cancer. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e924721-1–e924721-8. [Google Scholar] [CrossRef] [PubMed]
- Nagy, Z.B.; Barták, B.K.; Kalmár, A.; Galamb, O.; Wichmann, B.; Dank, M.; Igaz, P.; Tulassay, Z.; Molnár, B. Comparison of Circulating miRNAs Expression Alterations in Matched Tissue and Plasma Samples During Colorectal Cancer Progression. Pathol. Oncol. Res. 2019, 25, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Xu, L.; Wang, X.; Niu, S.; Chen, H.; Li, C. A novel prognostic mRNA/miRNA signature for esophageal cancer and its immune landscape in cancer progression. Mol. Oncol. 2021, 15, 1088–1109. [Google Scholar] [CrossRef]
- Jin, R.-H.; Yu, D.-J.; Zhong, M. MiR-1269a Acts as an Onco-MiRNA in Non-Small Cell Lung Cancer via down-Regulating SOX6. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4648. [Google Scholar] [CrossRef]
- Falzone, L.; Scandurra, G.; Lombardo, V.; Gattuso, G.; Lavoro, A.; Distefano, A.B.; Scibilia, G.; Scollo, P. A multidisciplinary approach remains the best strategy to improve and strengthen the management of ovarian cancer (Review). Int. J. Oncol. 2021, 59, 53. [Google Scholar] [CrossRef]
- Scott, R.; Hawarden, A.; Russell, B.; Edmondson, R.J. Decision-Making in Gynaecological Oncology Multidisciplinary Team Meetings: A Cross-Sectional, Observational Study of Ovarian Cancer Cases. Oncol. Res. Treat. 2020, 43, 70–77. [Google Scholar] [CrossRef]
- Ugwumadu, L.; Chakrabarti, R.; Williams-Brown, E.; Rendle, J.; Swift, I.; John, B.; Allen-Coward, H.; Ofuasia, E. The role of the multidisciplinary team in the management of deep infiltrating endometriosis. Gynecol. Surg. 2017, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Emons, G.; Steiner, E.; Vordermark, D.; Uleer, C.; Bock, N.; Paradies, K.; Ortmann, O.; Aretz, S.; Mallmann, P.; Kurzeder, C.; et al. Interdisciplinary Diagnosis, Therapy and Follow-Up of Patients with Endometrial Cancer. Guideline (S3-Level, AWMF Registry Nummer 032/034-OL, April 2018)—Part 1 with Recommendations on the Epidemiology, Screening, Diagnosis and Hereditary Factors of Endometrial Cancer. Geburtshilfe Frauenheilkd. 2018, 78, 949–971. [Google Scholar] [CrossRef] [Green Version]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ni, L.; Tang, C.; Wang, Y.; Wan, J.; Charles, M.G.; Zhang, Z.; Li, C.; Zeng, R.; Jin, Y.; Song, P.; et al. Construction of a miRNA-Based Nomogram Model to Predict the Prognosis of Endometrial Cancer. J. Pers. Med. 2022, 12, 1154. https://doi.org/10.3390/jpm12071154
Ni L, Tang C, Wang Y, Wan J, Charles MG, Zhang Z, Li C, Zeng R, Jin Y, Song P, et al. Construction of a miRNA-Based Nomogram Model to Predict the Prognosis of Endometrial Cancer. Journal of Personalized Medicine. 2022; 12(7):1154. https://doi.org/10.3390/jpm12071154
Chicago/Turabian StyleNi, Leyi, Chengyun Tang, Yuning Wang, Jiaming Wan, Morgan G. Charles, Zilong Zhang, Chen Li, Ruijie Zeng, Yiyao Jin, Penghao Song, and et al. 2022. "Construction of a miRNA-Based Nomogram Model to Predict the Prognosis of Endometrial Cancer" Journal of Personalized Medicine 12, no. 7: 1154. https://doi.org/10.3390/jpm12071154