
Effect Modification by Social Determinants of Pharmacogenetic Medication Interactions on 90-Day Hospital Readmissions within an Integrated U.S. Healthcare System

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
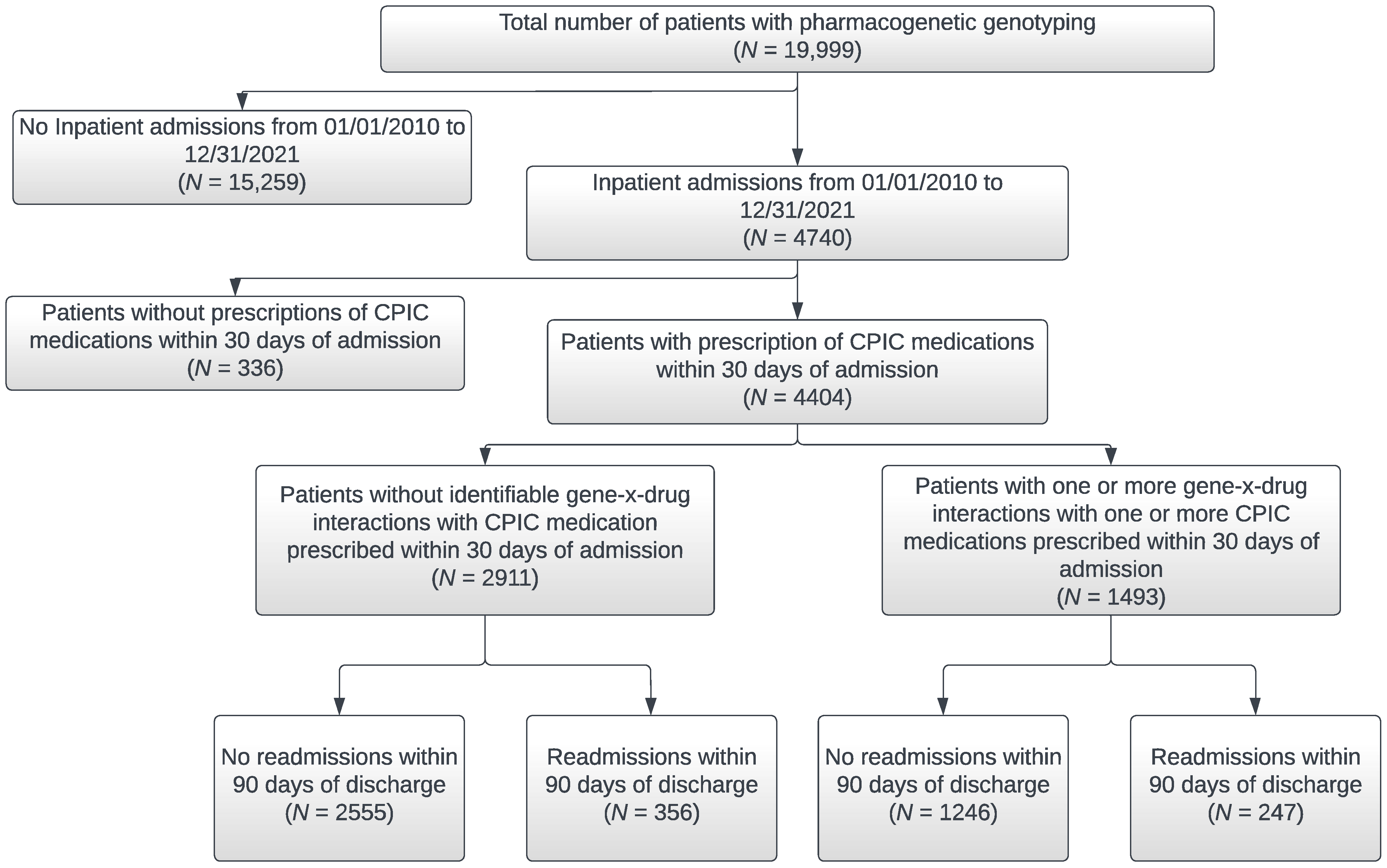
2.1. Study Setting and Population
2.2. Data Collection
2.3. Descriptive Analyses
2.4. Statistical Analyses
3. Results
3.1. Overall Study Population Sociodemographic and Clinical Characteristics
3.2. Characteristics of Patient Subpopulations with Inpatient Admissions and 90-Day Hospital Readmissions
3.3. Presence of at Least One Gene-x-Drug Interaction by Race/Ethnicity and 90-Day Hospital Readmissions
3.4. Effect Modification of Patient Sociodemographic and Clinical Characteristics on 90 Day Hospital Readmissions
4. Conclusions
4.1. Study Conclusions
4.2. Study Limitations
4.3. Study Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Committee for Quality Assurance. Plan All-Cause Readmissions (PCR). Available online: https://www.ncqa.org/hedis/measures/plan-all-cause-readmissions/ (accessed on 16 June 2022).
- Chin, D.L.; Bang, H.; Manickam, R.N.; Romano, P.S. Rethinking Thirty-Day Hospital Readmissions: Shorter Intervals Might Be Better Indicators of Quality of Care. Health Aff. 2016, 35, 1867–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, C.; Lingsma, H.F.; Marang-van de Mheen, P.J.; Kringos, D.S.; Klazinga, N.S.; Steyerberg, E.W. Is the readmission rate a valid quality indicator? A review of the evidence. PLoS ONE 2014, 9, e112282, Erratum in PLoS ONE 2015, 10, e0118968. [Google Scholar] [CrossRef] [Green Version]
- El Morabet, N.; Uitvlugt, E.B.; van den Bemt, B.J.F.; van den Bemt, P.; Janssen, M.J.A.; Karapinar-Carkit, F. Prevalence and Preventability of Drug-Related Hospital Readmissions: A Systematic Review. J. Am. Geriatr. Soc. 2018, 66, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Medicine. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care; The National Academies Press: Washington, DC, USA, 2003. [Google Scholar]
- Hockings, J.K.; Pasternak, A.L.; Erwin, A.L.; Mason, N.T.; Eng, C.; Hicks, J.K. Pharmacogenomics: An evolving clinical tool for precision medicine. Clevel. Clin. J. Med. 2020, 87, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, G.; Mohorn, P.; Yacoub, K.; May, D.W. Adverse Drug Reaction Deaths Reported in United States Vital Statistics, 1999–2006. Ann. Pharmacother. 2012, 46, 169–175. [Google Scholar] [CrossRef]
- David, V.; Fylan, B.; Bryant, E.; Smith, H.; Sagoo, G.S.; Rattray, M. An Analysis of Pharmacogenomic-Guided Pathways and Their Effect on Medication Changes and Hospital Admissions: A Systematic Review and Meta-Analysis. Front. Genet. 2021, 12, 698148. [Google Scholar] [CrossRef]
- Saulsberry, L.; Danahey, K.; Middlestadt, M.; Nutescu, E.A.; Chen, T.; Lee, J.C.; Ruhnke, G.W.; George, D.; House, L.; Choksi, A.; et al. Applicability of Pharmacogenomically Guided Medication Treatment during Hospitalization of At-Risk Minority Patients. J. Pers. Med. 2021, 11, 1343. [Google Scholar] [CrossRef]
- Williams, D.R.; Priest, N.; Anderson, N.B. Understanding associations among race, socioeconomic status, and health: Patterns and prospects. Health Psychol. 2016, 35, 407–411. [Google Scholar] [CrossRef]
- Goodman, C.W.; Brett, A.S. Race and Pharmacogenomics-Personalized Medicine or Misguided Practice? JAMA 2021, 325, 625–626. [Google Scholar] [CrossRef]
- Oni-Orisan, A.; Mavura, Y.; Banda, Y.; Thornton, T.A.; Sebro, R. Embracing Genetic Diversity to Improve Black Health. New. Engl. J. Med. 2021, 384, 1163–1167. [Google Scholar] [CrossRef]
- Bilal, U.; Jemmott, J.B.; Schnake-Mahl, A.; Murphy, K.; Momplaisir, F. Racial/ethnic and neighbourhood social vulnerability disparities in COVID-19 testing positivity, hospitalization, and in-hospital mortality in a large hospital system in Pennsylvania: A prospective study of electronic health records. Lancet Reg. Health Am. 2022, 10, 100220. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, P.Y.; Ryu, E.; Pathak, J.; Jenkins, G.D.; Batzler, A.; Hathcock, M.A.; Black, J.L.; Olson, J.E.; Cerhan, J.R.; Bielinski, S.J. Increased risk of hospitalization for ultrarapid metabolizers of cytochrome P450 2D6. Pharmgenomics Pers. Med. 2017, 10, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, P.Y.; Ryu, E.; Bielinski, S.J.; Hathcock, M.; Jenkins, G.D.; Cerhan, J.R.; Olson, J.E. No Association Between Pharmacogenomics Variants and Hospital and Emergency Department Utilization: A Mayo Clinic Biobank Retrospective Study. Pharmgenomics Pers. Med. 2021, 14, 229–237. [Google Scholar] [CrossRef] [PubMed]
- David, S.P.; Singh, L.; Pruitt, J.; Hensing, A.; Hulick, P.; Meltzer, D.O.; O’Donnell, P.H.; Dunnenberger, H.M. The Contribution of Pharmacogenetic Drug Interactions to 90-Day Hospital Readmissions: Preliminary Results from a Real-World Healthcare System. J. Pers. Med. 2021, 11, 1242. [Google Scholar] [CrossRef] [PubMed]
- David, S.P.; Dunnenberger, H.M.; Ali, R.; Matsil, A.; Lemke, A.A.; Singh, L.; Zimmer, A.; Hulick, P. Implementing Primary Care Mediated Population Genetic Screening Within an Integrated Health System. J. Am. Board Fam. Med. 2021, 34, 861–865. [Google Scholar] [CrossRef]
- Metopio. Available online: https://metop.io (accessed on 5 May 2022).
- Lloren, A.; Liu, S.; Herrin, J.; Lin, Z.; Zhou, G.; Wang, Y.; Kuang, M.; Zhou, S.; Farietta, T.; McCole, K.; et al. Measuring Hospital-Specific Disparities by Dual Eligibility and Race to Reduce Health Inequities. Health Serv. Res. 2019, 54, 243–254. [Google Scholar] [CrossRef] [Green Version]
- Downing, N.S.; Wang, C.; Gupta, A.; Wang, Y.; Nuti, S.V.; Ross, J.S.; Bernheim, S.M.; Lin, Z.; Normand, S.L.; Krumholz, H.M. Association of Racial and Socioeconomic Disparities with Outcomes among Patients Hospitalized with Acute Myocardial Infarction, Heart Failure, and Pneumonia: An Analysis of within- and between-Hospital Variation. JAMA Netw. Open 2018, 1, e182044. [Google Scholar] [CrossRef]
- Li, Y.; Cen, X.; Cai, X.; Thirukumaran, C.P.; Zhou, J.; Glance, L.G. Medicare Advantage Associated with More Racial Disparity Than Traditional Medicare For Hospital Readmissions. Health Aff. 2017, 36, 1328–1335. [Google Scholar] [CrossRef]
- Popejoy, A.B.; Fullerton, S.M. Genomics is failing on diversity. Nature 2016, 538, 161–164. [Google Scholar] [CrossRef] [Green Version]
- Popejoy, A.B. Diversity in Precision Medicine and Pharmacogenetics: Methodological and Conceptual Considerations for Broadening Participation. Pharmgenomics Pers. Med. 2019, 12, 257–271. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, J.M.; Alexander, G.C.; Palamuttam, N.; Mehta, H.B. Projected Utility of Pharmacogenomic Testing Among Individuals Hospitalized With COVID-19: A Retrospective Multicenter Study in the United States. Clin. Transl. Sci. 2021, 14, 153–162. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n (%) √ | Inpatient Admissions 2010–2020 a | ||||||
|---|---|---|---|---|---|---|---|
| Overall 19,999 (100) | No 15,259 (76) | Yes 4740 (24) | 90-Day Hospital Readmission b | ||||
| n = 4740 | |||||||
| No 4120 (87) | Yes 620 (13) | ||||||
| Age, median (IQR) | 53 (42–64) | 53 (42–63) | 54 (41–68) | * | 52 (41–67) | 62 (46–72) | * |
| Age group (years) | |||||||
| 18–39 | 4097 (20.5) | 3128 (76.3) | 969 (23.7) | 877 (90.5) | 92 (9.5) | ||
| 40–49 | 4275 (21.4) | 3208 (75) | 1067 (25) | 976 (91.5) | 91 (8.5) | ||
| 50–64 | 6849 (34.2) | 5679 (82.9) | 1170 (17.1) | 1011 (86.4) | 159 (13.6) | ||
| 65 or above | 4778 (23.9) | 3244 (67.9) | 1534 (32.1) | 1256 (81.9) | 278 (18.1) | ||
| Gender | * | * | |||||
| Female | 12,852 (64.3) | 9324 (72.5) | 3528 (27.5) | 3106 (88) | 422 (12) | ||
| Male | 7147 (35.7) | 5935 (83) | 1212 (17) | 1014 (83.7) | 198 (16.3) | ||
| Race | * | * | |||||
| White | 13,961 (69.9) | 10,292 (73.7) | 3669 (26.3) | 3172 (86.5) | 497 (13.5) | ||
| Black/African American | 612 (3.1) | 437 (71.4) | 175 (28.6) | 131 (74.9) | 44 (25.1) | ||
| Asian | 1293 (6.5) | 1020 (78.9) | 273 (21.1) | 254 (93) | 19 (7) | ||
| American Indian/Alaska Native | 37 (0.2) | 28 (75.7) | 9 (24.3) | 8 (88.9) | 1 (11.1) | ||
| Pacific Islander/Hawaiian Native | 18 (0.1) | 16 (88.9) | 2 (11.1) | 2 (100) | 0 (0) | ||
| Other | 3751 (18.8) | 3157 (84.2) | 594 (15.8) | 537 (90.4) | 57 (9.6) | ||
| Ethnicity | * | ||||||
| Hispanic/Latino | 981 (4.9) | 758 (77.3) | 223 (22.7) | 196 (87.9) | 27 (12.1) | ||
| Non-Hispanic | 18,653 (93.4) | 14,159 (75.9) | 4494 (24.1) | 3902 (86.8) | 592 (13.2) | ||
| Marital status | * | * | |||||
| Unmarried | 5700 (28.5) | 4472 (78.5) | 1228 (21.5) | 1010 (82.2) | 218 (17.8) | ||
| Married | 14,123 (70.6) | 10,620 (75.2) | 3503 (24.8) | 3102 (88.6) | 401 (11.4) | ||
| Employment status | * | * | |||||
| Employed | 12,961 (64.8) | 10,309 (79.5) | 2652 (20.5) | 2405 (90.7) | 247 (9.3) | ||
| Unemployed | 6328 (31.6) | 4338 (68.6) | 1990 (31.4) | 1624 (81.6) | 366 (18.4) | ||
| Insurance status | * | * | |||||
| Commercial | 16,387 (81.9) | 12,851 (78.4) | 3536 (21.6) | 3144 (88.9) | 392 (11.1) | ||
| Government | 3425 (17.1) | 2244 (65.5) | 1181 (34.5) | 957 (81) | 224 (19) | ||
| Out-of-pocket (self-pay) | 187 (0.9) | 164 (87.7) | 23 (12.3) | 19 (82.6) | 4 (17.4) | ||
| Median Household income in relation to US median household income *** | |||||||
| Above 64,994 | 18,634 (93.3) | 14,198 (76.2) | 4436 (23.8) | 3849 (86.8) | 587 (13.2) | ||
| 64,994 or less | 1330 (6.7) | 1030 (77.4) | 300 (22.6) | 268 (89.3) | 32 (10.7) | ||
| BMI, median (range, 13.3–79.2) | 27.0 (23.7–31.2) | 26.8 (23.7–30.8) | 27.6 (23.9–32.3) | * | 27.5 (23.8–32.1) | 28.6 (24.3–33.5) | * |
| Smoking status | |||||||
| No | 17,854 (96.6) | 13,349 (74.8) | 4505 (25.2) | 3918 (87) | 587 (13) | ||
| Yes | 632 (3.4) | 478 (75.6) | 154 (24.4) | 127 (82.5) | 27 (17.5) | ||
| COVID Status | |||||||
| Yes | 176 (0.9) | 130 (73.9) | 46 (26.1) | 41 (89.1) | 5 (10.9) | ||
| Number of comorbidities **** | * | * | |||||
| 0 | 11,972 (64.8) | 9398 (78.5) | 2574 (21.5) | 2334 (90.7) | 240 (9.3) | ||
| 1 | 4170 (22.6) | 3074 (73.7) | 1096 (26.3) | 946 (86.3) | 150 (13.7) | ||
| 2 | 1197 (6.5) | 749 (62.6) | 448 (37.4) | 360 (80.4) | 88 (19.6) | ||
| 3 or more | 1147 (6.2) | 606 (52.8) | 541 (47.2) | 405 (74.9) | 136 (25.1) | ||
| Comorbidities | |||||||
| Cancer | 225 (1.2) | 112 (49.8) | 113 (50.2) | * | 82 (72.6) | 31 (27.4) | * |
| COPD | 226 (1.2) | 99 (43.8) | 127 (56.2) | * | 92 (72.4) | 35 (27.6) | * |
| Diabetes | 1378 (7.5) | 851 (61.8) | 527 (38.2) | * | 412 (78.2) | 115 (21.8) | * |
| History of Diabetes | 1518 (8.2) | 930 (61.3) | 588 (38.7) | * | 461 (78.4) | 127 (21.6) | * |
| Myocardial Infarction | 129 (0.7) | 41 (31.8) | 88 (68.2) | * | 72 (81.8) | 16 (18.2) | |
| Heart Failure | 247 (1.3) | 91 (36.8) | 156 (63.2) | * | 101 (64.7) | 55 (35.3) | * |
| Hypertension | 4211 (22.7) | 2861 (67.9) | 1350 (32.1) | * | 1093 (81) | 257 (19) | * |
| PVD | 219 (1.2) | 97 (44.3) | 122 (55.7) | * | 96 (78.7) | 26 (21.3) | * |
| Asthma | 1745 (9.4) | 1195 (68.5) | 550 (31.5) | * | 456 (82.9) | 94 (17.1) | * |
| CVA | 547 (3) | 257 (47) | 290 (53) | * | 212 (73.1) | 78 (26.9) | * |
| CPIC medications prescribed within 30 days prior to inpatient admission (n = 4404) | 3801/4404 (86.3) | 603/4404 (13.7) | |||||
| 1 or more gene-x-drug interactions with 1 or more CPIC medications prescribed within 30 days prior to inpatient admission | * | ||||||
| Absent | 2874 (88.5) | 373 (11.5) | |||||
| Present | 1246 (83.5) | 247 (16.5) | |||||
| Number of CPIC medications prescribed within 30 days prior to inpatient admission | * | ||||||
| 1 | 777 (92.4) | 64 (7.6) | |||||
| 2 | 1749 (92) | 152 (8) | |||||
| 3 | 620 (83.6) | 122 (16.4) | |||||
| 4 | 390 (80.7) | 93 (19.3) | |||||
| 5 or more | 265 (60.6) | 172 (39.4) | |||||
| Inpatient Admissions from 1 January 2010 to 31 December 2020 | |||||||
|---|---|---|---|---|---|---|---|
| Overall | No | Yes | Yes | ||||
| 4740 | |||||||
| 90-Day Hospital Readmissions | |||||||
| No | Yes | ||||||
| n (%) | 19,999 | 15,259 (76) | 4740 (24) | p-Value | 4120 (87) | 620 (13) | p-Value |
| Race by US median household income | 0.32 | <0.0001 | |||||
| White and below US median income | 706 (4.9) | 512 (72.5) | 194 (27.5) | 175 (90.2) | 19 (9.8) | ||
| White and above US median income | 13,241 (91) | 9769 (73.8) | 3472 (26.2) | 2995 (86.3) | 477 (13.7) | ||
| Black and below US median income | 137 (0.9) | 102 (74.5) | 35 (25.5) | 28 (80) | 7 (20) | ||
| Black and above US median income | 466 (3.2) | 327 (70.2) | 139 (29.8) | 102 (73.4) | 37 (26.6) | ||
| Number of comorbidities by race | <0.0001 | <0.0001 | |||||
| 0 and White | 8316 (60.3) | 6391 (76.9) | 1925 (23.1) | 1737 (90.2) | 188 (9.8) | ||
| 0 and Black | 268 (1.9) | 199 (74.3) | 69 (25.7) | 56 (81.2) | 13 (18.8) | ||
| 1 and White | 3164 (23) | 2254 (71.2) | 910 (28.8) | 786 (86.4) | 124 (13.6) | ||
| 1 and Black | 150 (1.1) | 112 (74.7) | 38 (25.3) | 29 (76.3) | 9 (23.7) | ||
| 2 and White | 891 (6.5) | 538 (60.4) | 353 (39.6) | 283 (80.2) | 70 (19.8) | ||
| 2 and Black | 60 (0.4) | 30 (50) | 30 (50) | 20 (66.7) | 10 (33.3) | ||
| 3+ and White | 850 (6.2) | 414 (48.7) | 436 (51.3) | 325 (74.5) | 111 (25.5) | ||
| 3+ and Black | 81 (0.6) | 47 (58) | 34 (42) | 22 (64.7) | 12 (35.3) | ||
| Number of comorbidities by US median household income | <0.0001 | <0.0001 | |||||
| 0 and ≤ $64,994 (below median) | 700 (3.8) | 563 (80.4) | 137 (19.6) | 126 (92) | 11 (8) | ||
| 0 and > $64,994 (above median) | 11,248 (61) | 8813 (78.4) | 2435 (21.6) | 2207 (90.6) | 228 (9.4) | ||
| 1 and ≤ $64,994 (below median) | 279 (1.5) | 203 (72.8) | 76 (27.2) | 65 (85.5) | 11 (14.5) | ||
| 1 and > $64,994 (above median) | 3884 (21) | 2865 (73.8) | 1019 (26.2) | 880 (86.4) | 139 (13.6) | ||
| 2 and ≤ $64,994 (below median) | 79 (0.4) | 47 (59.5) | 32 (40.5) | 29 (90.6) | 3 (9.4) | ||
| 2 and > $64,994 (above median) | 1117 (6.1) | 701 (62.8) | 416 (37.2) | 331 (79.6) | 85 (20.4) | ||
| 3+ and ≤ $64,994 (below median) | 100 (0.5) | 54 (54) | 46 (46) | 40 (87) | 6 (13) | ||
| 3+ and > $64,994 (above median) | 1046 (5.7) | 552 (52.8) | 494 (47.2) | 364 (73.7) | 130 (26.3) | ||
| Number of CPIC medications prescribed within 30 days before admission date by race | <0.0001 | ||||||
| 1 and White | 639 (17.9) | 589 (92.2) | 50 (7.8) | ||||
| 1 and Black | 30 (0.8) | 29 (96.7) | 1 (3.3) | ||||
| 2 and White | 1375 (38.5) | 1258 (91.5) | 117 (8.5) | ||||
| 2 and Black | 62 (1.7) | 49 (79) | 13 (21) | ||||
| 3 and White | 606 (17) | 507 (83.7) | 99 (16.3) | ||||
| 3 and Black | 28 (0.8) | 20 (71.4) | 8 (28.6) | ||||
| 4 and White | 407 (11.4) | 328 (80.6) | 79 (19.4) | ||||
| 4 and Black | 18 (0.5) | 11 (61.1) | 7 (38.9) | ||||
| 5+ and White | 390 (10.9) | 247 (63.3) | 143 (36.7) | ||||
| 5+ and Black | 19 (0.5) | 7 (36.8) | 12 (63.2) | ||||
| Number of CPIC medications prescribed within 30 days before admission date by US median household income | <0.0001 | ||||||
| 1 and ≤ $64,994 (below median) | 57 (1.3) | 53 (93) | 4 (7) | ||||
| 1 and > $64,994 (above median) | 782 (17.8) | 723 (92.5) | 59 (7.5) | ||||
| 2 and ≤ $64,994 (below median) | 111 (2.5) | 105 (94.6) | 6 (5.4) | ||||
| 2 and > $64,994 (above median) | 1789 (40.7) | 1643 (91.8) | 146 (8.2) | ||||
| 3 and ≤ $64,994 (below median) | 40 (0.9) | 37 (92.5) | 3 (7.5) | ||||
| 3 and > $64,994 (above median) | 702 (16) | 583 (83) | 119 (17) | ||||
| 4 and ≤ $64,994 (below median) | 34 (0.8) | 27 (79.4) | 7 (20.6) | ||||
| 4 and > $64,994 (above median) | 448 (10.2) | 362 (80.8) | 86 (19.2) | ||||
| 5+ and ≤ $64,994 (below median) | 31 (0.7) | 23 (74.2) | 8 (25.8) | ||||
| 5+ and > $64,994 (above median) | 406 (9.2) | 242 (59.6) | 164 (40.4) | ||||
| No 90-Day Readmission | 90-Day Readmission | |||||
|---|---|---|---|---|---|---|
| CPIC Medications Ordered within 30 Days of Inpatient Admission (n = 4404) | n = 3801 | n = 603 | ||||
| 1 or more Gene-x-Drug Interactions | Absent | Present | Absent | Present | ||
| n (%) | 2555 (67) | 1246 (33) | p-Value | 356 (59) | 247 (41) | p-Value |
| Race | <0.0001 | 0.70 | ||||
| White | 1898 (64.8) | 1031 (35.2) | 284 (58.2) | 204 (41.8) | ||
| Black or African American | 86 (74.1) | 30 (25.9) | 24 (58.5) | 17 (41.5) | ||
| Asian | 196 (81.7) | 44 (18.3) | 10 (58.8) | 7 (41.2) | ||
| American Indian or Alaska Native | 6 (75) | 2 (25) | 1 (100) | 0 (0) | ||
| Pacific Islander/Hawaiian Native | 1 (50) | 1 (50) | 0 (0) | 0 (0) | ||
| Other | 355 (72.3) | 136 (27.7) | 35 (64.8) | 19 (35.2) | ||
| Ethnicity | 0.12 | 0.12 | ||||
| Hispanic/Latino | 133 (72.7) | 50 (27.3) | 20 (76.9) | 6 (23.1) | ||
| Non-Hispanic | 2405 (66.9) | 1192 (33.1) | 335 (58.2) | 241 (41.8) | ||
| uOR (95% CI) | p-Value | aOR (95% CI) | p-Value | |
|---|---|---|---|---|
| Age Group | ||||
| 18–39 | Reference | Reference | ||
| 40–49 | 1.05 (0.75–1.47) | 0.001 | 1.04 (0.74–1.47) | 0.529 |
| 50–64 | 1.73 (1.27–2.35) | 0.026 | 1.28 (0.93–1.78) | 0.104 |
| 65 or above | 2.35 (1.77–3.12) | <0.0001 | 1.14 (0.80–1.65) | 0.783 |
| Gender | ||||
| Female | Reference | Reference | ||
| Male | 1.47 (1.21–1.80) | 0.0001 | 1.11 (0.89–1.38) | 0.371 |
| Race * | ||||
| White | Reference | Reference | ||
| Black/African American | 2.12 (1.47–3.07) | <0.0001 | 2.12 (1.42–3.17) | <0.0001 |
| Asian | 0.43 (0.26–0.70) | <0.0001 | 0.62 (0.37–1.03) | 0.002 |
| Ethnicity | ||||
| Non-Hispanic | Reference | |||
| Hispanic/Latino | 1.10 (0.54–2.26) | 0.975 | ||
| Marital status | ||||
| Unmarried | Reference | - | - | |
| Married | 0.60 (0.49–0.72) | 0.441 | ||
| Employment status ** | ||||
| Employed | Reference | Reference | ||
| Unemployed | 2.19 (1.82–2.64) | <0.0001 | 1.74 (1.39–2.18) | 0.007 |
| Insurance status | ||||
| Commercial | Reference | Reference | ||
| Government | 1.81 (1.50–2.20) | 0.307 | 1.04 (0.81–1.34) | 0.6605 |
| Out-of-pocket (self-pay) | 1.67 (0.47–5.90) | 0.736 | 1.48 (0.41–5.32) | 0.5742 |
| Median household income in relation to US median household income *** | ||||
| Less than $64,994 | Reference | Reference | ||
| $64,994 or more | 1.33 (0.86–2.05) | 0.203 | 1.63 (1.03–2.58) | 0.035 |
| BMI, range 13.3–79.2 | 1.03 (1.02–1.04) | <0.0001 | 1.01 (1.00–1.03) | 0.050 |
| Smoking status | ||||
| No | Reference | Reference | ||
| Yes | 1.38 (0.87–2.18) | 0.176 | 1.26 (0.78–2.04) | 0.347 |
| COVID status | ||||
| Yes vs. No | 0.56 (0.17–1.84) | 0.341 | ||
| Number of comorbidities **** | ||||
| 0 | Reference | Reference | ||
| 1 | 1.57 (1.24–1.98) | 0.018 | 1.28 (0.99–1.64) | 0.044 |
| 2 | 2.54 (1.91–3.39) | 0.006 | 1.83 (1.33–2.52) | 0.070 |
| 3 or more | 3.36 (2.61–4.32) | <0.0001 | 2.23 (1.66–3.02) | <0.0001 |
| Number of CPIC medications prescribed within 30 days prior to inpatient admission | ||||
| 1 | Reference | |||
| 2 | 1.14 (0.82–1.58) | <0.0001 | - | - |
| 3 | 2.50 (1.77–3.53) | 0.417 | - | - |
| 4 | 3.07 (2.13–4.41) | 0.008 | - | - |
| 5 or more | 7.66 (5.45–10.77) | <0.0001 | - | - |
| Gene-x-drug interactions within 30 days prior to inpatient admission | ||||
| Absent | Reference | Reference | ||
| Present | 1.41 (1.18–1.70) | 0.0002 | 1.31 (1.08–1.59) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saulsberry, L.; Singh, L.; Pruitt, J.; Ward, C.; Wake, D.T.; Gibbons, R.D.; Meltzer, D.O.; O’Donnell, P.H.; Cruz-Knight, W.; Hulick, P.J.; et al. Effect Modification by Social Determinants of Pharmacogenetic Medication Interactions on 90-Day Hospital Readmissions within an Integrated U.S. Healthcare System. J. Pers. Med. 2022, 12, 1145. https://doi.org/10.3390/jpm12071145
Saulsberry L, Singh L, Pruitt J, Ward C, Wake DT, Gibbons RD, Meltzer DO, O’Donnell PH, Cruz-Knight W, Hulick PJ, et al. Effect Modification by Social Determinants of Pharmacogenetic Medication Interactions on 90-Day Hospital Readmissions within an Integrated U.S. Healthcare System. Journal of Personalized Medicine. 2022; 12(7):1145. https://doi.org/10.3390/jpm12071145
Chicago/Turabian StyleSaulsberry, Loren, Lavisha Singh, Jaclyn Pruitt, Christopher Ward, Dyson T. Wake, Robert D. Gibbons, David O. Meltzer, Peter H. O’Donnell, Wanda Cruz-Knight, Peter J. Hulick, and et al. 2022. "Effect Modification by Social Determinants of Pharmacogenetic Medication Interactions on 90-Day Hospital Readmissions within an Integrated U.S. Healthcare System" Journal of Personalized Medicine 12, no. 7: 1145. https://doi.org/10.3390/jpm12071145