
Changes in the Incidence Rates of Gastrointestinal Diseases Due to the COVID-19 Pandemic in South Korea: A Long-Term Perspective

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants and Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, K.H.; Kim, S.B.; Kim, T.N. Changes in endoscopic patterns before and during COVID-19 outbreak: Experience at a single tertiary center in Korean. World J. Clin. Cases 2021, 9, 3576–3585. [Google Scholar] [CrossRef] [PubMed]
- Chiriac, S.; Stanciu, C.; Cojocariu, C.; Sfarti, C.; Singeap, A.M.; Girleanu, I.; Cuciureanu, T.; Huiban, L.; David, D.; Zenovia, S.; et al. The impact of the COVID-19 pandemic on gastrointestinal endoscopy activity in a tertiary care center from Northeastern Romania. Healthcare 2021, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- Dighe, A.; Cattarino, L.; Cuomo-Dannenburg, G.; Skarp, J.; Imai, N.; Bhatia, S.; Gaythorpe, K.A.M.; Ainslie, K.E.C.; Baguelin, M.; Bhatt, S.; et al. Response to COVID-19 in South Korea and implications for lifting stringent interventions. BMC Med. 2020, 18, 321. [Google Scholar] [CrossRef] [PubMed]
- Aiello, A.E.; Murray, G.F.; Perez, V.; Coulborn, R.M.; Davis, B.M.; Uddin, M.; Shay, D.K.; Waterman, S.H.; Monto, A.S. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: A randomized intervention trial. J. Infect. Dis. 2010, 201, 491–498. [Google Scholar] [CrossRef] [Green Version]
- Mun, S.K.; Yang, B.R.; Chang, M. Changes in respiratory diseases in South Korea during the COVID-19 pandemic: An interrupted time series study. BMJ Glob. Health 2021, 6, e006912. [Google Scholar] [CrossRef]
- Yoo, I.H.; Kang, H.M.; Jeong, D.C. Changes in the incidence of intussusception and infectious diseases after the COVID-19 Pandemic in Korea. J. Korean Med. Sci. 2022, 37, e60. [Google Scholar] [CrossRef]
- Huang, Q.S.; Wood, T.; Jelley, L.; Jennings, T.; Jefferies, S.; Daniells, K.; Nesdale, A.; Dowell, T.; Turner, N.; Campbell-Stokes, P.; et al. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat. Commun. 2021, 12, 1001. [Google Scholar] [CrossRef]
- Liu, P.; Xu, M.; Cao, L.; Su, L.; Lu, L.; Dong, N.; Jia, R.; Zhu, X.; Xu, J. Impact of COVID-19 pandemic on the prevalence of respiratory viruses in children with lower respiratory tract infections in China. Virol. J. 2021, 18, 159. [Google Scholar] [CrossRef]
- Tempia, S.; Walaza, S.; Bhiman, J.N.; McMorrow, M.L.; Moyes, J.; Mkhencele, T.; Meiring, S.; Quan, V.; Bishop, K.; McAnerney, J.M.; et al. Decline of influenza and respiratory syncytial virus detection in facility-based surveillance during the COVID-19 pandemic, South Africa, January to October 2020. Eurosurveillance 2021, 26, 2001600. [Google Scholar] [CrossRef]
- Lee, K.H.; Yon, D.K.; Suh, D.I. Prevalence of allergic diseases among Korean adolescents during the COVID-19 pandemic: Comparison with pre-COVID-19 11-year trends. Eur. Rev. Med. Pharm. Sci. 2022, 26, 2556–2568. [Google Scholar] [CrossRef]
- Ielpo, B.; Prieto, M.; Ortega, I.; Balibrea, J.M.; Rubio-Perez, I.; Juvany, M.; Gomez-Bravo, M.A.; Ramia, J.M. National survey on the treatment of cholelitiasis in Spain during the initial period of the COVID-19 pandemic. Cir. Esp. 2021, 99, 346–353. [Google Scholar] [CrossRef]
- Lisi, G.; Campanelli, M.; Grande, S.; Milito, G.; Grande, M. Sclerotherapy with 3% polidocanol foam for third- and fourth-degree hemorrhoids as “bridge treatment” during the COVID-19 pandemic in Italy. Int. J. Colorectal Dis. 2021, 36, 1321–1322. [Google Scholar] [CrossRef]
- Seo, S.; Suda, K.; Kato, H.; Abe, E.; Kosaka, S.; Fujiwara, K.; Ochi, T.; Koga, H.; Urao, M.; Okazaki, T.; et al. Decreased incidence of intussusception during the COVID-19 pandemic. Trends in pediatric surgical emergencies. Pediatr. Surg. Int. 2021, 37, 1761–1764. [Google Scholar] [CrossRef]
- Ahn, S.Y.; Park, J.Y.; Lim, I.S.; Chae, S.A.; Yun, S.W.; Lee, N.M.; Kim, S.Y.; Choi, B.S.; Yi, D.Y. Changes in the occurrence of gastrointestinal infections after COVID-19 in Korea. J. Korean Med. Sci. 2021, 36, e180. [Google Scholar] [CrossRef]
- Velez, C.; Paz, M.; Silvernale, C.; Stratton, L.W.; Kuo, B.; Staller, K.; Suffolk County, C.-G.S.A. Factors associated with chronic de novo post-coronavirus disease gastrointestinal disorders in a metropolitan US County. Clin. Gastroenterol. Hepatol. 2021, 20, e1488–e1492. [Google Scholar] [CrossRef]
- Nordstokke, D.W.; Zumbo, B.D. A New Nonparametric Levene Test for Equal Variances. Psicológica 2010, 31, 401–430. [Google Scholar]
- Monteleone, G.; Ardizzone, S. Are patients with inflammatory bowel disease at increased risk for COVID-19 infection? J. Crohns Colitis 2020, 14, 1334–1336. [Google Scholar] [CrossRef]
- Jeong, G.H.; Lee, H.J.; Lee, J.; Lee, J.Y.; Lee, K.H.; Han, Y.J.; Yoon, S.; Ryu, S.; Kim, D.K.; Park, M.B.; et al. Effective control of COVID-19 in South Korea: Cross-sectional study of epidemiological data. J. Med. Internet Res. 2020, 22, e22103. [Google Scholar] [CrossRef]
- Goodday, S.M.; Travis, S.; Walsh, A.; Friend, S.H. Stress-related consequences of the coronavirus disease 2019 pandemic on symptoms of Crohn’s disease. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1511–1516. [Google Scholar] [CrossRef]
- Shiga, H.; Miyazawa, T.; Kinouchi, Y.; Takahashi, S.; Tominaga, G.; Takahashi, H.; Takagi, S.; Obana, N.; Kikuchi, T.; Oomori, S.; et al. Life-event stress induced by the Great East Japan Earthquake was associated with relapse in ulcerative colitis but not Crohn’s disease: A retrospective cohort study. BMJ Open 2013, 3, e002294. [Google Scholar] [CrossRef]
- Kaufman, K.R.; Petkova, E.; Bhui, K.S.; Schulze, T.G. A global needs assessment in times of a global crisis: World psychiatry response to the COVID-19 pandemic. BJPsych Open 2020, 6, e48. [Google Scholar] [CrossRef]
- Lee, S.Y.; Ro, Y.S.; Jeong, J.; Shin, S.D.; Moon, S. Impact of the COVID-19 Pandemic on the incidence and characteristics of patients with psychiatric illnesses visiting emergency departments in Korea. J. Clin. Med. 2022, 11, 488. [Google Scholar] [CrossRef]
- Portincasa, P.; Molina-Molina, E.; Garruti, G.; Wang, D.Q. Critical care aspects of gallstone disease. J. Crit. Care Med. 2019, 5, 6–18. [Google Scholar] [CrossRef] [Green Version]
- Ong, J.S.; Gharahkhani, P.; Vaughan, T.L.; Whiteman, D.; Kendall, B.J.; MacGregor, S. Assessing the genetic relationship between gastro-esophageal reflux disease and risk of COVID-19 infection. Hum. Mol. Genet. 2022, 31, 471–480. [Google Scholar] [CrossRef]
- Sikavi, D.R.; Cai, J.X.; Leung, R.; Carroll, T.L.; Chan, W.W. Impaired proximal esophageal contractility predicts pharyngeal reflux in patients with laryngopharyngeal reflux symptoms. Clin. Transl. Gastroenterol. 2021, 12, e00408. [Google Scholar] [CrossRef]
- Konturek, P.C.; Brzozowski, T.; Konturek, S.J. Stress and the gut: Pathophysiology, clinical consequences, diagnostic approach and treatment options. J. Physiol. Pharm. 2011, 62, 591–599. [Google Scholar]
- Hu, P.; Samuels, S.; Maciejewski, K.R.; Li, F.; Aloe, C.; Name, M.V.; Savoye, M.; Sharifi, M. Changes in weight-related health behaviors and social determinants of health among youth with overweight/obesity during the COVID-19 Pandemic. Child. Obes. 2021; ahead of print. [Google Scholar] [CrossRef]
- Jaehn, P.; Holmberg, C.; Uhlenbrock, G.; Pohl, A.; Finkenzeller, T.; Pawlik, M.T.; Quack, I.; Ernstberger, A.; Rockmann, F.; Schreyer, A.G. Differential trends of admissions in accident and emergency departments during the COVID-19 pandemic in Germany. BMC Emerg. Med. 2021, 21, 42. [Google Scholar] [CrossRef]
- Prieto, M.; Ortega, I.; Balibrea, J.M.; Ielpo, B. Management of cholelithiasis in times of COVID-19: A challenge for the system. Cir. Esp. 2021, 99, 699–700. [Google Scholar] [CrossRef]
- Quek, S.X.Z.; Loo, E.X.L.; Demutska, A.; Chua, C.E.; Kew, G.S.; Wong, S.; Lau, H.X.; Low, E.X.S.; Loh, T.L.; Lung, O.S.; et al. Impact of the coronavirus disease 2019 pandemic on irritable bowel syndrome. J. Gastroenterol. Hepatol. 2021, 36, 2187–2197. [Google Scholar] [CrossRef]
- Sabate, J.M.; Deutsch, D.; Melchior, C.; Entremont, A.; Mion, F.; Bouchoucha, M.; Facon, S.; Raynaud, J.J.; Zerbib, F.; Jouet, P. COVID-19 pandemic and lockdown stress consequences in people with and without Irritable Bowel Syndrome. Ethics Med. Public Health 2021, 18, 100660. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, L.; McCarthy, J.; Kelly, P.; Hurley, G.; Luo, F.; Chen, K.; O’Sullivan, G.C.; Kiely, B.; Collins, J.K.; Shanahan, F.; et al. Lactobacillus and bifidobacterium in irritable bowel syndrome: Symptom responses and relationship to cytokine profiles. Gastroenterology 2005, 128, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Oshima, T.; Siah, K.T.H.; Yoshimoto, T.; Miura, K.; Tomita, T.; Fukui, H.; Miwa, H. Impacts of the COVID-19 pandemic on functional dyspepsia and irritable bowel syndrome: A population-based survey. J. Gastroenterol. Hepatol. 2021, 36, 1820–1827. [Google Scholar] [CrossRef] [PubMed]
- Yawar, B.; Marzouk, A.; Ali, H.; Asim, A.; Ghorab, T.; Bahli, Z.; Abousamra, M.; Fleville, S. Acute pancreatitis during COVID-19 pandemic: An overview of patient demographics, disease severity, management and outcomes in an acute district hospital in Northern Ireland. Cureus 2021, 13, e18520. [Google Scholar] [CrossRef]
- Baral, S.; Chhetri, R.K.; Thapa, N. Comparison of acute appendicitis before and within lockdown period in COVID-19 era: A retrospective study from rural Nepal. PLoS ONE 2021, 16, e0245137. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, D.W. Does the clinical spectrum of Coronavirus Disease 2019 (COVID-19) show regional differences? Clin. Exp. Otorhinolaryngol. 2020, 13, 83–84. [Google Scholar] [CrossRef]
- Park, J.H.; Jang, W.; Kim, S.W.; Lee, J.; Lim, Y.S.; Cho, C.G.; Park, S.W.; Kim, B.H. The clinical manifestations and chest computed tomography findings of Coronavirus Disease 2019 (COVID-19) patients in China: A proportion meta-analysis. Clin. Exp. Otorhinolaryngol. 2020, 13, 95–105. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Diseases | Before COVID-19 | During COVID-19 | p-Values of Difference | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | Variance † | |
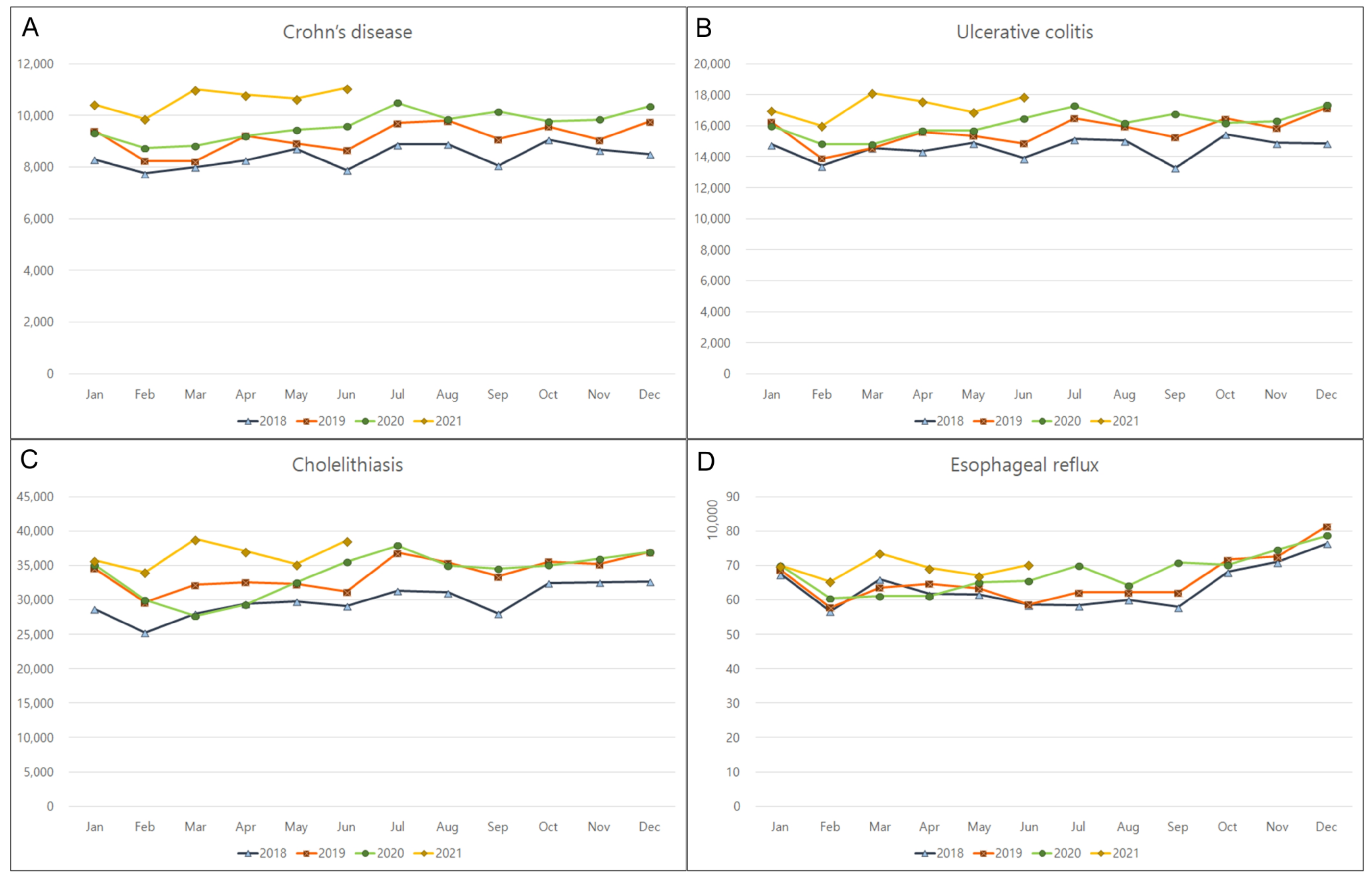
| Cholelithiasis | 31,908.2 | 2980.4 | 34,999.7 | 3053.7 | 0.003 * | 0.842 |
| Pancreatitis | 9376.2 | 487.7 | 9397.0 | 562.6 | 0.786 | 0.952 |
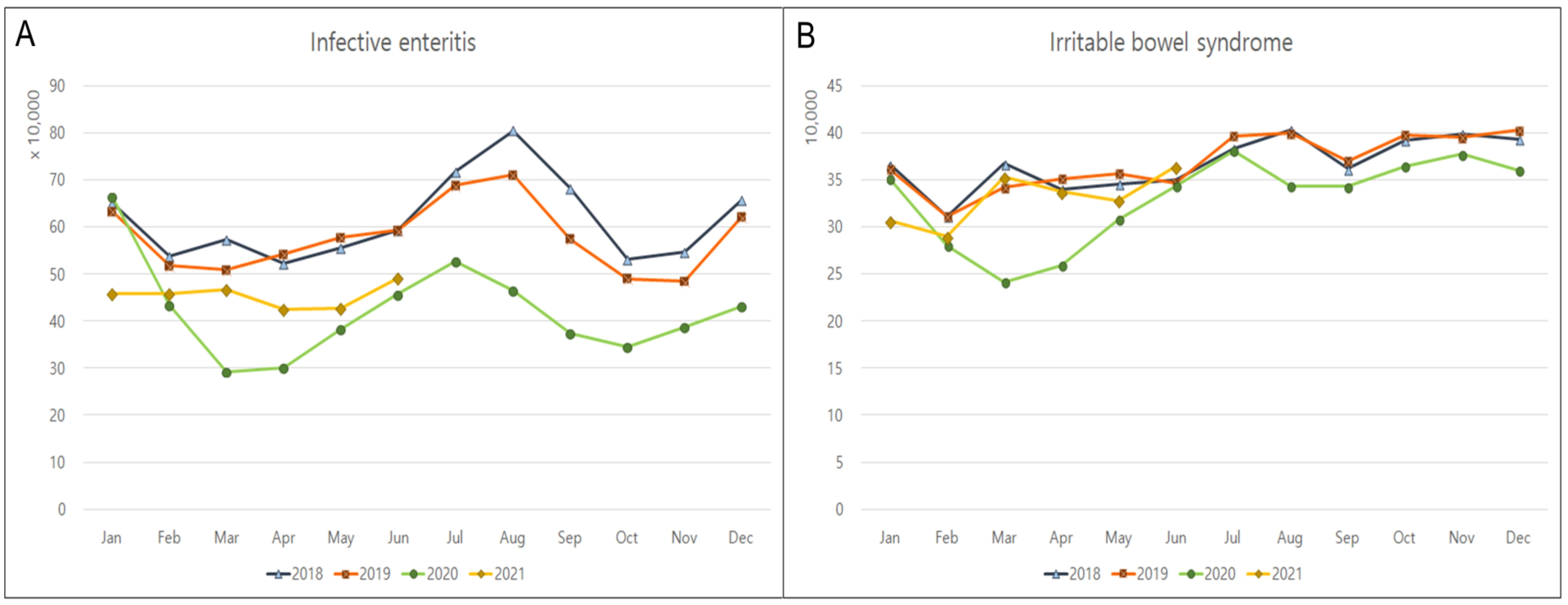
| Infective enteritis | 592,974.9 | 86,207.8 | 418,206.6 | 66,354.2 | <0.001 * | 0.117 |
| Crohn’s disease | 8799.0 | 595.7 | 10,087.6 | 644.9 | <0.001 * | 0.268 |
| Ulcerative colitis | 15,125.1 | 946.1 | 16,638.8 | 889.8 | <0.001 * | 0.501 |
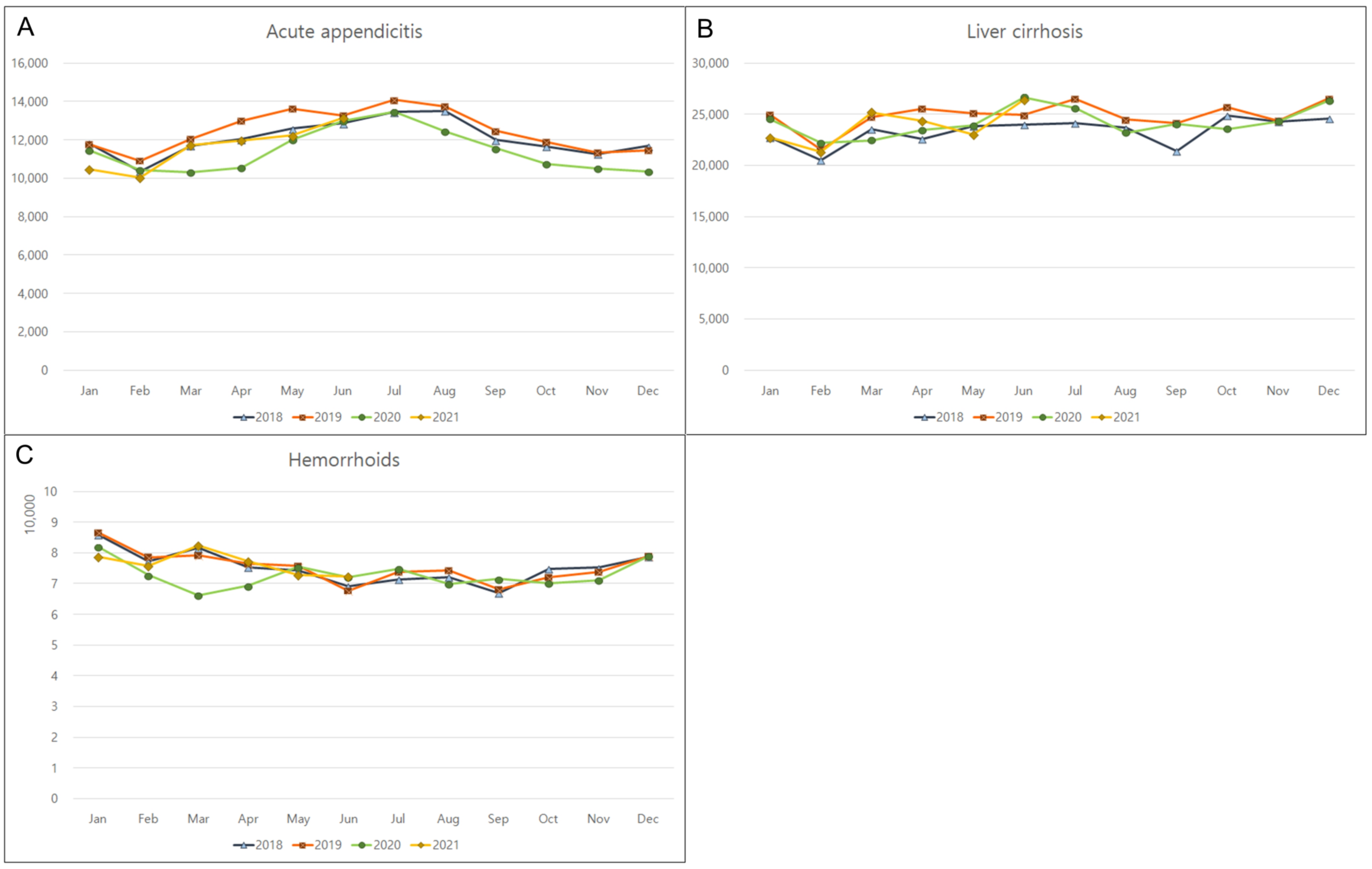
| Acute appendicitis | 12,173.0 | 1016.7 | 11,537.4 | 1127.0 | 0.100 | 0.506 |
| Liver cirrhosis | 24,059.7 | 1490.0 | 24,171.6 | 1535.7 | 0.816 | 0.559 |
| Esophageal reflux | 647,717.8 | 62,784.3 | 685,385.2 | 47,978.9 | 0.030 * | 0.141 |
| Hemorrhoids | 75,509.2 | 5076.9 | 73,697.4 | 4252.5 | 0.300 | 0.988 |
| Irritable bowel syndrome | 364,276.6 | 31,985.2 | 331,089.3 | 40,512.7 | 0.007 * | 0.499 |
| Diseases | Before COVID-19 | During COVID-19 | p-Values of Difference | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | Variance † | |
| Men | ||||||
| Cholelithiasis | 15,126.3 | 1399.4 | 16,671.3 | 1336.0 | 0.002 * | 0.901 |
| Pancreatitis | 6460.2 | 326.1 | 6424.1 | 352.6 | 0.698 | 0.990 |
| Infective enteritis | 280,916.2 | 42,954.1 | 195,956.6 | 32,499.2 | <0.001 * | 0.109 |
| Crohn’s disease | 6170.8 | 426.8 | 7138.8 | 468.1 | <0.001 * | 0.187 |
| Ulcerative colitis | 9028.5 | 554.6 | 9952.4 | 508.6 | <0.001 * | 0.282 |
| Acute appendicitis | 6292.9 | 508.5 | 5951.8 | 554.3 | 0.070 | 0.342 |
| Liver cirrhosis | 14,234.9 | 830.9 | 14,091.3 | 858.3 | 0.338 | 0.672 |
| Esophageal reflux | 274,281.2 | 29,925.5 | 287,298.8 | 22,815.4 | 0.049 * | 0.141 |
| Hemorrhoids | 39,706.4 | 2771.5 | 38,089.9 | 2122.7 | 0.055 | 0.674 |
| Irritable bowel syndrome | 170,369.7 | 16,209.7 | 153,845.9 | 19,914.3 | 0.011 * | 0.866 |
| Women | ||||||
| Cholelithiasis | 16,781.9 | 1598.0 | 18,328.4 | 1739.5 | 0.005 * | 0.942 |
| Pancreatitis | 2935.6 | 173.7 | 2972.9 | 216.8 | 0.453 | 0.211 |
| Infective enteritis | 312,058.7 | 43,398.8 | 222,250.1 | 33,911.1 | <0.001 * | 0.103 |
| Crohn’s disease | 2628.3 | 176.0 | 2948.8 | 182.7 | <0.001 * | 0.459 |
| Ulcerative colitis | 6096.6 | 396.8 | 6686.4 | 391.3 | <0.001 * | 0.579 |
| Acute appendicitis | 5880.1 | 518.6 | 5585.6 | 580.9 | 0.178 | 0.499 |
| Liver cirrhosis | 9824.8 | 667.1 | 10,080.3 | 699.2 | 0.468 | 0.550 |
| Esophageal reflux | 373,436.5 | 33,381.3 | 398,086.4 | 25,737.6 | 0.013 * | 0.276 |
| Hemorrhoids | 35,802.8 | 2341.0 | 35,607.6 | 2195.4 | 0.816 | 0.878 |
| Irritable bowel syndrome | 193,907.0 | 16,213.5 | 177,243.3 | 20,934.0 | 0.004 * | 0.451 |
| Diseases | Before COVID-19 | During COVID-19 | p-Values of Difference | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | Variance | |
| Age 0–19 years old | ||||||
| Cholelithiasis | 126.0 | 17.4 | 129.3 | 18.3 | 0.364 | 0.469 |
| Pancreatitis | 154.9 | 24.2 | 150.4 | 24.4 | 0.907 | 0.140 |
| Infective enteritis | 253,267.9 | 43,009.3 | 148,682.7 | 36,095.9 | <0.001 * | 0.076 |
| Crohn’s disease | 1198.3 | 72.2 | 1391.4 | 139.5 | <0.001 * | 0.905 |
| Ulcerative colitis | 510.6 | 40.3 | 506.8 | 34.0 | 0.907 | 0.923 |
| Acute appendicitis | 2668.0 | 334.7 | 2128.2 | 321.7 | <0.001 * | 0.211 |
| Liver cirrhosis | 21.9 | 6.5 | 20.1 | 3.6 | 0.194 | 0.010 † |
| Esophageal reflux | 18,068.5 | 2626.0 | 18,186.0 | 4486.2 | 0.816 | 0.003 † |
| Hemorrhoids | 2165.0 | 283.3 | 1941.1 | 166.7 | 0.004 * | 0.895 |
| Irritable bowel syndrome | 59,571.1 | 9637.7 | 44,838.4 | 9480.1 | <0.001 * | 0.173 |
| Age 20–59 years old | ||||||
| Cholelithiasis | 14,874.7 | 1467.3 | 15,915.9 | 1463.0 | 0.026 * | 0.754 |
| Pancreatitis | 5609.0 | 257.6 | 5393.8 | 278.6 | 0.008 * | 0.680 |
| Infective enteritis | 249,570.0 | 40,599.1 | 189,414.1 | 29,746.8 | <0.001 * | 0.428 |
| Crohn’s disease | 6928.2 | 491.9 | 7876.1 | 456.5 | <0.001 * | 0.272 |
| Ulcerative colitis | 10,469.3 | 628.4 | 11,397.7 | 578.1 | <0.001 * | 0.651 |
| Acute appendicitis | 7431.3 | 626.9 | 7214.0 | 664.0 | 0.319 | 0.183 |
| Liver cirrhosis | 10,709.2 | 537.2 | 9589.1 | 678.8 | <0.001 * | 0.296 |
| Esophageal reflux | 353,522.5 | 41,252.4 | 362,350.3 | 27,233.5 | 0.147 | 0.008 † |
| Hemorrhoids | 54,427.3 | 3560.4 | 51,725.9 | 2417.1 | 0.013 * | 0.510 |
| Irritable bowel syndrome | 163,525.9 | 18,245.6 | 143,566.3 | 20,468.9 | 0.004 * | 0.861 |
| Age 60+ years old | ||||||
| Cholelithiasis | 16,934.4 | 1563.0 | 18,987.3 | 1649.2 | <0.001 * | 0.848 |
| Pancreatitis | 3639.8 | 257.5 | 3861.1 | 289.1 | 0.013 * | 0.365 |
| Infective enteritis | 90,246.6 | 8755.6 | 80,201.4 | 8146.2 | 0.003 * | 0.575 |
| Crohn’s disease | 680.1 | 67.3 | 829.5 | 78.0 | <0.001 * | 0.191 |
| Ulcerative colitis | 4156.8 | 313.8 | 4748.4 | 312.2 | <0.001 * | 0.163 |
| Acute appendicitis | 2086.7 | 149.7 | 2209.4 | 203.7 | 0.076 | 0.312 |
| Liver cirrhosis | 13,350.0 | 1051.1 | 14,581.4 | 1014.7 | 0.001 * | 0.701 |
| Esophageal reflux | 276,550.2 | 24,140.3 | 305,290.8 | 21,752.4 | 0.001 * | 0.405 |
| Hemorrhoids | 19,012.7 | 1777.7 | 20,122.5 | 2018.1 | 0.120 | 0.916 |
| Irritable bowel syndrome | 141,340.6 | 9617.7 | 142,834.1 | 13,519.3 | 0.365 | 0.100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, H.G.; Kang, H.S.; Lim, H.; Kim, J.-H.; Kim, J.H.; Cho, S.-J.; Nam, E.S.; Min, K.-W.; Park, H.Y.; Kim, N.Y.; et al. Changes in the Incidence Rates of Gastrointestinal Diseases Due to the COVID-19 Pandemic in South Korea: A Long-Term Perspective. J. Pers. Med. 2022, 12, 1144. https://doi.org/10.3390/jpm12071144
Choi HG, Kang HS, Lim H, Kim J-H, Kim JH, Cho S-J, Nam ES, Min K-W, Park HY, Kim NY, et al. Changes in the Incidence Rates of Gastrointestinal Diseases Due to the COVID-19 Pandemic in South Korea: A Long-Term Perspective. Journal of Personalized Medicine. 2022; 12(7):1144. https://doi.org/10.3390/jpm12071144
Chicago/Turabian StyleChoi, Hyo Geun, Ho Suk Kang, Hyun Lim, Joo-Hee Kim, Ji Hee Kim, Seong-Jin Cho, Eun Sook Nam, Kyueng-Whan Min, Ha Young Park, Nan Young Kim, and et al. 2022. "Changes in the Incidence Rates of Gastrointestinal Diseases Due to the COVID-19 Pandemic in South Korea: A Long-Term Perspective" Journal of Personalized Medicine 12, no. 7: 1144. https://doi.org/10.3390/jpm12071144