
Autonomic Dysfunction and Management after Spinal Cord Injury: A Narrative Review


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
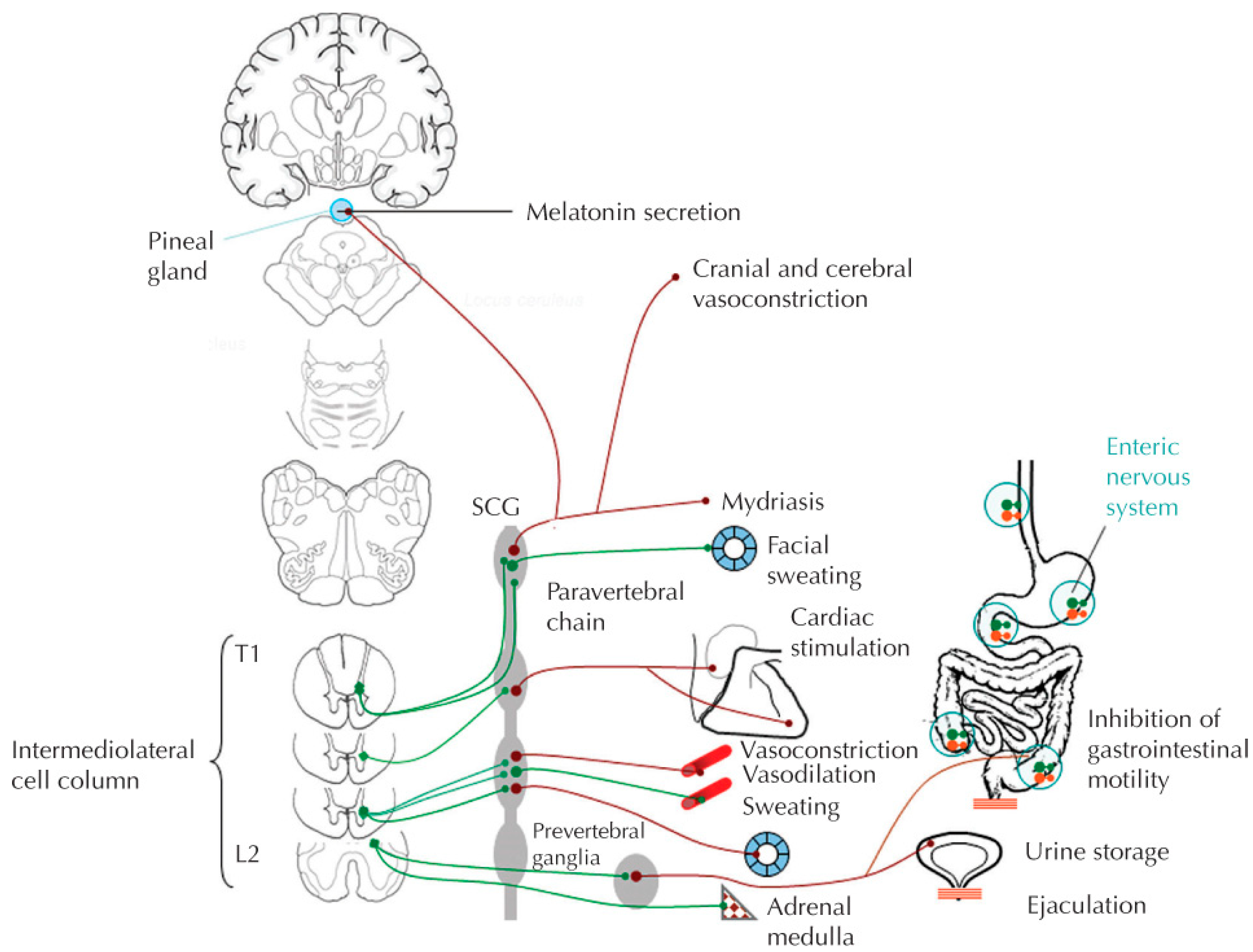
2. Sympathetic Nervous System
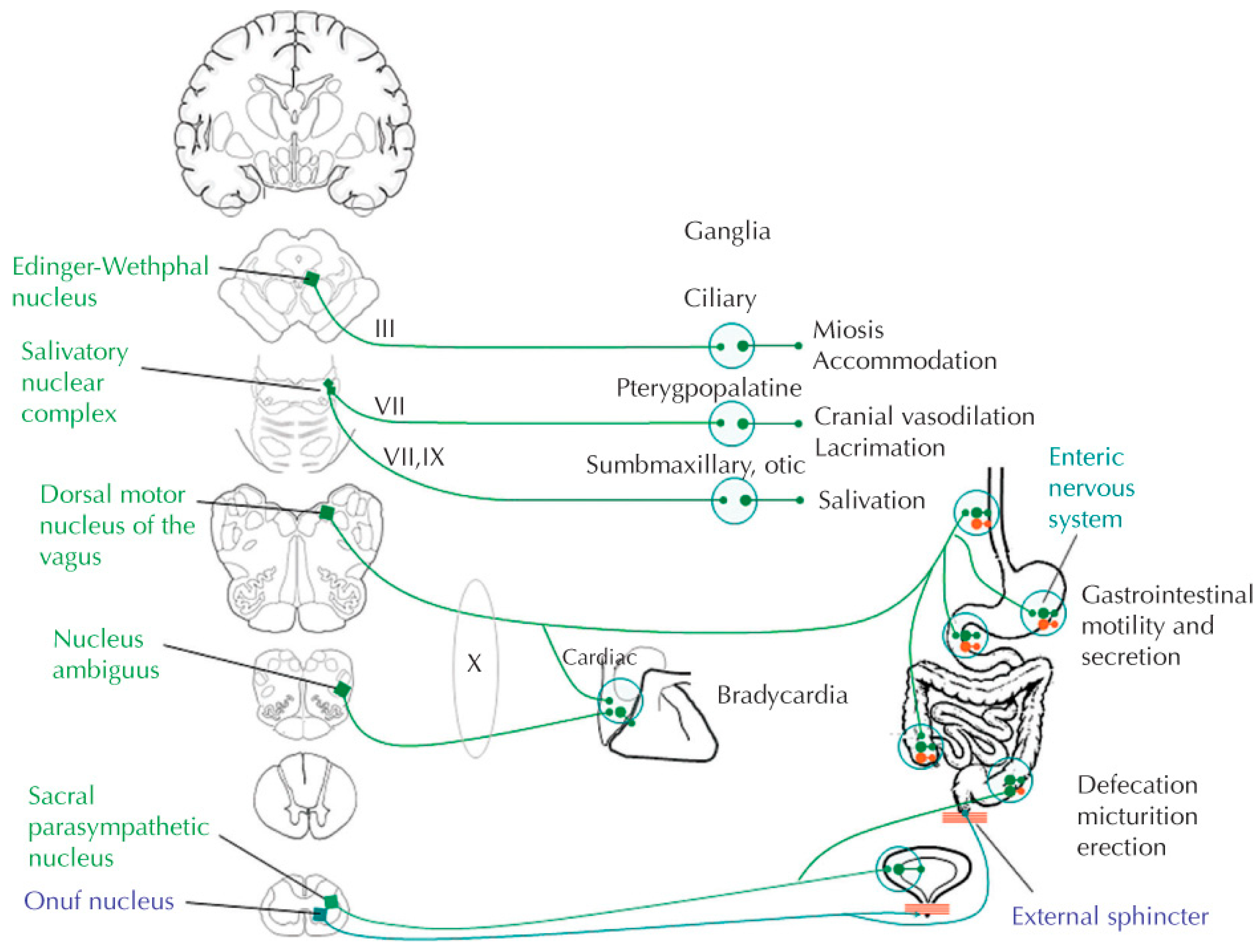
3. Parasympathetic Nervous System (PNS)
4. Mechanism of SCI: Emerging from Neurogenic Shock
5. SCI Influence on ANS Dysfunction
5.1. Cardiovascular Dysfunction
5.2. Thermoregulatory Dysfunction
5.3. Respiratory
5.4. Genitourinary Dysfunction
5.5. Gastrointestinal Dysfunction
5.6. Diagnosing Autonomic Dysfunction
6. Management of Autonomic Dysfunction after SCI
6.1. Cardiovascular Management
6.2. Managing Autonomic Dysreflexia
6.3. Thermodysregulation
6.4. Managing Hyperhidrosis
6.5. Managing Genitourinary and Gastrointestinal Dysfunction
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ANS | autonomic nervous system |
| AD | autonomic dysreflexia |
| ISAFSCI | International Standards to Determine Remaining Autonomic Function after Spinal Cord Injury |
| INCSCI | International Standards for Neurological Classification of Spinal Cord Injury |
| NOH | neurogenic orthostatic hypotension |
| PNS | parasympathetic nervous system |
| SCI | spinal cord injury |
| SNS | sympathetic nervous system |
| SSR | sympathetic skin response |
References
- Benarroch, E.E. Physiology and Pathophysiology of the Autonomic Nervous System. Continuum (Minneap Minn). CONTINUUM Lifelong Learn. Neurol. 2020, 26, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Wecht, J.M.; Krassioukov, A.V.; Alexander, M.; Handrakis, J.P.; McKenna, S.L.; Kennelly, M.; Trbovich, M.; Biering-Sorensen, F.; Burns, S.; Elliott, S.L.; et al. International Standards to document Autonomic Function following SCI (ISAFSCI): Second Edition. Top. Spinal Cord Inj. Rehabil. 2021, 27, 23–49. [Google Scholar] [CrossRef] [PubMed]
- Hakim, S.; Gaglani, T.; Cash, B.D. Neurogenic Bowel Dysfunction: The Impact of the Central Nervous System in Constipation and Fecal Incontinence. Gastroenterol. Clin. N. Am. 2022, 51, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Johns, J.; Krogh, K.; Rodriguez, G.M.; Eng, J.; Haller, E.; Heinen, M.; Laredo, R.; Longo, W.; Montero-Colon, W.; Korsten, M. Management of Neurogenic Bowel Dysfunction in Adults after Spinal Cord Injury: Clinical Practice Guideline for Healthcare Providers. J. Spinal Cord Med. 2021, 44, 442–510. [Google Scholar] [CrossRef] [PubMed]
- Krassioukov, A.; Linsenmeyer, T.A.; Beck, L.A.; Elliott, S.; Gorman, P.; Kirshblum, S.; Vogel, L.; Wecht, J.; Clay, S. Evaluation and Management of Autonomic Dysreflexia and Other Autonomic Dysfunctions: Preventing the Highs and Lows: Management of Blood Pressure, Sweating, and Temperature Dysfunction. Top. Spinal Cord Inj. Rehabil. 2021, 27, 225–290. [Google Scholar] [CrossRef]
- Furlan, J.C.; Fehlings, M.G. Cardiovascular complications after acute spinal cord injury: Pathophysiology, diagnosis, and management. Neurosurg. Focus 2008, 25, E13. [Google Scholar] [CrossRef] [Green Version]
- Weinberg, J.A.; Farber, S.H.; Kalamchi, L.D.; Brigeman, S.T.; Bohl, M.A.; Varda, B.M.; Sioda, N.A.; Radosevich, J.J.; Chapple, K.M.; Snyder, L.A. Mean arterial pressure maintenance following spinal cord injury: Does meeting the target matter? J. Trauma Acute Care Surg. 2021, 90, 97–106. [Google Scholar] [CrossRef]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065.
- El-Kotob, R.; Craven, B.; Mathur, S.; Ditor, D.S.; Oh, P.; Miyatani, M.; Verrier, M.C. Assessing Heart Rate Variability As a Surrogate Measure of Cardiac Autonomic Function in Chronic Traumatic Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2018, 24, 28–36. [Google Scholar] [CrossRef]
- Kyriakides, A.; Poulikakos, D.; Galata, A.; Konstantinou, D.; Panagiotopoulos, E.; Chroni, E. The effect of level of injury and physical activity on heart rate variability following spinal cord injury. J. Spinal Cord Med. 2019, 42, 212–219. [Google Scholar] [CrossRef]
- Malmqvist, L.; Biering-Sørensen, T.; Bartholdy, K.; Krassioukov, A.; Welling, K.-L.; Svendsen, J.H.; Kruse, A.; Hansen, B.; Biering-Sørensen, F. Assessment of autonomic function after acute spinal cord injury using heart rate variability analyses. Spinal Cord. 2015, 53, 54–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschlböck, S.; Wenning, G.; Fanciulli, A. Evidence-based treatment of neurogenic orthostatic hypotension and related symptoms. J. Neural Transm. 2017, 124, 1567–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illman, A.; Stiller, K.; Williams, M. The prevalence of orthostatic hypotension during physiotherapy treatment in patients with an acute spinal cord injury. Spinal Cord. 2000, 38, 741–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, G.M. Exercise capacity of individuals with paraplegia. Med. Sci. Sports Exerc. 1993, 25, 423–432. [Google Scholar] [CrossRef]
- Faghri, P.D.; Yount, J.P.; Pesce, W.J.; Seetharama, S.; Votto, J.J. Circulatory hypokinesis and functional electric stimulation during standing in persons with spinal cord injury. Arch. Phys. Med. Rehabil. 2001, 82, 1587–1595. [Google Scholar] [CrossRef]
- Figoni, S.F. Exercise responses and quadriplegia. Med. Sci. Sports Exerc. 1993, 25, 433–441. [Google Scholar] [CrossRef]
- Linsenmeyer, T.A.; Gibbs, K.; Solinsky, R. Autonomic Dysreflexia After Spinal Cord Injury: Beyond the Basics. Curr. Phys. Med. Rehabil. Rep. 2020, 8, 443–451. [Google Scholar] [CrossRef]
- Bowlby, A.A. On the Condition of the Reflexes in Cases of Injury to the Spinal Cord; with special reference to the Indications for Operative Interference. Med. Chir. Trans. 1890, 73, 313–325. [Google Scholar] [CrossRef] [Green Version]
- Krassioukov, A.; Stillman, M.; Beck, L.A. A Primary Care Provider’s Guide to Autonomic Dysfunction Following Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2020, 26, 123–127. [Google Scholar] [CrossRef]
- Wecht, J.M.; Harel, N.Y.; Guest, J.; Kirshblum, S.C.; Forrest, G.F.; Bloom, O.; Ovechkin, A.V.; Harkema, S. Cardiovascular Autonomic Dysfunction in Spinal Cord Injury: Epidemiology, Diagnosis, and Management. In Seminars in Neurology; Thieme Medical Publishers: New York, NY, USA, 2020; Volume 40, pp. 550–559. [Google Scholar]
- Morrison, S.F.; Nakamura, K. Central neural pathways for thermoregulation. Front. Biosci. 2011, 16, 74–104. [Google Scholar] [CrossRef] [Green Version]
- Phillips, A.A.; Squair, J.; Sayenko, D.G.; Edgerton, V.R.; Gerasimenko, Y.; Krassioukov, A.V. An Autonomic Neuroprosthesis: Noninvasive Electrical Spinal Cord Stimulation Restores Autonomic Cardiovascular Function in Individuals with Spinal Cord Injury. J. Neurotrauma 2018, 35, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.D.; Chan, C.W. Thermoregulation and fever in normal persons and in those with spinal cord injuries. Mayo Clin. Proc. 1992, 67, 469–475. [Google Scholar] [CrossRef] [Green Version]
- Grossmann, F.; Flueck, J.L.; Perret, C.; Meeusen, R.; Roelands, B. The Thermoregulatory and Thermal Responses of Individuals With a Spinal Cord Injury During Exercise, Acclimation and by Using Cooling Strategies–A Systematic Review. Front. Physiol. 2021, 12, 636997. [Google Scholar] [CrossRef] [PubMed]
- West, C.; AlYahya, A.; Laher, I.; Krassioukov, A. Peripheral vascular function in spinal cord injury: A systematic review. Spinal Cord. 2013, 51, 10–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, K.E.; Oleson, C.V.; Schroeder, G.D.; Sidhu, G.S.; Vaccaro, A.R. Neurogenic Fever after Acute Traumatic Spinal Cord Injury: A Qualitative Systematic Review. Glob. Spine J. 2016, 6, 607–614. [Google Scholar] [CrossRef] [Green Version]
- Ülger, F.; Küçük, M.P.; Öztürk, E.; Aksoy, I.; Küçük, A.O.; Murat, N. Non-infectious Fever After Acute Spinal Cord Injury in the Intensive Care Unit. J. Spinal Cord Med. 2019, 42, 310–317. [Google Scholar] [CrossRef]
- Menard, M.R.; Hahn, G. Acute and chronic hypothermia in a man with spinal cord injury: Environmental and pharmacologic causes. Arch. Phys. Med. Rehabil. 1991, 72, 421–424. [Google Scholar]
- Smith, T.M.; Berk, A.S.; Upadhyay, H. Severe hypothermia in a patient with spinal cord injury without radiological abnormality. J. Emerg. Trauma Shock 2011, 4, 421–424. [Google Scholar] [CrossRef]
- Schilero, G.J.; Bauman, W.A.; Radulovic, M. Traumatic Spinal Cord Injury: Pulmonary Physiologic Principles and Management. Clin. Chest Med. 2018, 39, 411–425. [Google Scholar] [CrossRef]
- Henzel, M.K.; Ms, J.M.S.; Dyson-Hudson, T.A.; Svircev, J.N.; DiMarco, A.F.; Gater, D.R. Initial assessment and management of respiratory infections in persons with spinal cord injuries and disorders in the COVID-19 era. J. Am. Coll. Emerg. Physicians Open 2020, 1, 1404–1412. [Google Scholar] [CrossRef]
- Coutts, K.D.; McKenzie, D.C. Ventilatory thresholds during wheelchair exercise in individuals with spinal cord injuries. Paraplegia 1995, 33, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, D.A.; Boone, T.B.; Cameron, A.P.; Gousse, A.; Kaufman, M.R.; Keays, E.; Kennelly, M.J.; Lemack, G.E.; Rovner, E.S.; Souter, L.H.; et al. The AUA/SUFU Guideline on Adult Neurogenic Lower Urinary Tract Dysfunction: Diagnosis and Evaluation. J. Urol. 2021, 206, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.; Lynne, C.M.; Brackett, N.L. Male fertility following spinal cord injury: An update. Andrology 2016, 4, 13–26. [Google Scholar] [CrossRef] [Green Version]
- Pereira, L. Obstetric management of the patient with spinal cord injury. Obstet. Gynecol. Surv. 2003, 58, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Obstetric Management of Patients with Spinal Cord Injuries: ACOG Committee Opinion, Number 808. Obstet. Gynecol. 2020, 135, e230–e236. [CrossRef]
- Holmes, G.M.; Blanke, E.N. Gastrointestinal dysfunction after spinal cord injury. Exp. Neurol. 2019, 320, 113009. [Google Scholar] [CrossRef]
- Hsu, C.L.; Wang, M.T.; Ho, Y.C.; Pan, S.L. Increased Risk of Acute Cholecystitis in Patients With Spinal Cord Injury: A Nationwide Population-Based Cohort Study. Spine 2018, 43, 934–939. [Google Scholar] [CrossRef]
- Tandon, R.K.; Jain, R.K.; Garg, P.K. Increased incidence of biliary sludge and normal gall bladder contractility in patients with high spinal cord injury. Gut 1997, 41, 682–687. [Google Scholar] [CrossRef]
- Rupp, R.; Biering-Sørensen, F.; Burns, S.P.; Graves, D.E.; Guest, J.; Jones, L.; Read, M.S.; Rodriguez, G.M.; Schuld, C.; Tansey, K.E.; et al. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top. Spinal Cord Inj. Rehabil. 2021, 27, 1–22. [Google Scholar] [CrossRef]
- Curt, A.; Weinhardt, C.; Dietz, V. Significance of sympathetic skin response in the assessment of autonomic failure in patients with spinal cord injury. J. Auton. Nerv. Syst. 1996, 61, 175–180. [Google Scholar] [CrossRef]
- Wecht, J.M.; Weir, J.P.; Katzelnick, C.G.; Chiaravalloti, N.; Kirshblum, S.C.; Dyson-Hudson, T.A.; Weber, E.; Bauman, W.A. Double-blinded, placebo-controlled crossover trial to determine the effects of midodrine on blood pressure during cognitive testing in persons with SCI. Spinal Cord. 2020, 58, 959–969. [Google Scholar] [CrossRef]
- Caruso, D.; Gater, D.; Harnish, C. Prevention of recurrent autonomic dysreflexia: A survey of current practice. Clin. Auton Res. 2015, 25, 293–300. [Google Scholar] [CrossRef]
- Song, S.H.; Svircev, J.N.; Teng, B.J.; Dominitz, J.A.; Burns, S.P. A safe and effective multi-day colonoscopy bowel preparation for individuals with spinal cord injuries. J. Spinal Cord Med. 2018, 41, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Cosman, B.C.; Vu, T.T. Lidocaine anal block limits autonomic dysreflexia during anorectal procedures in spinal cord injury: A randomized, double-blind, placebo-controlled trial. Dis. Colon. Rectum. 2005, 48, 1556–1561. [Google Scholar] [CrossRef] [PubMed]
- Crane, D.A.; Ms, D.R.D.; Schiff, M.A.; Mueller, B.A. Pregnancy Outcomes in Women with Spinal Cord Injuries: A Population-Based Study. PM&R 2019, 11, 795–806. [Google Scholar]
- Morton, C.; Le, J.T.; Shahbandar, L.; Hammond, C.; Murphy, E.A.; Kirschner, K.L. Pregnancy outcomes of women with physical disabilities: A matched cohort study. PM&R 2013, 5, 90–98. [Google Scholar]
- Robertson, K.; Dawood, R.; Ashworth, F. Vaginal delivery is safely achieved in pregnancies complicated by spinal cord injury: A retrospective 25-year observational study of pregnancy outcomes in a national spinal injuries centre. BMC Pregnancy Childbirth 2020, 20, 56. [Google Scholar] [CrossRef] [PubMed]
- Mazzeo, F.; Santamaria, S.; Iavarone, A. “Boosting” in Paralympic athletes with spinal cord injury: Doping without drugs. Funct. Neurol. 2015, 30, 91–98. [Google Scholar]
- Wheeler, G.; Cumming, D.; Burnham, R.; MacLean, I.; Sloley, B.D.; Bhambhani, Y.; Steadward, R.D. Testosterone, cortisol and catecholamine responses to exercise stress and autonomic dysreflexia in elite quadriplegic athletes. Paraplegia 1994, 32, 292–299. [Google Scholar] [CrossRef]
- Burnham, R.; Wheeler, G.; Bhambhani, Y.; Belanger, M. Intentional induction of autonomic dysreflexia among quadriplegic athletes for performance enhancement: Efficacy, safety, and mechanism of action. Clin. J. Sport Med. 1994, 4, 1–10. [Google Scholar]
- Andersen, L.S.; Biering-Sørensen, F.; Muller, P.G.; Jensen, I.L.; Aggerbeck, B. The Prevalence of Hyperhidrosis in Patients with Spinal-Cord Injuries and an Evaluation of the Effect of Dextropropoxyphene Hydrochloride in Therapy. Paraplegia 1992, 30, 184–191. [Google Scholar] [CrossRef]
- Adams, B.B.; Vargus-Adams, J.N.; Franz, D.N.; Kinnett, D.G. Hyperhidrosis in pediatric spinal cord injury: A case report and gabapentin therapy. J. Am. Acad. Dermatol. 2002, 46, 444–446. [Google Scholar] [CrossRef] [PubMed]
- Tkach, J.R. Indomethacin treatment of generalized hyperhidrosis. J. Am. Acad. Dermatol. 1982, 6 Pt 1, 545. [Google Scholar] [CrossRef]
- Sergi, R.; Massone, A.; Moretto, S.; Oggerino, C.; Bertolotto, F.; Losio, L.; Ottonello, M. Hyperhidrosis treatment with bornaprine in the acute phase of spinal cord-injured patients. Spinal Cord. 2008, 46, 571–573. [Google Scholar] [CrossRef] [Green Version]
- Canaday, B.R.; Stanford, R.H. Propantheline Bromide in the Management of Hyperhidrosis Associated with Spinal-Cord Injury. Ann. Pharmacother. 1995, 29, 489–492. [Google Scholar] [CrossRef]
- Shessel, F.S.; Carrion, H.M.; Politano, V.A. Phenoxybenzamine and sweating in the spinal cord injury patient. J. Urol. 1978, 120, 60–61. [Google Scholar] [CrossRef]
- Albadrani, A. Clonidine is effective for the treatment of primary idiopathic hyperhidrosis and hot flushes: A case report. J. Med. Case Rep. 2017, 11, 16. [Google Scholar] [CrossRef] [Green Version]
- Walling, H.W.; Swick, B.L. Treatment options for hyperhidrosis. Am. J. Clin. Dermatol. 2011, 12, 285–295. [Google Scholar] [CrossRef] [PubMed]
- Han, J.W.; Kim, J.J.; Jeong, S.C.; Kim, Y.H.; Kim, I.-S. Sympathotomy for severe compensatory hyperhidrosis in the trunk due to traumatic cervical spinal cord injury. J. Thorac. Dis. 2020, 12, 1115–1117. [Google Scholar] [CrossRef]
- Nawrocki, S.; Cha, J. Botulinum toxin: Pharmacology and injectable administration for the treatment of primary hyperhidrosis. J. Am. Acad. Dermatol. 2020, 82, 969–979. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henke, A.M.; Billington, Z.J.; Gater, D.R., Jr. Autonomic Dysfunction and Management after Spinal Cord Injury: A Narrative Review. J. Pers. Med. 2022, 12, 1110. https://doi.org/10.3390/jpm12071110
Henke AM, Billington ZJ, Gater DR Jr. Autonomic Dysfunction and Management after Spinal Cord Injury: A Narrative Review. Journal of Personalized Medicine. 2022; 12(7):1110. https://doi.org/10.3390/jpm12071110
Chicago/Turabian StyleHenke, Austin M., Zackery J. Billington, and David R. Gater, Jr. 2022. "Autonomic Dysfunction and Management after Spinal Cord Injury: A Narrative Review" Journal of Personalized Medicine 12, no. 7: 1110. https://doi.org/10.3390/jpm12071110