
TRIM24 Expression as an Independent Biomarker for Prognosis and Tumor Recurrence in HNSCC

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Data and Tumor Material
2.2. Immunohistochemistry and Evaluation
2.3. Statistical Analysis and Visualization
3. Results
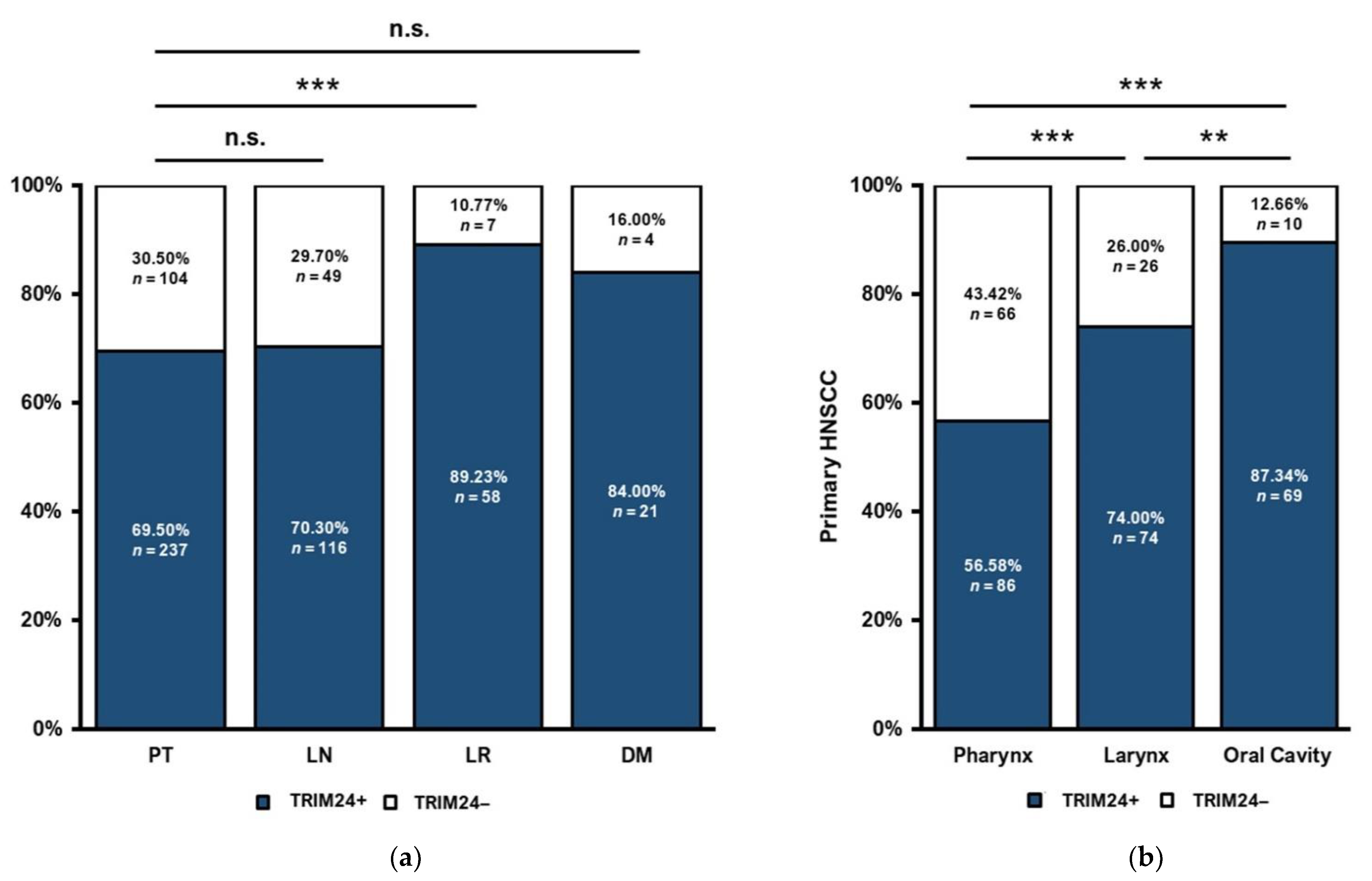
3.1. TRIM24 Expression Is Different in Primary Tumors, Lymph Node Metastases, Local Recurrences, and Distant Metastases
3.2. Distinct TRIM24 Expression in HNSCC Tumor Sites
3.3. TRIM24 Expression Is Lower in HNSCC Primary Tumors with Lymph Node Metastases
3.4. Association of TRIM24 Expression and the p16 Expression of HNSCC Primary Tumors
3.5. TRIM24 Is Expressed More Frequently in HNSCC Primary Tumors with Local Recurrences
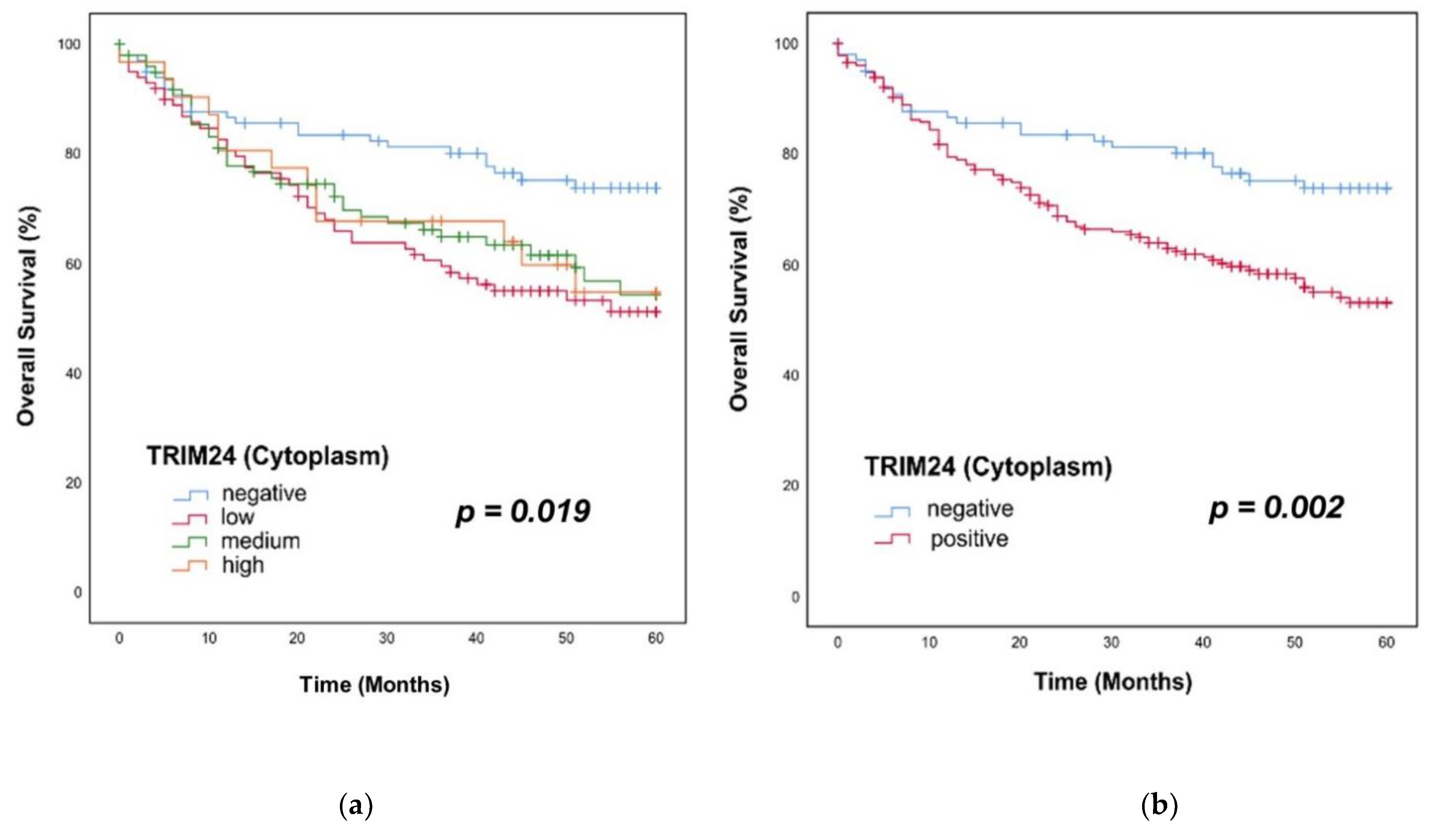
3.6. Overall Survival in Patients with TRIM24+ Tumors
3.7. Progression-Free Survival in Patients with TRIM24+ Tumors
3.8. TRIM24 Expression Is Independent of T Stage and UICC Stage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| DM | Distant metastasis |
| ER | Estrogen receptor |
| FFPE | Formalin-fixed paraffin-embedded |
| HE | hematoxylin-eosin |
| HNSCC | Head and neck squamous cell carcinoma |
| HPV | Human papillomavirus |
| LN | Lymph node metastasis |
| LR | Local recurrence |
| NSCLC | non-small cell lung cancer |
| OS | Overall survival |
| OSCC | Oropharyngeal squamous cell carcinoma |
| p16− | p16 negative tumors |
| p16+ | p16 positive tumors |
| PD-1 | programmed cell death protein 1 |
| PFS | progression-free survival |
| PT | Primary tumor |
| RAR-α | Retinoic acid-receptor-α |
| TMA | Tissue microarray |
| TRIM | Tripartite Motif |
| TRIM24− | TRIM24 negative tumors |
| TRIM24 | Tripartite Motif-Containing 24 |
| TRIM24+ | TRIM24 positive tumors |
References
- Parker, S.L.; Tong, T.; Bolden, S.; Wingo, P.A. Cancer Statistics, 1996. CA Cancer J. Clin. 1996, 46, 5–27. [Google Scholar] [CrossRef] [PubMed]
- Vokes, E.E.; Weichselbaum, R.R.; Lippman, S.M.; Hong, W.K. Head and Neck Cancer. N. Engl. J. Med. 1993, 328, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaatsch, P.; Spix, C.; Katalinic, A.; Hentschel, S.; Luttmann, S.; Waldeyer-Sauerland, M.; Waldmann, A. Krebs in Deutschland für 2015/2016; Robert Koch-Institut: Berlin, Germany, 2019; Available online: https://edoc.rki.de/handle/176904/6012.3 (accessed on 2 May 2022).
- Canning, M.; Guo, G.; Yu, M.; Myint, C.; Groves, M.W.; Byrd, J.K.; Cui, Y. Heterogeneity of the Head and Neck Squamous Cell Carcinoma Immune Landscape and Its Impact on Immunotherapy. Front. Cell Dev. Biol. 2019, 7, 52. [Google Scholar] [CrossRef]
- Leemans, C.R.; Snijders, P.J.F.; Brakenhoff, R.H. The Molecular Landscape of Head and Neck Cancer. Nat. Rev. Cancer 2018, 18, 269–282. [Google Scholar] [CrossRef]
- McDermott, J.D.; Bowles, D.W. Epidemiology of Head and Neck Squamous Cell Carcinomas: Impact on Staging and Prevention Strategies. Curr. Treat. Options Oncol. 2019, 20, 43. [Google Scholar] [CrossRef]
- Pezzuto, F.; Buonaguro, L.; Caponigro, F.; Ionna, F.; Starita, N.; Annunziata, C.; Buonaguro, F.M.; Tornesello, M.L. Update on Head and Neck Cancer: Current Knowledge on Epidemiology, Risk Factors, Molecular Features and Novel Therapies. Oncology 2015, 89, 125–136. [Google Scholar] [CrossRef]
- D’Souza, G.; Kreimer, A.R.; Viscidi, R.; Pawlita, M.; Fakhry, C.; Koch, W.M.; Westra, W.H.; Gillison, M.L. Case-Control Study of Human Papillomavirus and Oropharyngeal Cancer. N. Engl. J. Med. 2007, 356, 1944–1956. [Google Scholar] [CrossRef] [Green Version]
- Castellsagué, X.; Alemany, L.; Quer, M.; Halec, G.; Quirós, B.; Tous, S.; Clavero, O.; Alòs, L.; Biegner, T.; Szafarowski, T.; et al. HPV Involvement in Head and Neck Cancers: Comprehensive Assessment of Biomarkers in 3680 Patients. J. Natl. Cancer Inst. 2016, 108, djv403. [Google Scholar] [CrossRef]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and Neck Squamous Cell Carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global Cancer Statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [Green Version]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ervin, T.J.; Clark, J.R.; Weichselbaum, R.R.; Fallon, B.G.; Miller, D.; Fabian, R.L.; Posner, M.R.; Norris, C.M.; Tuttle, S.A.; Schoenfeld, D.A. An Analysis of Induction and Adjuvant Chemotherapy in the Multidisciplinary Treatment of Squamous-Cell Carcinoma of the Head and Neck. J. Clin. Oncol. 1987, 5, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Chin, D.; Boyle, G.M.; Porceddu, S.; Theile, D.R.; Parsons, P.G.; Coman, W.B. Head and Neck Cancer: Past, Present and Future. Expert Rev. Anticancer Ther. 2006, 6, 1111–1118. [Google Scholar] [CrossRef]
- Bernier, J. A Multidisciplinary Approach to Squamous Cell Carcinomas of the Head and Neck: An Update. Curr. Opin. Oncol. 2008, 20, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Larson, D.L.; Lindberg, R.D.; Lane, E.; Goepfert, H. Major Complications of Radiotherapy in Cancer of the Oral Cavity and Oropharynx. A 10 Year Retrospective Study. Am. J. Surg. 1983, 146, 531–536. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Bell, R.B.; Bifulco, C.B.; Burtness, B.; Gillison, M.L.; Harrington, K.J.; Le, Q.-T.; Lee, N.Y.; Leidner, R.; Lewis, R.L.; et al. The Society for Immunotherapy of Cancer Consensus Statement on Immunotherapy for the Treatment of Squamous Cell Carcinoma of the Head and Neck (HNSCC). J. Immunother. Cancer 2019, 7, 184. [Google Scholar] [CrossRef] [Green Version]
- Murdoch, D. Standard, and Novel Cytotoxic and Molecular-Targeted, Therapies for HNSCC: An Evidence-Based Review. Curr. Opin. Oncol. 2007, 19, 216–221. [Google Scholar] [CrossRef]
- Sher, D.J.; Yan, J.; Day, A.; Sumer, B.D.; Pham, N.-L.; Khan, S.; Zhu, H. Comparative Effectiveness of Primary Radiotherapy versus Surgery in Elderly Patients with Locally Advanced Oropharyngeal Squamous Cell Carcinoma. Oral Oncol. 2019, 88, 18–26. [Google Scholar] [CrossRef]
- Allton, K.; Jain, A.K.; Herz, H.-M.; Tsai, W.-W.; Jung, S.Y.; Qin, J.; Bergmann, A.; Johnson, R.L.; Barton, M.C. Trim24 Targets Endogenous P53 for Degradation. Proc. Natl. Acad. Sci. USA 2009, 106, 11612–11616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatakeyama, S. TRIM Proteins and Cancer. Nat. Rev. Cancer 2011, 11, 792–804. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.K.; Barton, M.C. Regulation of P53: TRIM24 Enters the RING. Cell Cycle 2009, 8, 3668–3674. [Google Scholar] [CrossRef] [PubMed]
- Chambon, M.; Orsetti, B.; Berthe, M.-L.; Bascoul-Mollevi, C.; Rodriguez, C.; Duong, V.; Gleizes, M.; Thénot, S.; Bibeau, F.; Theillet, C.; et al. Prognostic Significance of TRIM24/TIF-1α Gene Expression in Breast Cancer. Am. J. Pathol. 2011, 178, 1461–1469. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Zhao, W.; Sun, B.; Wang, X.; Liu, Q. Overexpression of TRIM24 Is Correlated with the Progression of Human Cervical Cancer. Am. J. Transl. Res. 2017, 9, 620–628. [Google Scholar] [PubMed]
- Li, H.; Sun, L.; Tang, Z.; Fu, L.; Xu, Y.; Li, Z.; Luo, W.; Qiu, X.; Wang, E. Overexpression of TRIM24 Correlates with Tumor Progression in Non-Small Cell Lung Cancer. PLoS ONE 2012, 7, e37657. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Xue, W.; Jiang, X. Overexpression of TRIM24 Stimulates Proliferation and Glucose Metabolism of Head and Neck Squamous Cell Carcinoma. BioMed Res. Int. 2018, 2018, 6142843. [Google Scholar] [CrossRef] [Green Version]
- Cui, Z.; Cao, W.; Li, J.; Song, X.; Mao, L.; Chen, W. TRIM24 Overexpression Is Common in Locally Advanced Head and Neck Squamous Cell Carcinoma and Correlates with Aggressive Malignant Phenotypes. PLoS ONE 2013, 8, e63887. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, M.; Okumura, F.; Tsukiyama, T.; Watanabe, M.; Miyajima, N.; Tanaka, J.; Imamura, M.; Hatakeyama, S. TRIM24 Mediates Ligand-Dependent Activation of Androgen Receptor and Is Repressed by a Bromodomain-Containing Protein, BRD7, in Prostate Cancer Cells. Biochim. Biophys. Acta Mol. Cell Res. 2009, 1793, 1828–1836. [Google Scholar] [CrossRef] [Green Version]
- Tsai, W.-W.; Wang, Z.; Yiu, T.T.; Akdemir, K.C.; Xia, W.; Winter, S.; Tsai, C.-Y.; Shi, X.; Schwarzer, D.; Plunkett, W.; et al. TRIM24 Links a Non-Canonical Histone Signature to Breast Cancer. Nature 2010, 468, 927–932. [Google Scholar] [CrossRef] [Green Version]
- Scheble, V.J.; Braun, M.; Beroukhim, R.; Mermel, C.H.; Ruiz, C.; Wilbertz, T.; Stiedl, A.-C.; Petersen, K.; Reischl, M.; Kuefer, R.; et al. ERG Rearrangement Is Specific to Prostate Cancer and Does Not Occur in Any Other Common Tumor. Mod. Pathol. 2010, 23, 1061–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribbat-Idel, J.; Dressler, F.F.; Krupar, R.; Watermann, C.; Paulsen, F.-O.; Kuppler, P.; Klapper, L.; Offermann, A.; Wollenberg, B.; Rades, D.; et al. Performance of Different Diagnostic PD-L1 Clones in Head and Neck Squamous Cell Carcinoma. Front. Med. 2021, 8, 640515. [Google Scholar] [CrossRef] [PubMed]
- Braun, M.; Goltz, D.; Adler, D.; Vogel, W.; Böhm, D.; Scheble, V.; Sotlar, K.; Fend, F.; Tan, S.-H.; Dobi, A.; et al. ERG Protein Expression and Genomic Rearrangement Status in Primary and Metastatic Prostate Cancer—A Comparative Study of Two Monoclonal Antibodies. Prostate Cancer Prostatic Dis. 2012, 15, 165–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Queisser, A.; Hagedorn, S.; Wang, H.; Schaefer, T.; Konantz, M.; Alavi, S.; Deng, M.; Vogel, W.; von Mässenhausen, A.; Kristiansen, G.; et al. Ecotropic Viral Integration Site 1, a Novel Oncogene in Prostate Cancer. Oncogene 2017, 36, 1573–1584. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open Source Software for Digital Pathology Image Analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Li, M.; Zhang, X.; Huang, H.; Huang, J.; Ke, J.; Ding, H.; Xiao, J.; Shan, X.; Liu, Q.; et al. Upregulation of CDK7 in Gastric Cancer Cell Promotes Tumor Cell Proliferation and Predicts Poor Prognosis. Exp. Mol. Pathol. 2016, 100, 514–521. [Google Scholar] [CrossRef]
- Jiang, L.; Huang, R.; Wu, Y.; Diao, P.; Zhang, W.; Li, J.; Li, Z.; Wang, Y.; Cheng, J.; Yang, J. Overexpression of CDK7 Is Associated with Unfavourable Prognosis in Oral Squamous Cell Carcinoma. Pathology 2019, 51, 74–80. [Google Scholar] [CrossRef]
- Kim, J.; Cho, Y.-J.; Ryu, J.-Y.; Hwang, I.; Han, H.D.; Ahn, H.J.; Kim, W.Y.; Cho, H.; Chung, J.-Y.; Hewitt, S.M.; et al. CDK7 Is a Reliable Prognostic Factor and Novel Therapeutic Target in Epithelial Ovarian Cancer. Gynecol. Oncol. 2020, 156, 211–221. [Google Scholar] [CrossRef] [Green Version]
- Ribbat-Idel, J.; Perner, S.; Kuppler, P.; Klapper, L.; Krupar, R.; Watermann, C.; Paulsen, F.-O.; Offermann, A.; Bruchhage, K.-L.; Wollenberg, B.; et al. Immunologic “Cold” Squamous Cell Carcinomas of the Head and Neck Are Associated with an Unfavorable Prognosis. Front. Med. 2021, 8, 622330. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, C.; Wang, X.; Hu, W.; Feng, Z. Tumor Suppressor P53 Cross-Talks with TRIM Family Proteins. Genes Dis. 2020, 8, 463–474. [Google Scholar] [CrossRef]
- Offermann, A.; Roth, D.; Hupe, M.C.; Hohensteiner, S.; Becker, F.; Joerg, V.; Carlsson, J.; Kuempers, C.; Ribbat-Idel, J.; Tharun, L.; et al. TRIM24 as an Independent Prognostic Biomarker for Prostate Cancer. Urol. Oncol. 2019, 37, 576.e1–576.e10. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Huang, Y.; Yang, D.; Li, X.; Liang, J.; Lin, L.; Zhang, M.; Zhong, K.; Liang, B.; Li, J. Overexpression of TRIM24 Is Associated with the Onset and Progress of Human Hepatocellular Carcinoma. PLoS ONE 2014, 9, e85462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, J.; Yang, Q.; Xie, X.-F.; Yang, X.-Z.; Zhang, M.-Y.; Wang, H.-Y.; Xu, G.-L. Clinical Significance and Prognostic Value of TRIM24 Expression in Esophageal Squamous Cell Carcinoma. Aging 2016, 8, 2204–2217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, J.F.; Timmermans, A.J.; van Dijk, B.A.C.; Overbeek, L.I.H.; Smit, L.A.; Hilgers, F.J.M.; Stuiver, M.M.; van den Brekel, M.W.M. Trends in Treatment, Incidence and Survival of Hypopharynx Cancer: A 20-Year Population-Based Study in the Netherlands. Eur. Arch. Otorhinolaryngol. 2018, 275, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, S.; Ganguly, K.; Muniyan, S.; Pothuraju, R.; Sayed, Z.; Jones, D.T.; Batra, S.K.; Macha, M.A. Immunometabolic Alterations by HPV Infection: New Dimensions to Head and Neck Cancer Disparity. J. Natl. Cancer Inst. 2019, 111, 233–244. [Google Scholar] [CrossRef] [Green Version]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and Neck Cancers-Major Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef]
- Benson, E.; Li, R.; Eisele, D.; Fakhry, C. The Clinical Impact of HPV Tumor Status upon Head and Neck Squamous Cell Carcinomas. Oral Oncol. 2014, 50, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Hufbauer, M.; Maltseva, M.; Meinrath, J.; Lechner, A.; Beutner, D.; Huebbers, C.U.; Akgül, B. HPV16 Increases the Number of Migratory Cancer Stem Cells and Modulates Their MiRNA Expression Profile in Oropharyngeal Cancer. Int. J. Cancer 2018, 143, 1426–1439. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Univariate Cox Regression | Multivariate Cox Regression | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% Confidence Interval | p-Value | Hazard Ratio | 95% Confidence Interval | p-Value | |
| Cytoplasmatic TRIM24 Expression | 1.973 | 1.260–3.091 | 0.003 * | 1.890 | 1.194–2.990 | 0.007 * |
| P16 Expression | 0.478 | 0.310–0.737 | 0.001 * | 0.641 | 0.395–1.041 | 0.072 |
| Grading | 1.316 | 0.909–1.906 | 0.146 | |||
| T Stage (T1 + T2/T3 + T4) | 2.289 | 1.613–3.248 | <0.001 * | 1.906 | 1.302–2.791 | 0.001 * |
| N Stage (N0 + N1/N2 + N3) | 2.252 | 1.799–3.546 | <0.001 * | 1.990 | 1.374–2.882 | <0.001 * |
| Variable | Univariate Cox Regression | Multivariate Cox Regression | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% Confidence Interval | p-Value | Hazard Ratio | 95% Confidence Interval | p-Value | |
| Cytoplasmatic TRIM24 Expression | 2.122 | 1.420–3.170 | <0.001 * | 2.114 | 1.396–3.202 | <0.001 * |
| P16 Expression | 0.456 | 0.313–0.666 | <0.001 * | 0.530 | 0.338–0.829 | 0.005 * |
| Grading | 1.040 | 0.740–1.461 | 0.823 | |||
| T Stage (T1 + T2/T3 + T4) | 2.157 | 1.593–2.920 | <0.001 * | 1.925 | 1.373–2.698 | <0.001 * |
| N Stage (N0 + N1/N2 + N3) | 1.959 | 1.457–2.633 | <0.001 * | 1.653 | 1.188–2.300 | 0.003 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klapper, L.; Idel, C.; Kuppler, P.; Jagomast, T.; von Bernuth, A.; Bruchhage, K.-L.; Rades, D.; Offermann, A.; Kirfel, J.; Perner, S.; et al. TRIM24 Expression as an Independent Biomarker for Prognosis and Tumor Recurrence in HNSCC. J. Pers. Med. 2022, 12, 991. https://doi.org/10.3390/jpm12060991
Klapper L, Idel C, Kuppler P, Jagomast T, von Bernuth A, Bruchhage K-L, Rades D, Offermann A, Kirfel J, Perner S, et al. TRIM24 Expression as an Independent Biomarker for Prognosis and Tumor Recurrence in HNSCC. Journal of Personalized Medicine. 2022; 12(6):991. https://doi.org/10.3390/jpm12060991
Chicago/Turabian StyleKlapper, Luise, Christian Idel, Patrick Kuppler, Tobias Jagomast, Amelie von Bernuth, Karl-Ludwig Bruchhage, Dirk Rades, Anne Offermann, Jutta Kirfel, Sven Perner, and et al. 2022. "TRIM24 Expression as an Independent Biomarker for Prognosis and Tumor Recurrence in HNSCC" Journal of Personalized Medicine 12, no. 6: 991. https://doi.org/10.3390/jpm12060991