
The Greek Collaborative Long COVID Study: Non-Hospitalized and Hospitalized Patients Share Similar Symptom Patterns


 , , and
, , and
Abstract
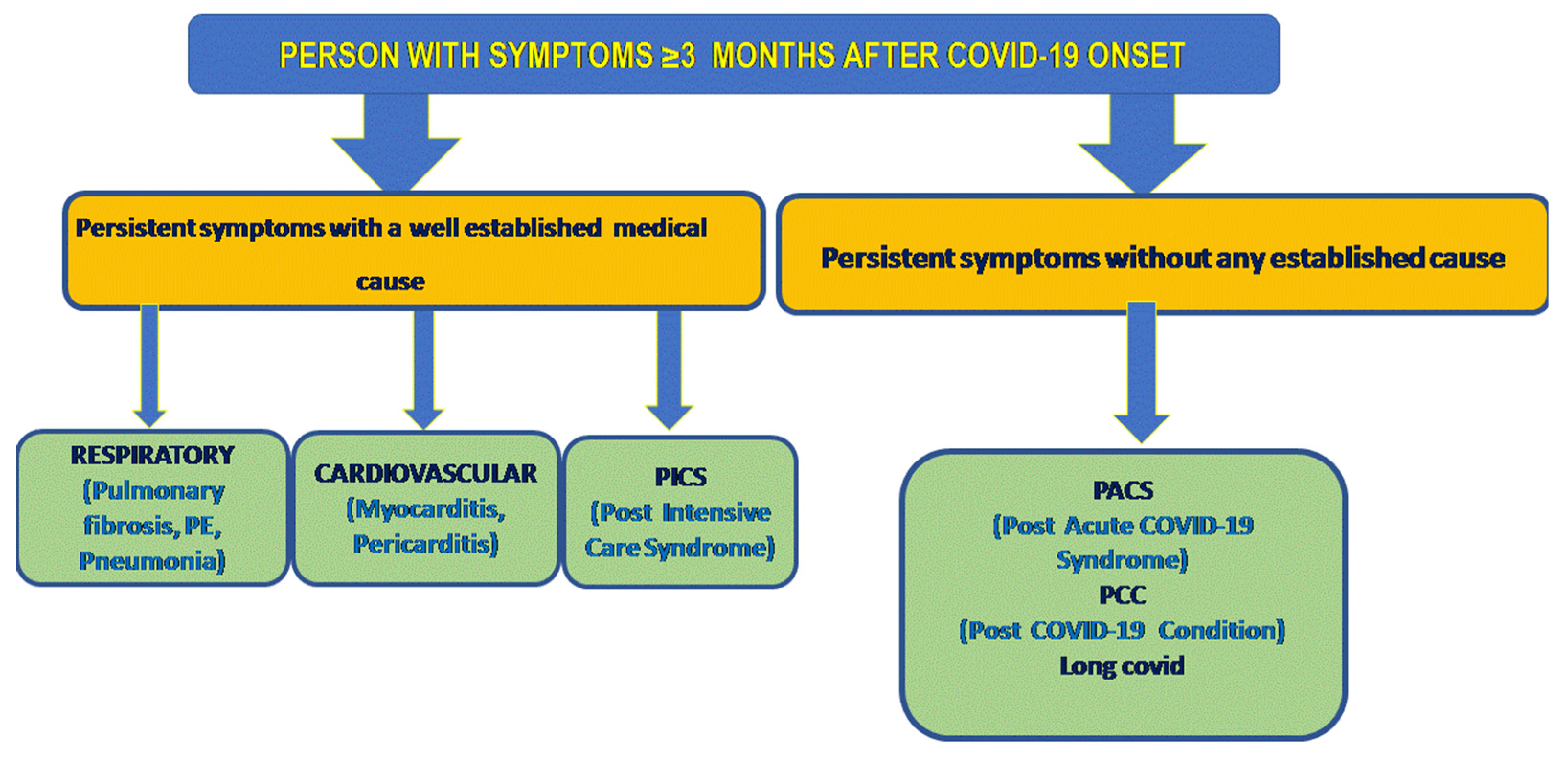
:1. Introduction
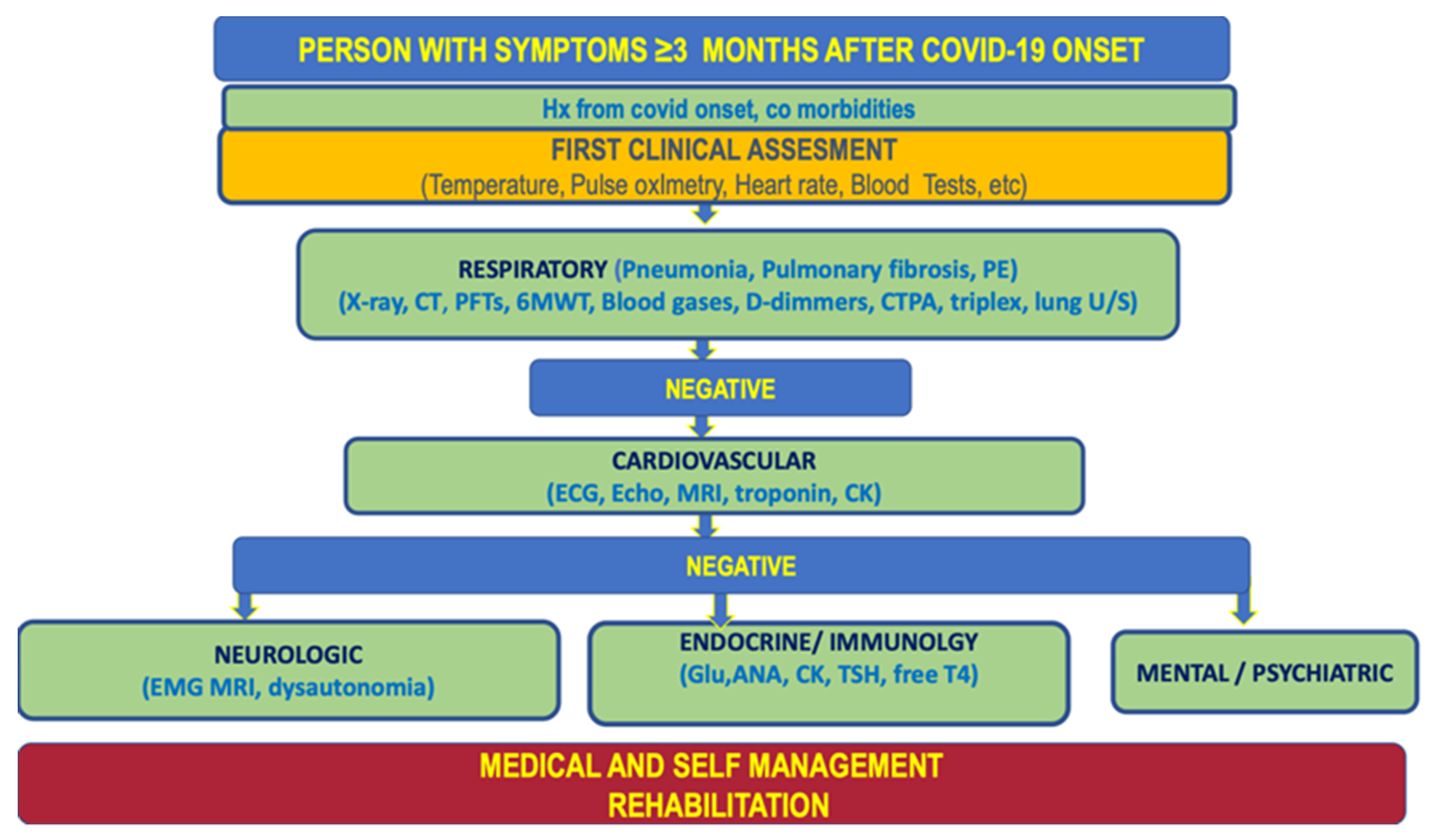
2. Materials and Methods
3. Results
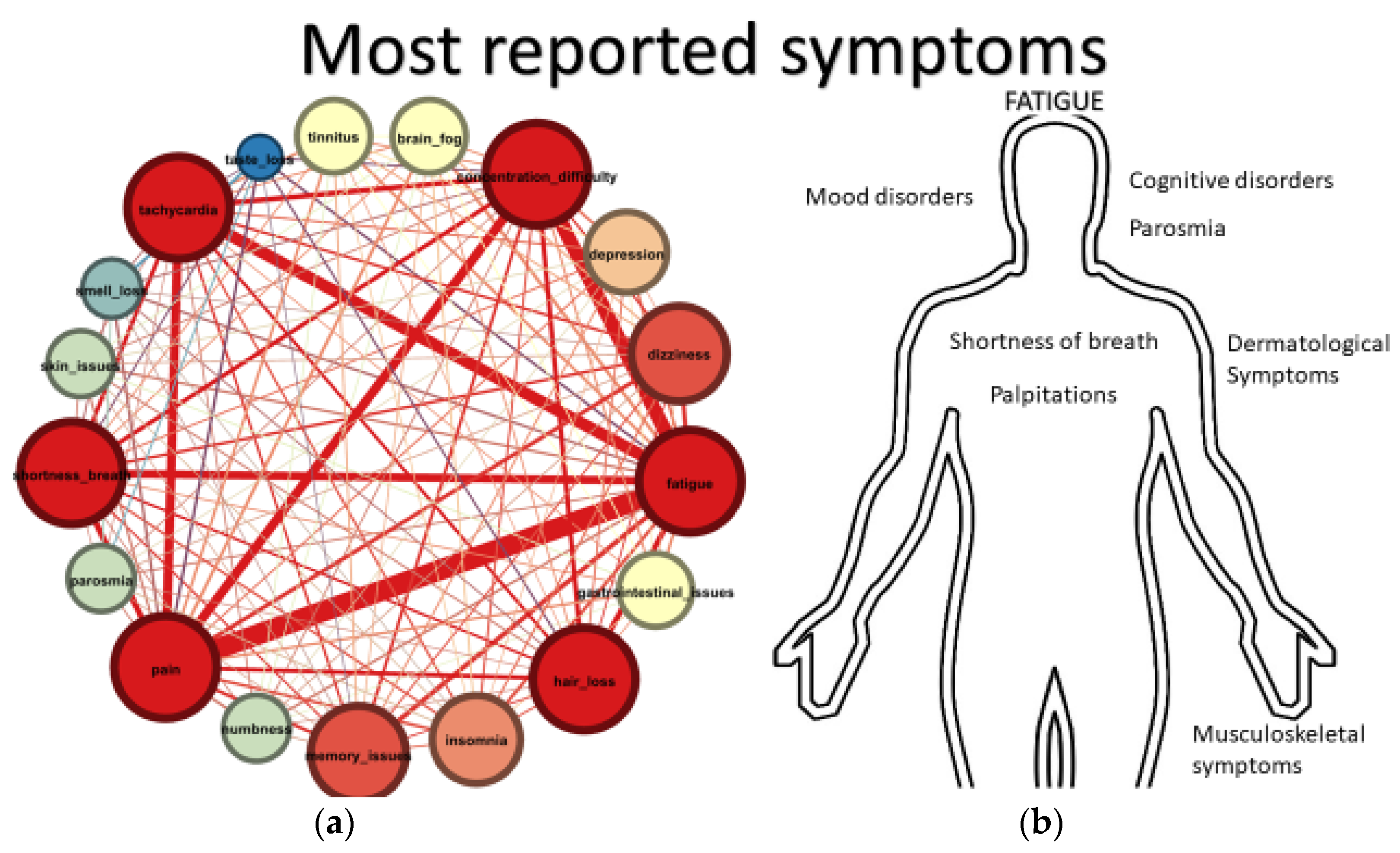
3.1. Persistent Symptoms
3.1.1. Fatigue
3.1.2. Musculoskeletal
3.1.3. Neurological, Cognitive, and Psychiatric Symptoms
3.1.4. Palpitations
3.1.5. Shortness of Breath
3.1.6. Dermatological
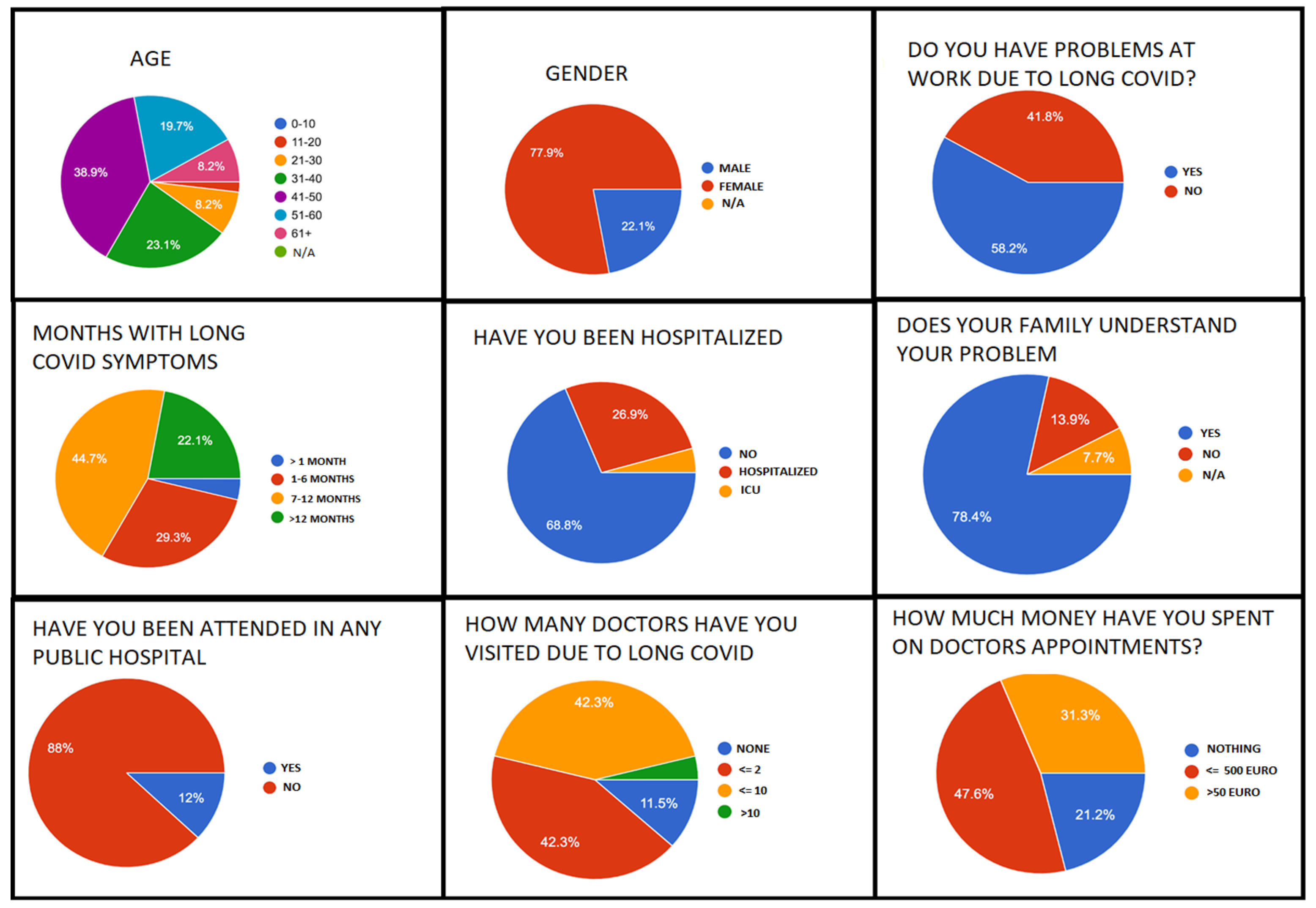
3.2. Socioeconomic Impact
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dani, M.; Dirksen, A.; Taraborrelli, P.; Torocastro, M.; Panagopoulos, D.; Sutton, R.; Lim, P.B. Autonomic dysfunction in ‘Long COVID’: Rationale, physiology and management strategies. Clin. Med. 2021, 21, e63–e67. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Haupert, S.R.; Zimmermann, L.; Shi, X.; Fritsche, L.G.; Mukherjee, B. Global prevalence of post-acute sequelae of COVID-19 (PASC) or long COVID: A meta-analysis and systematic review. medRxiv 2021. [Google Scholar] [CrossRef]
- Chertow, D.; Stein, S.; Ramelli, S.; Grazioli, A.; Winkler, C.; Dickey, J.; Platt, A.; Pittaluga, S.; Herr, D.; Mccurdy, M. SARS-CoV-2 Infection and Persistence throughout the Human Body and Brain; National Institutes of Health: Bethesda, MD, USA, 2021; ISBN 0000000150415. [Google Scholar]
- Centers for Disease Control and Prevention. Post-COVID Conditions: Information for Healthcare Providers; U.S. Department of Health & Human Services: Washington, DC, USA, 2021; pp. 1–3. [Google Scholar]
- Fernández-de-las-Peñas, C. Long COVID: Current definition. Infection 2022, 50, 285–286. [Google Scholar] [CrossRef] [PubMed]
- Daniel, A. Office for National Statistics. Available online: https://blog.ons.gov.uk/2021/09/16/how-common-is-long-covid-that-depends-on-how-you-measure-it/ (accessed on 16 September 2021).
- Groff, D.; Sun, A.; Ssentongo, A.E.; Ba, D.M.; Parsons, N.; Poudel, G.R.; Lekoubou, A.; Oh, J.S.; Ericson, J.E.; Ssentongo, P.; et al. Short-Term and Long-Term Rates of Postacute Sequelae of SARS-CoV-2 Infection. JAMA Netw. Open 2021, 4, e2128568. [Google Scholar] [CrossRef] [PubMed]
- First Findings from World’s Largest Study on Long COVID in Children. UCLHome, 2 September 2021; 1–4.
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post COVID-19 condition by a delphi consensus. Lancet Infect. Dis. 2021, 22, 2019–2022. [Google Scholar] [CrossRef]
- National Institute for Health and Care Research. Available online: https://www.nihr.ac.uk/news/new-definitions-for-long-covid-developed-with-patients-and-carers/29865?pr= (accessed on 8 February 2022).
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re’em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Osuchowski, M.F.; Winkler, M.S.; Skirecki, T.; Cajander, S.; Shankar-Hari, M.; Lachmann, G.; Monneret, G.; Venet, F.; Bauer, M.; Brunkhorst, F.M.; et al. The COVID-19 puzzle: Deciphering pathophysiology and phenotypes of a new disease entity. Lancet Respir. Med. 2021, 9, 622–642. [Google Scholar] [CrossRef]
- Charfeddine, S.; Ibn Hadj Amor, H.; Jdidi, J.; Torjmen, S.; Kraiem, S.; Hammami, R.; Bahloul, A.; Kallel, N.; Moussa, N.; Touil, I.; et al. Long COVID 19 syndrome: Is it related to microcirculation and endothelial dysfunction? Insights from TUN-EndCOVSsudy. Front. Cardiovasc. Med. 2021, 8, 5758. [Google Scholar] [CrossRef]
- Wechsler, J.B.; Butuci, M.; Wong, A.; Kamboj, A.P.; Youngblood, B.A. Mast cell activation is associated with post-acute COVID-19 syndrome. Allergy 2021, 77, 1288–1291. [Google Scholar] [CrossRef]
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; Howe, A.; Munier, C.M.L.; Patel, S.K.; Juno, J.A.; Burrell, L.M.; Kent, S.J.; Dore, G.J.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat. Immunol. 2022, 23, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.; Yuan, D.; Chen, D.G.; Ng, R.H.; Wang, K.; Choi, J.; Li, S.; Hong, S.; Zhang, R.; Xie, J.; et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022, 185, 881–895.e20. [Google Scholar] [CrossRef] [PubMed]
- Mehandru, S.; Merad, M. Pathological sequelae of long-haul COVID. Nat. Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, S. Computing the Levenshtein distance of a regular language. IEEE Inform. Theory Workshop 2005, 2005, 4. [Google Scholar] [CrossRef]
- Berthold, M.R.; Cebron, N.; Dill, F.; Gabriel, T.R.; Kötter, T.; Meinl, T.; Ohl, P.; Sieb, C.; Thiel, K.; Wiswedel, B. KNIME: The Konstanz Information Miner; Springer: Berlin/Heidelberg, Germany, 2008; pp. 319–326. [Google Scholar]
- Salzberg, S.L. C4.5: Programs for Machine Learning by J. Ross Quinlan. In Machine Learning; Morgan Kaufmann Publishers Inc.: Burlington, MA, USA, 1994; Volume 16, pp. 235–240. [Google Scholar] [CrossRef] [Green Version]
- Shafer, J.; Mehta, M.; Agrawal, R.; Jose, S. SPRINT: A Scalable. In Extending Database Technology; IBM Almaden Research Center: San Jose, CA, USA, 1996; pp. 544–555. [Google Scholar]
- Breiman, L.; Friedman, J.H.; Olshen, R.A.; Stone, C.J. Classification and Regression Trees; Routledge: London, UK, 2017; ISBN 9781315139470. [Google Scholar]
- Otte, E.; Rousseau, R. Social network analysis: A powerful strategy, also for the information sciences. J. Inform. Sci. 2002, 28, 441–453. [Google Scholar] [CrossRef]
- Collins, F.S. NIH Launches New Initiative to Study “Long COVID”; National Institutes of Health (NIH): Bethesda, MD, USA; U.S. Department of Health and Human Services: Washington, DC, USA, 2021; pp. 2–3. [Google Scholar]
- Stefanou, M.-I.; Palaiodimou, L.; Bakola, E.; Smyrnis, N.; Papadopoulou, M.; Paraskevas, G.P.; Rizos, E.; Boutati, E.; Grigoriadis, N.; Krogias, C.; et al. Neurological manifestations of Long-COVID syndrome: A narrative review. Ther. Adv. Chronic Dis. 2022, 13, 204062232210768. [Google Scholar] [CrossRef]
- d’Ettorre, G.; GentiliniCacciola, E.; Santinelli, L.; de Girolamo, G.; Spagnolello, O.; Russo, A.; Tarsitani, L.; Ciccozzi, M.; Mastroianni, C.M.; d’Ettorre, G.; et al. COVID-19 sequelae in working age patients: A systematic review. J. Med. Virol. 2022, 94, 858–868. [Google Scholar] [CrossRef]
- Ohla, K.; Geraldine Veldhuizen, M.; Green, T.; Hannum, M.E.; Bakke, A.J.; Moein, S.; Tognetti, A.; Postma, E.M.; Pellegrino, R.; Hwang, L.-D.; et al. A follow-up on quantitative and qualitative olfactory dysfunction and other symptoms in patients recovering from COVID-19 smell loss. Rhinology 2022. [Google Scholar] [CrossRef]
- Pérez-González, A.; Araújo-Ameijeiras, A.; Fernández-Villar, A.; Crespo, M.; Poveda, E. Long COVID in hospitalized and non-hospitalized patients in a large cohort in Northwest Spain, a prospective cohort study. Sci. Rep. 2022, 12, 3369. [Google Scholar] [CrossRef]
- Sareen, T.A.; Kang, A.K.; Patel, T.R.; Clark, J.R.; Perez-Giraldo, G.S.; Orban, Z.S.; Lim, P.H.; Jimenez, M.; Graham, E.L.; Batra, A.; et al. Evolution of neurologic symptoms in non-hospitalized COVID-19 "long haulers”. Ann. Clin. Transl. Neurol. 2022. ahead of print. [Google Scholar] [CrossRef]
- Titze-de-Almeida, R.; da Cunha, T.R.; dos Santos Silva, L.D.; Ferreira, C.S.; Silva, C.P.; Ribeiro, A.P.; de Castro Moreira Santos Júnior, A.; de Paula Brandão, P.R.; Silva, A.P.B.; da Rocha, M.C.O.; et al. Persistent, new-onset symptoms and mental health complaints in long COVID in a brazilian cohort of non-hospitalized patients. BMC Infect. Dis. 2022, 22, 133. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Barmparessou, Z.; Athanasiou, N.; Sakka, E.; Eleftheriou, K.; Patrinos, S.; Sakkas, N.; Pappas, A.; Kalomenidis, I.; Katsaounou, P. Depression, insomnia and post-traumatic stress disorder in COVID-19 survivors: Role of gender and impact on quality of life. J. Pers. Med. 2022, 12, 486. [Google Scholar] [CrossRef] [PubMed]
- Katsarou, M.S.; Giakoumaki, M.; Papadimitriou, A.; Demertzis, N.; Androutsopoulos, V.; Drakoulis, N. Genetically driven antioxidant capacity in a caucasian southeastern european population. Mech. Ageing Dev. 2018, 172, 1–5. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Please select your age (in years) |
| 2. Sex |
| 3. Elapsed number of months since you experience symptoms after COVID-19 infection |
| 4. Long COVID symptoms (please use a comma to separate each symptom) |
| 5. Have you been hospitalized? |
| 6. Do you have work issues from the prolonged illness due to Long COVID? |
| 7. Do you have understanding and support in your professional life? |
| -I am self-employed |
| -I have not returned to my work yet |
| 8. Do you have understanding and support from your family? |
| 9. Are you being monitored in any public hospital? |
| 10. Have you found appropriate medical support and monitoring? |
| -Yes, in the public sector |
| -Yes, at private Medical doctors |
| -Yes, in the public sector and private medical doctors |
| 11. Have you visited several doctors in order to find a solution to your symptoms? |
| 12. Have you encountered medical doctors who were not aware of the Long COVID syndrome? |
| They have heard about Long COVID but were not fully aware of its symptoms |
| 13. How much (in Euros) have you spent on doctor visits due to Long COVID? |
| 14. Have you had any rehabilitation treatment? |
| Hospitalized (n =64) | Non-Hospitalized (n =144) | p-Value | |
|---|---|---|---|
| Male Female Fatigue | 33.84% (22/64) | 17.34% (25/144) | 0.00677 |
| 64.61% (42/64) | 82.6% (119/144) | 0.00677 | |
| 71.87% (46/64) | 69.44% (100/144) | 0.72356 | |
| Musculoskeletal symptoms Cognitive disorders Mood disorders | 64.06% (41/64) | 45.80% (66/144) | 0.01519 |
| 46.15% (30/64) 18.75% (12/64) | 38.19 (55/144) 6.94 (10/144) | 0.27820 0.01061 | |
| Palpitations Parosmia Olfactory disorders (incl.parosmia) At least one neurological (excl. fatigue) | 26.56% (17/64) | 28.4% (41/144) | 0.77681 |
| 1.56% (1/64) | 13.19% (19/144) | 0.00862 | |
| 3.13% (2/64) | 22.22% (32/144) | 0.00058 | |
| 75.00% (48/64) | 77.77% (112/144) | 0.66076 | |
| Shortness of breath Dermatological | 23.43% (15/64) | 15.27% (22/144) | 0.15552 |
| 18.75% (12/64) | 18.05% (26/144) | 0.90478 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katsarou, M.-S.; Iasonidou, E.; Osarogue, A.; Kalafatis, E.; Stefanatou, M.; Pappa, S.; Gatzonis, S.; Verentzioti, A.; Gounopoulos, P.; Demponeras, C.; et al. The Greek Collaborative Long COVID Study: Non-Hospitalized and Hospitalized Patients Share Similar Symptom Patterns. J. Pers. Med. 2022, 12, 987. https://doi.org/10.3390/jpm12060987
Katsarou M-S, Iasonidou E, Osarogue A, Kalafatis E, Stefanatou M, Pappa S, Gatzonis S, Verentzioti A, Gounopoulos P, Demponeras C, et al. The Greek Collaborative Long COVID Study: Non-Hospitalized and Hospitalized Patients Share Similar Symptom Patterns. Journal of Personalized Medicine. 2022; 12(6):987. https://doi.org/10.3390/jpm12060987
Chicago/Turabian StyleKatsarou, Martha-Spyridoula, Eleni Iasonidou, Alexander Osarogue, Efthymios Kalafatis, Maria Stefanatou, Sofia Pappa, Stylianos Gatzonis, Anastasia Verentzioti, Pantelis Gounopoulos, Christos Demponeras, and et al. 2022. "The Greek Collaborative Long COVID Study: Non-Hospitalized and Hospitalized Patients Share Similar Symptom Patterns" Journal of Personalized Medicine 12, no. 6: 987. https://doi.org/10.3390/jpm12060987