
High-Sensitivity Troponin T: A Potential Safety Predictive Biomarker for Discharge from the Emergency Department of Patients with Confirmed Influenza

 , ,
, ,
Abstract
:1. Introduction
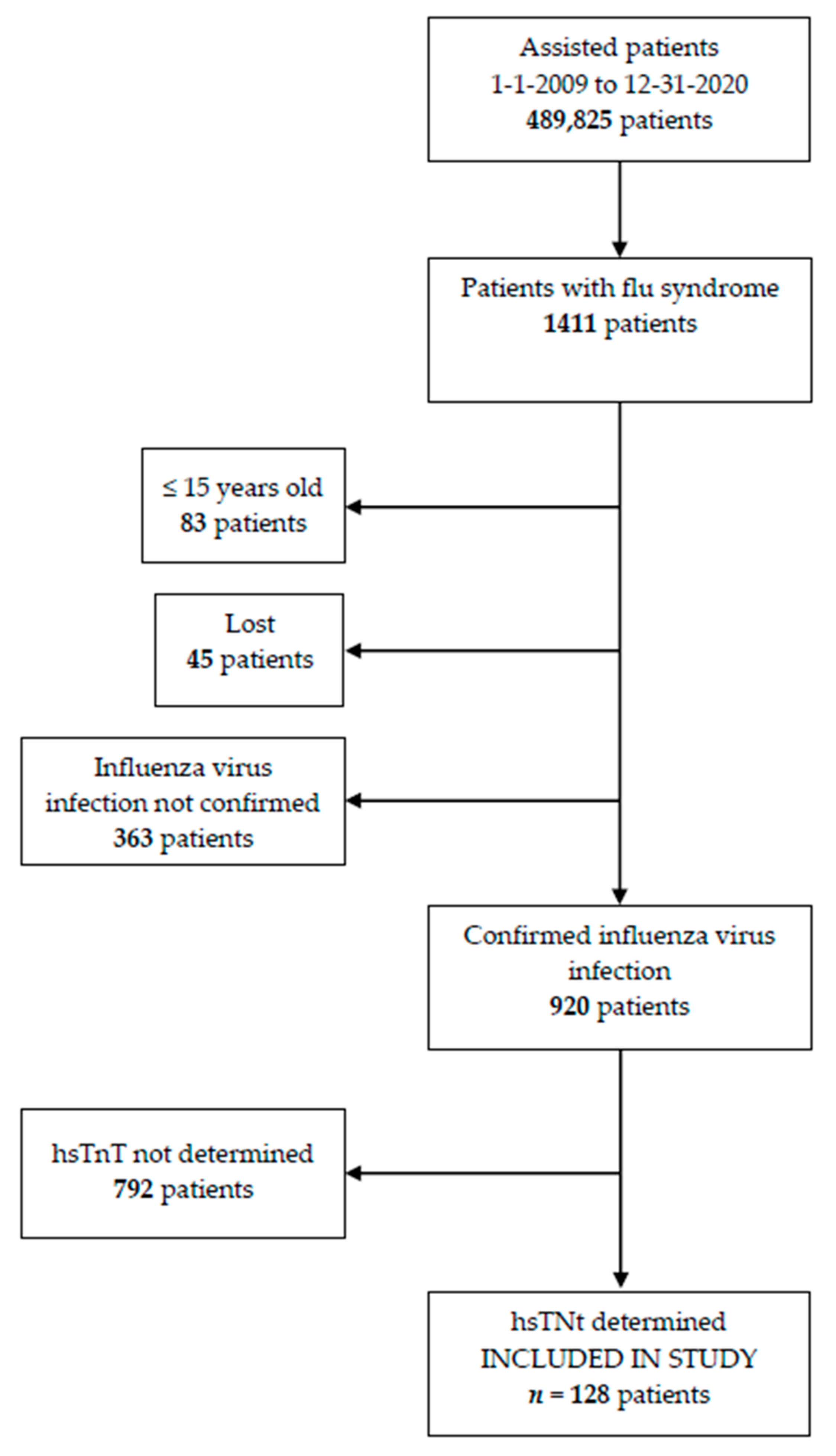
2. Materials and Methods
2.1. Enrolled Patients’ Characteristics
2.2. Diagnostic
2.3. Statistical Analysis
2.4. Bioethical Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Available online: https://www.who.int/mediacentre/infographic/influenza/en/ (accessed on 11 May 2021).
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Global Seasonal Influenza-associated Mor-tality Collaborator Network. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Consumo y Bienestar Social. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/programasDeVacunacion/gripe/faq/home.htm#:~:text=En%20la%20temporada%202019%2D2020%20se%20produjeron%2027.700%20hospitalizaciones%2C%201.800,factor%20de%20riesgo%20de%20complicaciones (accessed on 11 May 2021).
- Instituto de Salud Carlos III. Sistema de Vigilancia de la Gripe y otros virus respiratorios en España (SVGE). Available online: https://vgripe.isciii.es/documentos/20202021/boletines/Informe%20semanal%20SVGE%20y%20otros%20virus%20respiratorios_2020-2021_172021.pdf (accessed on 11 May 2021).
- Instituto de Salud Carlos III. Sistema de Vigilancia de la Gripe y Otros Virus Respiratorios en España (SVGE). Available online: https://vgripe.isciii.es/inicio.do;jsessionid=71A23A4BFD707E40C4C9E68F89829CB9 (accessed on 11 May 2021).
- Kunutsor, S.K.; Laukkanen, J.A. Cardiovascular complications in COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, e139–e141. [Google Scholar] [CrossRef] [PubMed]
- Tazón Varela, M.A.; Alonso Valle, H.; Muñoz Cacho, P.; Colomo Mármol, L.F.; Gallo Terán, J.; Hernández Herrero, M. N-terminal fragment of pro-brain natriuretic peptide plasma concentration: A new predictive biomarker for community acquired pneumonia? Emergencias 2014, 26, 94–100. [Google Scholar]
- Tazón-Varela, M.A.; Muñoz-Cacho, P.; Alonso-Valle, H.; Gallo-Terán, J.; Pérez-Mier, L.A.; Colomo-Mármol, L.F. The Amino-Terminal Fragment of Pro-Brain Natriuretic Peptide in Plasma as a Biological Marker for Predicting Mortality in Community-Acquired Pneumonia: A Cohort Study. Eurasian J. Emerg. Med. 2016, 15, 30–38. [Google Scholar] [CrossRef]
- Warren-Gash, C.; Smeeth, L.; Hayward, A. Influenza as a trigger for acute myocardial infarction or death from cardiovascular disease: A systematic review. Lancet Infect. Dis. 2009, 9, 601–610. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F. Cardiac troponin elevation in patients with influenza virus infections. Biomed. J. 2020, 44, 183–189. [Google Scholar] [CrossRef]
- Collins, S.D. Excess Mortality from Causes Other than Influenza and Pneumonia during Influenza Epidemics. Public Health Rep. 1932, 47, 2159. [Google Scholar] [CrossRef]
- Kwong, J.C.; Schwartz, K.L.; Campitelli, M.A.; Chung, H.; Crowcroft, N.S.; Karnauchow, T.; Katz, K.; Ko, D.; McGeer, A.J.; McNally, D.; et al. Acute Myocardial Infarction after Laboratory-Confirmed Influenza Infection. New Engl. J. Med. 2018, 378, 345–353. [Google Scholar] [CrossRef]
- Sellers, S.A.; Hagan, R.S.; Hayden, F.G.; Fischer, W.A. The hidden burden of influenza: A review of the extra-pulmonary complications of influenza infection. Influ. Other Respir. Viruses 2017, 11, 372–393. [Google Scholar] [CrossRef] [PubMed]
- López-Fernández, L.; López-Messa, J.; Llano, J.A.-D.; Garmendia-Leiza, J.R.; García-Cruces, J.; García-Crespo, J. Relación entre las tasas de gripe estacional y las tasas de hospitalización y mortalidad hospitalaria por enfermedades cardiovasculares agudas en una región española. Med. Clin. 2019, 153, 133–140. [Google Scholar] [CrossRef]
- Barnes, M.; E Heywood, A.; Mahimbo, A.; Rahman, B.; Newall, A.; MacIntyre, C.R. Acute myocardial infarction and influenza: A meta-analysis of case–control studies. Heart 2015, 101, 1738–1747. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, A.; Lucero-Obusan, C.; Schirmer, P.; Winston, C.; Holodniy, M. Acute cardiac injury events ≤ 30 days after laboratory-confirmed influenza virus infection among U.S.veterans, 2010–2012. BMC Cardiovasc. Disord. 2015, 15, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tazón-Varela, M.; Alonso-Valle, H.; Muñoz-Cacho, P.; Gallo-Terán, J.; Piris-García, X.; Pérez-Mier, L. Aumento de microorganismos no habituales en la neumonía adquirida en la comunidad. SEMERGEN-Med. Fam. 2017, 43, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- Azar, R.R.; Sarkis, A.; Giannitsis, E. A Practical Approach for the Use of High-Sensitivity Cardiac Troponin Assays in the Evaluation of Patients With Chest Pain. Am. J. Cardiol. 2020, 139, 1–7. [Google Scholar] [CrossRef]
- Lee, N.; Ison, M.G. Diagnosis, management and outcomes of adults hospitalized with influenza. Antivir. Ther. 2012, 17, 143–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, J.; Shah, P.J.; Korimilli, V.; Win, H. Frequency of troponin elevations in patients with influenza infection during the 2017–2018 influenza season. IJC Hear. Vasc. 2019, 22, 145–147. [Google Scholar] [CrossRef]
- Pizzini, A.; Burkert, F.; Theurl, I.; Weiss, G.; Bellmann-Weiler, R. Prognostic impact of high sensitive Troponin T in patients with influenza virus infection: A retrospective analysis. Hear. Lung 2020, 49, 105–109. [Google Scholar] [CrossRef]
- Gobierno de España. Ministerio de Sanidad. Sistema de Información de Atención Especializada (SIAE). Registro de Actividad de Atención Especializada. RAE-CMBD. Available online: https://www.sanidad.gob.es/estadEstudios/estadisticas/cmbdhome.htm (accessed on 11 May 2021).
- Sharma, Y.; Horwood, C.; Chua, A.; Hakendorf, P.; Thompson, C. Prognostic impact of high sensitive troponin in predicting 30-day mortality among patients admitted to hospital with influenza. IJC Hear. Vasc. 2020, 32, 100682. [Google Scholar] [CrossRef]
- Rezkalla, S.H.; Kloner, R.A. Viral myocarditis: 1917–2020: From the Influenza A to the COVID-19 pandemics. Trends Cardiovasc. Med. 2020, 31, 163–169. [Google Scholar] [CrossRef]
- Cuadrado-Payán, E.; Montagud-Marrahi, E.; Torres-Elorza, M.; Bodro, M.; Blasco, M.; Poch, E.; Soriano, A.; Piñeiro, G.J. SARS-CoV-2 and influenza virus co-infection. Lancet 2020, 395, e84. [Google Scholar] [CrossRef]
- Ma, S.; Lai, X.; Chen, Z.; Tu, S.; Qin, K. Clinical characteristics of critically ill patients co-infected with SARS-CoV-2 and the influenza virus in Wuhan, China. Int. J. Infect. Dis. 2020, 96, 683–687. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Chart. General Characteristics of the Sample. | |||||
|---|---|---|---|---|---|
| SURVIVORS (n = 124) | DECEASED (n = 4) | p-Value | |||
| n | % | n | % | ||
| SOCIODEMOGRAPHIC VARIABLES | |||||
| Age (years) [mean (SD)] | 68.2 | 15.7 | 85.8 | 4.9 | 0.008 |
| Female sex | 46 | 37.1 | 3 | 75 | 0.156 |
| ASSOCIATED COMORBIDITY | |||||
| Active smoker (n = 19) | 19 | 15.3 | 0 | 0 | 0.822 |
| Essential hypertension (n = 79) | 76 | 61.3 | 3 | 75 | 0.504 |
| DM-1 (n = 2) | 2 | 1.6 | 0 | 0 | 0.936 |
| DM-2 (n = 28) | 28 | 22.6 | 0 | 0 | 0.546 |
| Dyslipidemia (n = 57) | 56 | 45.2 | 1 | 25 | 0.396 |
| Heart failure (n = 15) | 14 | 11.3 | 1 | 25 | 0.396 |
| Ischemic heart disease (n = 25) | 25 | 20.2 | 0 | 0 | 0.414 |
| Cardiac arrhythmia (n = 22) | 21 | 16.9 | 1 | 25 | 0.534 |
| Asthma (n = 14) | 12 | 9.7 | 2 | 50 | 0.059 |
| COPD (n = 26) | 25 | 20.2 | 1 | 25 | 0.813 |
| Chronic Kidney Disease (n = 12) | 11 | 8.9 | 1 | 25 | 0.329 |
| Chronic liver disease (n = 12) | 11 | 8.9 | 1 | 25 | 0.546 |
| Cognitive dysfunction (n = 7) | 5 | 4 | 2 | 50 | 0.015 |
| Neoplasia (n = 11) | 10 | 8.1 | 1 | 25 | 0.305 |
| CLINICAL PRESENTING VARIABLES | |||||
| Dyspneic feeling (n = 65) | 61 | 49.2 | 4 | 100 | 0.062 |
| Body temperature (ºC) [mean (SD)] (n = 125) | 37.1 | 0.9 | 36.8 | 0.4 | 0.487 |
| HR (bpm) [median (IQR)] (n = 124) | 88 | 28.3 | 71 | 7.3 | 0.035 |
| RF (rpm) [median (IQR)] (n = 67) | 15 | 6 | 14.5 | 2.5 | 0.716 |
| TAS (mmHg) [median (IQR)] (n = 126) | 136 | 37.3 | 140 | 37.3 | 0.765 |
| DBP (mmHg) [median (IQR)] (n = 126) | 75 | 17.3 | 78.5 | 22.3 | 0.440 |
| Pulse oximetry (n = 119) | 96 | 4 | 86.5 | 4 | 0.002 |
| ANALYTICAL VARIABLES | |||||
| Leukocytes x103/µL [median (IQR)] (n = 127) | 8000 | 4100 | 7250 | 4575 | 0.310 |
| Neutrophils x103/µL [median (IQR)] (n = 125) | 5450 | 3825 | 5400 | 1800 | 0.904 |
| Lymphocytes x103/µL [median (IQR)] (n = 125) | 900 | 900 | 800 | 700 | 0.784 |
| Hematocrit % [median (IQR)] (n = 127) | 41 | 6.2 | 41.3 | 11.3 | 0.836 |
| Hemoglobin g/dL [median (IQR)] (n = 127) | 13.6 | 1.9 | 13.7 | 4 | 0.820 |
| Platelets x103/µL [median (IQR)] (n = 126) | 176 | 74 | 140 | 99 | 0.300 |
| Glucose mg/dL [median (IQR)] (n = 127) | 126 | 73 | 144.5 | 64 | 0.945 |
| Urea mg/dL [median (IQR)] (n = 127) | 41 | 26 | 38.5 | 17.8 | 0.709 |
| Creatinine mg/dL [median (IQR)] (n = 126) | 0.91 | 0.33 | 1.17 | 0.78 | 0.337 |
| Sodium mEq/L [median (IQR)] (n = 124) | 136 | 4 | 139 | 3 | 0.214 |
| Potassium mEq/L [median (IQR)] (n = 120) | 4.2 | 0.7 | 4.2 | 0.8 | 0.372 |
| Bilirubin mg/dL [median (IQR)] (n = 56) | 0.4 | 0.4 | 0.5 | 0.2 | 0.941 |
| Prothrombin time % [median (IQR)] (n = 119) | 88 | 30 | 64 | 75 | 0.272 |
| Arterial pH [median (IQR)] (n = 100) | 7.45 | 0.06 | 7.41 | 0.07 | 0.085 |
| pO2 mmHg [median (IQR)] (n = 99) | 62 | 16 | 53.5 | 8.5 | 0.052 |
| pCO2 mmHg [median (IQR)] (n = 100) | 36.5 | 9 | 40.5 | 8 | 0.149 |
| BIOMARKERS | |||||
| CRP mg/dL [median (IQR)] (n = 124) | 3.8 | 8.4 | 1.9 | 1.1 | 0.095 |
| Lactate mg/dL [median (IQR)] (n = 22) | 14 | 10 | 13 | 0 | 0.909 |
| NT-proBNP ng/L [median (IQR)] (n = 71) | 575 | 2186 | 3481 | 4408 | 0.077 |
| hsTnT ng/L [median (IQR)] (n = 128) | 14.5 | 16 | 40.5 | 266.5 | 0.012 |
| RADIOLOGICAL CHARACTERISTICS | |||||
| Chest X-ray performed (n = 124) | 120 | 96.8 | 4 | 100 | 0.936 |
| Parenchymal condensation/infiltrate (n = 27) | 27 | 21.8 | 0 | 0 | 0.383 |
| Pleural effusion (n = 3) | 2 | 1.6 | 1 | 25 | 0.009 |
| EVOLUTION VARIABLES | |||||
| Entrance to conventional ward (n = 88) | 84 | 67.7 | 4 | 100 | 0.391 |
| Admission to intensive care unit (n = 2) | 2 | 1.6 | 0 | 0 | 0.936 |
| Days of survival in deceased [mean (SD)] | - | - | 7.3 | 5.6 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tazón-Varela, M.A.; Ortiz de Salido-Menchaca, J.; Muñoz-Cacho, P.; Iriondo-Bernabeu, E.; Martos-Almagro, M.J.; Lavín-López, E.; Vega-Zubiaur, A.; Escalona-Canal, E.J.; Alcalde-Díez, I.; Gómez-Vildosola, C.; et al. High-Sensitivity Troponin T: A Potential Safety Predictive Biomarker for Discharge from the Emergency Department of Patients with Confirmed Influenza. J. Pers. Med. 2022, 12, 520. https://doi.org/10.3390/jpm12040520
Tazón-Varela MA, Ortiz de Salido-Menchaca J, Muñoz-Cacho P, Iriondo-Bernabeu E, Martos-Almagro MJ, Lavín-López E, Vega-Zubiaur A, Escalona-Canal EJ, Alcalde-Díez I, Gómez-Vildosola C, et al. High-Sensitivity Troponin T: A Potential Safety Predictive Biomarker for Discharge from the Emergency Department of Patients with Confirmed Influenza. Journal of Personalized Medicine. 2022; 12(4):520. https://doi.org/10.3390/jpm12040520
Chicago/Turabian StyleTazón-Varela, Manuel Antonio, Jon Ortiz de Salido-Menchaca, Pedro Muñoz-Cacho, Enara Iriondo-Bernabeu, María Josefa Martos-Almagro, Emma Lavín-López, Ander Vega-Zubiaur, Edgar José Escalona-Canal, Iratxe Alcalde-Díez, Carmen Gómez-Vildosola, and et al. 2022. "High-Sensitivity Troponin T: A Potential Safety Predictive Biomarker for Discharge from the Emergency Department of Patients with Confirmed Influenza" Journal of Personalized Medicine 12, no. 4: 520. https://doi.org/10.3390/jpm12040520