
Effectiveness of Virtual Reality-Based Training on Oral Healthcare for Disabled Elderly Persons: A Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Randomization and Allocation
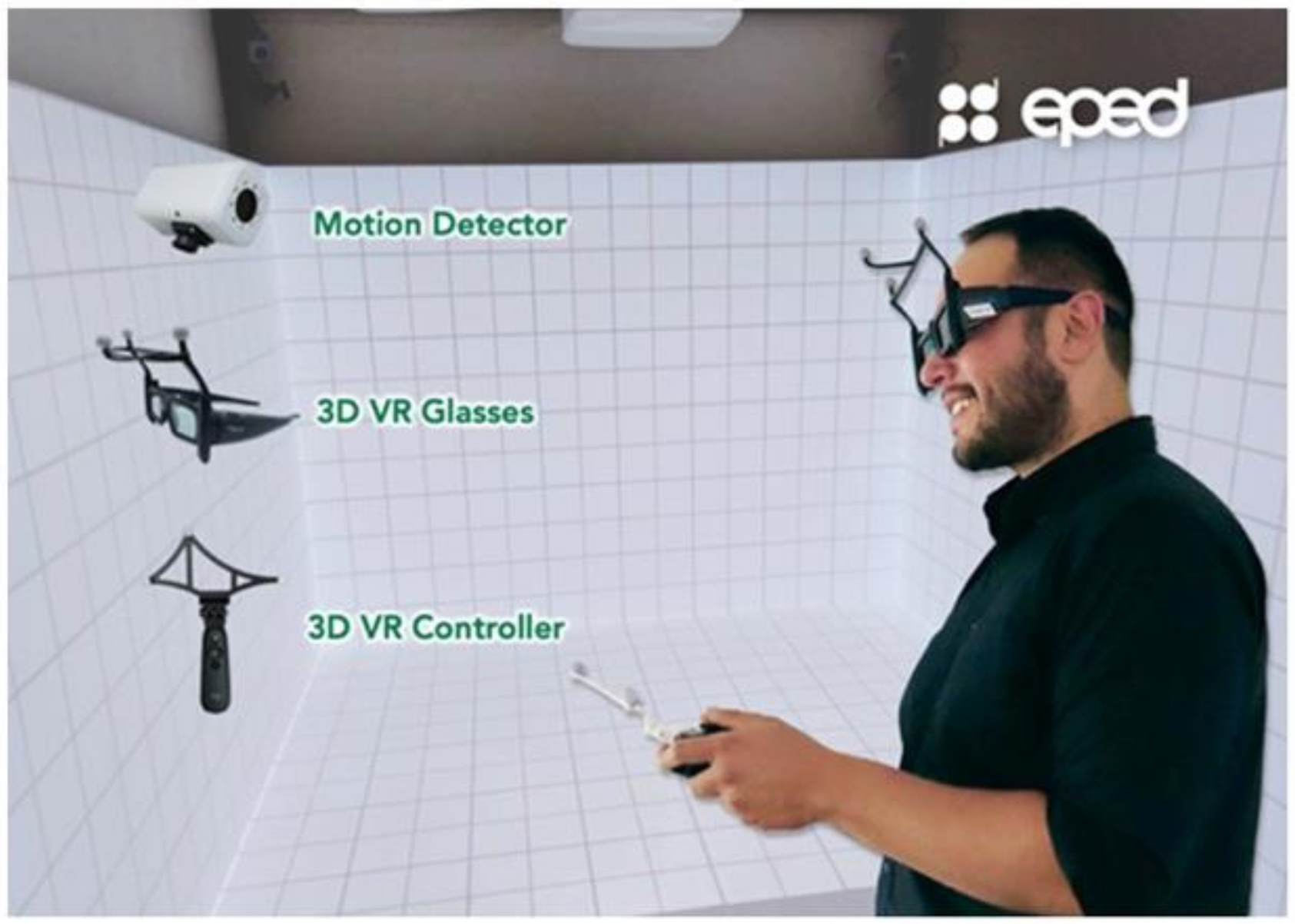
2.3. Instrument
2.4. Outcome Measures
2.4.1. Oral Care-Related Knowledge
2.4.2. Attitude toward Oral Healthcare
2.4.3. Self-Efficacy of Oral Healthcare
2.4.4. Intention to Assist in Oral Care Behaviors
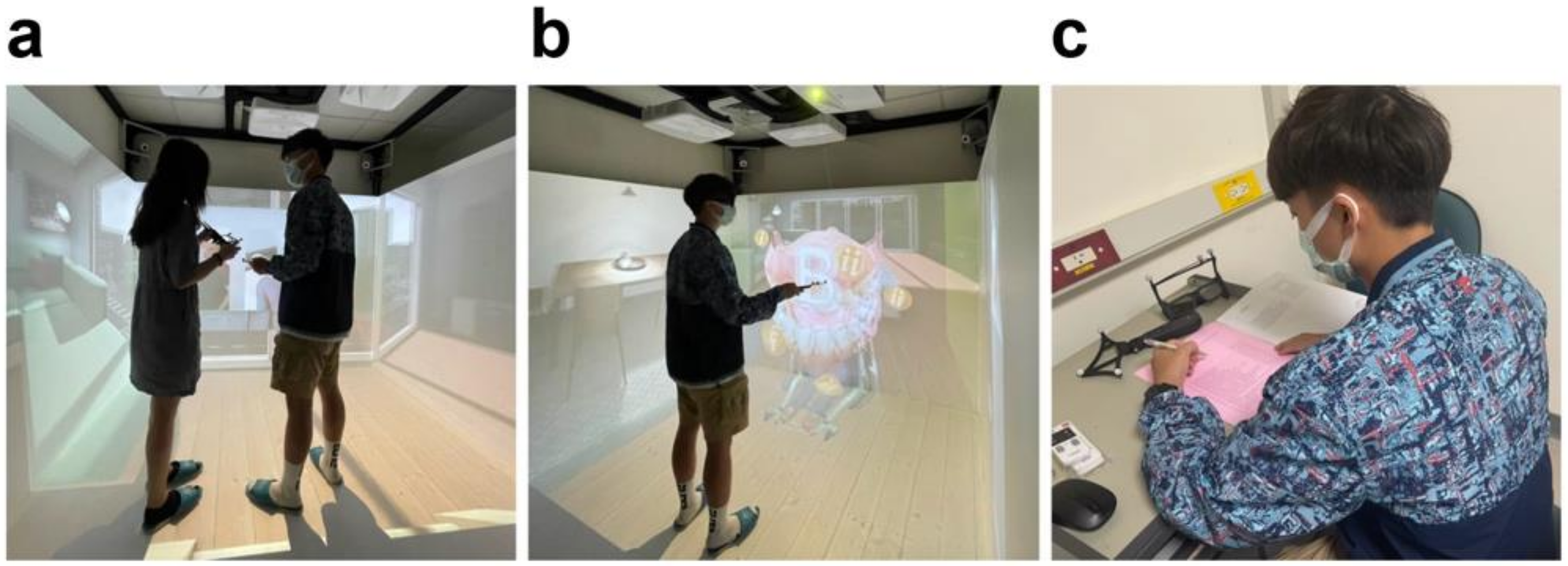
2.5. Interventions
2.6. Data Collection
2.7. Statistical Analysis
3. Results
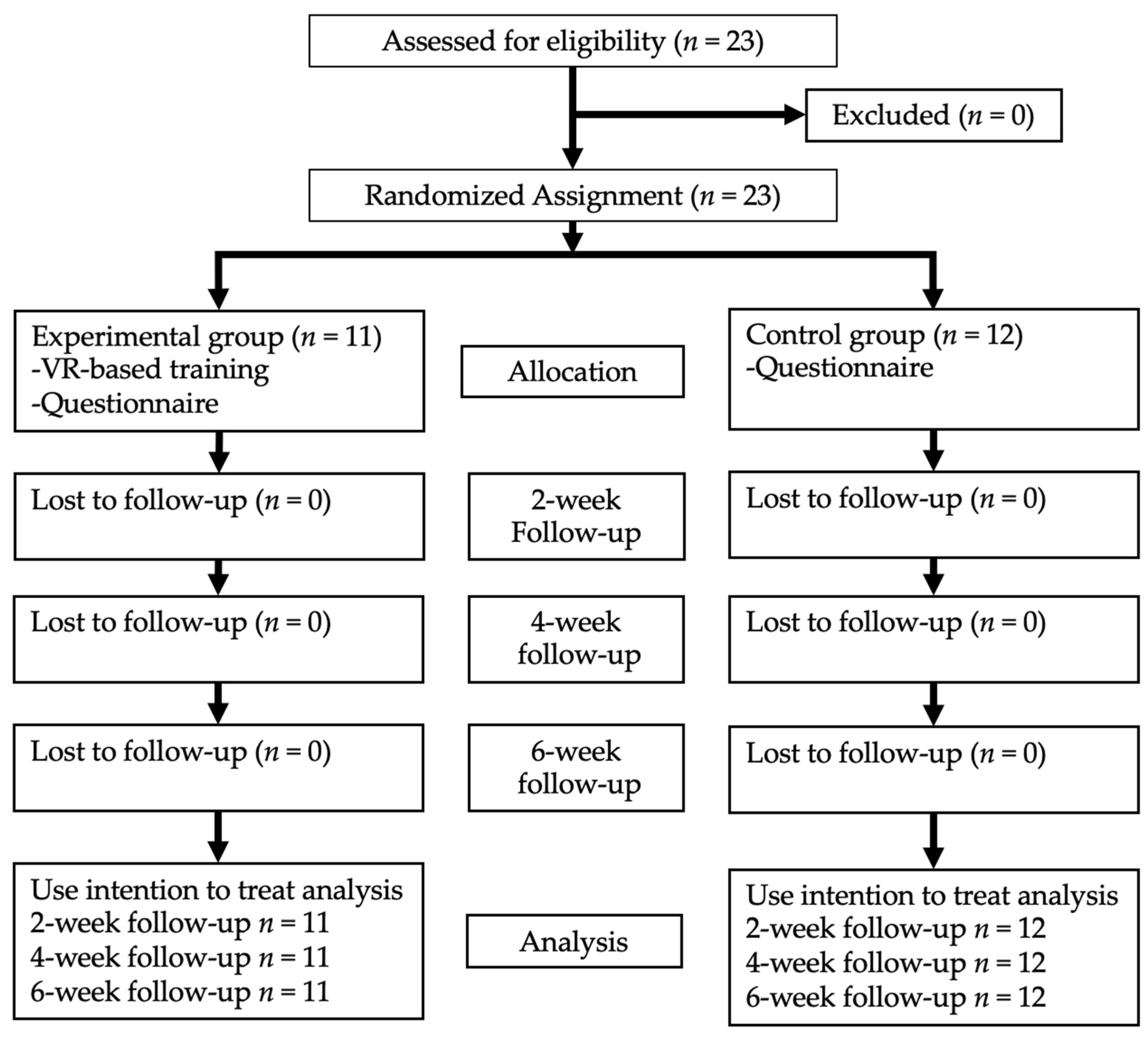
3.1. Recruitment
3.2. Baseline Information between the Two Groups
3.3. Intervention Effects on Knowledge, Attitude, Self-Efficacy, and Intentions
3.4. Intervention Effects on Intention to Assist in Oral Care Behaviors
3.5. SUS of the VR-Based System
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Pottle, J. Virtual reality and the transformation of medical education. Future Health J. 2019, 6, 181–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graafland, M.; Schraagen, J.M.; Schijven, M.P. Systematic review of serious games for medical education and surgical skills training. Br. J. Surg. 2012, 99, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Abe, S.; Noguchi, N.; Matsuka, Y.; Shinohara, C.; Kimura, T.; Oka, K.; Okura, K.; Rodis, O.M.M.; Kawano, F. Educational effects using a robot patient simulation system for development of clinical attitude. Eur. J. Dent. Educ. 2018, 22, e327–e336. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, C.; Jamal, A.; Nguyen, R.; Kudryk, A.; Mann, J.; Mendez, I. Immersive and interactive virtual reality to improve learning and retention of neuroanatomy in medical students: A randomized controlled study. CMAJ Open 2018, 6, E103–E109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Towers, A.; Field, J.; Stokes, C.; Maddock, S.; Martin, N. A scoping review of the use and application of virtual reality in pre-clinical dental education. Br. Dent. J. 2019, 226, 358–366. [Google Scholar] [CrossRef]
- Li, Y.; Ye, H.; Ye, F.; Liu, Y.; Lv, L.; Zhang, P.; Zhang, X.; Zhou, Y. The Current Situation and Future Prospects of Simulators in Dental Education. J. Med Internet Res. 2021, 23, e23635. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.-K.; Yang, C.-H.; Hsieh, Y.-H.; Wang, J.-C.; Hung, C.-C. Augmented reality (AR) and virtual reality (VR) applied in dentistry. Kaohsiung J. Med Sci. 2018, 34, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Luciano, C.; Banerjee, P.; DeFanti, T. Haptics-based virtual reality periodontal training simulator. Virtual Real. 2009, 13, 69–85. [Google Scholar] [CrossRef]
- Welk, A.; Splieth, C.; Rosin, M.; Kordas, B.; Meyer, G. DentSim-a future teaching option for dentists. Int. J. Comput. Dent. 2004, 7, 123–130. [Google Scholar]
- Kishimoto, N.; Mukai, N.; Honda, Y.; Hirata, Y.; Tanaka, M.; Momota, Y. Simulation training for medical emergencies in the dental setting using an inexpensive software application. Eur. J. Dent. Educ. 2018, 22, e350–e357. [Google Scholar] [CrossRef] [PubMed]
- Roy, E.; Quinsat, V.E.; Bazin, O.; Lesclous, P.; Lejus-Bourdeau, C. High-fidelity simulation in training dental students for medical life-threatening emergency. Eur. J. Dent. Educ. 2018, 22, e261–e268. [Google Scholar] [CrossRef]
- Soltanimehr, E.; Bahrampour, E.; Imani, M.M.; Rahimi, F.; Almasi, B.; Moattari, M. Effect of virtual versus traditional education on theoretical knowledge and reporting skills of dental students in radiographic interpretation of bony lesions of the jaw. BMC Med. Educ. 2019, 19, 233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbankova, A. Impact of Computerized Dental Simulation Training on Preclinical Operative Dentistry Examination Scores. J. Dent. Educ. 2010, 74, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Quinn, F.; Keogh, P.; McDonald, A.; Hussey, D. A study comparing the effectiveness of conventional training and virtual reality simulation in the skills acquisition of junior dental students. Eur. J. Dent. Educ. 2003, 7, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Leblanc, V.R.; Urbankova, A.; Hadavi, F.; Lichtenthal, R.M. A Preliminary Study in Using Virtual Reality to Train Dental Students. J. Dent. Educ. 2004, 68, 378–383. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Department of Economic and Social Affairs Population Dynamics. Revis. World Popul. Prospect. 2019. Available online: https://population.un.org/wpp2019/ (accessed on 13 December 2021).
- National Development Council. Taiwan Executive Yuan, Population Estimation. 2020. Available online: https://www.ndc.gov.tw/Content_List.aspx? (accessed on 13 December 2021).
- Batchelor, P. The changing epidemiology of oral diseases in the elderly, their growing importance for care and how they can be managed. Age Ageing 2015, 44, 1064–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Red, A.; O’Neal, P.V. Implementation of an Evidence-Based Oral Care Protocol to Improve the Delivery of Mouth Care in Nursing Home Residents. J. Gerontol. Nurs. 2020, 46, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Warren, C.; Medei, M.K.; Wood, B.; Schutte, D. A Nurse-Driven Oral Care Protocol to Reduce Hospital-Acquired Pneumonia. AJN Am. J. Nurs. 2019, 119, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.; Edwards, S.; Whiting, G.; Donnelly, F. Evaluating student learning outcomes in oral health knowledge and skills. J. Clin. Nurs. 2018, 27, 2438–2449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, H.; Steinsbekk, A. Is individual practice in an immersive and interactive virtual reality application non-inferior to practicing with traditional equipment in learning systematic clinical observation? A randomized controlled trial. BMC Med. Educ. 2020, 20, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohre, R.; Bois, A.J.; Pollock, J.W.; Lapner, P.; McIlquham, K.; Athwal, G.S.; Goel, D.P. Effectiveness of Immersive Virtual Reality on Orthopedic Surgical Skills and Knowledge Acquisition Among Senior Surgical Residents: A Randomized Clinical Trial. JAMA Netw Open 2020, 3, e2031217. [Google Scholar] [CrossRef]
- Aksoy, E. Comparing the Effects on Learning Outcomes of Tablet-Based and Virtual Reality–Based Serious Gaming Modules for Basic Life Support Training: Randomized Trial. JMIR Serious Games 2019, 7, e13442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J. SUS: A ’Quick and Dirty’ Usability Scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Lewis, J.R. The System Usability Scale: Past, Present, and Future. Int. J. HumaŽ Comput. Interact. 2018, 34, 577–590. [Google Scholar] [CrossRef]
- Kotrlik, J.; Williams, H.A. The Incorporation of Effect Size in The Incorporation of Effect Size in Information Technology, Learning, Information Technology, Learning, and Performance Research and Performance Research. Inf. Technol. Learn. Perform. J. 2003, 21, 1. [Google Scholar]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. Ann. Intern. Med. 2010, 152, 726–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stepan, K.; Zeiger, J.; Hanchuk, S.; Del Signore, A.; Shrivastava, R.; Govindaraj, S.; Iloreta, A. Immersive virtual reality as a teaching tool for neuroanatomy. Int. Forum Allergy Rhinol. 2017, 7, 1006–1013. [Google Scholar] [CrossRef]
- Serrano, C.; Wesselink, P.; Vervoorn, J. Real patients in virtual reality: The link between phantom heads and clinical dentistry. Ned. Tijdschr. Voor Tandheelkd. 2018, 125, 263–267. [Google Scholar] [CrossRef]
- Zaveri, P.P.; Davis, A.B.; O’Connell, K.J.; Willner, E.; Schinasi, D.A.A.; Ottolini, M. Virtual Reality for Pediatric Sedation: A Randomized Controlled Trial Using Simulation. Cureus 2016, 8, e486. [Google Scholar] [CrossRef] [Green Version]
- Ingrassia, P.L.; Ragazzoni, L.; Carenzo, L.; Colombo, D.; Gallardo, A.R.; Della Corte, F. Virtual reality and live simulation: A comparison between two simulation tools for assessing mass casualty triage skills. Eur. J. Emerg. Med. 2015, 22, 121–127. [Google Scholar] [CrossRef]
- Khan, R.; Plahouras, J.; Johnston, B.C.; Scaffidi, M.A.; Grover, S.C.; Walsh, C.M. Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy. Cochrane Database Syst. Rev. 2018, 2018, CD008237. [Google Scholar] [CrossRef] [PubMed]
- Bakhos, D.; Galvin, J.; Aoustin, J.-M.; Robier, M.; Kerneis, S.; Bechet, G.; Montembault, N.; Laurent, S.; Godey, B.; Aussedat, C. Training outcomes for audiology students using virtual reality or traditional training methods. PLoS ONE 2020, 15, e0243380. [Google Scholar] [CrossRef] [PubMed]
- Pike, T.; O’Donnell, V. The impact of clinical simulation on learner self-efficacy in pre-registration nursing education. Nurse Educ. Today 2010, 30, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Meechan-Rogers, R.; Jones, H.; Valler-Jones, T. Students’ perspectives on their skills acquisition and confidence. Br. J. Nurs. 2011, 20, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Sattar, M.U.; Palaniappan, S.; Lokman, A.; Hassan, A.; Shah, N.; Riaz, Z. Effects of Virtual Reality training on medical students’ learning motivation and competency. Pak. J. Med Sci. 2019, 35, 852–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boelen, C.; Heck, J. Defining and Measuring the Social Accountability of Medical Schools; World Health Organization: Geneva, Switzerland, 1995. [Google Scholar]
- Alexander, C.; Millar, J.; Szmidt, N.; Hanlon, K.; Cleland, J. Can new doctors be prepared for practice? A review. Clin. Teach. 2014, 11, 188–192. [Google Scholar] [PubMed]
- Ferguson, G.R.; Bacila, I.A.; Swamy, M. Does current provision of undergraduate education prepare UK medical students in ENT? A systematic literature review. BMJ Open 2016, 6, e010054. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EG (n = 11) | CG (n = 12) | ||||
|---|---|---|---|---|---|
| n | % | n | % | p | |
| Gender | 0.466 | ||||
| Male | 2 | 18.2 | 1 | 8.3 | |
| Female | 9 | 81.8 | 11 | 91.7 | |
| Oral care-related knowledge, mean ± SD † | 18.4 | ±0.3 | 18.9 | ±0.3 | 0.224 |
| Attitude toward oral healthcare, mean ± SD † | 31.0 | ±1.2 | 30.3 | ±0.6 | 0.202 |
| Self-efficacy of oral healthcare, mean ± SD † | 46.0 | ±1.1 | 45.2 | ±1.6 | 0.734 |
| Intention to assist in oral care behaviors, mean ± SD † | 51.6 | ±4.8 | 51.9 | ±5.7 | 0.801 |
| EG (n = 11) | CG (n = 12) | Effect Size d | β | (95% CI) | |
|---|---|---|---|---|---|
| Diff ± SD † | Diff ± SD† | ||||
| Oral Care-Related Knowledge (0–20) | |||||
| Group (EG) × Time (second) | 1.3 ± 1.0 | −0.3 ± 0.5 | 2.05 | 1.61 | (0.92, 2.30) |
| Group (EG) × Time (third) | 1.2 ± 1.5 | −0.2 ± 0.6 | 1.23 | 1.35 | (0.66, 2.04) |
| Group (EG) × Time (fourth) | 1.3 ± 0.9 | 0.1 ± 0.9 | 1.32 | 1.19 | (0.50, 1.88) |
| Effect size a | 1.30 | 0.6 | |||
| Effect size b | 0.80 | 0.33 | |||
| Effect size c | 1.44 | 0.11 | |||
| Attitude toward oral care (7–35) | |||||
| Group (EG) × Time (second) | 1.5 ± 3.6 | −1.3 ± 2.2 | 0.95 | 2.79 | (0.56, 5.02) |
| Group (EG) × Time (third) | 1.3 ± 3.2 | −1.1 ± 3.0 | 0.75 | 2.36 | (0.13, 4.59) |
| Group (EG) × Time (fourth) | 1.7 ± 3.7 | −1.2 ± 4.0 | 0.75 | 2.89 | (0.66, 5.12) |
| Effect size a | 0.42 | 0.59 | |||
| Effect size b | 0.41 | 0.37 | |||
| Effect size c | 0.46 | 0.30 | |||
| Self-efficacy of oral care (11–55) | |||||
| Group (EG) × Time (second) | 6.1 ± 3.9 | −1.1 ± 4.2 | 1.75 | 7.17 | (4.06, 10.29) |
| Group (EG) × Time (third) | 6.8 ± 3.5 | 0.6 ± 6.0 | 1.26 | 6.23 | (3.12, 9.35) |
| Group (EG) × Time (fourth) | 5.8 ± 4.1 | 0.8 ± 5.3 | 1.05 | 4.98 | (1.87, 8.10) |
| Effect size a | 1.56 | 0.26 | |||
| Effect size b | 1.94 | 0.10 | |||
| Effect size c | 1.41 | 0.15 | |||
| Intention to assist in oral care behaviors (11–55) | |||||
| Group (EG) × Time (second) | 4.5 ± 5.1 | −1.3 ± 3.2 | 1.37 | 5.79 | (2.07, 9.51) |
| Group (EG) × Time (third) | 6.2 ± 4.1 | −0.2 ± 5.1 | 1.35 | 6.35 | (2.63, 10.07) |
| Group (EG) × Time (fourth) | 5.1 ± 5.2 | 0.7 ± 4.8 | 0.89 | 4.42 | (0.70, 8.15) |
| Effect size a | 0.88 | 0.41 | |||
| Effect size b | 1.51 | 0.04 | |||
| Effect size c | 0.98 | 0.15 |
| EG (n = 11) | CG (n = 12) | Effect Size d | β | (95% CI) | ||
|---|---|---|---|---|---|---|
| Diff ± SD † | Diff ± SD † | |||||
| Mouth cleaning (I will take the initiative to…) | ||||||
| remind elderly people with disabilities to perform oral care after each meal | ||||||
| Group (EG) × Time (second) | 0.3 ± 0.6 | - | - | 0.61 | 0.27 | (−0.13, 0.68) |
| Group (EG) × Time (third) | 0.4 ± 0.5 | 0.2 ± 0.4 | 0.44 | 0.20 | (−0.21, 0.60) | |
| Group (EG) × Time (fourth) | 0.3 ± 0.5 | 0.3 ± 0.6 | 0.04 | 0.02 | (−0.38, 0.43) | |
| Effect size a | 0.50 | - | ||||
| Effect size b | 0.80 | 0.50 | ||||
| Effect size c | 0.60 | 0.50 | ||||
| remind elderly people with disabilities to clean their mouths before bedtime | ||||||
| Group (EG) × Time (second) | 0.2 ± 0.6 | - | - | 0.44 | 0.18 | (−0.20, 0.56) |
| Group (EG) × Time (third) | 0.4 ± 0.5 | 0.2 ± 0.4 | 0.44 | 0.20 | (−0.19, 0.58) | |
| Group (EG) × Time (fourth) | 0.3 ± 0.5 | 0.3 ± 0.7 | 0.11 | −0.06 | (−0.44, 0.32) | |
| Effect size a | 0.33 | - | ||||
| Effect size b | 0.80 | 0.50 | ||||
| Effect size c | 0.60 | 0.43 | ||||
| assist elderly people with disabilities in cleaning their dentures | ||||||
| Group (EG) × Time (second) | 0.5 ± 0.7 | 0.2 ± 0.4 | 0.69 | 0.38 | (−0.09, 0.85) | |
| Group (EG) × Time (third) | 0.5 ± 0.5 | 0.3 ± 0.5 | 0.61 | 0.30 | (−0.18, 0.77) | |
| Group (EG) × Time (fourth) | 0.5 ± 0.8 | 0.4 ± 0.8 | 0.16 | 0.13 | (−0.34, 0.60) | |
| Effect size a | 0.71 | 0.50 | ||||
| Effect size b | 1.00 | 0.60 | ||||
| Effect size c | 0.63 | 0.50 | ||||
| assist elderly people with disabilities in using the Bass brushing technique to brush their teeth | ||||||
| Group (EG) × Time (second) | 0.5 ± 0.7 | −0.2 ± 0.6 | 1.27 | 0.71 | (0.19, 1.24) | |
| Group (EG) × Time (third) | 0.5 ± 0.9 | −0.1 ± 0.7 | 0.78 | 0.63 | (0.11, 1.15) | |
| Group (EG) × Time (fourth) | 0.5 ± 0.8 | 0.1 ± 0.7 | 0.62 | 0.46 | (−0.06, 0.99) | |
| Effect size a | 0.71 | 0.33 | ||||
| Effect size b | 0.56 | 0.14 | ||||
| Effect size c | 0.63 | 0.14 | ||||
| assist elderly people with disabilities in using the interdental brush | ||||||
| Group (EG) × Time (second) | 0.7 ± 0.6 | 0.0 ± 0.4 | 1.34 | 0.73 | (0.26, 1.19) | |
| Group (EG) × Time (third) | 0.7 ± 0.8 | 0.0 ± 0.6 | 1.04 | 0.73 | (0.26, 1.19) | |
| Group (EG) × Time (fourth) | 0.9 ± 0.5 | 0.0 ± 0.7 | 1.40 | 0.91 | (0.44, 1.37) | |
| Effect size a | 1.17 | 0.00 | ||||
| Effect size b | 0.88 | 0.00 | ||||
| Effect size c | 1.80 | 0.00 | ||||
| assist elderly people with disabilities with soft tissue cleaning | ||||||
| Group (EG) × Time (second) | 0.4 ± 0.5 | −0.1 ± 0.5 | 0.88 | 0.45 | (0.00, 0.89) | |
| Group (EG) × Time (third) | 0.5 ± 0.7 | −0.2 ± 0.7 | 1.01 | 0.71 | (0.27, 1.16) | |
| Group (EG) × Time (fourth) | 0.4 ± 0.8 | −0.2 ± 0.6 | 0.76 | 0.53 | (0.08, 0.98) | |
| Effect size a | 0.80 | 0.20 | ||||
| Effect size b | 0.71 | 0.29 | ||||
| Effect size c | 0.50 | 0.33 | ||||
| To choose oral care tools | ||||||
| recommend proper tools for oral care to elderly people with disabilities | ||||||
| Group (EG) × Time (second) | 0.3 ± 0.6 | −0.2 ± 0.4 | 0.83 | 0.44 | (0.01, 0.87) | |
| Group (EG) × Time (third) | 0.4 ± 0.5 | −0.2 ± 0.6 | 0.96 | 0.53 | (0.10, 0.96) | |
| Group (EG) × Time (fourth) | 0.4 ± 0.7 | 0.0 ± 0.6 | 0.57 | 0.36 | (−0.06, 0.79) | |
| Effect size a | 0.50 | 0.50 | ||||
| Effect size b | 0.80 | 0.33 | ||||
| Effect size c | 0.57 | 0.00 | ||||
| Check the suitability of oral care tools for elderly people with disabilities | ||||||
| Group (EG) × Time (second) | 0.5 ± 0.7 | −0.3 ± 0.6 | 1.08 | 0.70 | (0.24, 1.17) | |
| Group (EG) × Time (third) | 0.6 ± 0.7 | 0.0 ±0.7 | 1.00 | 0.64 | (0.17, 1.10) | |
| Group (EG) × Time (fourth) | 0.3 ± 0.5 | 0.0 ± 0.6 | 0.50 | 0.27 | (−0.19, 0.73) | |
| Effect size a | 0.71 | 0.50 | ||||
| Effect size b | 1.20 | 0.00 | ||||
| Effect size c | 0.60 | 0.00 | ||||
| Dental visit | ||||||
| Remind elderly people with disabilities to have regular dental visits every 6 months | ||||||
| Group (EG) × Time (second) | 0.3 ± 0.5 | −0.3 ± 0.5 | 1.26 | 0.61 | (0.22, 0.99) | |
| Group (EG) × Time (third) | 0.5 ± 0.5 | −0.2 ± 0.6 | 1.13 | 0.62 | (0.23, 1.01) | |
| Group (EG) × Time (fourth) | 0.4 ± 0.5 | −0.3 ± 0.6 | 1.08 | 0.61 | (0.23, 1.00) | |
| Effect size a | 0.60 | 0.60 | ||||
| Effect size b | 1.00 | 0.33 | ||||
| Effect size c | 0.80 | 0.50 | ||||
| Implement safe position | ||||||
| Help elderly people with disabilities into a safe position before an oral care session is commenced | ||||||
| Group (EG) × Time (second) | 0.5 ± 0.5 | −0.2 ± 0.6 | 1.13 | 0.62 | (0.09, 1.15) | |
| Group (EG) × Time (third) | 0.6 ± 0.7 | 0.2 ± 0.9 | 0.57 | 0.47 | (−0.06, 1.00) | |
| Group (EG) × Time (fourth) | 0.5 ± 0.8 | 0.1 ± 0.7 | 0.62 | 0.46 | (−0.07, 0.99) | |
| Effect size a | 1.00 | 0.33 | ||||
| Effect size b | 0.86 | 0.22 | ||||
| Effect size c | 0.63 | 0.14 | ||||
| Implement oral desensitization | ||||||
| Assist elderly people with disabilities with oral desensitization before an oral care session is commenced | ||||||
| Group (EG) × Time (second) | 0.2 ± 0.6 | −0.3 ± 0.6 | 0.70 | 0.43 | (−0.09, 0.95) | |
| Group (EG) × Time (third) | 0.5 ± 0.7 | −1.2 ± 0.8 | 0.93 | 0.71 | (0.19, 1.23) | |
| Group (EG) × Time (fourth) | 0.4 ± 0.8 | −0.2 ± 0.7 | 0.70 | 0.53 | (0.01, 1.05) | |
| Effect size a | 0.33 | 0.50 | ||||
| Effect size b | 0.71 | 1.50 | ||||
| Effect size c | 0.50 | 0.29 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, A.-H.; Lin, P.-C.; Lin, P.-C.; Lin, Y.-C.; Kabasawa, Y.; Lin, C.-Y.; Huang, H.-L. Effectiveness of Virtual Reality-Based Training on Oral Healthcare for Disabled Elderly Persons: A Randomized Controlled Trial. J. Pers. Med. 2022, 12, 218. https://doi.org/10.3390/jpm12020218
Chang A-H, Lin P-C, Lin P-C, Lin Y-C, Kabasawa Y, Lin C-Y, Huang H-L. Effectiveness of Virtual Reality-Based Training on Oral Healthcare for Disabled Elderly Persons: A Randomized Controlled Trial. Journal of Personalized Medicine. 2022; 12(2):218. https://doi.org/10.3390/jpm12020218
Chicago/Turabian StyleChang, Ai-Hua, Pei-Chen Lin, Pei-Chao Lin, Yi-Ching Lin, Yuji Kabasawa, Cheng-Yu Lin, and Hsiao-Ling Huang. 2022. "Effectiveness of Virtual Reality-Based Training on Oral Healthcare for Disabled Elderly Persons: A Randomized Controlled Trial" Journal of Personalized Medicine 12, no. 2: 218. https://doi.org/10.3390/jpm12020218