
Clinical Disease Severity Mediates the Relationship between Stride Length and Speed and the Risk of Falling in Parkinson’s Disease

 ,
, 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design and Patient Selection
2.2. Severity and Subtypes of PD
2.3. Severity and Frequency and Situations of Falling
2.4. Assessment of Gait Analysis
2.5. Assessment of the Functional Mobility
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of Patients with PD
3.2. Baseline Spatiotemporal and Kinematic Variables
3.3. Effect of Dopamine Replacement Therapy on Spatiotemporal and Kinematic Variables
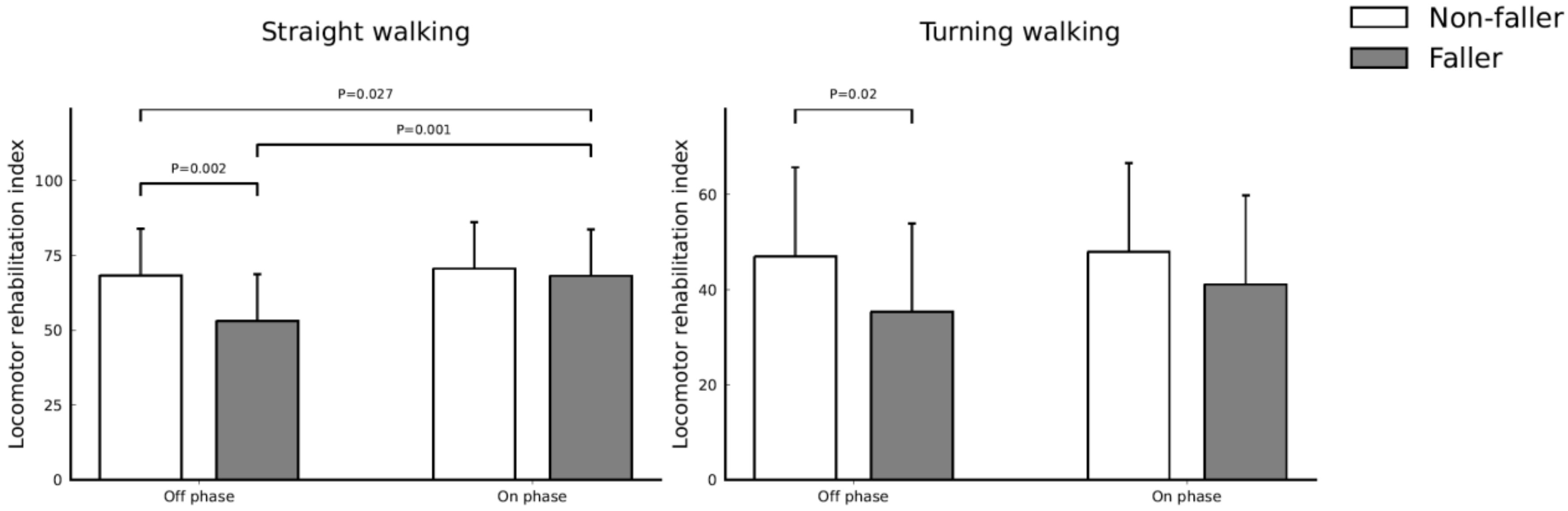
3.4. Effect of Dopamine Replacement Therapy on Functional Mobility
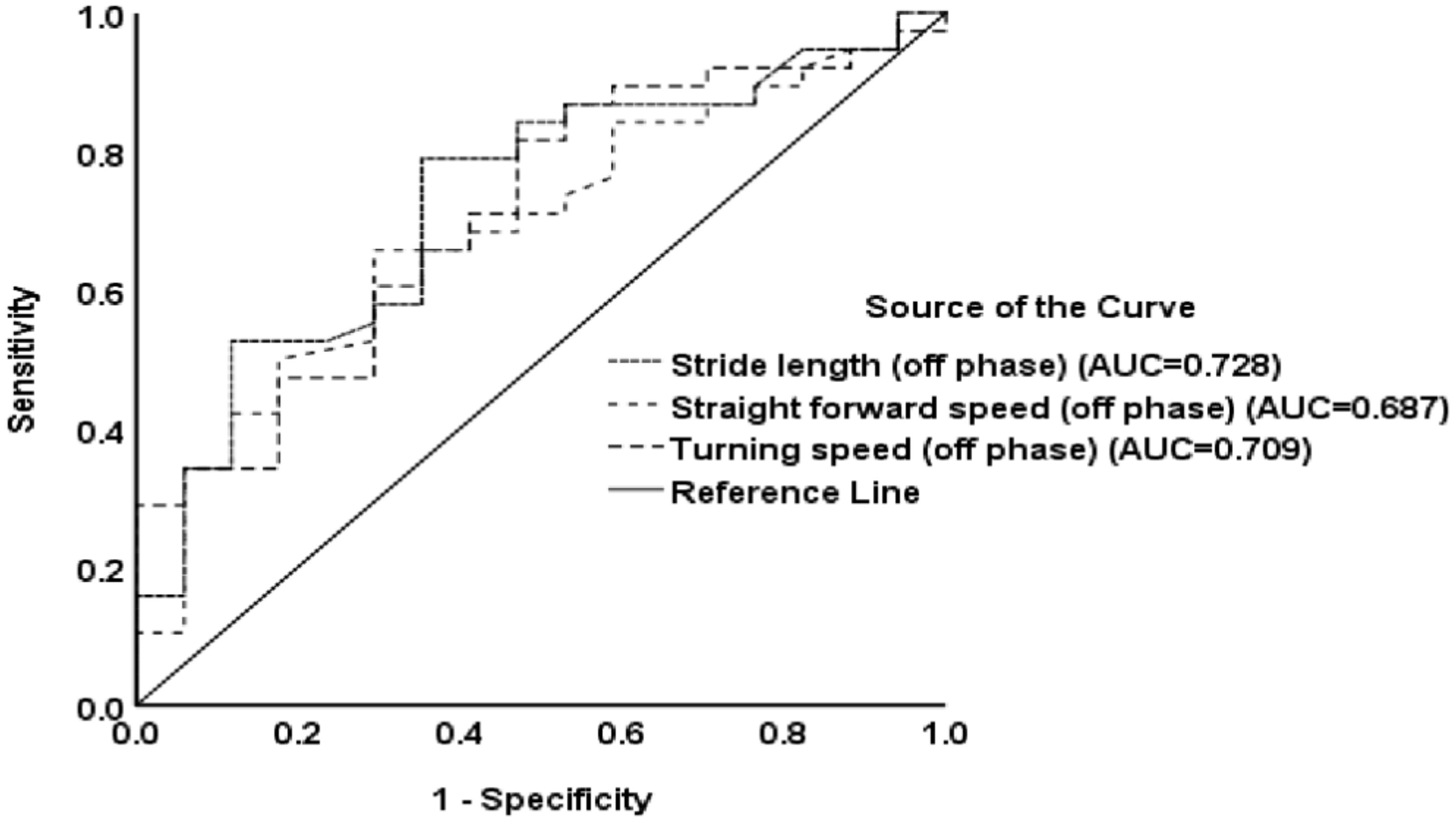
3.5. Correlation Analyses of Spatiotemporal and Kinematic Parameters, as well as Baseline Characteristics on the Three-Step Fall Prediction Model Score
3.6. Clinical Factors Significantly Associated with the Three-Step Fall Prediction Model Score
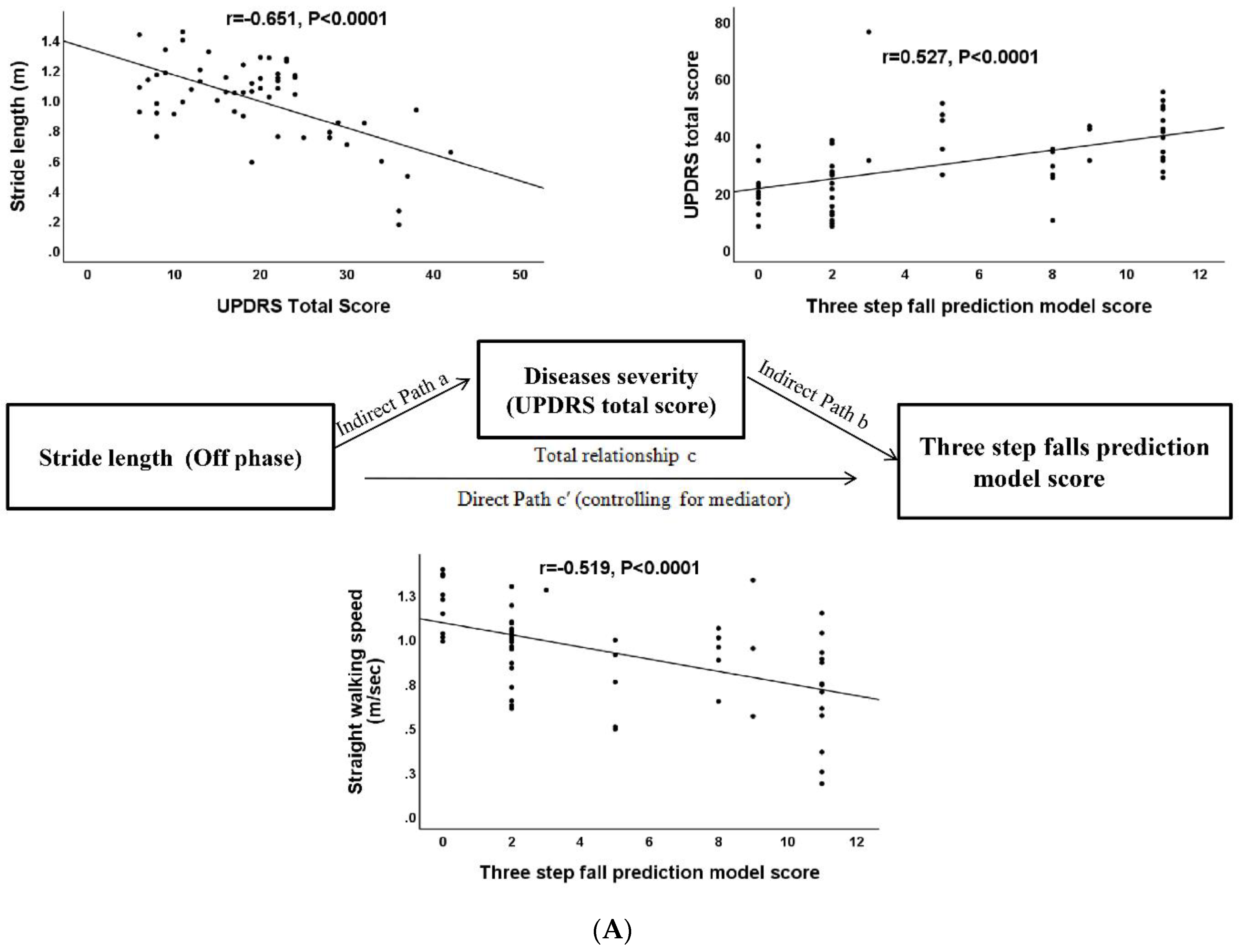
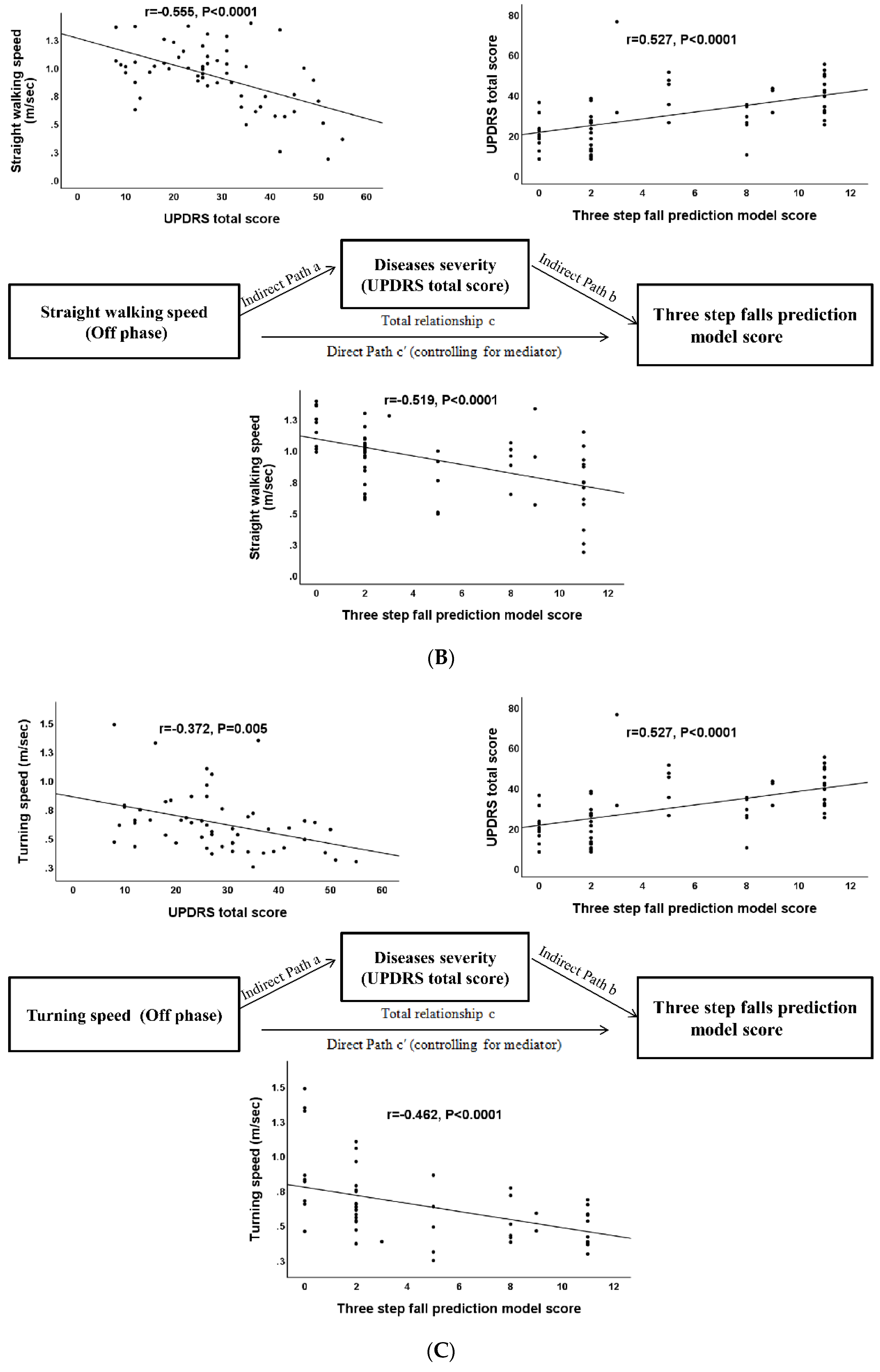
3.7. Mediation Analysis for the Severity of Spatiotemporal Parameters, Clinical Disease Severity, and Risk of Falling
4. Discussion
4.1. Major Findings of Our Study
4.2. Spatiotemporal and Kinematic Parameters Associated with Risk of Falling
4.3. The Effects of Dopamine Replacement Therapy on the Walking Gait Cycle
4.4. Three Candidate Variables in the Mediation Analysis Model
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fasano, A.; Canning, C.G.; Hausdorff, J.M.; Lord, S.; Rochester, L. Falls in Parkinson’s disease: A complex and evolving picture. Mov. Disord. 2017, 32, 1524–1536. [Google Scholar] [CrossRef] [PubMed]
- Voss, T.S.; Elm, J.J.; Wielinski, C.L.; Aminoff, M.J.; Bandyopadhyay, D.; Chou, K.L.; Sudarsky, L.R.; Tilley, B.C. Fall frequency and risk assessment in early Parkinson’s disease. Parkinsonism Relat. Disord. 2012, 18, 837–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farombi, T.H.; Owolabi, M.O.; Ogunniyi, A. Falls and Their Associated Risks in Parkinson’s Disease Patients in Nigeria. J. Mov. Disord. 2016, 9, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Youn, J.; Okuma, Y.; Hwang, M.; Kim, D.; Cho, J.W. Falling Direction can Predict the Mechanism of Recurrent Falls in Advanced Parkinson’s Disease. Sci. Rep. 2017, 7, 3921. [Google Scholar] [CrossRef] [PubMed]
- Pelicioni, P.H.S.; Menant, J.C.; Latt, M.D.; Lord, S.R. Falls in Parkinson’s Disease Subtypes: Risk Factors, Locations and Circumstances. Int. J. Environ. Res. Public Health 2019, 16, 2216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matinolli, M.; Korpelainen, J.T.; Korpelainen, R.; Sotaniemi, K.A.; Virranniemi, M.; Myllyla, V.V. Postural sway and falls in Parkinson’s disease: A regression approach. Mov. Disord. 2007, 22, 1927–1935. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.; Alcock, L.; Yarnall, A.J.; Lord, S.; Lawson, R.A.; Morris, R.; Taylor, J.P.; Burn, D.J.; Rochester, L.; Galna, B. Gait Progression Over 6 Years in Parkinson’s Disease: Effects of Age, Medication, and Pathology. Front. Aging Neurosci. 2020, 12, 577435. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Williams, T.F.; Mayewski, R. Fall risk index for elderly patients based on number of chronic disabilities. Am. J. Med. 1986, 80, 429–434. [Google Scholar] [CrossRef]
- Leddy, A.L.; Crowner, B.E.; Earhart, G.M. Functional gait assessment and balance evaluation system test: Reliability, validity, sensitivity, and specificity for identifying individuals with Parkinson disease who fall. Phys. Ther. 2011, 91, 102–113. [Google Scholar] [CrossRef] [Green Version]
- Lindholm, B.; Nilsson, M.H.; Hansson, O.; Hagell, P. External validation of a 3-step falls prediction model in mild Parkinson’s disease. J. Neurol. 2016, 263, 2462–2469. [Google Scholar] [CrossRef] [Green Version]
- Pan, D.; Dhall, R.; Lieberman, A.; Petitti, D.B. A mobile cloud-based Parkinson’s disease assessment system for home-based monitoring. JMIR Mhealth Uhealth 2015, 3, e29. [Google Scholar] [CrossRef] [PubMed]
- Hubble, R.P.; Naughton, G.A.; Silburn, P.A.; Cole, M.H. Wearable sensor use for assessing standing balance and walking stability in people with Parkinson’s disease: A systematic review. PLoS ONE 2015, 10, e0123705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plotnik, M.; Giladi, N.; Dagan, Y.; Hausdorff, J.M. Postural instability and fall risk in Parkinson’s disease: Impaired dual tasking, pacing, and bilateral coordination of gait during the “ON” medication state. Exp. Brain Res. 2011, 210, 529–538. [Google Scholar] [CrossRef] [PubMed]
- Toosizadeh, N.; Mohler, J.; Lei, H.; Parvaneh, S.; Sherman, S.; Najafi, B. Motor Performance Assessment in Parkinson’s Disease: Association between Objective In-Clinic, Objective In-Home, and Subjective/Semi-Objective Measures. PLoS ONE 2015, 10, e0124763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cole, M.H.; Naughton, G.A.; Silburn, P.A. Neuromuscular Impairments Are Associated With Impaired Head and Trunk Stability During Gait in Parkinson Fallers. Neurorehabil. Neural Repair 2017, 31, 34–47. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.H.; Silburn, P.A.; Wood, J.M.; Worringham, C.J.; Kerr, G.K. Falls in Parkinson’s disease: Kinematic evidence for impaired head and trunk control. Mov. Disord. 2010, 25, 2369–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lord, S.; Galna, B.; Yarnall, A.J.; Coleman, S.; Burn, D.; Rochester, L. Predicting first fall in newly diagnosed Parkinson’s disease: Insights from a fall-naive cohort. Mov. Disord. 2016, 31, 1829–1836. [Google Scholar] [CrossRef] [PubMed]
- Curtze, C.; Nutt, J.G.; Carlson-Kuhta, P.; Mancini, M.; Horak, F.B. Levodopa Is a Double-Edged Sword for Balance and Gait in People With Parkinson’s Disease. Mov. Disord. 2015, 30, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Martin, P.; Gil-Nagel, A.; Gracia, L.M.; Gomez, J.B.; Martinez-Sarries, J.; Bermejo, F. Unified Parkinson’s Disease Rating Scale characteristics and structure. The Cooperative Multicentric Group. Mov. Disord. 1994, 9, 76–83. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J.; McDermott, M.; Carter, J.; Gauthier, S.; Goetz, C.; Golbe, L.; Huber, S.; Koller, W.; Olanow, C.; Shoulson, I.; et al. Variable expression of Parkinson’s disease: A base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology 1990, 40, 1529–1534. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Li, T.N.; Yuan, Y.S.; Jiang, S.M.; Tong, Q.; Wang, M.; Wang, J.W.; Chen, H.J.; Ding, J.; Xu, Q.R.; et al. The Neural Basis of Postural Instability Gait Disorder Subtype of Parkinson’s Disease: A PET and fMRI Study. CNS Neurosci. Ther. 2016, 22, 360–367. [Google Scholar] [CrossRef] [Green Version]
- Nieuwboer, A.; Rochester, L.; Herman, T.; Vandenberghe, W.; Emil, G.E.; Thomaes, T.; Giladi, N. Reliability of the new freezing of gait questionnaire: Agreement between patients with Parkinson’s disease and their carers. Gait Posture 2009, 30, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.T.; Chang, C.C.; Chang, W.N.; Tsai, N.W.; Huang, C.C.; Chang, Y.T.; Wang, H.C.; Kung, C.T.; Su, Y.J.; Lin, W.C.; et al. Neuropsychiatric symptoms in Alzheimer’s disease: Associations with caregiver burden and treatment outcomes. QJM 2017, 110, 565–570. [Google Scholar] [CrossRef]
- Luukinen, H.; Koski, K.; Hiltunen, L.; Kivela, S.L. Incidence rate of falls in an aged population in northern Finland. J. Clin. Epidemiol. 1994, 47, 843–850. [Google Scholar] [CrossRef]
- Eltoukhy, M.; Kuenze, C.; Oh, J.; Jacopetti, M.; Wooten, S.; Signorile, J. Microsoft Kinect can distinguish differences in over-ground gait between older persons with and without Parkinson’s disease. Med. Eng. Phys. 2017, 44, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Latorre, J.; Colomer, C.; Alcaniz, M.; Llorens, R. Gait analysis with the Kinect v2: Normative study with healthy individuals and comprehensive study of its sensitivity, validity, and reliability in individuals with stroke. J. Neuroeng. Rehabil. 2019, 16, 97. [Google Scholar] [CrossRef] [Green Version]
- Leurs, F.; Ivanenko, Y.P.; Bengoetxea, A.; Cebolla, A.M.; Dan, B.; Lacquaniti, F.; Cheron, G.A. Optimal walking speed following changes in limb geometry. J. Exp. Biol. 2011, 214, 2276–2282. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, E.P.; Franzoni, L.T.; Cubillos, D.M.; de Oliveira Fagundes, A.; Carvalho, A.R.; Oliveira, H.B.; Pantoja, P.D.; Schuch, F.B.; Rieder, C.R.; Martinez, F.G.; et al. Effects of Nordic walking training on functional parameters in Parkinson’s disease: A randomized controlled clinical trial. Scand. J. Med. Sci. Sports 2017, 27, 351–358. [Google Scholar] [CrossRef]
- Wager, T.D.; Davidson, M.L.; Hughes, B.L.; Lindquist, M.A.; Ochsner, K.N. Prefrontal-subcortical pathways mediating successful emotion regulation. Neuron 2008, 59, 1037–1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, M.E.; Iansek, R.; Matyas, T.A.; Summers, J.J. Stride length regulation in Parkinson’s disease. Normalization strategies and underlying mechanisms. Brain 1996, 119, 551–568. [Google Scholar] [CrossRef] [PubMed]
- Zanardi, A.P.J.; da Silva, E.S.; Costa, R.R.; Passos-Monteiro, E.; Dos Santos, I.O.; Kruel, L.F.M.; Peyre-Tartaruga, L.A. Gait parameters of Parkinson’s disease compared with healthy controls: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 752. [Google Scholar] [CrossRef] [PubMed]
- Smulders, K.; Dale, M.L.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B. Pharmacological treatment in Parkinson’s disease: Effects on gait. Parkinsonism Relat. Disord. 2016, 31, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baudendistel, S.T.; Schmitt, A.C.; Roemmich, R.T.; Harrison, I.L.; Hass, C.J. Levodopa facilitates improvements in gait kinetics at the hip, not the ankle, in individuals with Parkinson’s disease. J. Biomech. 2021, 121, 110366. [Google Scholar] [CrossRef] [PubMed]
- Rocchi, L.; Chiari, L.; Horak, F.B. Effects of deep brain stimulation and levodopa on postural sway in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 73, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Bekkers, E.M.J.; Dijkstra, B.W.; Heremans, E.; Verschueren, S.M.P.; Bloem, B.R.; Nieuwboer, A. Balancing between the two: Are freezing of gait and postural instability in Parkinson’s disease connected? Neurosci. Biobehav. Rev. 2018, 94, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Liu, J.; Tan, Y.; Chen, S. Freezing of gait in Parkinson’s disease: Pathophysiology, risk factors and treatments. Transl. Neurodegener. 2020, 9, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloem, B.R.; Marinus, J.; Almeida, Q.; Dibble, L.; Nieuwboer, A.; Post, B.; Ruzicka, E.; Goetz, C.; Stebbins, G.; Martinez-Martin, P.; et al. Measurement instruments to assess posture, gait, and balance in Parkinson’s disease: Critique and recommendations. Mov. Disord. 2016, 31, 1342–1355. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Schlueter, H.; El-Gohary, M.; Mattek, N.; Duncan, C.; Kaye, J.; Horak, F.B. Continuous Monitoring of Turning Mobility and Its Association to Falls and Cognitive Function: A Pilot Study. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1102–1108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nantel, J.; McDonald, J.C.; Bronte-Stewart, H. Effect of medication and STN-DBS on postural control in subjects with Parkinson’s disease. Parkinsonism Relat. Disord. 2012, 18, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Burn, D.J. The effects of deep brain stimulation and levodopa on postural sway in subjects with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2002, 73, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Fallers (n = 39) | Fallers (n = 22) | p-Value | |
|---|---|---|---|
| Age, years | 67.9 ± 8.6 | 66.3 ± 8.9 | 0.48 |
| Sex (men/women) | 21/18 | 8/14 | 0.19 |
| Height (m) | 1.60 ± 0.08 | 1.57 ± 0.08 | 0.14 |
| Body mass (kg) | 64.8 ± 10.1 | 61.5 ± 12.6 | 0.26 |
| Body mass index (kg/m2) | 25.4 ± 3.8 | 25.1 ± 5.3 | 0.79 |
| Waist circumference (cm) | 89.4 ± 9.3 | 87.8 ± 11.3 | 0.56 |
| Disease duration, years | 4.7 ± 3.7 | 8.9 ± 5.3 | 0.001 * |
| Total LED (mg) | 612.9 ± 348.5 | 1312.3 ± 745.4 | <0.0001 ** |
| UPDRS total score α (off phase) | 25.3 ± 13.7 | 37.2 ± 10.5 | 0.001 * |
| UPDRS I β (off phase) | 1.2 ± 1.1 | 2.1 ± 1.5 | 0.008 * |
| UPDRS II γ (off phase) | 7.8 ± 4.6 | 14.5 ± 4.8 | <0.0001 ** |
| UPDRS III δ (off phase) | 16.3 ± 10.0 | 20.3 ± 7.2 | 0.11 |
| UPDRS-derived PIGD score (off phase) Ω | 2.8 ± 2.3 | 7.6 ± 3.6 | <0.0001 ** |
| Hoehn and Yahr stages | 1.7 ± 0.8 | 2.5 ± 1.0 | 0.001 * |
| Freezing of gait | 8 | 15 | <0.0001 ** |
| Dyskinesia | 3 | 7 | 0.02 * |
| Motor fluctuation | 4 | 9 | 0.004 * |
| “Off” dystonia | 4 | 5 | 0.23 |
| Cognitive Abilities Screening Instrument | 82.2 ± 16.0 | 82.1 ± 13.9 | 0.99 |
| Underlying diseases | |||
| Hypertension | 15 | 6 | 0.38 |
| Hyperlipidemia | 27 | 9 | 0.03 |
| Coronary artery diseases | 4 | 4 | 0.44 |
| Falling severity Ф | |||
| Mild | 0 | 6 | |
| Moderate | 0 | 12 | |
| Severe | 0 | 0 |
| Non-Fallers (n = 39) | Fallers (n = 22) | p-Value | |
|---|---|---|---|
| Spatiotemporal parameters (off phase) | |||
| Straight forward | |||
| Cadence (steps/s) | 1.84 ± 0.17 | 1.85 ± 0.22 | 0.78 |
| Speed (m/s) | 1.0 ± 0.23 | 0.77 ± 0.29 | 0.002 * |
| Stride length (m) | 1.08 ± 0.21 | 0.82 ± 0.28 | <0.0001 ** |
| Step length (m) | 0.54 ± 0.10 | 0.41 ± 0.14 | <0.0001 ** |
| Step length variability (CV) | 14.76 ± 5.0.2 | 21.08 ± 13.12 | 0.05 |
| Stride Time (s) | 1.09 ± 0.10 | 1.10 ± 0.15 | 0.72 |
| Step Time (s) | 0.55 ± 0.04 | 0.55 ± 0.08 | 0.91 |
| Step Time variability (CV) | 11.58 ± 3.76 | 18.76 ± 13.04 | 0.002 * |
| Turning | |||
| Turning time (s) | 2.45 ± 0.98 | 3.19 ± 1.59 | 0.09 |
| Turning speed (m/s) | 0.69 ± 0.28 | 0.51 ± 0.14 | 0.002 * |
| Turning step length (m) | 0.42 ± 0.08 | 0.38 ± 0.07 | 0.09 |
| Low extremities kinematics (off phase) | |||
| Total hip ROM (°) | 53.83 ± 9.28 | 48.53 ± 11.60 | 0.06 |
| Total Knee ROM (°) | 67.61 ± 6.55 | 65.08 ± 10.06 | 0.25 |
| Spatiotemporal parameters (on phase) | |||
| Straight forward | |||
| Cadence (steps/s) | 1.83 ± 0.18 | 1.93 ± 0.22 | 0.07 |
| Speed (m/s) | 1.03 ± 0.20 | 0.98 ± 0.21 | 0.40 |
| Stride length (m) | 1.11 ± 0.16 | 1.02 ± 0.17 | 0.03 * |
| Step length (m) | 0.56 ± 0.08 | 0.51 ± 0.09 | 0.03 * |
| Step length variability (CV) | 14.11 ± 4.78 | 15.03 ± 5.23 | 0.49 |
| Stride Time (s) | 1.10 ± 0.11 | 1.05 ± 0.14 | 0.15 |
| Step Time (s) | 0.55 ± 0.06 | 0.53 ± 0.07 | 0.14 |
| Step Time variability (CV) | 12.33 ± 3.49 | 13.61 ± 5.49 | 0.27 |
| Turning | |||
| Turning time (s) | 2.24 ± 0.63 | 2.65 ± 1.22 | 0.15 |
| Turning speed (m/s) | 0.70 ± 0.23 | 0.59 ± 0.28 | 0.12 |
| Turning step length (m) | 0.44 ± 0.07 | 0.42 ± 0.12 | 0.44 |
| Low extremities kinematics (on phase) | |||
| Total hip ROM (°) | 55.64 ± 7.53 | 56.02 ± 8.63 | 0.86 |
| Total Knee ROM (°) | 68.38 ± 6.09 | 67.67 ± 6.68 | 0.67 |
| Off Phase | On Phase | p-Value | Normal Reference ф | |
|---|---|---|---|---|
| Spatiotemporal parameters | ||||
| Straight forward | ||||
| Cadence (steps/s) | 1.83 ± 0.19 | 1.85 ± 0.20 | 0.49 | 1.82 ± 0.16 |
| speed (m/s) | 0.91 ± 0.28 | 1.0 ± 0.20 | 0.004 ** | 1.33 ± 0.32 |
| Stride length (m) | 0.99 ± 0.27 | 1.08 ± 0.18 | <0.0001 ** | 1.17 ± 0.24 |
| Step length (m) | 0.50 ± 0.13 | 0.54 ± 0.09 | 0.001 ** | 0.58 ± 0.12 |
| Step length variability (CV) | 17.25 ± 9.35 | 14.44 ± 5.13 | 0.01 * | 14.03 ± 14.56 |
| Stride time (s) | 1.10 ± 0.12 | 1.09 ± 0.13 | 0.85 | 0.90 ± 0.18 |
| Step time (s) | 0.55 ± 0.06 | 0.55 ± 0.06 | 0.55 | 0.47 ± 0.32 |
| Step time variability (CV) | 14.25 ± 9.1 | 13.05 ± 4.44 | 0.30 | 11.88 ± 8.69 |
| Turning | ||||
| Turning time (s) | 2.71 ± 1.27 | 2.27 ± 0.63 | 0.01 * | 1.77 ± 0.40 |
| Turning speed (m/s) | 0.62 ± 0.25 | 0.66 ± 0.26 | 0.37 | 0.79 ± 0.09 |
| Turning step length (m) | 0.41 ± 0.08 | 0.43 ± 0.10 | 0.11 | 0.52 ± 0.04 |
| Low extremities kinematics | ||||
| Total hip ROM (°) | 52.17 ± 10.55 | 55.70 ± 8.29 | <0.0001 ** | 66.52 ± 6.65 |
| Total Knee ROM (°) | 66.74 ± 7.94 | 68.15 ± 6.27 | 0.08 | 70.97 ± 3.31 |
| Non-Fallers (n = 39) | Fallers (n = 22) β, γ | |||
|---|---|---|---|---|
| Off Phase α | On Phase | Off Phase α | On Phase | |
| Optimal walking speed (m/s) | 1.45 ± 0.03 | 1.44 ± 0.0.3 | ||
| LRI (%) during straight walking | 68.42 ± 15.63 # | 70.68 ± 13.15 | 53.19 ± 20.03 | 68.27 ± 14.25 § |
| LRI (%) during turning walking | 47.03 ± 18.67 # | 47.97 ± 15.91 | 35.34 ± 10.57 | 41.13 ± 19.31 |
| Variables | Three-Step Fall Prediction Model Score | UPDRS Total Score | ||
|---|---|---|---|---|
| r | p-Value | r | p-Value | |
| Baseline characteristics | ||||
| Age, years | −0.094 | 0.474 | −0.047 | 0.724 |
| Disease duration, years | 0.520 | <0.0001 ** | 0.441 | <0.0001 ** |
| UPDRS total score | 0.527 | <0.0001 ** | --- | --- |
| Cognitive Abilities Screening Instrument | −0.125 | 0.425 | −0.241 | 0.107 |
| Levodopa equivalent dose | 0.519 | <0.0001 ** | 0.522 | <0.0001 ** |
| Spatiotemporal parameters (off phase) | ||||
| Cadence (steps/s) | 0.005 | 0.97 | −0.087 | 0.518 |
| Speed(m/s) | −0.519 | <0.0001 ** | −0.555 | <0.0001 ** |
| Stride length(m) | −0.583 | <0.0001 ** | −0.651 | <0.0001 ** |
| Step length(m) | −0.582 | <0.0001 ** | −0.601 | <0.0001 ** |
| Step length variability (CV) | 0.379 | 0.004 ** | 0.405 | 0.002 ** |
| Stride Time (s) | 0.089 | 0.51 | 0.133 | 0.321 |
| Step Time (s) | 0.047 | 0.731 | 0.152 | 0.156 |
| Step Time variability (CV) | 0.43 | 0.001 ** | 0.465 | <0.0001 ** |
| Double support time (s) | 0.26 | 0.051 | 0.361 | 0.005 |
| Single support time (s) | −0.043 | 0.748 | 0.153 | 0.252 |
| Swing phase (s) | −0.044 | 0.744 | 0.129 | 0.334 |
| Stance phase (s) | 0.123 | 0.363 | 0.182 | 0.171 |
| Turning time (s) | 0.394 | 0.003 ** | 0.501 | <0.0001 ** |
| Turning speed (m/s) | −0.462 | <0.0001 ** | −0.372 | 0.005 ** |
| Turning step length (m) | −0.352 | 0.0009 ** | −2.93 | 0.03 * |
| Low extremities kinematics (off phase) | ||||
| Total hip ROM (°) | −0.376 | 0.0004 ** | −0.512 | <0.0001 ** |
| Total Knee ROM (°) | −0.27 | 0.043 * | −0.460 | <0.0001 ** |
| Significant Univariable | Three-Step Fall Prediction Model Score | |
|---|---|---|
| Regression Coefficients | p-Value | |
| Constant | 6.58 | 0.056 |
| UPDRS total score | 0.14 | 0.003 * |
| Stride length (m) | −5.62 | 0.025 * |
| Mediation Analysis model Ω | Path Coefficient | Standard Error | p-Value | Sobel Test |
|---|---|---|---|---|
| Model 1: X = stride length | ||||
| Total effects, path c | −9.22 | 1.73 | <0.0001 | |
| Direct effects, path c′ | −5.26 | 2.02 | 0.012 | 0.018 |
| Indirect effect, path a | −28.38 | 5.08 | <0.0001 | |
| Indirect effect, path b | 0.16 | 0.04 | <0.0001 | |
| Model 2: X = Straight forward speed | ||||
| Total effects, path c | −7.81 | 1.74 | <0.0001 | |
| Direct effects, path c′ | −3.90 | 1.87 | 0.04 | 0.003 |
| Indirect effect, path a | −24.33 | 5.09 | <0.0001 | |
| Indirect effect, path b | 0.16 | 0.035 | <0.0001 | |
| Model 3: X = Turning speed | ||||
| Total effects, path c | −7.32 | 1.95 | <0.0001 | |
| Direct effects, path c′ | −4.34 | 1.90 | 0.027 | 0.017 |
| Indirect effect, path a | −17.78 | 5.95 | 0.004 | |
| Indirect effect, path b | 0.16 | 0.035 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-R.; Lien, C.-Y.; Huang, C.-C.; Lin, W.-C.; Chen, Y.-S.; Yu, C.-C.; Cheng, B.-C.; Kung, C.-T.; Kung, C.-F.; Chiang, Y.-F.; et al. Clinical Disease Severity Mediates the Relationship between Stride Length and Speed and the Risk of Falling in Parkinson’s Disease. J. Pers. Med. 2022, 12, 192. https://doi.org/10.3390/jpm12020192
Lai Y-R, Lien C-Y, Huang C-C, Lin W-C, Chen Y-S, Yu C-C, Cheng B-C, Kung C-T, Kung C-F, Chiang Y-F, et al. Clinical Disease Severity Mediates the Relationship between Stride Length and Speed and the Risk of Falling in Parkinson’s Disease. Journal of Personalized Medicine. 2022; 12(2):192. https://doi.org/10.3390/jpm12020192
Chicago/Turabian StyleLai, Yun-Ru, Chia-Yi Lien, Chih-Cheng Huang, Wei-Che Lin, Yueh-Sheng Chen, Chiun-Chieh Yu, Ben-Chung Cheng, Chia-Te Kung, Chien-Feng Kung, Yi-Fang Chiang, and et al. 2022. "Clinical Disease Severity Mediates the Relationship between Stride Length and Speed and the Risk of Falling in Parkinson’s Disease" Journal of Personalized Medicine 12, no. 2: 192. https://doi.org/10.3390/jpm12020192