
Devascularized Bone Surface Culture: A Novel Strategy for Identifying Osteomyelitis-Related Pathogens
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting, OM Diagnostic Criteria, and Inclusion and Exclusion Criteria
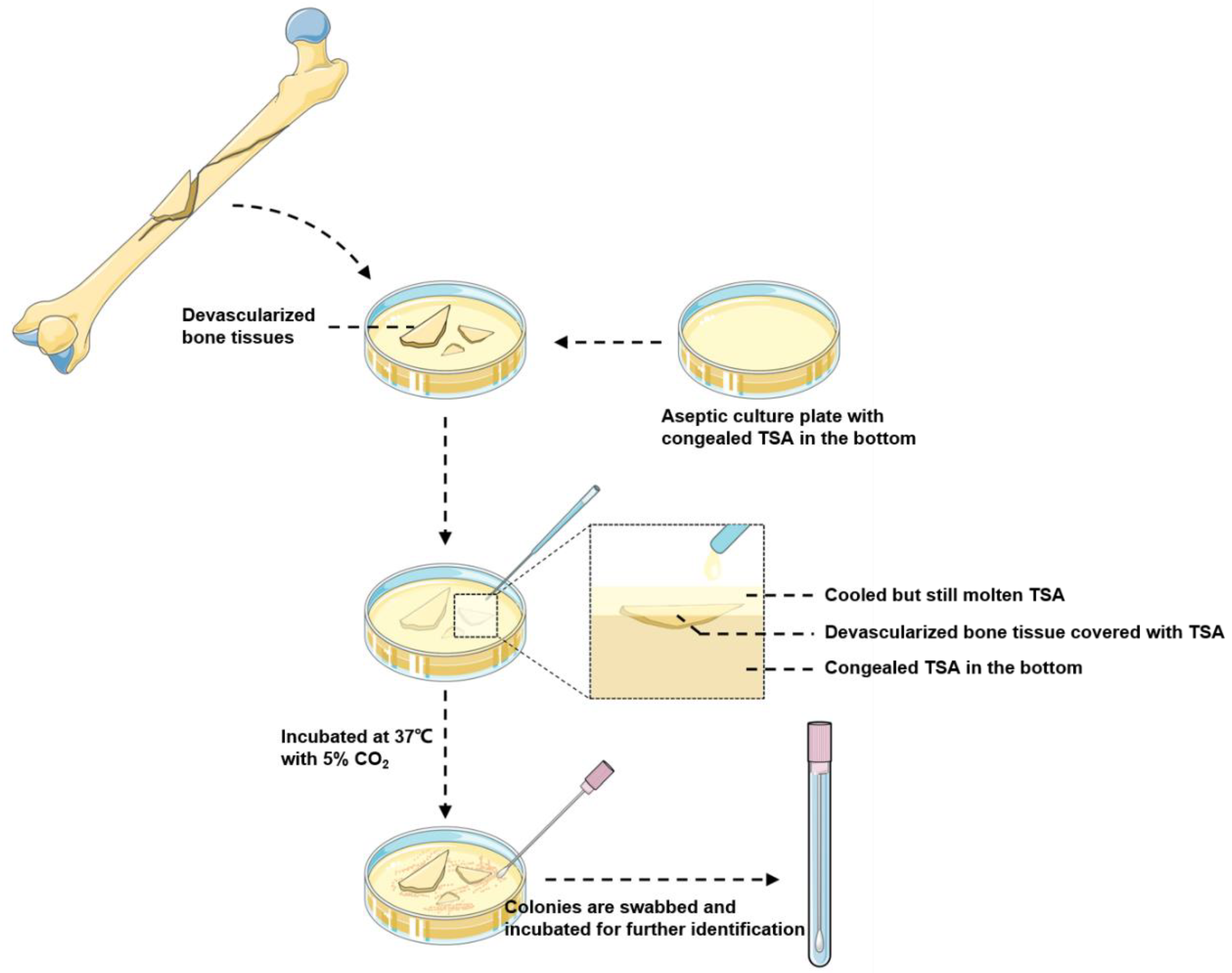
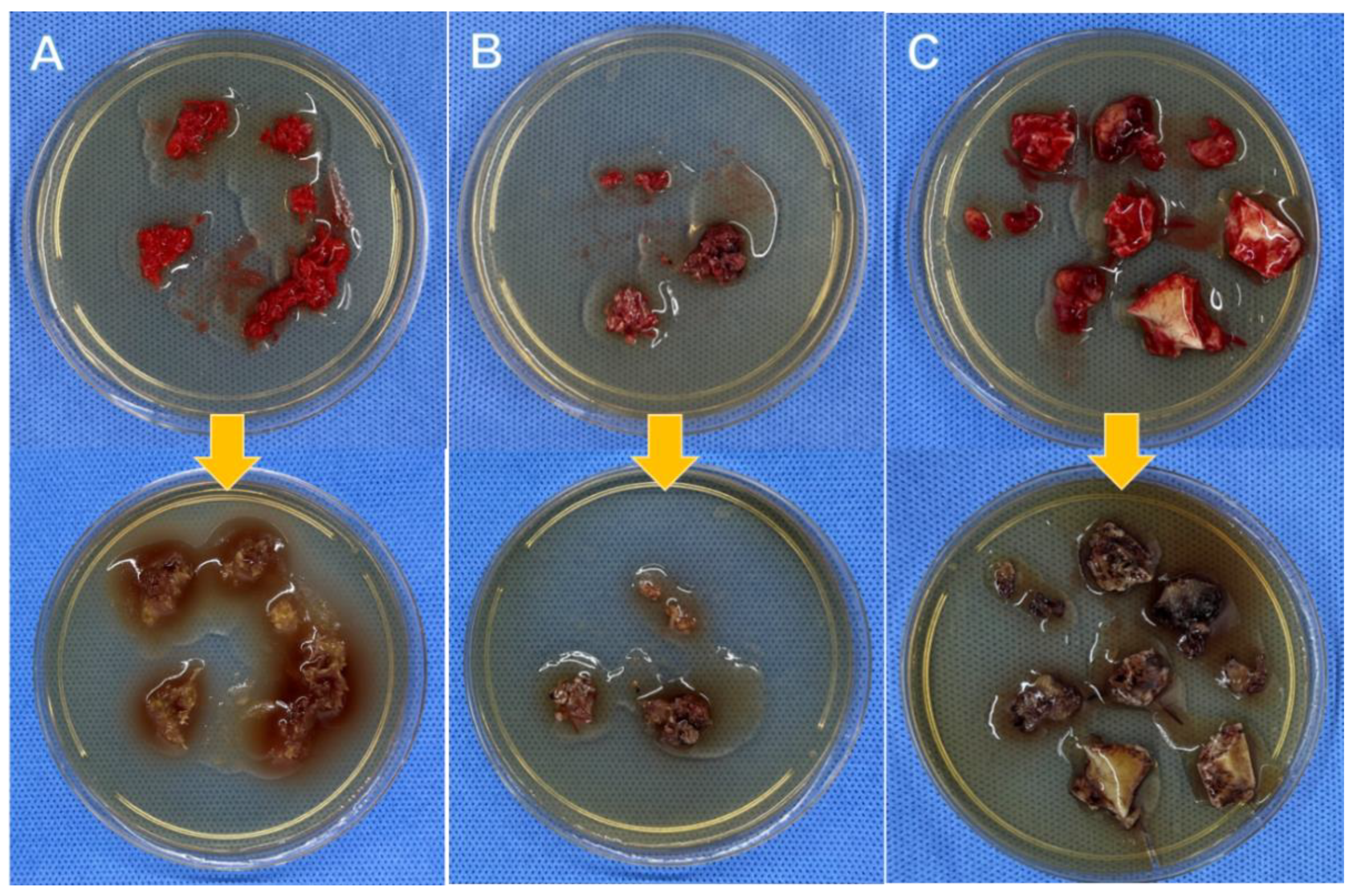
2.2. BSC and TSC Procedures
2.3. Statistical Analysis
3. Results
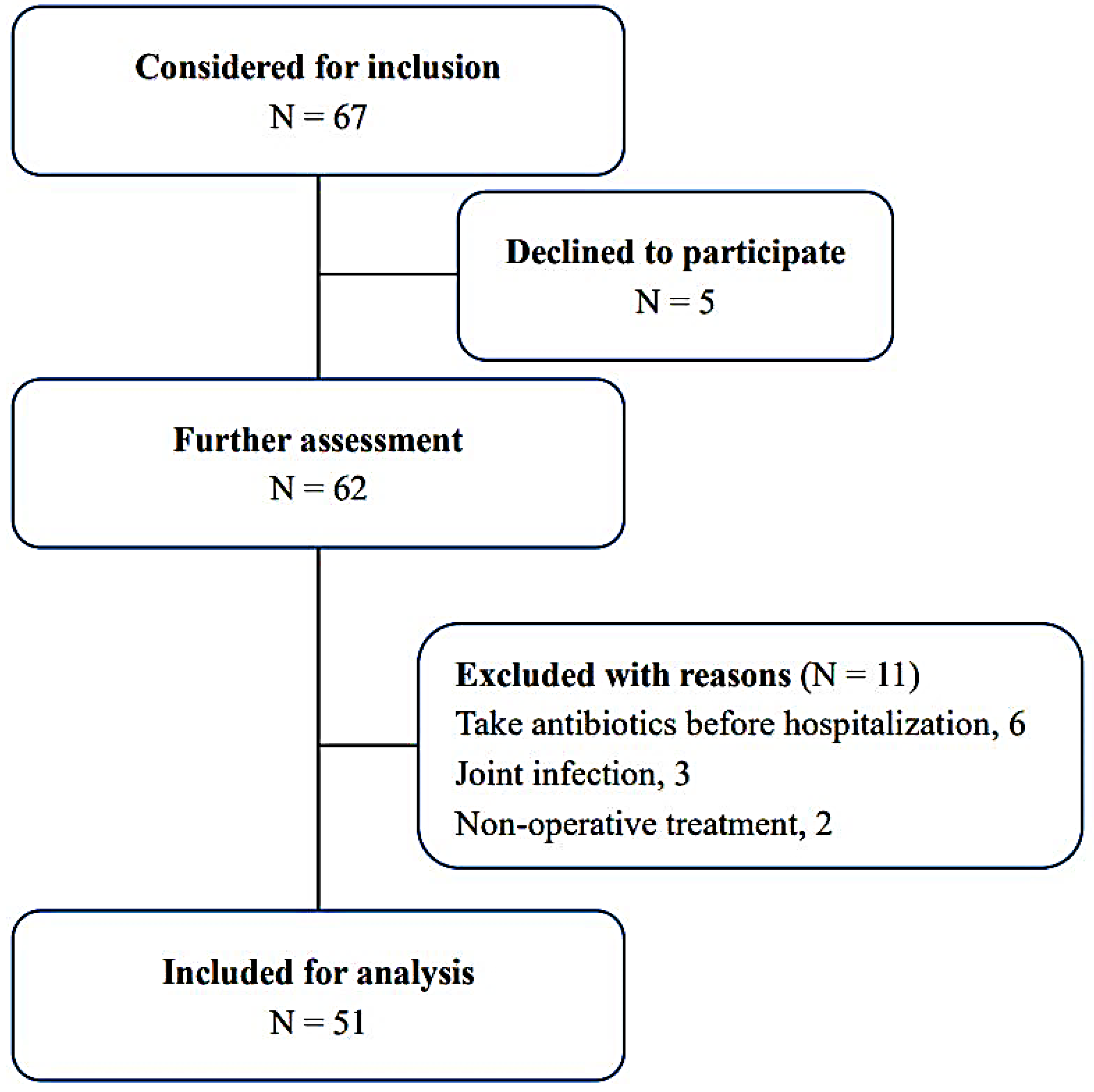
3.1. Participant Inclusion Flow Chart, Patient Demographics, OM Etiology, Body Side, and Infection Site Distributions
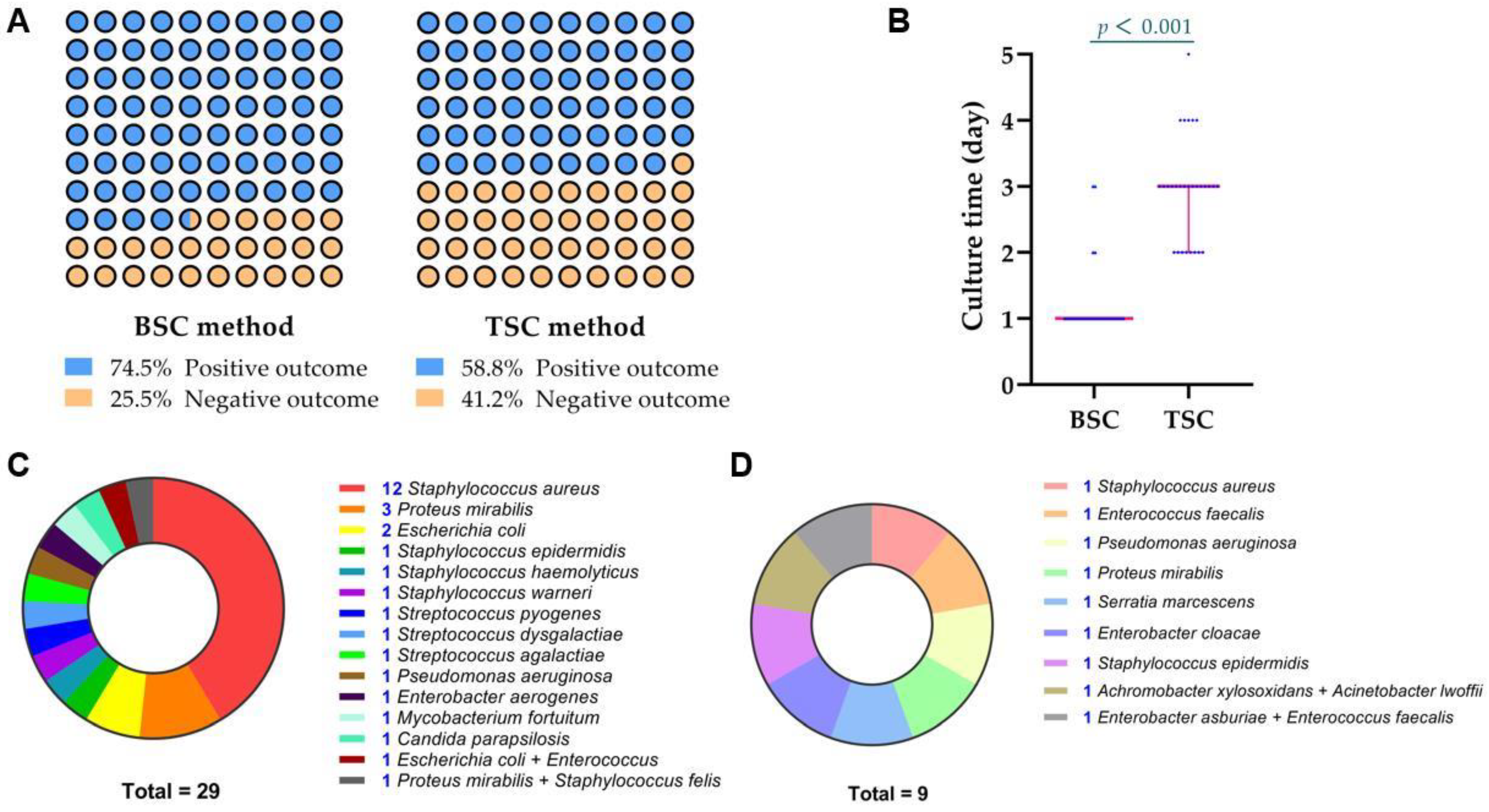
3.2. BSC and TSC Outcomes and Culture Time
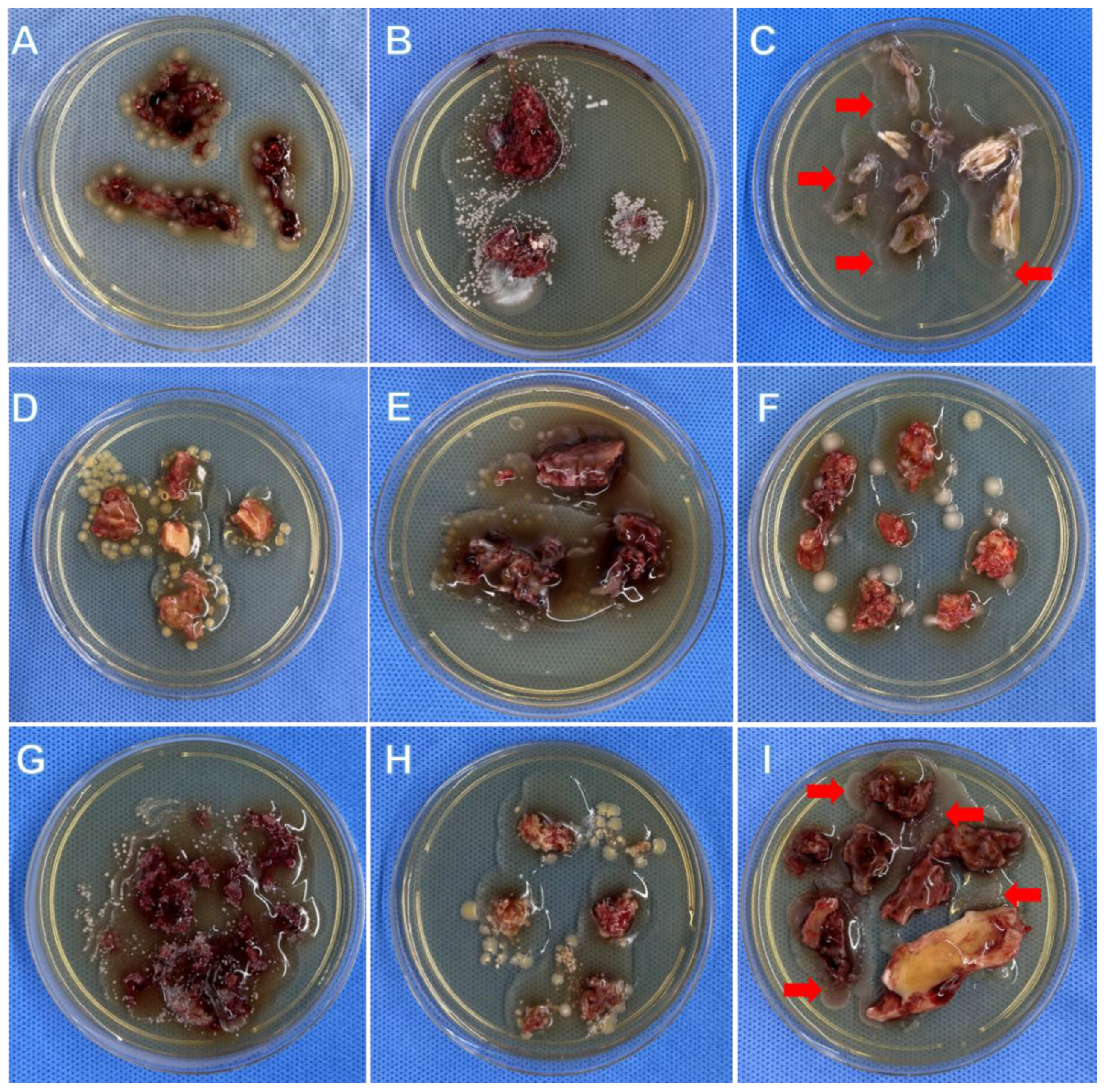
3.3. Microorganism Type
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arshad, Z.; Lau, E.J.-S.; Aslam, A.; Thahir, A.; Krkovic, M. Management of chronic osteomyelitis of the femur and tibia: A scoping review. EFORT Open Rev. 2021, 6, 704–715. [Google Scholar] [CrossRef] [PubMed]
- Lew, D.P.; Waldvogel, F.A. Osteomyelitis. Lancet 2004, 364, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Panteli, M.; Giannoudis, P.V. Chronic osteomyelitis: What the surgeon needs to know. EFORT Open Rev. 2016, 1, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Mathews, J.; Ward, J.; Chapman, T.; Khan, U.; Kelly, M. Single-stage orthoplastic reconstruction of Gustilo–Anderson Grade III open tibial fractures greatly reduces infection rates. Injury 2015, 46, 2263–2266. [Google Scholar] [CrossRef] [PubMed]
- Lazzarini, L.; Mader, J.T.; Calhoun, J.H. Osteomyelitis in long bones. J. Bone Joint Surg. Am. 2004, 86, 2305–2318. [Google Scholar] [CrossRef]
- Yong, T.M.; Rackard, F.A.; Dutton, L.K.; Sparks, M.B.; Harris, M.B.; Gitajn, I.L. Analyzing risk factors for treatment failure in fracture-related infection. Arch. Orthop. Trauma Surg. 2022. [Google Scholar] [CrossRef]
- Birt, M.C.; Anderson, D.W.; Toby, E.B.; Wang, J. Osteomyelitis: Recent advances in pathophysiology and therapeutic strategies. J. Orthop. 2017, 14, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Pardo, A.; Gómez-Florit, M.; Barbosa, S.; Taboada, P.; Domingues, R.M.A.; Gomes, M.E. Magnetic Nanocomposite Hydrogels for Tissue Engineering: Design Concepts and Remote Actuation Strategies to Control Cell Fate. ACS Nano 2021, 15, 175–209. [Google Scholar] [CrossRef]
- Post, J.C.; A Preston, R.; Aul, J.J.; Larkins-Pettigrew, M.; Rydquist-White, J.; Anderson, K.W.; Wadowsky, R.M.; Reagan, D.R.; Walker, E.S.; A Kingsley, L.; et al. Molecular analysis of bacterial pathogens in otitis media with effusion. JAMA 1995, 273, 1598–1604. [Google Scholar] [CrossRef]
- Ahmed, E.A.; Almutairi, M.K.; Alkaseb, A.T. Accuracy of Tissue and Sonication Fluid Sampling for the Diagnosis of Fracture-Related Infection: Diagnostic Meta-Analysis. Cureus 2021, 13, e14925. [Google Scholar] [CrossRef]
- Dudareva, M.; Barrett, L.; Morgenstern, M.; Atkins, B.; Brent, A.; McNally, M. Providing an Evidence Base for Tissue Sampling and Culture Interpretation in Suspected Fracture-Related Infection. J. Bone Joint Surg. Am. 2021, 103, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Finelli, C.A.; da Silva, C.B.; Murça, M.A.; dos Reis, F.B.; Miki, N.; Fernandes, H.A.; Dell’Aquila, A.; Salles, M.J. Microbiological diagnosis of intramedullary nailing infection: Comparison of bacterial growth between tissue sampling and sonication fluid cultures. Int. Orthop. 2021, 45, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Onsea, J.; Pallay, J.; Depypere, M.; Moriarty, T.F.; Van Lieshout, E.M.; Obremskey, W.T.; Sermon, A.; Hoekstra, H.; Verhofstad, M.H.; Nijs, S.; et al. Intramedullary tissue cultures from the Reamer-Irrigator-Aspirator system for diagnosing fracture-related infection. J. Orthop. Res. 2020, 39, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Moley, J.P.; McGrath, M.S.; Granger, J.F.; Sullivan, A.C.; Stoodley, P.; Dusane, D. Mapping bacterial biofilms on recovered orthopaedic implants by a novel agar candle dip method. APMIS 2019, 127, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Liang, N.; Hu, Y.J.; Lin, Q.R.; Chen, P.; Wan, H.Y.; He, S.Y.; Stoodley, P.; Yu, B. Implant surface culture may be a useful adjunct to standard tissue sampling culture for identification of pathogens accounting for fracture-device-related infection: A within-person randomized agreement study of 42 patients. Acta Orthop. 2022, 93, 703–708. [Google Scholar]
- Hofstee, M.I.; Muthukrishnan, G.; Atkins, G.J.; Riool, M.; Thompson, K.; Morgenstern, M.; Stoddart, M.J.; Richards, R.G.; Zaat, S.A.J.; Moriarty, T.F. Current Concepts of Osteomyelitis: From Pathologic Mechanisms to Advanced Research Methods. Am. J. Pathol 2020, 190, 1151–1163. [Google Scholar] [CrossRef]
- McNally, M.; Govaert, G.; Dudareva, M.; Morgenstern, M.; Metsemakers, W.-J. Definition and diagnosis of fracture-related infection. EFORT Open Rev. 2020, 5, 614–619. [Google Scholar] [CrossRef]
- Govaert, G.A.M.; Kuehl, R.; Atkins, B.L.; Trampuz, A.; Morgenstern, M.; Obremskey, W.T.; Verhofstad, M.H.J.; McNally, M.A.; Metsemakers, W.-J. Diagnosing Fracture-Related Infection: Current Concepts and Recommendations. J. Orthop. Trauma 2020, 34, 8–17. [Google Scholar] [CrossRef]
- Morgenstern, M.; Athanasou, N.A.; Ferguson, J.Y.; Metsemakers, W.-J.; Atkins, B.L.; McNally, M.A. The value of quantitative histology in the diagnosis of fracture-related infection. Bone Joint J. 2018, 100, 966–972. [Google Scholar] [CrossRef]
- Steinmetz, S.; Wernly, D.; Moerenhout, K.; Trampuz, A.; Borens, O. Infection after fracture fixation. EFORT Open Rev. 2019, 4, 468–475. [Google Scholar] [CrossRef]
- Wang, B.; Xiao, X.; Zhang, J.; Han, W.; Hersi, S.A.; Tang, X. Epidemiology and microbiology of fracture-related infection: A multicenter study in Northeast China. J. Orthop. Surg. Res. 2021, 16, 490. [Google Scholar] [CrossRef] [PubMed]
- Bariteau, J.T.; Waryasz, G.R.; McDonnell, M.; Fischer, S.A.; Hayda, C.R.A.; Born, C.T. Fungal Osteomyelitis and Septic Arthritis. J. Am. Acad. Orthop. Surg. 2014, 22, 390–401. [Google Scholar] [CrossRef] [PubMed]
- Gamaletsou, M.N.; Rammaert, B.; Bueno, M.A.; Sipsas, N.V.; Moriyama, B.; Kontoyiannis, D.P.; Roilides, E.; Zeller, V.; Taj-Aldeen, S.J.; Miller, A.O.; et al. Candida Arthritis: Analysis of 112 Pediatric and Adult Cases. Open Forum Infect. Dis. 2015, 3, ofv207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grantham, W.J.; Raynor, M.B.; Martus, J.E. Articular Sinus Tract with Mycobacterium fortuitum Osteomyelitis After Anterior Cruciate Ligament Reconstruction: A Case Report. JBJS Case Connect. 2015, 5, e105. [Google Scholar] [CrossRef] [PubMed]
- Fraga, K.; Maireles, M.; Jordan, M.; Soldevila, L.; Murillo, O. Mycobacterium fortuitum osteomyelitis of the cuboid bone treated with CERAMENT G and V: A case report. JBJT 2022, 7, 163–167. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Sex/Age (Year) | Infection Site | BSC Outcome | BSC Time (Day) | TSC Outcome | TSC Time (Day) |
|---|---|---|---|---|---|---|
| 1 | M/14 | Femur | Staphylococcus aureus | 1 | Staphylococcus aureus | 3 |
| 2 | M/29 | Tibia | Staphylococcus aureus | 1 | Staphylococcus aureus | 3 |
| 3 | M/41 | Tibia | Achromobacter xylosoxidans + Acinetobacter lwoffii | 3 | Negative | NA |
| 4 | M/49 | Tibia | Escherichia coli | 1 | Escherichia coli | 3 |
| 5 | F/49 | Calcaneus | Negative | NA | Negative | NA |
| 6 | M/44 | Tibia | Staphylococcus epidermidis | 3 | Negative | NA |
| 7 | M/53 | Femur | Staphylococcus aureus | 1 | Staphylococcus aureus | 3 |
| 8 | M/14 | Tibia | Streptococcus pyogenes | 1 | Streptococcus pyogenes | 2 |
| 9 | F/32 | Tibia | Candida parapsilosis | 1 | Candida parapsilosis | 2 |
| 10 | M/71 | Tibia | Proteus mirabilis | 1 | Proteus mirabilis | 2 |
| 11 | M/59 | Femur | Proteus mirabilis | 1 | Proteus mirabilis | 2 |
| 12 | M/10 | Phalange | Staphylococcus epidermidis | 1 | Staphylococcus epidermidis | 3 |
| 13 | M/53 | Calcaneus | Proteus mirabilis + Staphylococcus felis | 1 | Proteus mirabilis + Staphylococcus felis | 5 |
| 14 | M/51 | Calcaneus | Staphylococcus aureus | 1 | Staphylococcus aureus | 4 |
| 15 | M/59 | Radius | Staphylococcus aureus | 1 | Negative | NA |
| 16 | M/21 | Humerus | Negative | NA | Negative | NA |
| 17 | M/50 | Tibia | Staphylococcus aureus | 1 | Staphylococcus aureus | 2 |
| 18 | M/49 | Tibia | Staphylococcus aureus | 1 | Staphylococcus aureus | 4 |
| 19 | M/16 | Femur | Enterococcus faecalis | 1 | Negative | NA |
| 20 | F/68 | Tibia | Negative | NA | Negative | NA |
| 21 | M/68 | Calcaneus | Proteus mirabilis | 1 | Proteus mirabilis | 3 |
| 22 | F/54 | Calcaneus | Negative | NA | Negative | NA |
| 23 | M/46 | Calcaneus | Staphylococcus aureus | 1 | Staphylococcus aureus | 3 |
| 24 | F/48 | Femur | Staphylococcus aureus | 1 | Staphylococcus aureus | 4 |
| 25 | M/42 | Tibia | Enterobacter cloacae | 1 | Negative | NA |
| 26 | M/37 | Tibia | Negative | NA | Negative | NA |
| 27 | M/39 | Tibia | Mycobacterium fortuitum | 3 | Mycobacterium fortuitum | 3 |
| 28 | M/87 | Humerus | Pseudomonas aeruginosa | 3 | Pseudomonas aeruginosa | 3 |
| 29 | M/52 | Calcaneus | Negative | NA | Negative | NA |
| 30 | M/47 | Calcaneus | Staphylococcus aureus | 1 | Staphylococcus aureus | 3 |
| 31 | M/15 | Tibia | Negative | NA | Negative | NA |
| 32 | M/29 | Phalange | Staphylococcus aureus | 1 | Staphylococcus aureus | 2 |
| 33 | M/36 | Femur | Negative | NA | Staphylococcus aureus | 3 |
| 34 | M/52 | Tibia | Pseudomonas aeruginosa | 3 | Negative | NA |
| 35 | M/56 | Tibia | Staphylococcus warneri | 2 | Staphylococcus warneri | 3 |
| 36 | M/32 | Tibia | Negative | NA | Negative | NA |
| 37 | M/67 | Calcaneus | Escherichia coli | 1 | Escherichia coli | 4 |
| 38 | M/29 | Tibia | Staphylococcus haemolyticus | 1 | Staphylococcus haemolyticus | 3 |
| 39 | M/45 | Calcaneus | Negative | NA | Negative | NA |
| 40 | M/37 | Tibia | Negative | NA | Negative | NA |
| 41 | M/49 | Ulna | Serratia marcescens | 1 | Negative | NA |
| 42 | M/66 | Tibia | Staphylococcus aureus | 1 | Staphylococcus aureus | 2 |
| 43 | M/25 | Tibia | Staphylococcus aureus | 1 | Staphylococcus aureus | 3 |
| 44 | M/48 | Calcaneus | Streptococcus agalactiae | 1 | Streptococcus agalactiae | 4 |
| 45 | F/63 | Tibia | Streptococcus dysgalactiae | 2 | Streptococcus dysgalactiae | 3 |
| 46 | M/30 | Tibia | Proteus mirabilis | 1 | Negative | NA |
| 47 | M/43 | Femur | Enterobacter aerogenes | 1 | Enterobacter aerogenes | 3 |
| 48 | M/49 | Tibia | Negative | NA | Negative | NA |
| 49 | F/8 | Tibia | Negative | NA | Negative | NA |
| 50 | M/30 | Femur | Escherichia coli + Enterococcus | 1 | Escherichia coli + Enterococcus | 2 |
| 51 | F/65 | Humerus | Enterobacter asburiae + Enterococcus faecalis | 2 | Negative | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, P.; Lin, Q.-r.; Huang, M.-Z.; Zhang, X.; Hu, Y.-j.; Chen, J.; Jiang, N.; Yu, B. Devascularized Bone Surface Culture: A Novel Strategy for Identifying Osteomyelitis-Related Pathogens. J. Pers. Med. 2022, 12, 2050. https://doi.org/10.3390/jpm12122050
Chen P, Lin Q-r, Huang M-Z, Zhang X, Hu Y-j, Chen J, Jiang N, Yu B. Devascularized Bone Surface Culture: A Novel Strategy for Identifying Osteomyelitis-Related Pathogens. Journal of Personalized Medicine. 2022; 12(12):2050. https://doi.org/10.3390/jpm12122050
Chicago/Turabian StyleChen, Peng, Qing-rong Lin, Mou-Zhang Huang, Xin Zhang, Yan-jun Hu, Jing Chen, Nan Jiang, and Bin Yu. 2022. "Devascularized Bone Surface Culture: A Novel Strategy for Identifying Osteomyelitis-Related Pathogens" Journal of Personalized Medicine 12, no. 12: 2050. https://doi.org/10.3390/jpm12122050