
A Longitudinal Analysis of the Internal Rotation and Shift (IRO/Shift) Test Following Arthroscopic Repair of Superior Rotator Cuff Lesions
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
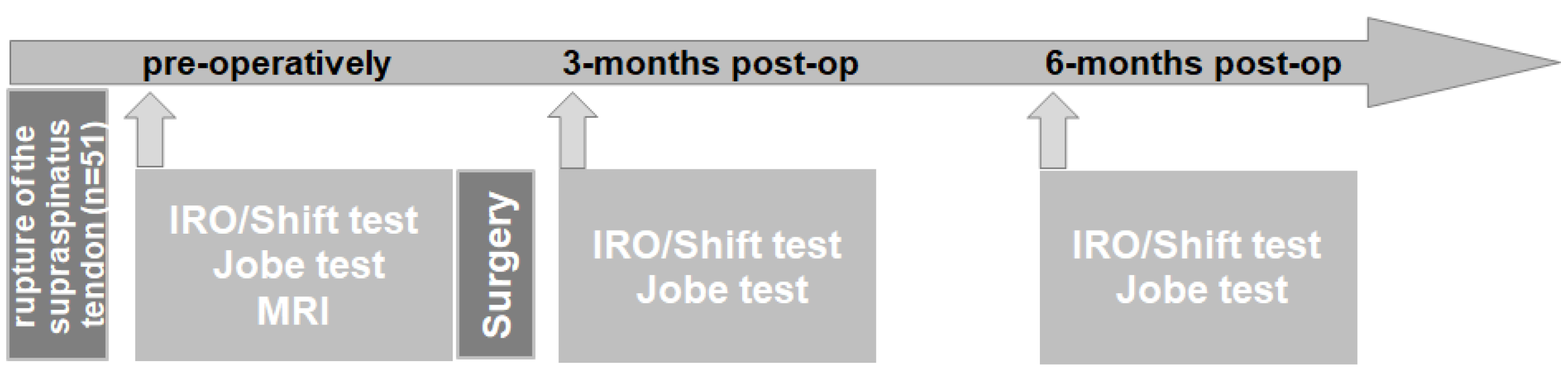
2.1. Subjects
2.2. Procedures
2.3. Statistical Analysis
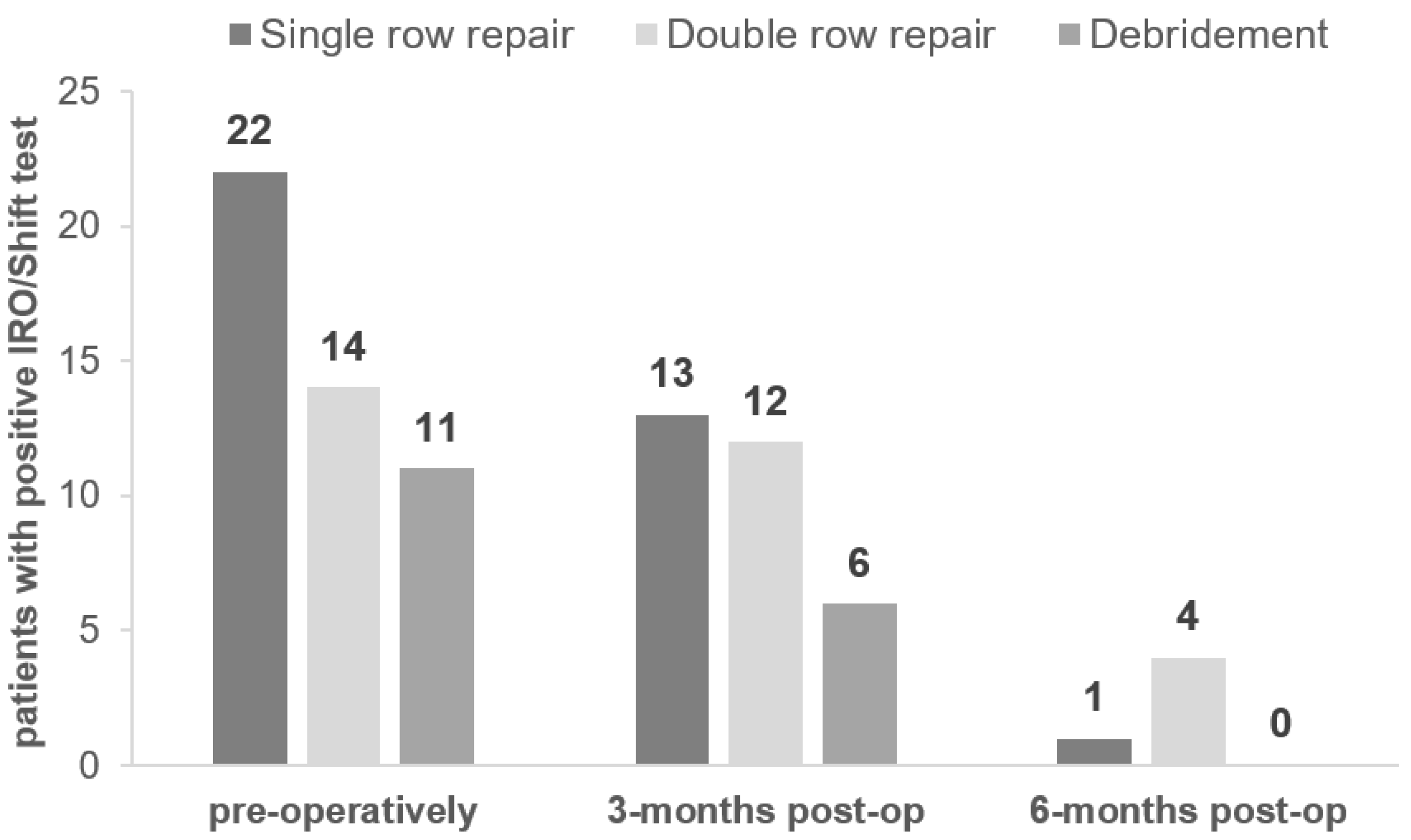
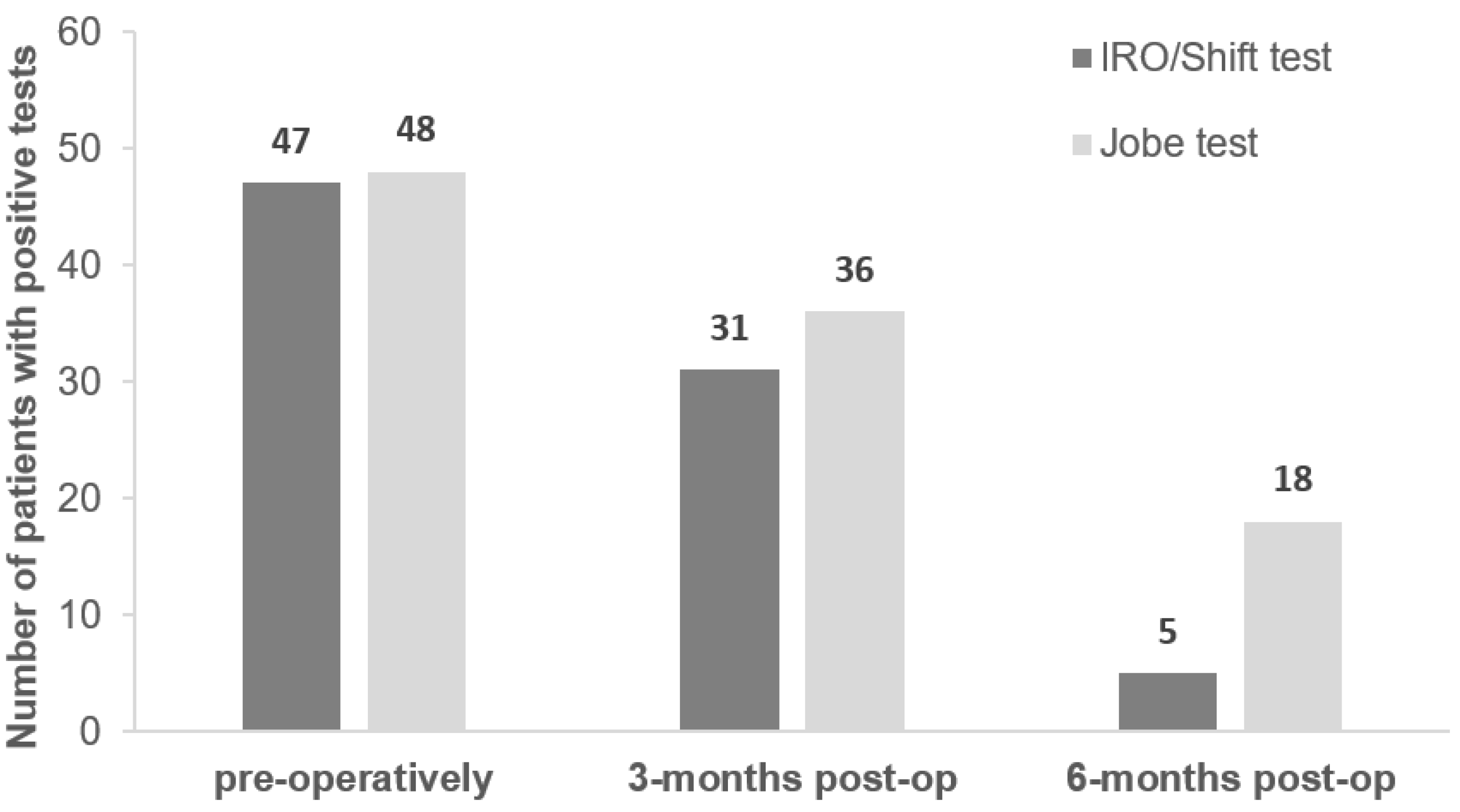
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hawkins, R.J.; Bokor, D.J. Clinical Evaluation of Shoulder Problems. The Shoulder; Saunders: Philadelphia, PA, USA, 1990. [Google Scholar]
- Lädermann, A.; Meynard, T.; Denard, P.J.; Ibrahim, M.; Saffarini, M.; Collin, P. Reliable diagnosis of posterosuperior rotator cuff tears requires a combination of clinical tests. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 2118–2133. [Google Scholar] [CrossRef] [PubMed]
- van Kampen, D.A.; van den Berg, T.; van der Woude, H.J.; Castelein, R.M.; Scholtes, V.A.; Terwee, C.B.; Willems, W.J. The diagnostic value of the combination of patient characteristics, history, and clinical shoulder tests for the diagnosis of rotator cuff tear. J. Orthop. Surg. Res. 2014, 9, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Águila-Ledesma, I.R.; Córdova-Fonseca, J.L.; Medina-Pontaza, O.; A Núñez-Gómez, D.; Calvache-García, C.; Pérez-Atanasio, J.M.; Torres-González, R. Diagnostic value of a predictive model for complete ruptures of the rotator cuff associated to subacromial impingement. Acta Ortop. Mex. 2017, 31, 108–112. [Google Scholar] [PubMed]
- Jain, N.B.; Luz, J.; Higgins, L.D.; Dong, Y.; Warner, J.J.P.; Matzkin, E.; Katz, J.N. The Diagnostic Accuracy of Special Tests for Rotator Cuff Tear: The ROW Cohort Study. Am. J. Phys. Med. Rehabil. 2017, 96, 176–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadogan, A.; McNair, P.J.; Laslett, M.; Hing, W.A. Diagnostic Accuracy of Clinical Examination and Imaging Findings for Identifying Subacromial Pain. PLoS ONE 2016, 11, e0167738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sgroi, M.; Loitsch, T.; Reichel, H.; Kappe, T. Diagnostic Value of Clinical Tests for Supraspinatus Tendon Tears. Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 2326–2333. [Google Scholar] [CrossRef]
- Somerville, L.E.; Willits, K.; Johnson, A.M.; Litchfield, R.; Lebel, M.-E.; Moro, J.; Bryant, D. Clinical Assessment of Physical Examination Maneuvers for Rotator Cuff Lesions. Am. J. Sports Med. 2014, 42, 1911–1919. [Google Scholar] [CrossRef]
- Fieseler, G.; Laudner, K.; Sendler, J.; Cornelius, J.; Schulze, S.; Lehmann, W.; Hermassi, S.; Delank, K.-S.; Schwesig, R. The internal rotation and shift-test for the detection of superior lesions of the rotator cuff: Reliability and clinical performance. JSES Int. 2022, 6, 495–499. [Google Scholar] [CrossRef]
- Fieseler, G. Der IRO-/Shift-Test zur klinischen Diagnostik superiorer Rotatorenmanschettendefekte. Arthroskopie 2021, 34, 456–458. [Google Scholar] [CrossRef]
- Fieseler, G.; Sendler, J.; Cornelius, J.; Schulze, S.; Delank, K.S.; Bartels, T.; Schwesig, R. Der Innenrotations/Shift-Test; Erweiterung der manuellen Diagnostik bei superioren Rotatorenmanschettendefekten—Übereinstimmung der klinischen Untersuchung mit fachradiologischen MRT-Befunden. Sport. Orthop. Traumatol. 2020, 32, 192–193. [Google Scholar] [CrossRef]
- Fieseler, G.; Schwesig, R.; Sendler, J.; Cornelius, J.; Schulze, S.; Lehmann, W.; Hermassi, S.; Delank, K.-S.; Laudner, K. IRO/Shift Test Is Comparable to the Jobe Test for Detection of Supraspinatus Lesions. J. Pers. Med. 2022, 12, 1422. [Google Scholar] [CrossRef] [PubMed]
- Iannotti, J.P.; Deutsch, A.; Green, A.; Rudicel, S.; Christensen, J.; Marraffino, S.; Rodeo, S. Time to failure after rotator cuff repair: A prospective imaging study. J. Bone Jt. Surg. Am. 2013, 95, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Voleti, P.B.; Buckley, M.R.; Soslowsky, L.J. Tendon Healing: Repair and Regeneration. Annu. Rev. Biomed. Eng. 2012, 14, 47–71. [Google Scholar] [CrossRef] [PubMed]
- Leadbetter, W.B. Cell-Matrix Response in Tendon Injury. Clin. Sports Med. 1992, 11, 533–578. [Google Scholar] [CrossRef] [PubMed]
- Nagasawa, K.; Noguchi, M.; Ikoma, K.; Kubo, T. Static and dynamic biomechanical properties of the regenerating rabbit Achilles tendon. Clin. Biomech. 2008, 23, 832–838. [Google Scholar] [CrossRef] [PubMed]
- He, H.B.; Wang, T.; Wang, M.C.; Zhu, H.F.; Meng, Y.; Pan, C.L.; Hu, Y.; Chao, X.M.; Yang, C.Y.; Wang, M. Tendon-to-bone healing after repairing full-thickness rotator cuff tear with a triple-loaded single-row method in young patients. BMC Musculoskelet. Disord. 2021, 22, 305. [Google Scholar] [CrossRef] [PubMed]
- Baysal, D.; Balyk, R.; Otto, D.; Luciak-Corea, C.; Beaupre, L. Functional Outcome and Health-Related Quality of Life after Surgical Repair of Full-Thickness Rotator Cuff Tear Using a Mini-Open Technique. Am. J. Sports Med. 2005, 33, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Charousset, C.; Grimberg, J.; Duranthon, L.D.; Bellaïche, L.; Petrover, D.; Kalra, K. The Time for Functional Recovery After Arthroscopic Rotator Cuff Repair: Correlation With Tendon Healing Controlled by Computed Tomography Arthrography. Arthrosc. J. Arthrosc. Relat. Surg. 2008, 24, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Rokito, A.S.; Zuckerman, J.D.; Gallagher, M.A.; Cuomo, F. Strength after surgical repair of the rotator cuff. J. Shoulder Elb. Surg. 1996, 5, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Tashjian, R.Z.; Hollins, A.M.; Kim, H.-M.; Teefey, S.A.; Middleton, W.D.; Steger-May, K.; Galatz, L.M.; Yamaguchi, K. Factors Affecting Healing Rates after Arthroscopic Double-Row Rotator Cuff Repair. Am. J. Sports Med. 2010, 38, 2435–2442. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Test | Sensitivity (95% CI) | Specificity (95% CI) |
|---|---|---|
| IRO/Shift (%) | 92 (87–100) | 68 (51–85) |
| Jobe (%) | 94 (88–100) | 78 (64–91) |
| Time Point | Observed Accuracy | Chi-Squared Test (p-Value) | ||
|---|---|---|---|---|
| Negative (n) | Positive (n) | % | ||
| Pre-operative | 1 | 45 | 90 | 2.87 (0.091) |
| 3 months post-op | 10 | 26 | 71 | 6.72 (0.010) |
| 6 months post-op | 31 | 3 | 67 | 1.48 (0.224) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwesig, R.; Fieseler, G.; Cornelius, J.; Sendler, J.; Schulze, S.; Hermassi, S.; Delank, K.-S.; Laudner, K. A Longitudinal Analysis of the Internal Rotation and Shift (IRO/Shift) Test Following Arthroscopic Repair of Superior Rotator Cuff Lesions. J. Pers. Med. 2022, 12, 2018. https://doi.org/10.3390/jpm12122018
Schwesig R, Fieseler G, Cornelius J, Sendler J, Schulze S, Hermassi S, Delank K-S, Laudner K. A Longitudinal Analysis of the Internal Rotation and Shift (IRO/Shift) Test Following Arthroscopic Repair of Superior Rotator Cuff Lesions. Journal of Personalized Medicine. 2022; 12(12):2018. https://doi.org/10.3390/jpm12122018
Chicago/Turabian StyleSchwesig, René, George Fieseler, Jakob Cornelius, Julia Sendler, Stephan Schulze, Souhail Hermassi, Karl-Stefan Delank, and Kevin Laudner. 2022. "A Longitudinal Analysis of the Internal Rotation and Shift (IRO/Shift) Test Following Arthroscopic Repair of Superior Rotator Cuff Lesions" Journal of Personalized Medicine 12, no. 12: 2018. https://doi.org/10.3390/jpm12122018