
A Body Shape Index (ABSI) as a Variant of Conicity Index Not Affected by the Obesity Paradox: A Cross-Sectional Study Using Arterial Stiffness Parameter

Abstract
:1. Introduction
2. Results
2.1. Clinical and Biochemical Characteristics of Male and Female Participants
2.2. Correlation of Each Adiposity Index with Age or CAVI by Obesity Grade
2.3. Discriminatory Power of Each Adiposity Index for High CAVI (≥9.0)
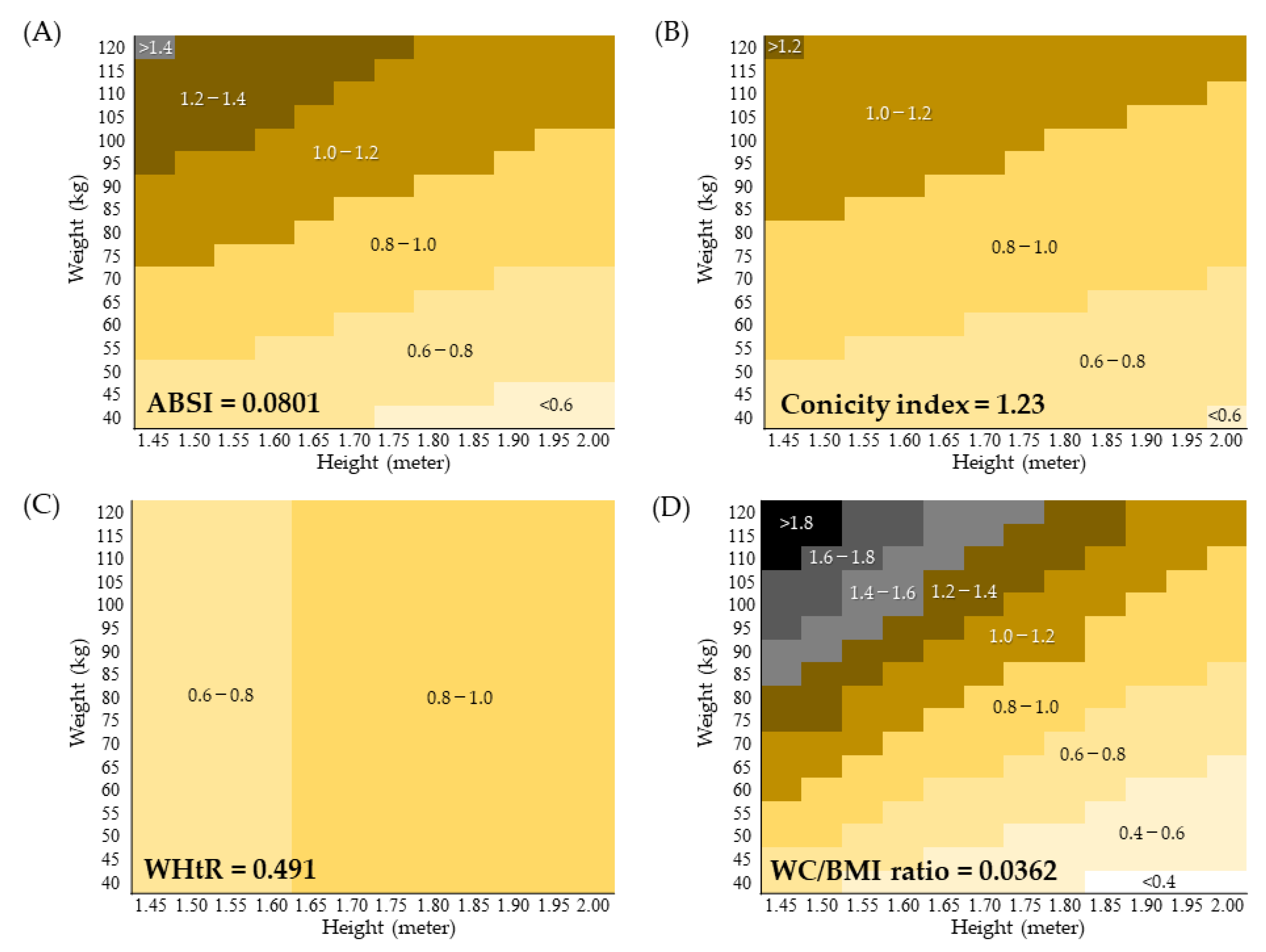
2.4. Waist Circumference Distribution Calculated from the Cutoff of Each Abdominal Obesity Index
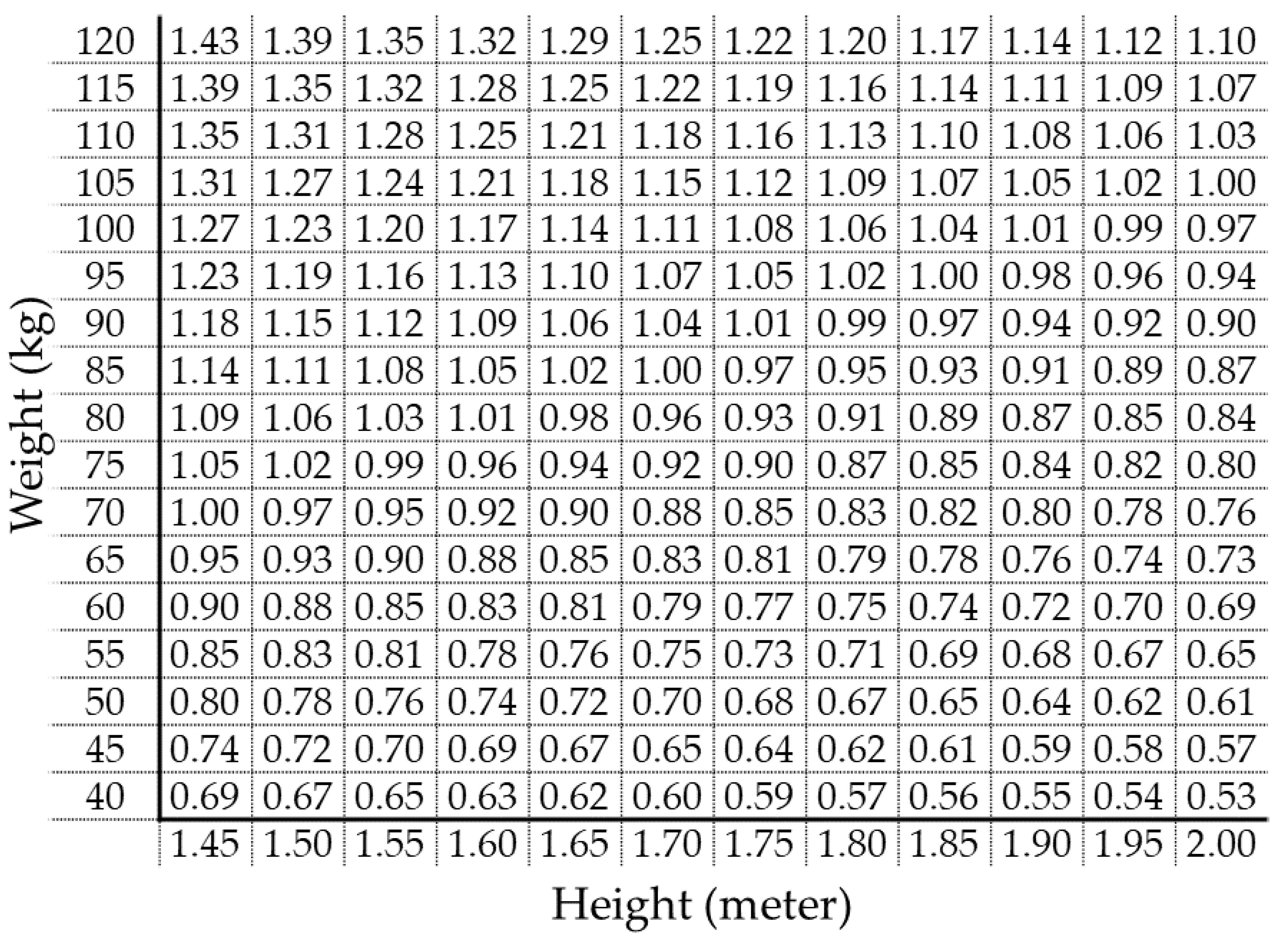
2.5. Waist Circumference Calculator Chart Corresponding to Cutoff of ABSI
2.6. Correlation between Body Adiposity Indices
3. Discussion
4. Materials and Methods
4.1. Subjects and Design
4.2. Data Collection and Methods of Measurement
4.3. Measurement of CAVI as an Arterial Stiffness Parameter
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matsuzawa, Y.; Funahashi, T.; Nakamura, T. The Concept of Metabolic Syndrome: Contribution of Visceral Fat Accumulation and Its Molecular Mechanism. J. Atheroscler. Thromb. 2011, 18, 629–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juonala, M.; Viikari, J.S.; Laitinen, T.; Marniemi, J.; Helenius, H.; Rönnemaa, T.; Raitakari, O.T. Interrelations Between Brachial Endothelial Function and Carotid Intima-Media Thickness in Young Adults: The cardiovascular risk in young Finns study. Circulation 2004, 110, 2918–2923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiura, T.; Dohi, Y.; Takagi, Y.; Yoshikane, N.; Ito, M.; Suzuki, K.; Nagami, T.; Iwase, M.; Seo, Y.; Ohte, N. Relationships of Obesity-Related Indices and Metabolic Syndrome with Subclinical Atherosclerosis in Middle-Aged Untreated Japanese Workers. J. Atheroscler. Thromb. 2020, 27, 342–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carbone, S.; Canada, J.M.; Billingsley, H.E.; Siddiqui, M.S.; Elagizi, A.; Lavie, C.J. Obesity paradox in cardiovascular disease: Where do we stand? Vasc. Health Risk Manag. 2019, 15, 89–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minetto, M.A.; Pietrobelli, A.; Busso, C.; Bennett, J.P.; Ferraris, A.; Shepherd, J.A.; Heymsfield, S.B. Digital Anthropometry for Body Circumference Measurements: European Phenotypic Variations throughout the Decades. J. Pers. Med. 2022, 12, 906. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, D.; Watanabe, Y.; Yamaguchi, T.; Maruyama, M.; Saiki, A.; Shirai, K.; Tatsuno, I. New index of abdominal obesity, a body shape index, is BMI-independently associated with systemic arterial stiffness in real-world Japanese population. Int. J. Clin. Pharmacol. Ther. 2020, 58, 709–717. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. Dynamic Association of Mortality Hazard with Body Shape. PLoS ONE 2014, 9, e88793. [Google Scholar] [CrossRef]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.; Pencina, M.J.; Hamburg, N.; Vita, J.; Levy, D.; Benjamin, E. Arterial Stiffness and Cardiovascular Events: The Framingham heart study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Shirai, K.; Utino, J.; Otsuka, K.; Takata, M. A Novel Blood Pressure-independent Arterial Wall Stiffness Parameter; Cardio-Ankle Vascular Index (CAVI). J. Atheroscler. Thromb. 2006, 13, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Saiki, A.; Ohira, M.; Yamaguchi, T.; Nagayama, D.; Shimizu, N.; Shirai, K.; Tatsuno, I. New Horizons of Arterial Stiffness Developed Using Cardio-Ankle Vascular Index (CAVI). J. Atheroscler. Thromb. 2020, 27, 732–748. [Google Scholar] [CrossRef]
- Namba, T.; Masaki, N.; Takase, B.; Adachi, T. Arterial Stiffness Assessed by Cardio-Ankle Vascular Index. Int. J. Mol. Sci. 2019, 20, 3664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagayama, D.; Watanabe, Y.; Yamaguchi, T.; Suzuki, K.; Saiki, A.; Fujishiro, K.; Shirai, K. Issue of Waist Circumference for the Diagnosis of Metabolic Syndrome Regarding Arterial Stiffness: Possible Utility of a Body Shape Index in Middle-Aged Nonobese Japanese Urban Residents Receiving Health Screening. Obes. Facts 2022, 15, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Roriz, A.K.C.; Passos, L.C.S.; De Oliveira, C.C.; Eickemberg, M.; Moreira, P.D.A.; Sampaio, L.R. Evaluation of the Accuracy of Anthropometric Clinical Indicators of Visceral Fat in Adults and Elderly. PLoS ONE 2014, 9, e103499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valdez, R. A simple model-based index of abdominal adiposity. J. Clin. Epidemiol. 1991, 44, 955–956. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, D.; Endo, K.; Ohira, M.; Yamaguchi, T.; Ban, N.; Kawana, H.; Nagumo, A.; Saiki, A.; Oyama, T.; Miyashita, Y.; et al. Effects of body weight reduction on cardio-ankle vascular index (CAVI). Obes. Res. Clin. Pract. 2013, 7, e139–e145. [Google Scholar] [CrossRef] [PubMed]
- Anoop, S.; Krakauer, J.; Krakauer, N.; Misra, A. A Body shape index significantly predicts MRI-defined abdominal adipose tissue depots in non-obese Asian Indians with type 2 diabetes mellitus. BMJ Open Diabetes Res. Care 2020, 8, e001324. [Google Scholar] [CrossRef]
- Bertoli, S.; Leone, A.; Krakauer, N.Y.; Bedogni, G.; Vanzulli, A.; Redaelli, V.I.; De Amicis, R.; Vignati, L.; Krakauer, J.C.; Battezzati, A. Association of Body Shape Index (ABSI) with cardio-metabolic risk factors: A cross-sectional study of 6081 Caucasian adults. PLoS ONE 2017, 12, e0185013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ofstad, A.P.; Sommer, C.; I Birkeland, K.; Bjørgaas, M.R.; Gran, J.M.; Gulseth, H.L.; Johansen, O.E. Comparison of the associations between non-traditional and traditional indices of adiposity and cardiovascular mortality: An observational study of one million person-years of follow-up. Int. J. Obes. 2019, 43, 1082–1092. [Google Scholar] [CrossRef] [Green Version]
- Leone, A.; Vizzuso, S.; Brambilla, P.; Mameli, C.; Ravella, S.; De Amicis, R.; Battezzati, A.; Zuccotti, G.; Bertoli, S.; Verduci, E. Evaluation of Different Adiposity Indices and Association with Metabolic Syndrome Risk in Obese Children: Is there a Winner? Int. J. Mol. Sci. 2020, 21, 4083. [Google Scholar] [CrossRef]
- Nagayama, D.; Fujishiro, K.; Tsuda, S.; Watanabe, Y.; Yamaguchi, T.; Suzuki, K.; Saiki, A.; Shirai, K. Enhanced prediction of renal function decline by replacing waist circumference with “A Body Shape Index (ABSI)” in diagnosing metabolic syndrome: A retrospective cohort study in Japan. Int. J. Obes. 2021, 46, 564–573. [Google Scholar] [CrossRef]
- Krakauer, N.Y.; Krakauer, J.C. Anthropometrics, Metabolic Syndrome, and Mortality Hazard. J. Obes. 2018, 2018, 9241904. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.M.Y.; Huxley, R.R.; Wildman, R.P.; Woodward, M. Indices of abdominal obesity are better discriminators of cardiovascular risk factors than BMI: A meta-analysis. J. Clin. Epidemiol. 2008, 61, 646–653. [Google Scholar] [CrossRef]
- Corrada, M.M.; Kawas, C.H.; Mozaffar, F.; Paganini-Hill, A. Association of Body Mass Index and Weight Change with All-Cause Mortality in the Elderly. Am. J. Epidemiol. 2006, 163, 938–949. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, A.; Tomiyama, H.; Maruhashi, T.; Matsuzawa, Y.; Miyoshi, T.; Kabutoya, T.; Kario, K.; Sugiyama, S.; Munakata, M.; Ito, H.; et al. Physiological Diagnostic Criteria for Vascular Failure. Hypertension 2018, 72, 1060–1071. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | All Subjects | Males | Females | p Value * |
|---|---|---|---|---|
| Number of subjects | 62,514 | 26,037 | 36,477 | - |
| Age (years) | 42 (34–54) | 40 (33–51) | 45 (36–55) | <0.001 |
| Height (m) | 1.62 (1.56–1.69) | 1.71 (1.67–1.75) | 1.57 (1.54–1.61) | <0.001 |
| Body weight (kg) | 57.2 (50.1–66.6) | 66.9 (60.7–74.1) | 51.6 (47.2–57.0) | <0.001 |
| BMI (kg/m2) | 21.7 (19.8–24.0) | 23.0 (21.2–25.2) | 20.8 (19.1–22.9) | <0.001 |
| WC (m) | 0.78 (0.72–0.85) | 0.82 (0.76–0.89) | 0.75 (0.70–0.82) | <0.001 |
| ABSI | 0.0785 (0.0757–0.0815) | 0.0778 (0.0754–0.0803) | 0.0791 (0.0760–0.0825) | <0.001 |
| Conicity index | 1.21 (1.16–1.26) | 1.207 (1.16–1.25) | 1.210 (1.15–1.26) | 0.012 |
| WHtR | 0.480 (0.444–0.521) | 0.484 (0.449–0.520) | 0.477 (0.441–0.521) | <0.001 |
| WC/BMI ratio | 0.0358 (0.0342–0.0375) | 0.0357 (0.0342–0.0372) | 0.0360 (0.0342–0.0378) | <0.001 |
| CAVI | 7.3 (6.8–8.0) | 7.3 (6.8–8.0) | 7.3 (6.8–8.0) | <0.001 |
| SBP (mmHg) | 120 (111–130) | 124 (116–132) | 118 (108–128) | <0.001 |
| DBP (mmHg) | 70 (64–78) | 74 (67–81) | 68 (62–76) | <0.001 |
| FPG (mg/dL) | 84 (79–90) | 86 (81–91) | 82 (78–88) | <0.001 |
| TG (mg/dL) | 76 (54–113) | 96 (67–146) | 66 (49–93) | <0.001 |
| HDL-C (mg/dL) | 67 (56–80) | 58 (49–69) | 74 (63–86) | <0.001 |
| No. of Subjects | BMI | WC | ABSI | Conicity Index | WHtR | WC/BMI Ratio | ||
|---|---|---|---|---|---|---|---|---|
| With Age | ||||||||
| Total | 62,514 | Rs | 0.111 | 0.203 | 0.389 | 0.387 | 0.346 | 0.128 |
| 95% CI | 0.103–0.119 | 0.195–0.211 | 0.382–0.396 | 0.380–0.394 | 0.339–0.353 | 0.120–0.136 | ||
| BMI < 20 kg/m2 | 17,570 | Rs | 0.044 | 0.197 | 0.322 | 0.326 | 0.355 | 0.186 |
| 95% CI | 0.029–0.059 | 0.182–0.211 | 0.308–0.336 | 0.312–0.339 | 0.342–0.369 | 0.171–0.200 | ||
| 20 ≤ BMI < 25 kg/m2 | 33,695 | Rs | 0.082 | 0.241 | 0.426 | 0.430 | 0.463 | 0.215 |
| 95% CI | 0.071–0.092 | 0.230–0.251 | 0.417–0.435 | 0.421–0.439 | 0.454–0.471 | 0.204–0.225 | ||
| 25 ≤ BMI < 30 kg/m2 | 9532 | Rs | −0.065 | 0.116 | 0.386 | 0.369 | 0.382 | 0.192 |
| 95% CI | −0.085–−0.044 | 0.095–0.136 | 0.369–0.404 | 0.351–0.387 | 0.365–0.400 | 0.172–0.211 | ||
| 30 kg/m2 ≤ BMI | 1717 | Rs | −0.139 | 0.002 | 0.296 | 0.266 | 0.278 | 0.132 |
| 95% CI | −0.187–−0.090 | −0.048–0.051 | 0.250–0.340 | 0.220–0.311 | 0.232–0.323 | 0.084–0.181 | ||
| With CAVI | ||||||||
| Total | 62,514 | Rs | 0.034 | 0.149 | 0.332 | 0.305 | 0.217 | 0.197 |
| 95% CI | 0.026–0.042 | 0.141–0.156 | 0.325–0.340 | 0.298–0.312 | 0.209–0.225 | 0.189–0.205 | ||
| BMI < 20 kg/m2 | 17,570 | Rs | 0.001 | 0.193 | 0.291 | 0.287 | 0.263 | 0.221 |
| 95% CI | −0.014–0.016 | 0.179–0.208 | 0.277–0.305 | 0.273–0.301 | 0.249–0.278 | 0.207–0.236 | ||
| 20 ≤ BMI < 25 kg/m2 | 33,695 | Rs | 0.058 | 0.250 | 0.364 | 0.365 | 0.342 | 0.250 |
| 95% CI | 0.047–0.069 | 0.239–0.260 | 0.354–0.373 | 0.356–0.375 | 0.332–0.352 | 0.240–0.261 | ||
| 25 ≤ BMI < 30 kg/m2 | 9532 | Rs | -0.106 | 0.114 | 0.309 | 0.286 | 0.229 | 0.229 |
| 95% CI | −0.127–−0.086 | 0.094–0.135 | 0.290–0.328 | 0.267–0.305 | 0.210–0.249 | 0.209–0.248 | ||
| 30 kg/m2 ≤ BMI | 1717 | Rs | −0.183 | 0.037 | 0.260 | 0.221 | 0.138 | 0.223 |
| 95% CI | −0.230–−0.134 | −0.012–0.086 | 0.213–0.305 | 0.173–0.267 | 0.089–0.186 | 0.175–0.269 | ||
| Index | Cutoff | C-Statistic | 95% CI | p Value |
|---|---|---|---|---|
| BMI (kg/m2) | 21.6 | 0.521 | 0.513–0.530 | <0.001 |
| WC (m) | 0.799 | 0.597 | 0.589–0.605 | <0.001 |
| ABSI | 0.0801 | 0.714 | 0.706–0.721 | <0.001 |
| Conicity index | 1.23 | 0.700 | 0.692–0.707 | <0.001 |
| WHtR | 0.491 | 0.645 | 0.637–0.653 | <0.001 |
| WC/BMI ratio | 0.0362 | 0.627 | 0.619–0.636 | <0.001 |
| Combination of Indices | Rs | 95% CI | p Value |
|---|---|---|---|
| BMI vs. WC | 0.870 | 0.868–0.872 | <0.001 |
| BMI vs. ABSI | 0.063 | 0.054–0.071 | <0.001 |
| BMI vs. Conicity index | 0.440 | 0.433–0.446 | <0.001 |
| BMI vs. WC/BMI ratio | −0.551 | −0.557–−0.545 | <0.001 |
| BMI vs. WHtR | 0.812 | 0.809–0.814 | <0.001 |
| WC vs. ABSI | 0.465 | 0.458–0.471 | <0.001 |
| WC vs. Conicity index | 0.766 | 0.763–0.769 | <0.001 |
| WC vs. WC/BMI | −0.107 | −0.115–−0.099 | <0.001 |
| WC vs. WHtR | 0.893 | 0.892–0.895 | <0.001 |
| ABSI vs. Conicity index | 0.909 | 0.907–0.910 | <0.001 |
| ABSI vs. WC/BMI ratio | 0.674 | 0.669–0.678 | <0.001 |
| ABSI vs. WHtR | 0.553 | 0.547–0.558 | <0.001 |
| Conicity index vs. WC/BMI ratio | 0.372 | 0.365–0.379 | <0.001 |
| Conicity index vs. WHtR | 0.827 | 0.824–0.829 | <0.001 |
| WC/BMI ratio vs. WHtR | −0.166 | −0.174–−0.158 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagayama, D.; Fujishiro, K.; Watanabe, Y.; Yamaguchi, T.; Suzuki, K.; Saiki, A.; Shirai, K. A Body Shape Index (ABSI) as a Variant of Conicity Index Not Affected by the Obesity Paradox: A Cross-Sectional Study Using Arterial Stiffness Parameter. J. Pers. Med. 2022, 12, 2014. https://doi.org/10.3390/jpm12122014
Nagayama D, Fujishiro K, Watanabe Y, Yamaguchi T, Suzuki K, Saiki A, Shirai K. A Body Shape Index (ABSI) as a Variant of Conicity Index Not Affected by the Obesity Paradox: A Cross-Sectional Study Using Arterial Stiffness Parameter. Journal of Personalized Medicine. 2022; 12(12):2014. https://doi.org/10.3390/jpm12122014
Chicago/Turabian StyleNagayama, Daiji, Kentaro Fujishiro, Yasuhiro Watanabe, Takashi Yamaguchi, Kenji Suzuki, Atsuhito Saiki, and Kohji Shirai. 2022. "A Body Shape Index (ABSI) as a Variant of Conicity Index Not Affected by the Obesity Paradox: A Cross-Sectional Study Using Arterial Stiffness Parameter" Journal of Personalized Medicine 12, no. 12: 2014. https://doi.org/10.3390/jpm12122014