
Cross-Cultural Validation of the Short Version of the Questionnaire of Olfactory Disorders—Negative Statements into Italian: Towards Personalized Patient Care
 , , , , , , ,
, , , , , , , 
Abstract
:1. Introduction
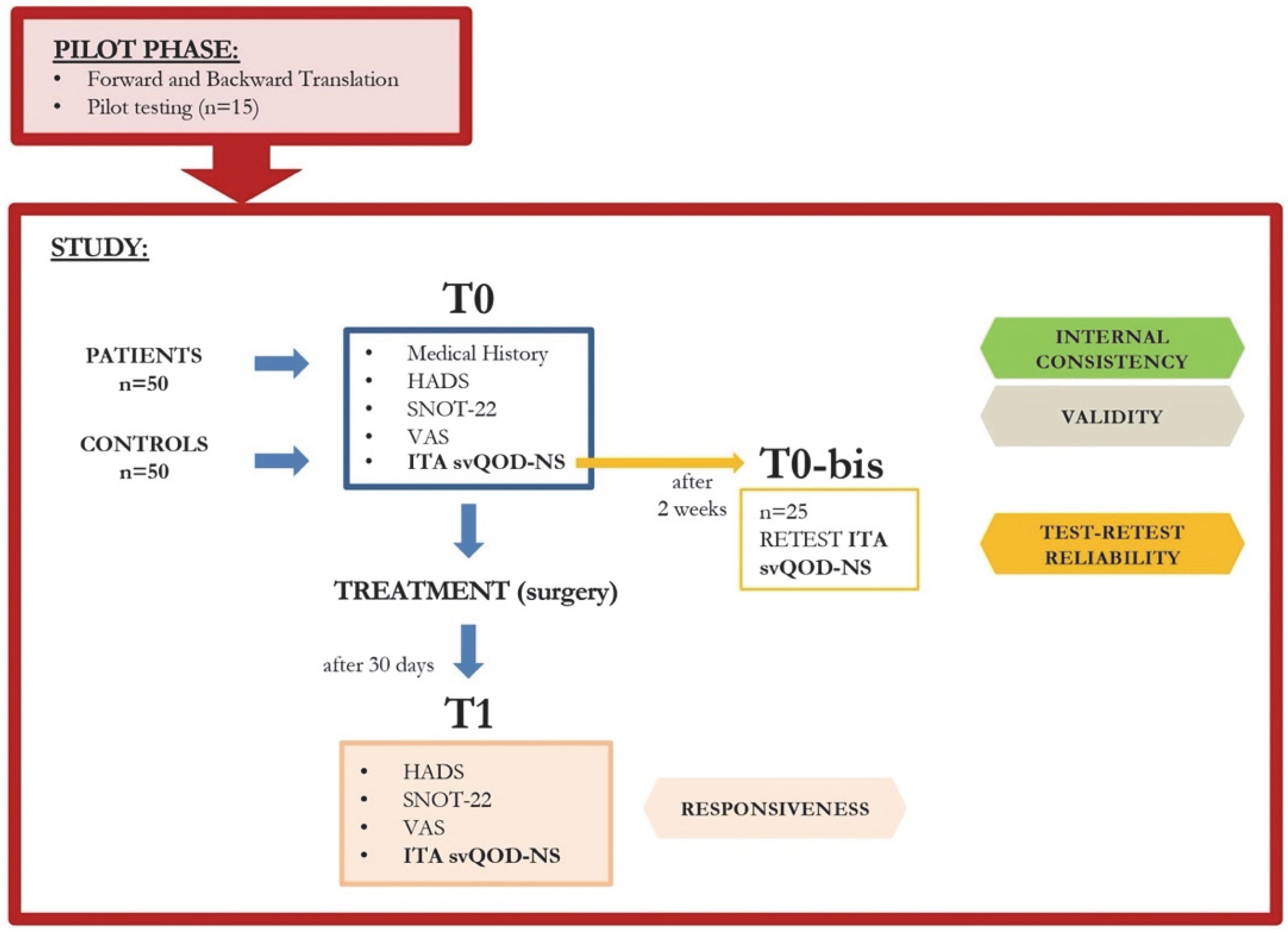
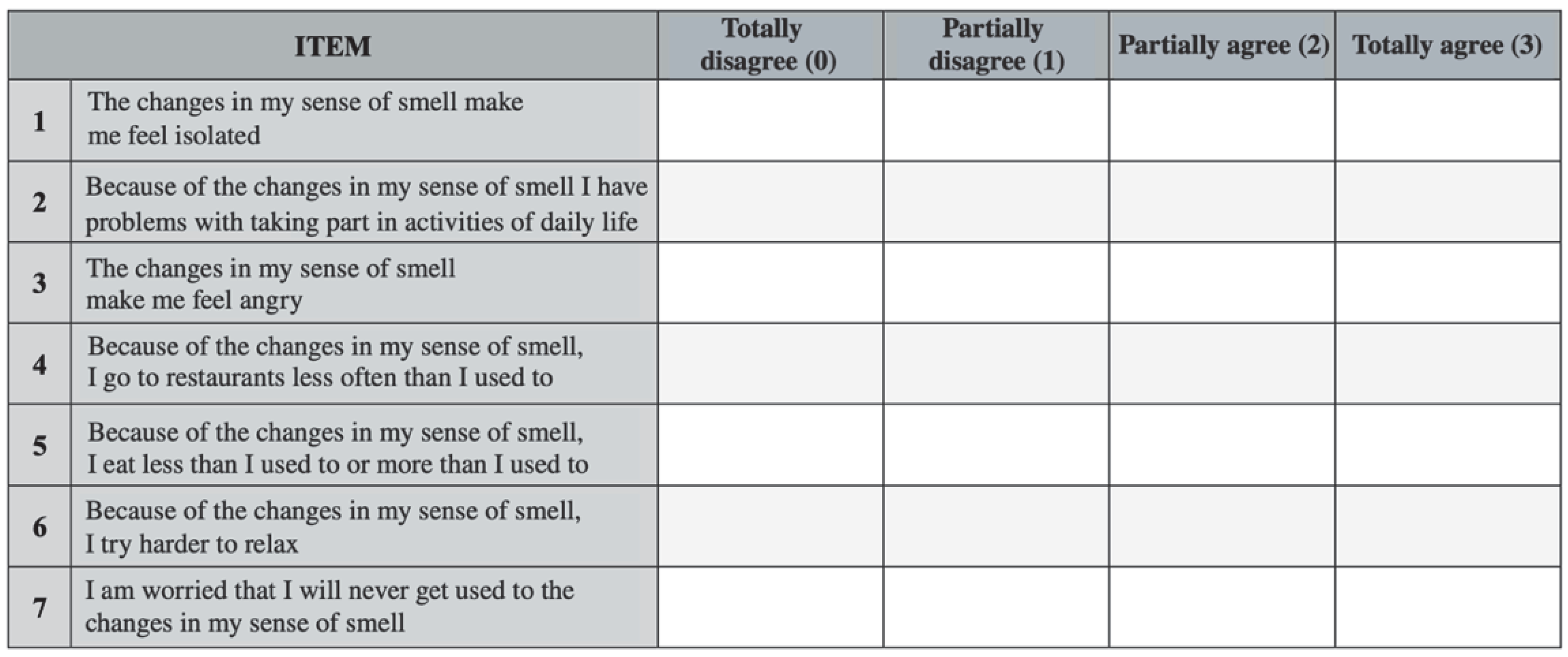
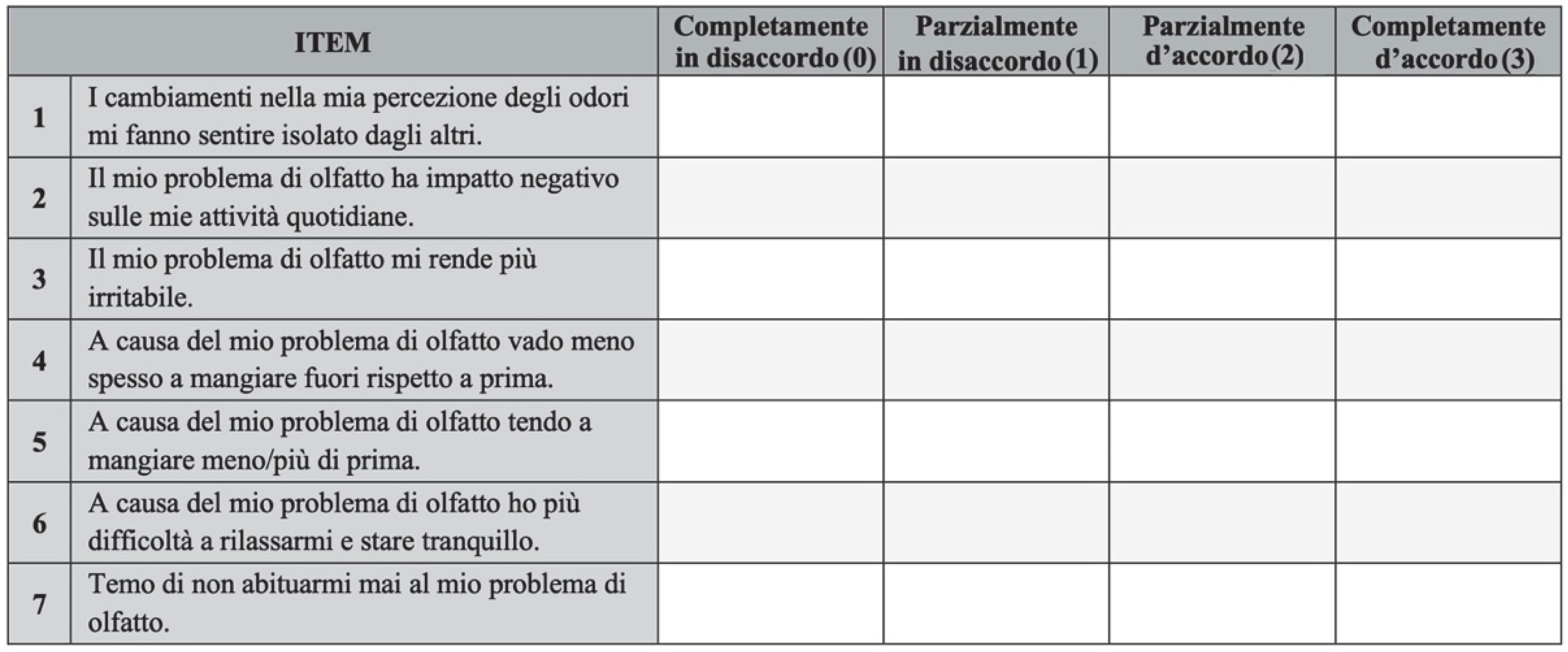
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Damm, M.; Temmel, A.; Welge-Lüssen, A.; Eckel, H.E.; Kreft, M.-P.; Klussmann, J.P.; Gudziol, H.; Hüttenbrink, K.-B.; Hummel, T. Olfactory dysfunctions. Epidemiology and therapy in Germany, Austria and Switzerland. HNO 2004, 52, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Mott, A.E.; Leopold, D.A. Disorders in Taste and Smell. Med. Clin. N. Am. 1991, 75, 1321–1353. [Google Scholar] [CrossRef] [PubMed]
- Cullen, M.M.; Leopold, D.A. Disorders of Smell and Taste. Med. Clin. N. Am. 1999, 83, 57–74. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C.H.; Shephard, B.C.; E Daniel, S. Olfactory dysfunction in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1997, 62, 436–446. [Google Scholar] [CrossRef] [Green Version]
- Úbeda-Bañón, I.; Saiz-Sanchez, D.; Flores-Cuadrado, A.; Rioja-Corroto, E.; Gonzalez-Rodriguez, M.; Villar-Conde, S.; Astillero-Lopez, V.; Cabello-De La Rosa, J.P.; Gallardo-Alcañiz, M.J.; Vaamonde-Gamo, J.; et al. The human olfactory system in two proteinopathies: Alzheimer’s and Parkinson’s diseases. Transl. Neurodegener. 2020, 9, 22. [Google Scholar] [CrossRef]
- Mercante, G.; Ferreli, F.; de Virgilio, A.; Gaino, F.; di Bari, M.; Colombo, G.; Russo, E.; Costantino, A.; Pirola, F.; Cugini, G. Prevalence of Taste and Smell Dysfunction in Coronavirus Disease 2019. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 723–728. [Google Scholar] [CrossRef]
- Whitcroft, K.L.; Hummel, T. Olfactory Dysfunction in COVID-19: Diagnosis and Management. JAMA 2020, 323, 2512. [Google Scholar] [CrossRef]
- Sedaghat, A.R.; Gengler, I.; Speth, M.M. Olfactory Dysfunction: A Highly Prevalent Symptom of COVID-19 with Public Health Significance. Otolaryngol. Neck Surg. 2020, 163, 12–15. [Google Scholar] [CrossRef]
- D’Ascanio, L.; Pandolfini, M.; Cingolani, C.; Latini, G.; Gradoni, P.; Capalbo, M.; Frausini, G.; Maranzano, M.; Brenner, M.J.; Di Stadio, A. Olfactory Dysfunction in COVID-19 Patients: Prevalence and Prognosis for Recovering Sense of Smell. Otolaryngol. Neck Surg. 2020, 164, 82–86. [Google Scholar] [CrossRef]
- Baiardini, I.; Paoletti, G.; Mariani, A.; Malvezzi, L.; Pirola, F.; Spriano, G.; Mercante, G.; Puggioni, F.; Racca, F.; Melone, G.; et al. Nasal Polyposis Quality of Life (NPQ): Development and Validation of the First Specific Quality of Life Questionnaire for Chronic Rhinosinusitis with Nasal Polyps. Healthcare 2022, 10, 253. [Google Scholar] [CrossRef]
- Philpott, C.; Boak, D. The Impact of Olfactory Disorders in the United Kingdom. Chem. Senses 2014, 39, 711–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Corso, E.; Bilò, M.B.; Matucci, A.; Seccia, V.; Braido, F.; Gelardi, M.; Heffler, E.; Latorre, M.; Malvezzi, L.; Pelaia, G.; et al. Personalized Management of Patients with Chronic Rhinosinusitis with Nasal Polyps in Clinical Practice: A Multidisciplinary Consensus Statement. J. Pers. Med. 2022, 12, 846. [Google Scholar] [CrossRef] [PubMed]
- Seccia, V.; D’Amato, M.; Scioscia, G.; Bagnasco, D.; Di Marco, F.; Fadda, G.; Menzella, F.; Pasquini, E.; Pelaia, G.; Tremante, E.; et al. Management of Patients with Severe Asthma and Chronic Rhinosinusitis with Nasal Polyps: A Multidisciplinary Shared Approach. J. Pers. Med. 2022, 12, 1096. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.; Asero, R.; Bagnasco, D.; Blasi, F.; Bonini, M.; Bussi, M.; Canevari, R.F.; Canonica, G.W.; Castelnuovo, P.; Cecchi, L.; et al. ARIA-ITALY multidisciplinary consensus on nasal polyposis and biological treatments. World Allergy Organ. J. 2021, 14, 100592. [Google Scholar] [CrossRef]
- Qu, S.; Wei, J.; Wang, Q.; Li, Y.; Jin, X.; Chaib, L. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin. Otolaryngol. 2009, 34, 447–454. [Google Scholar] [CrossRef]
- Kim, B.G.; Oh, J.-H.; Na Choi, H.; Park, S.Y. Simple assessment of olfaction in patients with chronic rhinosinusitis. Acta Oto-Laryngol. 2015, 135, 258–263. [Google Scholar] [CrossRef]
- Frasnelli, J.; Hummel, T. Olfactory dysfunction and daily life. Eur. Arch. Otorhinolaryngol. 2004, 262, 231–235. [Google Scholar] [CrossRef]
- Mattos, J.L.; Schlosser, R.J.; DeConde, A.S.; Hyer, M.; Mace, J.C.; Smith, T.L.; Soler, Z.M. Factor analysis of the questionnaire of olfactory disorders in patients with chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2018, 8, 777–782. [Google Scholar] [CrossRef]
- Guillemin, F.; Bombardier, C.; Beaton, D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J. Clin. Epidemiol. 1993, 46, 1417–1432. [Google Scholar] [CrossRef]
- Iavarone, A.; The Working Group; Mazzi, M.C.; Russo, G.; D’Anna, F.; Peluso, S.; Mazzeo, P.; De Luca, V.; De Michele, G.; Iaccarino, G.; et al. The Italian version of the quick mild cognitive impairment (Qmci-I) screen: Normative study on 307 healthy subjects. Aging Clin. Exp. Res. 2018, 31, 353–360. [Google Scholar] [CrossRef]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Puxeddu, I.; Petrelli, F.; Cristofani-Mencacci, L.; Scarano, M.; Latorre, M.; De Rosa, A.; Dallan, I.; Manca, M.L.; Berrettini, S.; Migliorini, P.; et al. Component-Resolved Diagnosis for Endotyping Patients with Chronic Rhinosinusitis with Nasal Polyps. Int. Arch. Allergy Immunol. 2022, 183, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Mattos, J.L.; Ba, C.E.; Schlosser, R.J.; Hyer, M.; Mace, J.C.; Smith, T.L.; Soler, Z.M. A brief version of the questionnaire of olfactory disorders in patients with chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2019, 9, 1144–1150. [Google Scholar] [CrossRef] [PubMed]
- Chiesa-Estomba, C.M.; Lechien, J.R.; Calvo-Henríquez, C.; Mayo, M.; Maldonado, B.; Maza, J.; Tucciarone, M.; Villareal, I.; Vaira, L.A.; Izquierdo-Dominguez, A.; et al. Translation and validation of the short version of the Questionnaire of Olfactory Disorders–Negative Statements to Spanish. Am. J. Otolaryngol. 2020, 42, 102775. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, C.; Chiesa-Estomba, C.M.; Horoi, M.; Le Bon, S.D.; Hans, S.; Distinguin, L.; Chekkoury-Idrissi, Y.; Circiu, M.P.; Khalife, M.; Saussez, S.; et al. Validity and reliability of the french short version of the questionnaire of olfactory disorders-negative statements (sQOD-NS). Ear Nose Throat J. 2021. [Google Scholar] [CrossRef]
- Alobid, I.; Benitez, P.; Bernal-Sprekelsen, M.; Roca, J.; Alonso, J.; Picado, C.; Mullol, J. Nasal polyposis and its impact on quality of life: Comparison between the effects of medical and surgical treatments. Allergy 2005, 60, 452–458. [Google Scholar] [CrossRef]
- Brämerson, A.; Nordin, S.; Bende, M. Clinical experience with patients with olfactory complaints, and their quality of life. Acta Oto-Laryngol. 2007, 127, 167–174. [Google Scholar] [CrossRef]
- Chung, J.H.; Lee, Y.J.; Kang, T.W.; Kim, K.R.; Jang, D.P.; Kim, I.Y.; Cho, S.H. Altered Quality of Life and Psychological Health (SCL-90-R) in Patients with Chronic Rhinosinusitis with Nasal Polyps. Ann. Otol. Rhinol. Laryngol. 2015, 124, 663–670. [Google Scholar] [CrossRef]
- Valsamidis, K.; Printza, A.; Titelis, K.; Constantinidis, J.; Triaridis, S. Olfaction and quality of life in patients with nasal septal deviation treated with septoplasty. Am. J. Otolaryngol. 2019, 40, 747–754. [Google Scholar] [CrossRef]
- Akay, H.G.; Muluk, N.B.; Inal, M.; Simsek, G.; Kiliç, R. Evaluation of Olfactory Sensation, Acoustic Rhinometry, and Quality of Life of the Patients with Nasal Septal Deviation. J. Craniofacial Surg. 2019, 30, 1221–1227. [Google Scholar] [CrossRef]
- Haytoğlu, S.; Dengiz, R.; Muluk, N.B.; Kuran, G.; Arikan, O.K. Effects of Septoplasty on Olfactory Function Evaluated by the Brief Smell Identification Test: A Study of 116 Patients. Ear Nose Throat J. 2017, 96, 433–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Philpott, C.M.; Wolstenholme, C.R.; Goodenough, P.C.; Clark, A.; Murty, G.E. Comparison of Subjective Perception with Objective Measurement of Olfaction. Otolaryngol. Neck Surg. 2006, 134, 488–490. [Google Scholar] [CrossRef] [PubMed]
- Coelho, D.H.; Reiter, E.R.; Budd, S.G.; Shin, Y.; Kons, Z.A.; Costanzo, R.M. Quality of life and safety impact of COVID-19 asso-ciated smell and taste disturbances. Am. J. Otolaryngol. 2021, 42, 103001. [Google Scholar] [CrossRef] [PubMed]
- Palmquist, E.; Larsson, M.; Olofsson, J.K.; Seubert, J.; Bäckman, L.; Laukka, E.J. A Prospective Study on Risk Factors for Olfactory Dysfunction in Aging. J. Gerontol. A Biol. Sci. Med. Sci. 2019, 75, 603–610. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cases | Controls | ||
|---|---|---|---|
| Gender | females (%) | 21 (42) | 26 (52) |
| males (%) | 29 (58) | 24 (48) | |
| Age | mean ± sd | 44.1 ± 13.9 | 43.0 ± 15.1 |
| Disease | CRSwNP (%) | 25 (50) | / |
| septal deviation (%) | 25 (50) | / | |
| NPS | mean ± sd | 4.7 ± 2.3 | / |
| Comorbidities | asthma (%) | 13 (26) | 4 (8) |
| allergy (%) | 22 (44) | 6 (12) | |
| Smoking | yes (%) | 10 (20) | 12 (24) |
| no (%) | 40 (80) | 38 (76) |
| Timepoint | |||
|---|---|---|---|
| Questionnaire | T0 (±sd) | T1 (±sd) | T2 (±sd) |
| ITA svQOD-NS | 8.58 ± 5.70 | 2.33 ± 3.11 | 1.49 ± 1.72 |
| SNOT-22 | 46.46 ± 19.11 | 19.42 ± 12.63 | 10.88 ± 8.12 |
| VAS | 6.10 ± 3.10 | 2.02 ± 2.56 | 0.98 ± 1.12 |
| HADS | 9.32 ± 6.92 | 6.02 ± 6.29 | 3.86 ± 3.31 |
| ITEM of the ITA svQOD-NS | Item-to-Total Correlation | Cronbach’s α if Item Deleted |
|---|---|---|
| item#1 | 0.646 | 0.922 |
| item#2 | 0.780 | 0.909 |
| item#3 | 0.789 | 0.908 |
| item#4 | 0.767 | 0.911 |
| item#5 | 0.744 | 0.913 |
| item#6 | 0.850 | 0.902 |
| item#7 | 0.757 | 0.913 |
| ITA svQOD-NS | Cases + Controls | CRSwNP | Septal Deviation | Healthy Controls |
|---|---|---|---|---|
| item#1 | 0.96 ± 1.05 | 1.45 ± 1.06 | 0.43 ± 0.34 | 0.04 ± 0.03 |
| item#2 | 1.61 ± 1.11 | 2.18 ± 0.80 | 0.97 ± 0.76 | 0.06 ± 0.04 |
| item#3 | 1.43 ± 1.17 | 2.00 ± 0.99 | 0.83 ± 0.73 | 0.08 ± 0.05 |
| item#4 | 0.70 ± 1.00 | 1.18 ± 1.14 | 0.19 ± 0.14 | 0.02 ± 0.02 |
| item#5 | 0.86 ± 1.08 | 1.34 ± 1.10 | 0.35 ± 0.29 | 0.02 ± 0.01 |
| item#6 | 1.39 ± 1.16 | 1.92 ± 1.00 | 0.81 ± 0.67 | 0.06 ± 0.04 |
| item#7 | 1.54 ± 1.13 | 2.16 ± 0.92 | 0.95 ± 0.81 | 0.08 ± 0.05 |
| TOTAL | 4.47 ± 5.80 | 12.23 ± 5.31 | 4.53 ± 4.34 | 0.37 ± 0.32 |
| ITA svQOD-NS | Score Difference | 95%CI | p Value | |
|---|---|---|---|---|
| in CRSwNP | vs. SD | +7.7 | 3.82–8.75 | <0.001 |
| vs. Controls | +11.86 | 9.26–13.62 | <0.001 | |
| in SD | vs. Controls | +4.16 | 3.06–7.34 | <0.001 |
| Questionnaire | Difference of the Means (±sd) | 95%CI | p Value |
|---|---|---|---|
| ITA svQOD-NS | |||
| T0 vs. T1 | 6.14 ± 5.28 | 4.64–7.64 | <0.001 |
| T1 vs. T2 | 0.84 ± 1.41 | 0.44–1.24 | <0.001 |
| T0 vs. T2 | 6.98 ± 5.27 | 5.48–8.48 | <0.001 |
| SNOT-22 | |||
| T0 vs. T1 | 27.04 ± 17.90 | 21.95–32.12 | <0.001 |
| T1 vs. T2 | 8.54 ± 7.73 | 6.34–10.74 | <0.001 |
| T0 vs. T2 | 35.58 ± 18.58 | 30.30–40.86 | <0.001 |
| VAS | |||
| T0 vs. T1 | 4.08 ± 3.15 | 3.19–4.97 | <0.001 |
| T1 vs. T2 | 1.04 ± 1.47 | 0.62–1.46 | <0.001 |
| T0 vs. T2 | 5.12 ± 2.90 | 4.29–5.95 | <0.001 |
| HADS | |||
| T0 vs. T1 | 3.30 ± 5.40 | 1.77–4.83 | <0.001 |
| T1 vs. T2 | 2.16 ± 2.35 | 1.49–2.83 | <0.001 |
| T0 vs. T2 | 5.46 ± 5.20 | 3.98–6.94 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirola, F.; Giombi, F.; Ferreli, F.; Costantino, A.; Mercante, G.; Paoletti, G.; Heffler, E.; Canonica, G.W.; Settimi, S.; De Corso, E.; et al. Cross-Cultural Validation of the Short Version of the Questionnaire of Olfactory Disorders—Negative Statements into Italian: Towards Personalized Patient Care. J. Pers. Med. 2022, 12, 2010. https://doi.org/10.3390/jpm12122010
Pirola F, Giombi F, Ferreli F, Costantino A, Mercante G, Paoletti G, Heffler E, Canonica GW, Settimi S, De Corso E, et al. Cross-Cultural Validation of the Short Version of the Questionnaire of Olfactory Disorders—Negative Statements into Italian: Towards Personalized Patient Care. Journal of Personalized Medicine. 2022; 12(12):2010. https://doi.org/10.3390/jpm12122010
Chicago/Turabian StylePirola, Francesca, Francesco Giombi, Fabio Ferreli, Andrea Costantino, Giuseppe Mercante, Giovanni Paoletti, Enrico Heffler, Giorgio Walter Canonica, Stefano Settimi, Eugenio De Corso, and et al. 2022. "Cross-Cultural Validation of the Short Version of the Questionnaire of Olfactory Disorders—Negative Statements into Italian: Towards Personalized Patient Care" Journal of Personalized Medicine 12, no. 12: 2010. https://doi.org/10.3390/jpm12122010