
Direct-Acting Antivirals and the Risk of Hepatitis B Reactivation in Hepatitis B and C Co-Infected Patients: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Included Studies
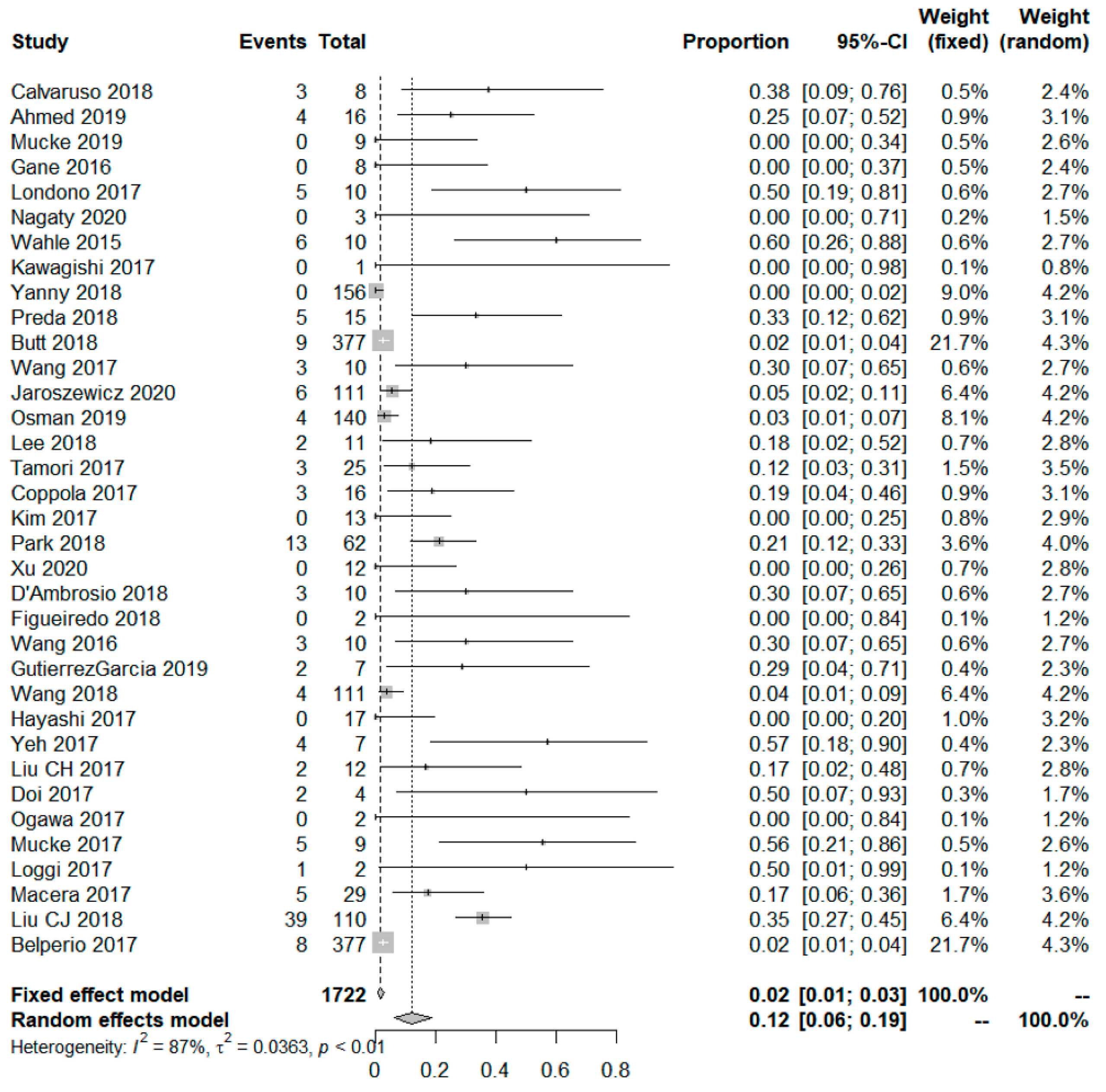
3.2. DAA-Associated HBV Reactivation in HBsAg (+) Patients
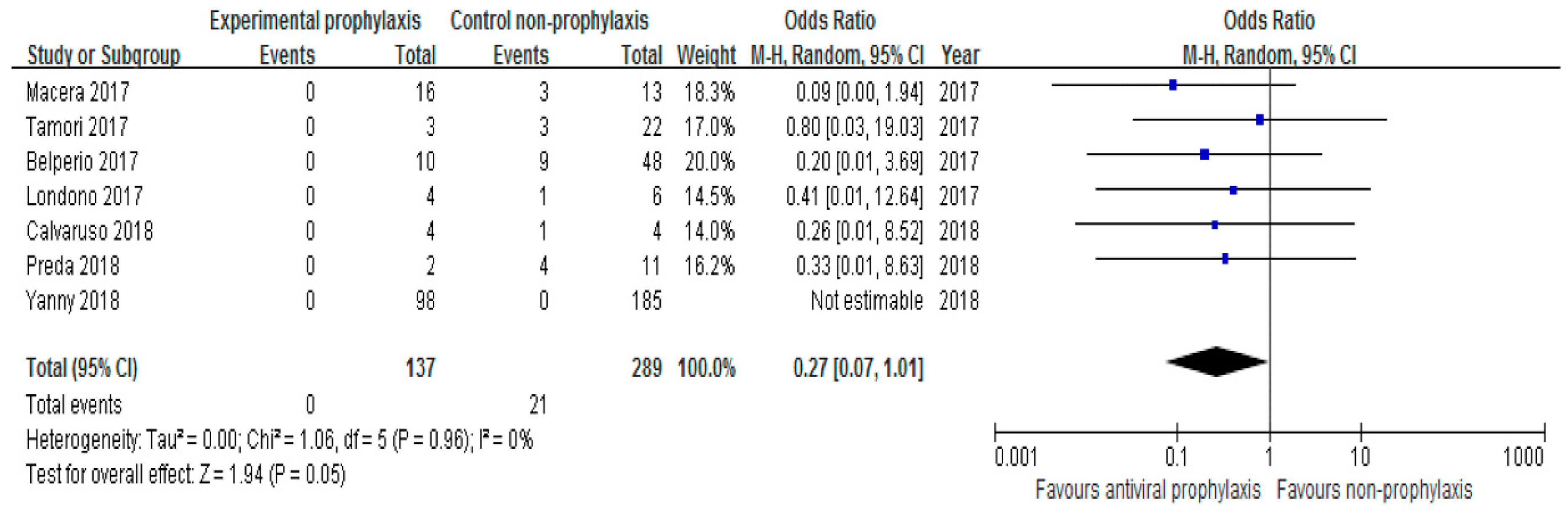
3.3. Subgroup Analysis
3.4. DAA-Associated HBV Reactivation in Resolved HBV Patients
3.5. Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stanaway, J.D.; Flaxman, A.D.; Naghavi, M.; Fitzmaurice, C.; Vos, T.; Abubakar, I.; Abu-Raddad, L.J.; Assadi, R.; Bhala, N.; Cowie, B.; et al. The global burden of viral hepatitis from 1990 to 2013: Findings from the Global Burden of Disease Study 2013. Lancet 2016, 388, 1081–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korean Association for the Study of the Liver (KASL). KASL clinical practice guidelines for management of chronic hepatitis B. Clin. Mol. Hepatol. 2019, 25, 93–159. [Google Scholar] [CrossRef] [Green Version]
- Donato, F.; Boffetta, P.; Puoti, M. A meta-analysis of epidemiological studies on the combined effect of hepatitis B and C virus infections in causing hepatocellular carcinoma. Int. J. Cancer 1998, 75, 347–354. [Google Scholar] [CrossRef]
- Bellecave, P.; Gouttenoire, J.; Gajer, M.; Brass, V.; Koutsoudakis, G.; Blum, H.E.; Bartenschlager, R.; Nassal, M.; Moradpour, D. Hepatitis B and C virus coinfection: A novel model system reveals the absence of direct viral interference. Hepatology 2009, 50, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.J.; Lee, S.D. Hepatitis B virus/hepatitis C virus coinfection: Epidemiology, clinical features, viral interactions and treatment. J. Gastroenterol. Hepatol. 2008, 23, 512–520. [Google Scholar] [CrossRef]
- Bini, E.J.; Perumalswami, P.V. Hepatitis B virus infection among American patients with chronic hepatitis C virus infection: Prevalence, racial/ethnic differences, and viral interactions. Hepatology 2010, 51, 759–766. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL). EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, M.L.; Huang, C.F.; Huang, C.I.; Holmes, J.A.; Hsieh, M.H.; Tsai, Y.S.; Liang, P.C.; Tsai, P.C.; Hsieh, M.Y.; Lin, Z.Y.; et al. Hepatitis B-related outcomes following direct-acting antiviral therapy in Taiwanese patients with chronic HBV/HCV co-infection. J. Hepatol. 2020, 73, 62–71. [Google Scholar] [CrossRef] [Green Version]
- Bersoff-Matcha, S.J.; Cao, K.; Jason, M.; Ajao, A.; Jones, S.C.; Meyer, T.; Brinker, A. Hepatitis B Virus Reactivation Associated with Direct-Acting Antiviral Therapy for Chronic Hepatitis C Virus: A Review of Cases Reported to the U.S. Food and Drug Administration Adverse Event Reporting System. Ann. Intern. Med. 2017, 166, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wang, C.; Chen, J.; Ji, D.; Wang, Y.; Wu, V.; Karlberg, J.; Lau, G. Hepatitis B reactivation in hepatitis B and C coinfected patients treated with antiviral agents: A systematic review and meta-analysis. Hepatology 2017, 66, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.N.; Liu, C.J.; Chen, C.Y.; Tseng, K.C.; Lo, C.C.; Peng, C.Y.; Lin, C.L.; Chiu, H.C.; Chiu, Y.C.; Chen, P.J. Entecavir Prevents HBV Reactivation During Direct Acting Antivirals for HCV/HBV Dual Infection: A Randomized Trial. Clin. Gastroenterol. Hepatol. 2021, 166, 792–798. [Google Scholar] [CrossRef]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [Green Version]
- Reddy, K.R.; Beavers, K.L.; Hammond, S.P.; Lim, J.K.; Falck-Ytter, Y.T. American Gastroenterological Association Institute guideline on the prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology 2015, 148, 215–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahle, R.C.; de Mello Perez, R.; Takemi Emori, C.; de Oliveira Uehara, S.N.; da Silva Fucuta, P.; Melo Rocha, C.; de Castro Amaral Feldner, A.C.; de Souza, E.S.I.S.; Carvalho-Filho, R.J.; Silva, A.E.; et al. Does hepatitis B virus coinfection have any impact on treatment outcome in hepatitis C patients on hemodialysis? Ann. Hepatol. 2015, 14, 317–324. [Google Scholar] [CrossRef]
- Gane, E.J.; Hyland, R.H.; An, D.; Svarovskaia, E.S.; Brainard, D.; McHutchison, J.G. Ledipasvir and sofosbuvir for HCV infection in patients coinfected with HBV. Antivir. Ther. 2016, 21, 605–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abstracts of the 25th Annual Conference of APASL, February 20–24, 2016, Tokyo, Japan. Hepatol. Int. 2016, 10 (Suppl. 1), 1–506. [CrossRef] [PubMed]
- Sulkowski, M.S.; Chuang, W.L.; Kao, J.H.; Yang, J.C.; Gao, B.; Brainard, D.M.; Han, K.H.; Gane, E. No Evidence of Reactivation of Hepatitis B Virus among Patients Treated with Ledipasvir-Sofosbuvir for Hepatitis C Virus Infection. Clin. Infect. Dis 2016, 63, 1202–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.-h.; Choe, W.H. S-148 HBV reactivation in a HBV/HCV-coinfected patient after daclatasvir and asunaprevir treatment. Korean Assoc. Intern. Med. Fall Conf. 2016, 2016, 123. [Google Scholar]
- Londoño, M.C.; Lens, S.; Mariño, Z.; Bonacci, M.; Ariza, X.; Broquetas, T.; Pla, A.; Bartres, C.; Adriani, M.V.; Rodríguez-Tajes, S.; et al. Hepatitis B reactivation in patients with chronic hepatitis C undergoing anti-viral therapy with an interferon-free regimen. Aliment. Pharm. 2017, 45, 1156–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawagishi, N.; Suda, G.; Onozawa, M.; Kimura, M.; Maehara, O.; Ohara, M.; Izumi, T.; Umemura, M.; Ito, J.; Nakai, M.; et al. Comparing the risk of hepatitis B virus reactivation between direct-acting antiviral therapies and interferon-based therapies for hepatitis C. J. Viral Hepat. 2017, 24, 1098–1106. [Google Scholar] [CrossRef]
- Wang, C.; Ji, D.; Chen, J.; Shao, Q.; Li, B.; Liu, J.; Wu, V.; Wong, A.; Wang, Y.; Zhang, X.; et al. Hepatitis due to Reactivation of Hepatitis B Virus in Endemic Areas among Patients with Hepatitis C Treated with Direct-acting Antiviral Agents. Clin. Gastroenterol. Hepatol. 2017, 15, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Tamori, A.; Abiru, S.; Enomoto, H.; Kioka, K.; Korenaga, M.; Tani, J.; Enomoto, M.; Sugiyama, M.; Masaki, T.; Kawada, N.; et al. Low incidence of hepatitis B virus reactivation and subsequent hepatitis in patients with chronic hepatitis C receiving direct-acting antiviral therapy. J. Viral Hepat. 2018, 25, 608–611. [Google Scholar] [CrossRef] [PubMed]
- Coppola, N.; Stanzione, M.; Messina, V.; D’Adamo, G.; Sangiovanni, V.; Fontanella, L.; De Pascalis, S.; Stornaiuolo, G.; Macera, M.; Piai, G. DAA-based regimens in HBsAg/anti-HCV positive patients: The need to control HBV replication to avoid HBV reactivation. J. Hepatol. 2017, 1, S727. [Google Scholar] [CrossRef]
- Ancha, A.; Modi, A.A. Risk of HBV Reactivation with DAA Therapy for HCV in those with evidence of Past HBV Exposure. Hepatology 2017, 66, 620A. [Google Scholar]
- Hayashi, K.; Ishigami, M.; Ishizu, Y.; Kuzuya, T.; Honda, T.; Hirooka, Y.; Goto, H. The impact of hepatitis B virus infection on sustained virologic response and HBV reactivation in patients with chronic hepatitis C who treated by all-oral direct-acting antivirals regimens. Gastroenterology 2017, 152, S1092–S1093. [Google Scholar] [CrossRef]
- Yeh, M.L.; Huang, C.F.; Hsieh, M.H.; Ko, Y.M.; Chen, K.Y.; Liu, T.W.; Lin, Y.H.; Liang, P.C.; Hsieh, M.Y.; Lin, Z.Y. Reactivation of hepatitis B in patients of chronic hepatitis C with hepatitis B virus infection treated with direct acting antivirals. J. Gastroenterol. Hepatol. 2017, 32, 1754–1762. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.H.; Liu, C.J.; Su, T.H.; Fang, Y.J.; Yang, H.C.; Chen, P.J.; Chen, D.S.; Kao, J.H. Hepatitis B Virus Reactivation in Patients Receiving Interferon-Free Direct-Acting Antiviral Agents for Chronic Hepatitis C Virus Infection. Open Forum Infect. Dis. 2017, 4, ofx028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doi, A.; Sakamori, R.; Tahata, Y.; Urabe, A.; Morishita, N.; Yamada, R.; Furuta, K.; Kodama, T.; Hikita, H.; Yakushijin, T. Frequency of, and factors associated with, hepatitis B virus reactivation in hepatitis C patients treated with all-oral direct-acting antivirals: Analysis of a Japanese prospective cohort. Hepatol. Res. 2017, 47, 1438–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogawa, E.; Furusyo, N.; Murata, M.; Toyoda, K.; Hayashi, T.; Ura, K. Potential risk of HBV reactivation in patients with resolved HBV infection undergoing direct-acting antiviral treatment for HCV. Liver Int. 2018, 38, 76–83. [Google Scholar] [CrossRef]
- Mücke, V.; Mücke, M.; Peiffer, K.H.; Weiler, N.; Welzel, T.; Sarrazin, C.; Zeuzem, S.; Berger, A.; Vermehren, J. No evidence of hepatitis B virus reactivation in patients with resolved infection treated with direct-acting antivirals for hepatitis C in a large real-world cohort. Aliment. Pharmacol. Ther. 2017, 46, 432–439. [Google Scholar] [CrossRef]
- Loggi, E.; Gitto, S.; Galli, S.; Minichiello, M.; Conti, F.; Grandini, E.; Scuteri, A.; Vitale, G.; Di Donato, R.; Cursaro, C. Hepatitis B virus reactivation among hepatitis C patients treated with direct-acting antiviral therapies in routine clinical practice. J. Clin. Virol. 2017, 93, 66–70. [Google Scholar] [CrossRef] [PubMed]
- Macera, M.; Stanzione, M.; Messina, V.; D’Adamo, G.; Sangiovanni, V.; Mioglioresi, L.; Fontanella, L.; De Pascalis, S.; Stornaiuolo, G.; Lanza, A.G. Interferon-free regimens in hepatitis B surface antigen/anti–hepatitis C virus positive patients: The need to control hepatitis B virus replication to avoid hepatitis B virus reactivation. Clin. Gastroenterol. Hepatol. 2017, 15, 1800–1802. [Google Scholar] [CrossRef] [PubMed]
- Belperio, P.S.; Shahoumian, T.A.; Mole, L.A.; Backus, L.I. Evaluation of hepatitis B reactivation among 62,920 veterans treated with oral hepatitis C antivirals. Hepatology 2017, 66, 27–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Tolaymat, M.; Stonesifer, E.; Kottilil, S.; Wilson, E. Absence of hepatitis B reactivation among veterans with serological evidence of previous hepatitis B infection receiving anti-hepatitis C direct acting antivirals. J. Hepatol. 2017, 1, S251–S252. [Google Scholar] [CrossRef]
- Calvaruso, V.; Ferraro, D.; Licata, A.; Bavetta, M.G.; Petta, S.; Bronte, F.; Colomba, G.; Craxì, A.; Di Marco, V. HBV reactivation in patients with HCV/HBV cirrhosis on treatment with direct-acting antivirals. J. Viral Hepat. 2018, 25, 72–79. [Google Scholar] [CrossRef]
- Yanny, B.; Sahota, A. Reactivation of hepatitis B virus among patients treated with ledipasvir-sofosbuvir (LDV/SOF) for hepatitis C virus infection in a community based setting. Gastroenterology 2017, 152, S1059. [Google Scholar] [CrossRef]
- Preda, C.; Popescu, C.; Baicus, C.; Constantinescu, I.; Oproiu, A.; Voiosu, T.; Diculescu, M.; Negreanu, L.; Gheorghe, L.; Sporea, I. Risk of hepatitis B virus reactivation in hepatitis B virus+ hepatitis C virus-co-infected patients with compensated liver cirrhosis treated with ombitasvir, paritaprevir/r+ dasabuvir+ ribavirin. J. Viral Hepat. 2018, 25, 834–841. [Google Scholar] [CrossRef]
- Butt, A.A.; Yan, P.; Shaikh, O.S.; Abou-Samra, A.B. Hepatitis B reactivation and outcomes in persons treated with directly acting antiviral agents against hepatitis C virus: Results from ERCHIVES. Aliment. Pharmacol. Ther. 2018, 47, 412–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.W.; Lee, T.Y.; Yang, S.S.; Peng, Y.C.; Yeh, H.Z.; Chang, C.S. Prevalence of Hepatitis B Reactivation among Chinese Individuals with Chronic Hepatitis C Treated with Pan-Oral Direct-Acting Antivirals. Gastroenterol. Res. 2018, 11, 124–129. [Google Scholar] [CrossRef] [Green Version]
- Woo, H.Y.; Park, Y.J.; Heo, J. The Risk of HBV Reactivation among HBV/HCV Co-Infected Patients Treated with Direct-Acting Antiviral Agents: A Single Center Experience; EASL: Geneva, Switzerland, 2019. [Google Scholar]
- D’Ambrosio, R.; Degasperi, E.; Aghemo, A.; Borghi, M.; Perbellini, R.; De Nicola, S.; Lunghi, G.; Lampertico, P. Risk and outcome of hepatitis B virus (HBV) reactivation during chronic hepatitis C treatment with direct-acting antivirals (DAAs) in patients with HCV-related advanced fibrosis: A single-center experience. Dig. Liver Dis. 2018, 50, 41. [Google Scholar] [CrossRef]
- Figueiredo, L.; Alexandrino, G.; Costa, M.; Carvalho, R.; Alberto, S.; Martins, A. Reactivation of Hepatitis B Virus Infection during Treatment of Hepatitis C with Direct-Acting Antivirals; United European Gastroenterology: Vienna, Austria, 2018. [Google Scholar]
- Liu, C.-J.; Chuang, W.-L.; Sheen, I.-S.; Wang, H.-Y.; Chen, C.-Y.; Tseng, K.-C.; Chang, T.-T.; Massetto, B.; Yang, J.C.; Yun, C. Efficacy of ledipasvir and sofosbuvir treatment of HCV infection in patients coinfected with HBV. Gastroenterology 2018, 154, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, A.; Elantouny, N.; Zidan, A.; Sadek, A.; Elrasad, M. Effect of treatment of hepatitis C by directly acting antivirals on chronic hepatitis C and B co-infected patients. Sci. Rep. 2018, 8, 1661. [Google Scholar] [CrossRef]
- Mücke, M.M.; Mücke, V.T.; Peiffer, K.H.; Sarrazin, C.; Zeuzem, S.; Berger, A.; Vermehren, J. Absence of HBV Reactivation in Patients with Resolved HBV Infection Following DAA Therapy for Hepatitis C: A 1-Year Follow-up Study. Open Forum Infect. Dis. 2019, 6, ofy340. [Google Scholar] [CrossRef]
- Osman, H.A.; Ghweil, A.A.; Sabry, A.M.; Mahdy, R.E.; Khodeary, A. Management of patients with hepatitis B virus reactivation post–DAA treatment of chronic hepatitis C virus infection in HCV–HBV coinfected patients with pretreatment HBeAg seroconversion and early degree of hepatic fibrosis. Infect. Drug Resist. 2019, 12, 3067. [Google Scholar] [CrossRef] [Green Version]
- Gutiérrez García, M.L.; Manzano Alonso, M.L.; Ferrer Rosique, J.; Muñoz Gómez, R.; Alonso López, S.; Fernández Álvarez, I.; Fernández Rodríguez, C.M. Hepatitis B virus in patients with chronic hepatitis C treated with direct antiviral agents. Rev. Esp. Enferm. Dig. 2019, 111, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Tahir, M.; Ravikumar, N.P.G.; Chathura, W.; Martinez, A. 1024 A Retrospective Analysis of Hepatitis-B Reactivation in Hepatitis-C Patients Treated with Direct-Acting Antivirals Therapy. Am. J. Gastroenterol. 2019, 114, S587. [Google Scholar] [CrossRef]
- Nagaty, A.; Helmy, S.H.; Abd El-Wahab, E.W. Sofosbuvir-/Daclatasvir-based therapy for chronic HCV and HCV/hepatitis B virus coinfected patients in Egypt. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Jaroszewicz, J.; Pawłowska, M.; Simon, K.; Zarębska-Michaluk, D.; Lorenc, B.; Klapaczyński, J.; Tudrujek-Zdunek, M.; Sitko, M.; Mazur, W.; Janczewska, E. Low risk of HBV reactivation in a large European cohort of HCV/HBV coinfected patients treated with DAA. Expert Rev. Anti-Infect. Ther. 2020, 18, 1045–1054. [Google Scholar] [CrossRef]
- Xu, Q.; Zhang, W.; Ma, Y.X.; He, C.N.; Zhang, L.T.; Abulitifu, Y.; Li, Y.; Wang, N.; Wang, H.L.; Zhao, Y.Y.; et al. Twelve-week of sofosbuvir/velpatasvir therapeutic regimen for chronic hepatitis C patients in northwest region of China: A real-world multicenter clinical study. Zhonghua Gan Zang Bing Za Zhi 2021, 29, 1046–1052. [Google Scholar]
- Jiang, X.W.; Ye, J.Z.; Li, Y.T.; Li, L.J. Hepatitis B reactivation in patients receiving direct-acting antiviral therapy or interferon-based therapy for hepatitis C: A systematic review and meta-analysis. World J. Gastroenterol. 2018, 24, 3181–3191. [Google Scholar] [CrossRef]
- El Kassas, M.; Shimakawa, Y.; Ali-Eldin, Z.; Funk, A.L.; Wifi, M.N.; Zaky, S.; El-Raey, F.; Esmat, G.; Fontanet, A. Risk of hepatitis B virus reactivation with direct-acting antivirals against hepatitis C virus: A cohort study from Egypt and meta-analysis of published data. Liver Int. 2018, 38, 2159–2169. [Google Scholar] [CrossRef] [PubMed]
- Mücke, M.M.; Backus, L.I.; Mücke, V.T.; Coppola, N.; Preda, C.M.; Yeh, M.L.; Tang, L.S.Y.; Belperio, P.S.; Wilson, E.M.; Yu, M.L.; et al. Hepatitis B virus reactivation during direct-acting antiviral therapy for hepatitis C: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2018, 3, 172–180. [Google Scholar] [CrossRef]
- Shih, C.M.; Lo, S.J.; Miyamura, T.; Chen, S.Y.; Lee, Y.H. Suppression of hepatitis B virus expression and replication by hepatitis C virus core protein in HuH-7 cells. J. Virol. 1993, 67, 5823–5832. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.M.; Chen, C.M.; Chen, S.Y.; Lee, Y.H. Modulation of the trans-suppression activity of hepatitis C virus core protein by phosphorylation. J. Virol. 1995, 69, 1160–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schüttler, C.G.; Fiedler, N.; Schmidt, K.; Repp, R.; Gerlich, W.H.; Schaefer, S. Suppression of hepatitis B virus enhancer 1 and 2 by hepatitis C virus core protein. J. Hepatol. 2002, 37, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.Y.; Kao, C.F.; Chen, C.M.; Shih, C.M.; Hsu, M.J.; Chao, C.H.; Wang, S.H.; You, L.R.; Lee, Y.H. Mechanisms for inhibition of hepatitis B virus gene expression and replication by hepatitis C virus core protein. J. Biol. Chem. 2003, 278, 591–607. [Google Scholar] [CrossRef] [Green Version]
- Holmes, J.A.; Yu, M.L.; Chung, R.T. Hepatitis B reactivation during or after direct acting antiviral therapy—Implication for susceptible individuals. Expert Opin. Drug Saf. 2017, 16, 651–672. [Google Scholar] [CrossRef]
- Takeuchi, O.; Akira, S. Innate immunity to virus infection. Immunol. Rev. 2009, 227, 75–86. [Google Scholar] [CrossRef]
- Guo, L.; Wang, D.; Ouyang, X.; Tang, N.; Chen, X.; Zhang, Y.; Zhu, H.; Li, X. Recent Advances in HBV Reactivation Research. Biomed. Res. Int. 2018, 2018, 2931402. [Google Scholar] [CrossRef]
- Seto, W.K.; Chan, T.S.; Hwang, Y.Y.; Wong, D.K.; Fung, J.; Liu, K.S.; Gill, H.; Lam, Y.F.; Lie, A.K.; Lai, C.L.; et al. Hepatitis B reactivation in patients with previous hepatitis B virus exposure undergoing rituximab-containing chemotherapy for lymphoma: A prospective study. J. Clin. Oncol. 2014, 32, 3736–3743. [Google Scholar] [CrossRef]
- Kusumoto, S.; Tanaka, Y.; Suzuki, R.; Watanabe, T.; Nakata, M.; Takasaki, H.; Fukushima, N.; Fukushima, T.; Moriuchi, Y.; Itoh, K.; et al. Monitoring of Hepatitis B Virus (HBV) DNA and Risk of HBV Reactivation in B-Cell Lymphoma: A Prospective Observational Study. Clin. Infect. Dis. 2015, 61, 719–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishida, T.; Hiramatsu, N.; Mizuki, M.; Nagatomo, I.; Kida, H.; Tazumi, K.; Shinzaki, S.; Miyazaki, M.; Yakushijin, T.; Tatsumi, T.; et al. Managing hepatitis B virus carriers with systemic chemotherapy or biologic therapy in the outpatient clinic. Hepatol. Res. 2013, 43, 339–346. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Study Design | Population | HBsAg(+) Population | HBsAg(−), Anti-HBc(+) Population | Genotype | DAA |
|---|---|---|---|---|---|---|---|
| Wahle 2015 [14] | Brazil | Retrospective | 10 | 10 | 0 | NA | DAA |
| Gane 2016 [15] | USA | Prospective | 8 | 8 | NA | 1 | LDV/SOF |
| Wang 2016 [16] | China | Prospective | 355 | 10 | 1,2,3,6 | SOF + DCV/LDV + SOF/OMB + PTR + DAS | |
| Sulkowski 2016 [17] | Taiwan/Korea | Prospective | 178 | 0 | 103 | NA | LDV + SOF |
| Kim 2017 [18] | Korea | Prospective | 821 | 13 | NA | NA | DAA |
| Londono 2017 [19] | Spain | Prospective | 352 | 10 | 64 | 1,2,3,4 | OBV/PTV ± DSV ± RBV LDV/SOF ± RBV DCV/SOF ± RBV SOF + RBV DCV/SMV |
| Kawagishi 2017 [20] | Japan | Retrospective | 85 | 1 | 82 | 1,2 | LDV/SOF DCV/ASV SOF + RBV |
| Wang 2017 [21] | China | Prospective | 327 | 10 | 124 | 1,2 | LDV/SOF, DCV/SOF, OBV/PTV + DSV |
| Tamori 2017 [22] | Japan | Prospective | 160 | 25 | 765 | 1,2 | LDV/SOF DCV/ASV OMB/PTR SOF + RBV |
| Coppola 2017 [23] | Italy | Prospective | 16 | 16 | 0 | NA | DAA |
| Ancha 2017 [24] | USA | Retrospective | 941 | 0 | 188 | NA | DAA |
| Hayashi 2017 [25] | Japan | Retrospective | 256 | 17 | 80 | NA | DAA |
| Yeh 2017 [26] | Taiwan | Prospective | 64 | 7 | 57 | NA | LDV/SOF ± RBV, SOF + RBV, OMB/PrOD |
| Liu 2017 [27] | Taiwan | Prospective | 93 | 12 | 81 | 1,2 | LDV/SOF, LDV/SOF + RBV, SOF + RBV, PrOD, PrOD+RBV |
| Doi 2017 [28] | Japan | Prospective | 461 | 4 | 75 | 1,2 | DAA |
| Ogawa 2017 [29] | Japan | Retrospective | 183 | 2 | 63 | 1,2 | LDV, SOF |
| Mucke 2017 [30] | Germany | Prospective | 848 | 9 | 272 | 1,2,3,4 | LDV, SOF RBV, OBV/PTV + DSV RBV, DCV, SOF + RBV |
| Loggi 2017 [31] | Italy | Prospective | 137 | 2 | 42 | 1,2,3,4 | SOF ± RBV, SOF + LDV ± RBV, SOF + SMV ± RBV, PrOD ± RBV |
| Macera 2017 [32] | Italy | Prospective | 29 | 29 | 0 | NA | DAA |
| Belperio 2017 [33] | USA | Retrospective | 62290 | 377 | 7295 | NA | DAA |
| Tang 2017 [34] | Unknown | Unknown | 192 | 0 | NA | LDV/SOF, PrOD, SOF/VEL, GZR/EBR | |
| Calvaruso 2018 [35] | Italy | Retrospective | 104 | 8 | 37 | 1,2,3,4 | LDV/SOF ± RBV DCV/SOF + RBV SMV/SOF + RBV OBV/PTV/DSV + RBV SOF + RBV |
| Yanny 2018 [36] | USA | Retrospective | 283 | 156 | 127 | 1,4 | LDV + SOF |
| Preda 2018 [37] | Romania | Prospective | 2070 | 15 | NA | 1 | OBV/PTV/DSV + RBV |
| Butt 2018 [38] | USA | Retrospective | DAA:34632, PEG:23475 | DAA group:3322, PEG:1751 | DAA:9343, PEG:5005 | NA | SOF/SMV, SOF/LDV, PrOD, SOF/RBV |
| Lee 2018 [39] | Taiwan | Retrospective | 153 | 11 | 53 | 1,2 | SOF + LDV, PrOD, DCV + ASV |
| Park 2018 [40] | Korea | Retrospective | 62 | 62 | NA | NA | IFN: 34, DAA:24 |
| D’Ambrosio 2018 [41] | Italy | Prospective | 692 | 10 | 301 | 1 | DAA |
| Figueiredo 2018 [42] | Portugal | Prospective | 329 | 2 | 123 | NA | DAA |
| Wang 2018 [16] | China | Prospective | 111 | 111 | 0 | 1,2 | LDV/SOF |
| Liu 2018 [43] | Taiwan | Prospective | 111 | 110 | 0 | 1,2 | LDV + SOF |
| Ahmed 2019 [44] | Egypt | Prospective | 20 | 16 | 20 | NA | SOF + DAC + RBV: SOF + DAC:7, SOF + SIM:5 |
| Mucke 2019 [45] | Germany | Prospective | 822 | 9 | 263 | 1,2,3,4 | LDV, SOF ± RBV, OBV/PTV + RBV, OBV/PTV+DSV ± RBV, SMV, SOF ± RBV, DCV, SOF ± RBV,SOF + RBV |
| Osman 2019 [46] | Egypt | Prospective | 140 | 140 | NA | SOF + DCV | |
| GutierrezGarcia 2019 [47] | Spain | Prospective | 1337 | 7 | 356 | NA | DAA |
| Tahir 2019 [48] | Pakistan | Retrospective | 260 | 0 | 51 | NA | DAA |
| Nagaty 2020 [49] | Egypt | Prospective | 287 | 3 | 38 | NA | SOF + DCV, SOF + DCV + RBV |
| Jaroszewicz 2020 [50] | Poland | Retrospective | 10152 | 111 | 1239 | 1,3,4 | OBV/PTV/RBV ± DSV ± RBV, SOF, GZR/EBR ± RBV |
| Xu 2020 [51] | China | Prospective | 113 | 12 | 0 | 1,2,3 | SOF/VEL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.H.; Park, D.A.; Ko, M.J.; Yoo, J.-J.; Yim, S.Y.; Ahn, J.-H.; Jun, D.W.; Ahn, S.B. Direct-Acting Antivirals and the Risk of Hepatitis B Reactivation in Hepatitis B and C Co-Infected Patients: A Systematic Review and Meta-Analysis. J. Pers. Med. 2022, 12, 1957. https://doi.org/10.3390/jpm12121957
Oh JH, Park DA, Ko MJ, Yoo J-J, Yim SY, Ahn J-H, Jun DW, Ahn SB. Direct-Acting Antivirals and the Risk of Hepatitis B Reactivation in Hepatitis B and C Co-Infected Patients: A Systematic Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(12):1957. https://doi.org/10.3390/jpm12121957
Chicago/Turabian StyleOh, Joo Hyun, Dong Ah Park, Min Jung Ko, Jeong-Ju Yoo, Sun Young Yim, Ji-Hyun Ahn, Dae Won Jun, and Sang Bong Ahn. 2022. "Direct-Acting Antivirals and the Risk of Hepatitis B Reactivation in Hepatitis B and C Co-Infected Patients: A Systematic Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 12: 1957. https://doi.org/10.3390/jpm12121957