
Ventricular and Atrial Remodeling after Transcatheter Edge-to-Edge Repair: A Pilot Study
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Echocardiographic Assessment
2.2. Statistical Analysis
3. Results
3.1. Patient Population
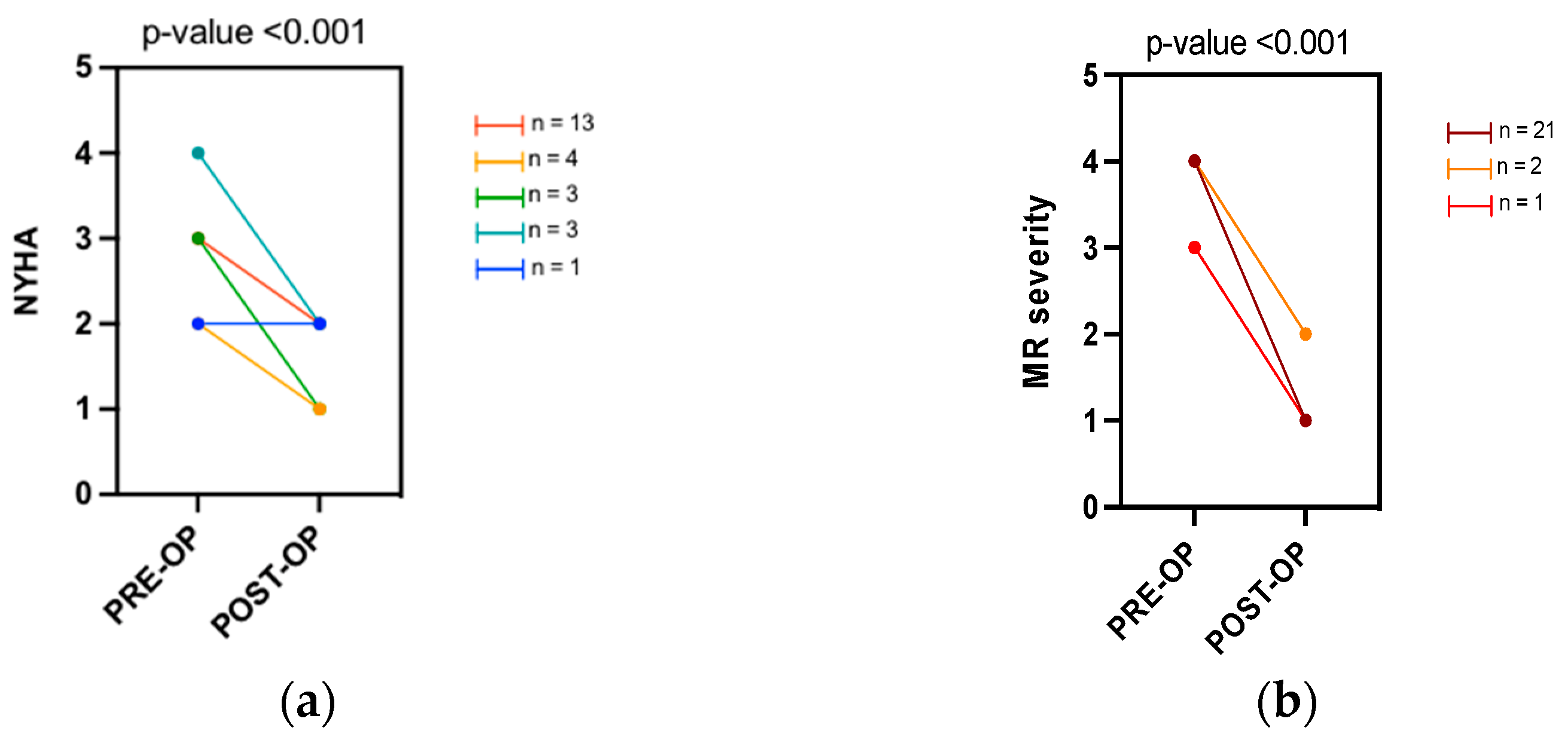
3.2. Clinical and Valve Regurgitation Assessment
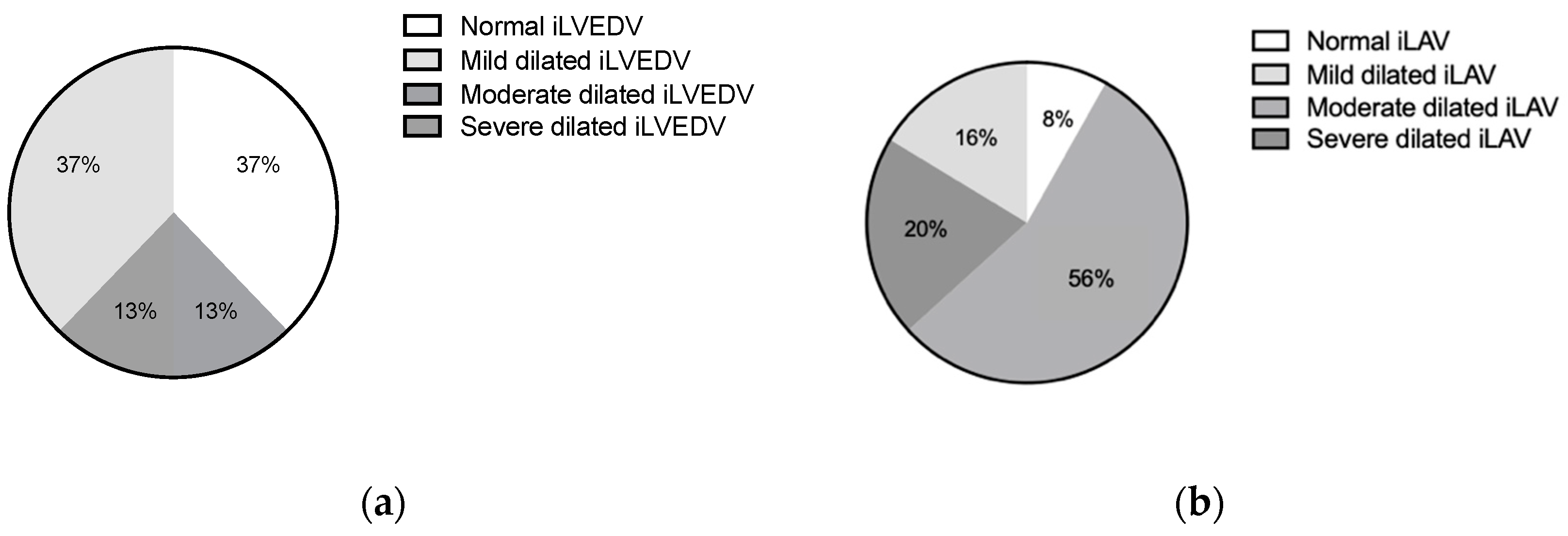
3.3. Baseline Echocardiographic Characteristics
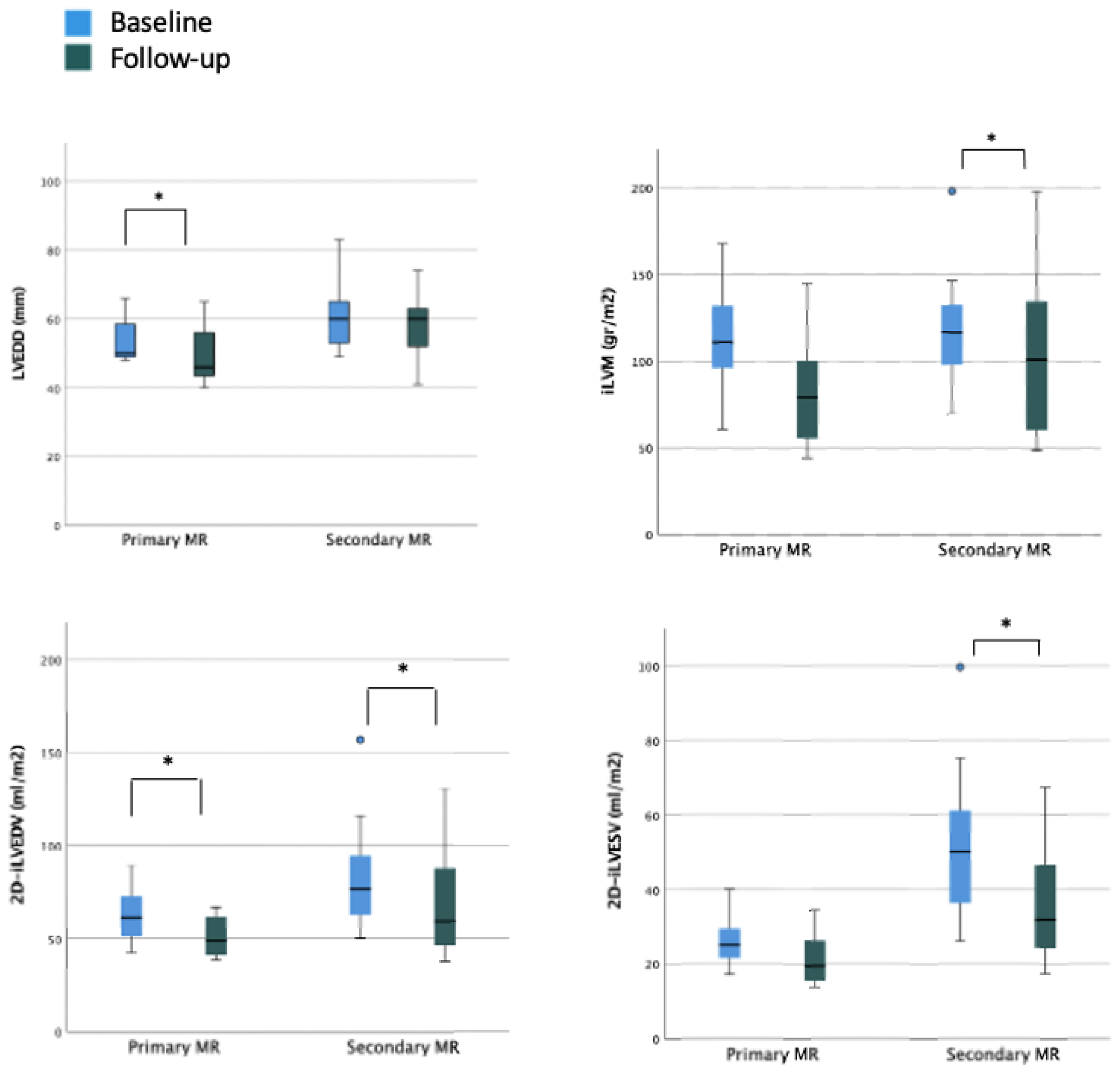
3.4. LV Size and Function during Follow-Up
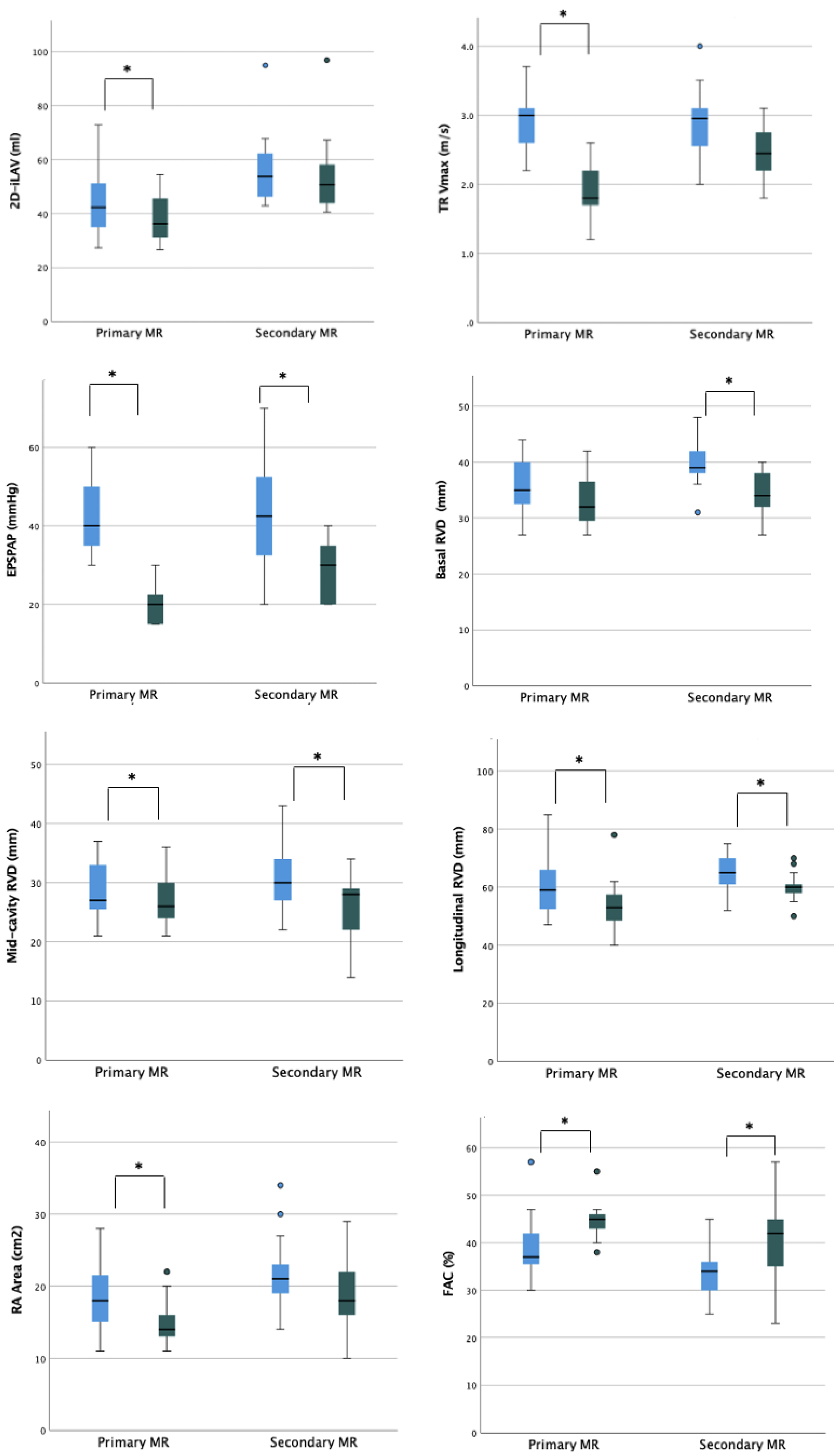
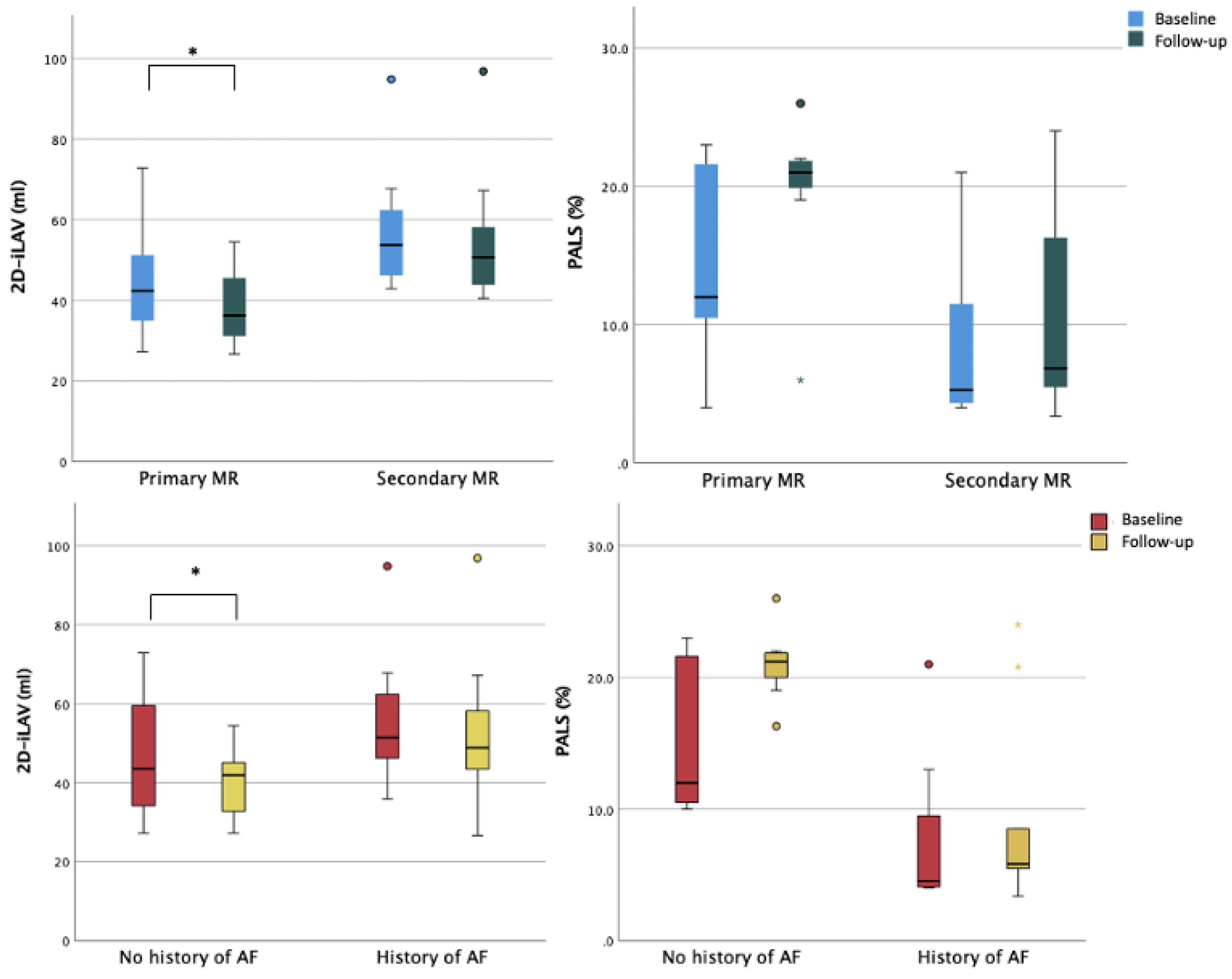
3.5. LA Size and Function during Follow-Up
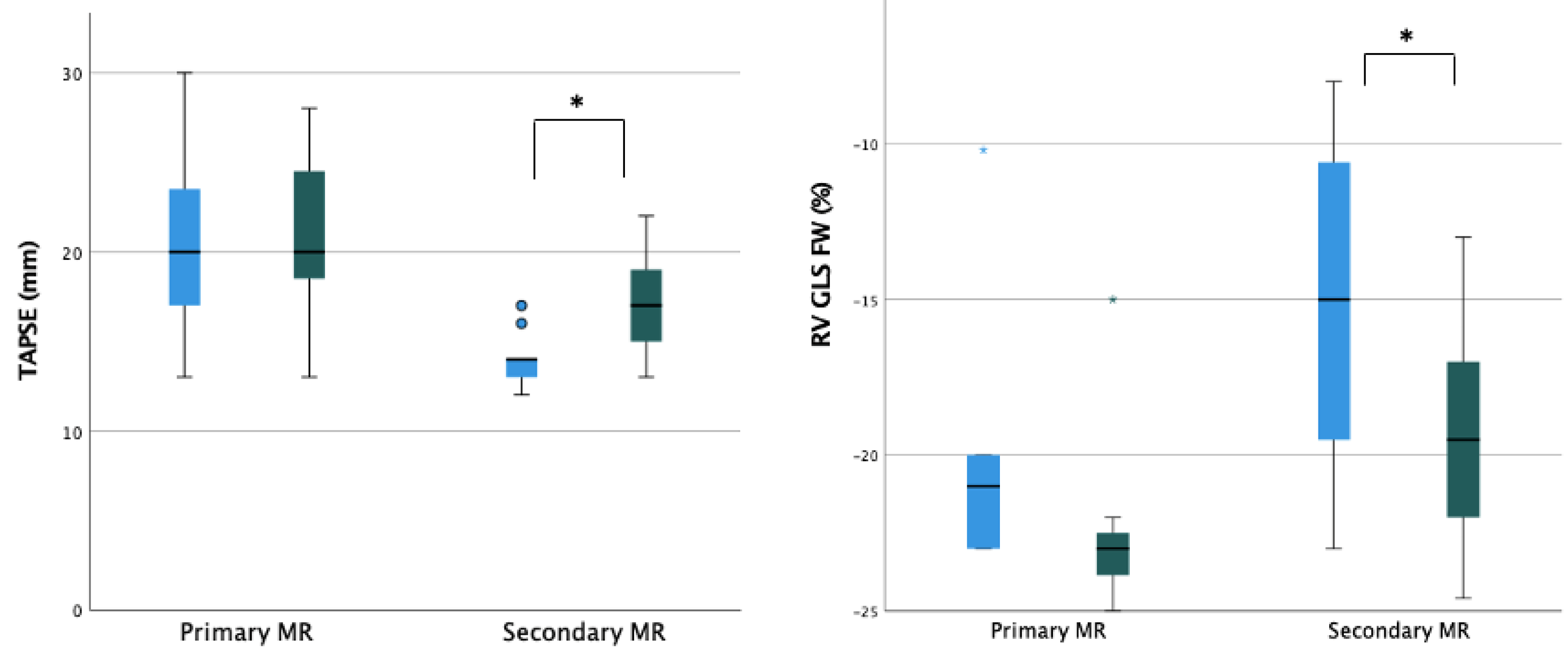
3.6. RV Size and Function during Follow-Up
4. Discussion
4.1. Right Chambers Remodeling
4.2. Left Ventricular and Atrial Chambers Remodeling
4.3. Overall Hemodynamic Impact of TEER
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El Sabbagh, A.; Reddy, Y.N.; Nishimura, R.A. Mitral Valve Regurgitation in the Contemporary Era: Insights into Diagnosis, Management, and Future Directions. JACC Cardiovasc. Imaging 2018, 11, 628–643. [Google Scholar] [CrossRef]
- SHyllen, S.; Nozohoor, S.; Ingvarsson, A.; Meurling, C.; Wierup, P.; Sjögren, J. Right ventricular performance after valve repair for chronic degenerative mitral regurgitation. Ann. Thorac. Surg. 2014, 98, 2023–2030. [Google Scholar] [CrossRef] [Green Version]
- Bonow, R.O.; O’Gara, P.T.; Adams, D.H.; Badhwar, V.; Bavaria, J.E.; Elmariah, S.; Hung, J.W.; Lindenfeld, J.; Morris, A.A.; Satpathy, R.; et al. 2020 Focused Update of the 2017 ACC Expert Consensus Decision Pathway on the Management of Mitral Regurgitation: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2020, 75, 2236–2270. [Google Scholar] [CrossRef]
- Lazam, S.; Vanoverschelde, J.-L.; Tribouilloy, C.; Grigioni, F.; M Suri, R.; Avierinos, J.-F.; de Meester, C.; Barbieri, A.; Rusinaru, D.; Russo, A.; et al. Twenty-Year Outcome after Mitral Repair Versus Replacement for Severe Degenerative Mitral Regurgitation: Analysis of a Large, Prospective, Multicenter, International Registry. Circulation 2017, 135, 410–422. [Google Scholar] [CrossRef]
- Feldman, T.; Kar, S.; Elmariah, S.; Smart, S.C.; Trento, A.; Siegel, R.J.; Apruzzese, P.; Fail, P.; Rinaldi, M.J.; Smalling, R.W.; et al. Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. J. Am. Coll. Cardiol. 2015, 66, 2844–2854. [Google Scholar] [CrossRef] [Green Version]
- Obadia, J.F.; Messika-Zeitoun, D.; Leurent, G.; Iung, B.; Bonnet, G.; Piriou, N.; Lefèvre, T.; Piot, C.; Rouleau, F.; Carrié, D.; et al. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. N. Engl. J. Med. 2018, 379, 2297–2306. [Google Scholar] [CrossRef]
- Grayburn, P.A.; Foster, E.; Sangli, C.; Weissman, N.J.; Massaro, J.; Glower, D.G.; Feldman, T.; Mauri, L. Relationship between the magnitude of reduction in mitral regurgitation severity and left ventricular and left atrial reverse remodeling after MitraClip therapy. Circulation 2013, 128, 1667–1674. [Google Scholar] [CrossRef] [Green Version]
- Nita, N.; Scharnbeck, D.; Schneider, L.M.; Seeger, J.; Wöhrle, J.; Rottbauer, W.; Keßler, M.; Markovic, S. Predictors of left ventricular reverse remodeling after percutaneous therapy for mitral regurgitation with the MitraClip system. Catheter. Cardiovasc. Interv. 2020, 96, 687–697. [Google Scholar] [CrossRef] [Green Version]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Ailawadi, G.; Lim, D.S.; Mack, M.J.; Trento, A.; Kar, S.; Grayburn, P.A.; Glower, D.D.; Wang, A.; Foster, E.; Qasim, A.; et al. One-Year Outcomes After MitraClip for Functional Mitral Regurgitation. Circulation 2019, 139, 37–47. [Google Scholar] [CrossRef]
- Shah, M.; Jorde, U.P. Percutaneous Mitral Valve Interventions (Repair): Current Indications and Future Perspectives. Front. Cardiovasc. Med. 2019, 6, 88. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [Green Version]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Mohammed, S.F.; Hussain, I.; AbouEzzeddine, O.F.; Takahama, H.; Kwon, S.H.; Forfia, P.; Roger, V.L.; Redfield, M.M. Right ventricular function in heart failure with preserved ejection fraction: A community-based study. Circulation 2014, 130, 2310–2320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer, P.; Filippatos, G.S.; Ahmed, M.I.; Iskandrian, A.E.; Bittner, V.; Perry, G.J.; White, M.; Aban, I.B.; Mujib, M.; Dell’Italia, L.J.; et al. Effects of right ventricular ejection fraction on outcomes in chronic systolic heart failure. Circulation 2010, 121, 252–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, C.; Hancock, B.W. Extreme pulmonary hypertension caused by mitral valve disease. Natural history and results of surgery. Br. Heart J. 1975, 37, 74–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onorati, F.; Santarpino, G.; Marturano, D.; Rubino, A.S.; Pasceri, E.; Zinzi, S.; Mascaro, G.; Cristodoro, L.; Renzulli, A. Successful surgical treatment of chronic ischemic mitral regurgitation achieves left ventricular reverse remodeling but does not affect right ventricular function. J. Thorac. Cardiovasc. Surg. 2009, 138, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Desai, R.R.; Abello, L.M.V.; Klein, A.L.; Marwick, T.H.; Krasuski, R.A.; Ye, Y.; Nowicki, E.R.; Rajeswaran, J.; Blackstone, E.H.; Pettersson, G.B. Tricuspid regurgitation and right ventricular function after mitral valve surgery with or without concomitant tricuspid valve procedure. J. Thorac. Cardiovasc. Surg. 2013, 146, 1126–1132.e10. [Google Scholar] [CrossRef] [Green Version]
- Le Tourneau, T.; Deswarte, G.; Lamblin, N.; Foucher-Hossein, C.; Fayad, G.; Richardson, M.; Polge, A.S.; Vannesson, C.; Topilsky, Y.; Juthier, F.; et al. Right ventricular systolic function in organic mitral regurgitation: Impact of biventricular impairment. Circulation 2013, 127, 1597–1608. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Ellis, J.; Kanda, L.; Corso, P.J. The role of right ventricular function in mitral valve surgery. Heart Surg. Forum 2013, 16, E170–E176. [Google Scholar] [CrossRef]
- Giannini, C.; Petronio, A.S.; De Carlo, M.; Guarracino, F.; Conte, L.; Fiorelli, F.; Pieroni, A.; Di Bello, V. Integrated reverse left and right ventricular remodelling after MitraClip implantation in functional mitral regurgitation: An echocardiographic study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godino, C.; Salerno, A.; Cera, M.; Agricola, E.; Fragasso, G.; Rosa, I.; Oppizzi, M.; Monello, A.; Scotti, A.; Magni, V.; et al. Impact and evolution of right ventricular dysfunction after successful MitraClip implantation in patients with functional mitral regurgitation. Int. J. Cardiol. Heart Vasc. 2016, 11, 90–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuser, J.; Buck, H.J.; Oldhafer, M.; Sieweke, J.T.; Bavendiek, U.; Bauersachs, J.; Widder, J.D.; Berliner, D. Right Ventricular Function Improves Early After Percutaneous Mitral Valve Repair in Patients Suffering From Severe Mitral Regurgitation. Front. Cardiovasc. Med. 2022, 9, 830944. [Google Scholar] [CrossRef] [PubMed]
- Scandura, S.; Ussia, G.P.; Capranzano, P.; Caggegi, A.; Sarkar, K.; Cammalleri, V.; Mangiafico, S.; Chiarandà, M.; Immè, S.; Di Pasqua, F.; et al. Left cardiac chambers reverse remodeling after percutaneous mitral valve repair with the MitraClip system. J. Am. Soc. Echocardiogr. 2012, 25, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Pleger, S.T.; Schulz-Schönhagen, M.; Geis, N.; Mereles, D.; Chorianopoulos, E.; Antaredja, M.; Lewening, M.; Katus, H.A.; Bekeredjian, R. One year clinical efficacy and reverse cardiac remodelling in patients with severe mitral regurgitation and reduced ejection fraction after MitraClip implantation. Eur. J. Heart Fail. 2013, 15, 919–927. [Google Scholar] [CrossRef]
- Toprak, C.; Kahveci, G.; Kilicgedik, A.; Pala, S.; Kirma, C.; Tabakci, M.M.; Inanir, M.; Esen, A.M. Left atrial remodeling in patients undergoing percutaneous mitral valve repair with the MitraClip system: An advanced echocardiography study. Echocardiography 2016, 33, 1504–1511. [Google Scholar] [CrossRef]
- Boriani, G.; Vitolo, M.; Imberti, J.F. Atrial cardiomyopathy: A derangement in atrial volumes, geometry, function, and pathology with important clinical implications. J. Cardiovasc. Med. 2022, 23, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Imberti, J.F.; Bonini, N.; Tosetti, A.; Mei, D.A.; Gerra, L.; Malavasi, V.L.; Mazza, A.; Lip, G.Y.; Boriani, G. Atrial High-Rate Episodes Detected by Cardiac Implantable Electronic Devices: Dynamic Changes in Episodes and Predictors of Incident Atrial Fibrillation. Biology 2022, 11, 443. [Google Scholar] [CrossRef]
- Boriani, G.; Vitolo, M.; Imberti, J.F.; Potpara, T.S.; Lip, G.Y. What do we do about atrial high rate episodes? Eur. Heart J. Suppl. 2020, 22, O42–O52. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Total Population (n = 24) | Primary MR (n = 11) | Secondary MR (n = 13) | p-Value |
|---|---|---|---|---|
| Males, n (%) | 15 (62.5) | 3 (27) | 12 (92) | 0.001 |
| Age (years), mean (± SD) | 78.5 (±7.6) | 77.09 (±7.8) | 79.7 (±7.5) | 0.404 |
| BSA Mosteller (m2), mean (± SD) | 1.8 (±0.2) | 1.7 (±0.2) | 2.0 (±0.2) | 0.019 |
| BMI (Kg/m2), mean (± SD) | 26.4 (± 4.1) | 26.2 (±4.3) | 26.7 (±4.2) | 0.398 |
| EuroSCORE II (%), median [IQR] | 4 [3.1–6.2] | 3.7 [2.8–4.5] | 4.8 [3.5–9.1] | 0.104 |
| STS score (%), median [IQR] | 3.5 [1.7–4.8] | 2.5 [1.2–5.8] | 3.6 [2.6–4.7] | 0.384 |
| NYHA class III, n (%) | 17 (70.8) | 7 (63) | 10 (77) | 0.476 |
| NYHA class IV, n (%) | 7 (29.2) | 4 (37) | 3 (23) | 0.476 |
| Dyslipidemia, n (%) | 13 (54.1) | 6 (54) | 7 (54) | 0.973 |
| Diabetes, n (%) | 7 (29.1) | 2 (19) | 5 (38) | 0.276 |
| Hypertension, n (%) | 16 (66.6) | 7 (64) | 9 (69) | 0.772 |
| Smoking history, n (%) | 7 (29.1) | 2 (19) | 5 (38) | 0.276 |
| Previous CABG, n (%) | 4 (16.6) | 1 (9) | 3 (23) | 0.360 |
| Previous PCI, n (%) | 13 (54.1) | 4 (36) | 9 (69) | 0.107 |
| Previous AMI, n (%) | 6 (25) | 1 (9) | 5 (38) | 0.098 |
| PM, n (%) | 2 (8.3) | 0 (0) | 2 (15) | 0.174 |
| Previous AV surgery, n (%) | 1 (4.1) | 0 (0) | 1 (7) | 0.347 |
| Previous TAVI, n (%) | 1 (4.1) | 0 (0) | 1 (7) | 0.347 |
| History of AF, n (%) | 14 (58.3) | 5 (45) | 9 (69) | 0.239 |
| DHP-CCBs, n (%) | 9 (37,5) | 4 (36) | 5 (38) | 0.916 |
| ACE-I, n (%) | 4 (16.6) | 2 (19) | 2 (15) | 0.855 |
| ARB, n (%) | 8 (33,3) | 2 (19) | 6 (46) | 0.148 |
| MRAs, n (%) | 22 (91.6) | 10 (90) | 12 (92) | 0.902 |
| Diuretics, n (%) | 23 (95.8) | 11 (100) | 12 (92) | 0.347 |
| Beta-blockers, n (%) | 21 (87.5) | 9 (82) | 12 (92) | 0.439 |
| Total Population (n = 24) | Primary MR (n = 11) | Secondary MR (n = 13) | p-Value | |
|---|---|---|---|---|
| LVEDD (mm) | 57.5 [50.0–64.5] | 50.0 [49.0–59.0] | 60.0 [53.0–65.0] | 0.059 |
| LVESD (mm) | 42.5 [37.8–50.5] | 42.0 [37.0–49.0] | 45.0 [40.5–52.0] | 0.450 |
| RWT | 0.32 [0.27–0.37] | 0.32 [0.29–0.38] | 0.31 [0.26–0.37] | 0.424 |
| iLVM (gr/m2) | 116.6 [95.7–132.4] | 111.1 [95.1–142.9] | 116.9 [96.2–136.4] | 0.820 |
| 2D-iLVEDV (mL/m2) | 67.5 [57.7–86.8] | 61.4 [45.4–77.7] | 76.4 [60.5–94.9] | 0.082 |
| 2D-iLVESV (mL/m2) | 35.4 [25.4–51.0] | 25.2 [21.2–39.8] | 50.2 [35.5–67.1] | 0.001 |
| 2D-LVEF (%) | 48.8 [39.8–58.1] | 59.1 [50.7–61.5] | 42.4 [35.9–48.2] | <0.001 |
| LV-S’ (TDI) (cm/s) | 8.0 [6.0–8.5] | 8.0 [7.5–9.5] | 6.5 [5.3–8.0] | 0.127 |
| 2D-iLAV (mL/m2) | 50.5 [42.5–62.3] | 42.3 [34.2–51.7] | 53.8 [45.2–62.6] | 0.052 |
| PALS (%) | 11.0 [4.5–19.0] | 12.0 [4.0–17.0] | 10.0 [5.0–17.0] | 0.786 |
| TR Vmax (m/s) | 2.9 [2.5–3.1] | 3.0 [2.5–3.1] | 2.9 [2.5–3.2] | 0.786 |
| EPSPAP (mmHg) | 40.0 [35.0–50.0] | 40.0 [35.0–50.0] | 42.5 [31.3–53.8] | 0.928 |
| Basal RVD (mm) | 38.5 [35.0–40.8] | 35.0 [31.0–40.0] | 39.0 [37.0–43.0] | 0.106 |
| Mid-cavity RVD (mm) | 29.5 [25.2–34.0] | 27.0 [25.0–34.0] | 30.0 [26.0–35.0] | 0.459 |
| Longitudinal RVD (mm) | 64.0 [55.2–69.8] | 59.0 [52–68] | 65.0 [60.5–71.0] | 0.119 |
| RA Area (cm2) | 19.5 [15.3–23.0] | 18.0 [15.0–23.0] | 21.0 [17.5–25.0] | 0.167 |
| FAC (%) | 35.5 [30.0–39.8] | 37.0 [35.0–44.0] | 34.0 [30.0–37.0] | 0.051 |
| TAPSE (mm) | 14.0 [13.0–19.2] | 20.0 [17.0–24.0] | 14.0 [13.0–14.0] | 0.003 |
| RV S’ (TDI) (cm/s) | 9.0 [7.0–12.0] | 9.0 [8.0–13.7] | 7.0 [6.0–10.8] | 0.127 |
| RV-FWLS (%) | −19.0 [−11.0–−22.0] | −21.0 [−15.1–−23.0] | −15.0 [−9.9–−19.8] | 0.127 |
| Baseline Assessment, Median [IQR] | Follow-Up Assessment, Median [IQR] | p-Value | |
|---|---|---|---|
| LVEDD (mm) | 57.5 [50.0–64.5] | 55.0 [45.3–60.0] | <0.001 |
| LVESD (mm) | 42.5 [37.8–50.5] | 44.5 [38.3–48.0] | 0.660 |
| RWT | 0.32 [0.27–0.37] | 0.34 [0.26–0.38] | 0.201 |
| iLVM (gr/m2) | 116.6 [95.7–132.4] | 90.2 [56.7–113.0] | 0.006 |
| 2D-iLVEDV (mL/m2) | 67.5 [57.7–86.8] | 53.5 [42.1–65.8] | <0.001 |
| 2D-iLVESV (mL/m2) | 35.4 [25.4–51.0] | 27.1 [19.7–42.9] | 0.002 |
| 2D-LVEF (%) | 48.8 [39.8–58.1] | 49.6 [43.8–60.6] | 0.248 |
| LV-S’ (TDI) (cm/s) | 8.0 [6.0–8.5] | 8.0 [7.5–9.0] | 0.053 |
| 2D-iLAV (ml/m2) | 50.5 [42.5–62.3] | 44.1 [37.4–56.4] | 0.004 |
| PALS (%) [N = 8] | 11.0 [4.5–19.0] | 14.6 [4.6–23.5] | 0.123 |
| TR Vmax (m/s) | 2.9 [2.5–3.1] | 2.2 [1.8–2.6] | <0.001 |
| EPSPAP (mmHg) | 40.0 [35.0–50.0] | 20.0 [20.0–30.0] | <0.001 |
| Basal RVD (mm) | 38.5 [35.0–40.8] | 33.5 [30.5–37.0] | <0.001 |
| Mid-cavity RVD (mm) | 29.5 [25.2–34.0] | 27.0 [22.3–29.8] | 0.001 |
| Longitudinal RVD (mm) | 64.0 [55.2–69.8] | 58.5 [53.0–61.0] | <0.001 |
| RA Area (cm2) | 19.5 [15.3–23.0] | 16.0 [13.2–20.0] | 0.002 |
| FAC (%) | 35.5 [30.0–39.8] | 44.0 [40.0–46.5] | <0.001 |
| TAPSE (mm) | 14.0 [13.0–19.2] | 18.5 [16.0–21.0] | <0.001 |
| RV S’ (TDI) (cm/s) | 9.0 [7.0–12.0] | 9.0 [9.0–12.0] | 0.049 |
| RV-FWLS (%) | −19.0 [−11.0–−22.0] | −21.0 [−16.0–−23.5] | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albini, A.; Passiatore, M.; Imberti, J.F.; Valenti, A.C.; Leo, G.; Vitolo, M.; Coppi, F.; Sgura, F.A.; Boriani, G. Ventricular and Atrial Remodeling after Transcatheter Edge-to-Edge Repair: A Pilot Study. J. Pers. Med. 2022, 12, 1916. https://doi.org/10.3390/jpm12111916
Albini A, Passiatore M, Imberti JF, Valenti AC, Leo G, Vitolo M, Coppi F, Sgura FA, Boriani G. Ventricular and Atrial Remodeling after Transcatheter Edge-to-Edge Repair: A Pilot Study. Journal of Personalized Medicine. 2022; 12(11):1916. https://doi.org/10.3390/jpm12111916
Chicago/Turabian StyleAlbini, Alessandro, Matteo Passiatore, Jacopo Francesco Imberti, Anna Chiara Valenti, Giulio Leo, Marco Vitolo, Francesca Coppi, Fabio Alfredo Sgura, and Giuseppe Boriani. 2022. "Ventricular and Atrial Remodeling after Transcatheter Edge-to-Edge Repair: A Pilot Study" Journal of Personalized Medicine 12, no. 11: 1916. https://doi.org/10.3390/jpm12111916